Analysis of Children’s Physical Characteristics Based on Clustering Analysis


Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Physical Growth Measurement
2.3. Physical Fitness Measurement
2.3.1. Muscular Endurance (Flexed Arm Hang)
2.3.2. Muscular Strength (Hand Grip Strength)
2.3.3. Flexibility (Sit and Reach)
2.3.4. Power (Long Jump)
2.3.5. Agility (Shuttle Run)
2.3.6. Balance (One Leg Stance Test)
2.4. Obesity
2.5. Basal Metabolic Rate (BMR)
2.6. Analysis Methods
2.6.1. Clustering Analysis on Factors of Physical Fitness
2.6.2. Statistical Analysis Method
3. Results
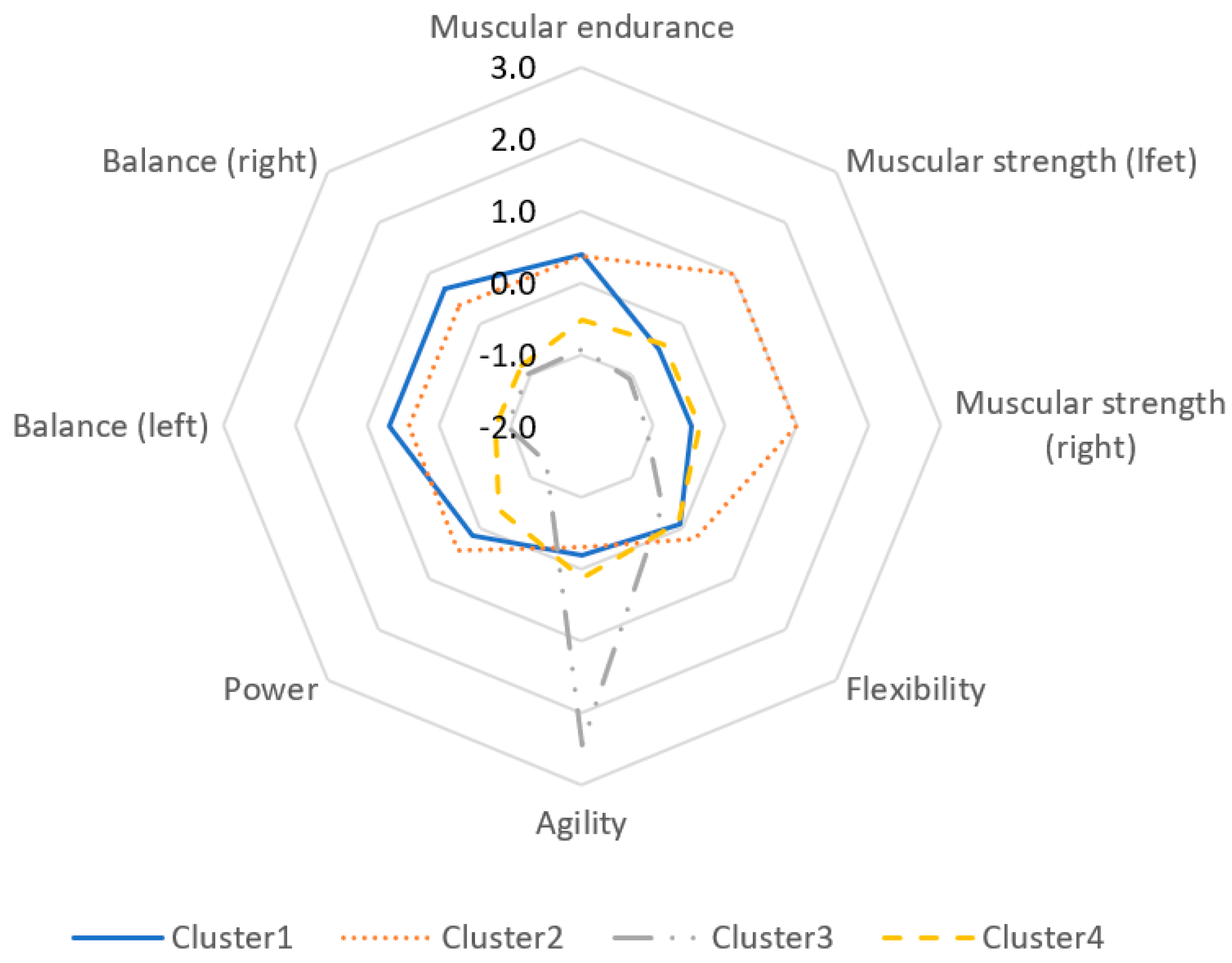
3.1. Physical Health Cluster
3.2. Distributional Difference of Physical Growth Clusters per Individual (Physical Development) Characteristic
3.3. Differences in Physical Development by Physical Fitness Clusters
3.4. Differences in Basal Metabolic Rate (BMR) by Physical Fitness Clusters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Conflicts of Interest
References
- World Health Organization. Guidelines on Physical Activity, Sedentary Behaviour and Sleep for Children under 5 Years of Age; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- World Health Organization. Report of the Commission on Ending Childhood Obesity; World Health Organization: Geneva, Switzerland. Available online: https://www.who.int/end-childhood-obesity/en/ (accessed on 20 February 2020).
- World Health Organization. Obesity and Overweight; World Health Organization: Geneva, Switzerland. Available online: https://www.who.int/en/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 20 February 2020).
- Waaler, H.T. Height. Weight and mortality the Norwegian experience. Acta Med. Scand. 1984, 215, 1–56. [Google Scholar] [CrossRef] [PubMed]
- Lindberg, L.; Danielsson, P.; Persson, M.; Marcus, C.; Hagman, E. Association of childhood obesity with risk of early all-cause and cause-specific mortality: A Swedish prospective cohort study. PLoS Med. 2020, 17, e1003078. [Google Scholar] [CrossRef]
- Black, R.E.; Morris, S.S.; Bryce, J. Where and why are 10 million children dying every year? Lancet 2003, 361, 2226–2234. [Google Scholar] [CrossRef]
- Moura-Dos-Santos, M.; Wellington-Barros, J.; Brito-Almeida, M.; Manhães-de-Castro, R.; Maia, J.; Góis Leandro, C. Permanent deficits in handgrip strength and running speed performance in low birth weight children. Am. J. Hum. Biol. 2013, 25, 58–62. [Google Scholar] [CrossRef]
- Lazzer, S.; Patrizi, A.; de Col, A.; Saezza, A.; Sartorio, A. Prediction of basal metabolic rate in obese children and adolescents considering pubertal stages and anthropometric characteristics or body composition. Eur. J. Clin. Nutr. 2014, 68, 695–699. [Google Scholar] [CrossRef]
- Raaijmakers, A.; Jacobs, L.; Rayyan, M.; van Tienoven, T.P.; Ortibus, E.; Levtchenko, E.; Staessen, J.A.; Allegaert, K. Catch–up growth in the first two years of life in Extremely Low Birth Weight (ELBW) infants is associated with lower body fat in young adolescence. PLoS ONE 2017, 12, e0173349. [Google Scholar] [CrossRef]
- Speakman, J.R.; Westerterp, K.R. Associations between energy demands, physical activity, and body composition in adult humans between 18 and 96 y of age. Am. J. Clin. Nutr. 2010, 92, 826–834. [Google Scholar] [CrossRef] [PubMed]
- Owen, O.E.; Kavle, E.; Owen, R.S.; Polansky, M.; Caprio, S.; Mozzoli, M.A.; Kendrick, Z.V.; Bushman, M.C.; Boden, G. A reappraisal of caloric requirements in healthy women. Am. J. Clin. Nutr. 1986, 44, 1–19. [Google Scholar] [CrossRef]
- Cunningham, J.J. Body composition as a determinant of energy expenditure: A synthetic review and a proposed general prediction equation. Am. J. Clin. Nutr. 1991, 54, 963–969. [Google Scholar] [CrossRef]
- Weinsier, R.L.; Schutz, Y.; Bracco, D. Reexamination of the relationship of resting metabolic rate to fat-free mass and to the metabolically active components of fat-free mass in humans. Am. J. Clin. Nutr. 1992, 55, 790–794. [Google Scholar] [CrossRef]
- Johnstone, A.M.; Murison, S.D.; Duncan, J.S.; Rance, K.A.; Speakman, J.R. Factors influencing variation in basal metabolic rate include fat-free mass, fat mass, age, and circulating thyroxine but not sex, circulating leptin, or triiodothyronine. Am. J. Clin. Nutr. 2005, 82, 941–948. [Google Scholar] [CrossRef]
- Powell, K.E.; Caspersen, C.J.; Koplan, J.P.; Ford, E.S. Physical activity and chronic diseases. Am. J. Clin. Nutr. 1989, 49, 999–1006. [Google Scholar] [CrossRef]
- Beunen, G.; Thomis, M. Muscular strength development in children and adolescents. Pediatric Exerc. Sci. 2000, 12, 174–197. [Google Scholar] [CrossRef]
- Ortega, F.B.; Tresaco, B.; Ruiz, J.R.; Moreno, L.A.; Martin-Matillas, M.; Mesa, J.L.; Warnberg, J.; Bueno, M.; Tercedor, P.; Gutiérrez, A. Cardiorespiratory fitness and sedentary activities are associated with adiposity in adolescents. Obesity 2007, 15, 1589–1599. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, J.R.; Ortega, F.B.; Meusel, D.; Harro, M.; Oja, P.; Sjöström, M. Cardiorespiratory fitness is associated with features of metabolic risk factors in children. Should cardiorespiratory fitness be assessed in a European health monitoring system? The European Youth Heart Study. J. Public Health 2006, 14, 94–102. [Google Scholar] [CrossRef]
- Andersen, L.B.; Hasselstrøm, H.; Grønfeldt, V.; Hansen, S.E.; Karsten, F. The relationship between physical fitness and clustered risk, and tracking of clustered risk from adolescence to young adulthood: Eight years follow-up in the Danish Youth and Sport Study. Int. J. Behav. Nutr. Phys. Act. 2004, 1, 1–4. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Cleland, V.J.; Ball, K.; Magnussen, C.; Dwyer, T.; Venn, A. Socioeconomic position and the tracking of physical activity and cardiorespiratory fitness from childhood to adulthood. Am. J. Epidemiol. 2009, 170, 1069–1077. [Google Scholar] [CrossRef]
- Twisk, J.W.; Kemper, H.C.; van Mechelen, W. The relationship between physical fitness and physical activity during adolescence and cardiovascular disease risk factors at adult age.The Amsterdam Growth and Health Longitudinal Study. Int. J. Sports Med. 2000, 32, 1455–1461. [Google Scholar] [CrossRef]
- Kristensen, P.L.; Wedderkopp, N.; Møller, N.C.; Andersen, L.B.; Bai, C.N.; Froberg, K. Tracking and prevalence of cardiovascular disease risk factors across socio-economic classes: A longitudinal substudy of the European Youth Heart Study. BMC Public Health 2006, 6, 20. [Google Scholar] [CrossRef]
- Cairney, J.; Hay, J.A.; Wade, T.J.; Faught, B.E.; Flouris, A. Developmental coordination disorder and aerobic fitness: Is it all in their heads or is measurement still the problem? Am. J. Hum. Biol. 2006, 18, 66–70. [Google Scholar] [CrossRef]
- Piek, J.B.; Bayman, G.B.; Barnett., N.C. The relathionship between fine and gross motor ability, self perception and self wort in children and adolescents. Hum. Mov. Sci. 2016, 25, 65–75. [Google Scholar] [CrossRef] [PubMed]
- Ortega, F.B.; Labayen, I.; Ruiz, J.R.; Kurvinen, E.; Loit, H.; Harro, J.; Veidebaum, T.; Sjöström, M. Improvements in fitness reduce the risk of becoming overweight across puberty. Med. Sci. Sports Exerc. 2011, 43, 1891–1897. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.J.; Eather, N.; Morgan, P.J.; Plotnikoff, R.C.; Faigenbaum, A.D.; Lubans, D.R. The health benefits of muscular fitness for children and adolescents: A systematic review and meta-analysis. Sports Med. 2014, 44, 1209–1223. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, J.R.; Castro-Piñero, J.; Artero, E.G.; Ortega, F.B.; Sjostrom, M.; Suni, J.; Castillo, M.J. Predictive validity of health-related fitness in youth: A systematic review. Br. J. Sports Med. 2009, 43, 909–923. [Google Scholar] [CrossRef] [PubMed]
- Högström, G.; Nordström, A.; Nordström, P. Aerobic fitness in late adolescence and the risk of early death: A prospective cohort study of 1.3 million Swedish men. Int. J. Epidemiol. 2016, 45, 1159–1168. [Google Scholar] [CrossRef]
- Ortega, F.B.; Silventoinen, K.; Tynelius, P.; Rasmussen, F. Muscular strength in male adolescents and premature death: Cohort study of one million participants. BMJ 2012, 345, e7279. [Google Scholar] [CrossRef]
- Sato, M.; Kodama, S.; Sugawara, A.; Saito, K.; Sone, H. Physical Fitness During Adolescence and Adult Mortality. Epidemiology 2009, 20, 463–464. [Google Scholar] [CrossRef]
- Gottlieb, G. The Relevance of Developmental-Psychobiological Metatheory to Developmental Neuropsychology. Dev. Neuropsychol. 2001, 19, 1–9. [Google Scholar] [CrossRef]
- Piek, J.P.; Hands, B.; Licari, M.K. Assessment of motor functioning in the preschool period. Neuropsychol. Rev. 2012, 22, 402–413. [Google Scholar] [CrossRef]
- Moore, L.L.; Nguyen, U.D.; Rothman, K.J.; Cupples, L.A.; Ellison, R.C. Preschool physical activity level and change in body fatness in young children: The Framingham Children’s Study. Am. J. Epidemiol. 1995, 142, 982–988. [Google Scholar] [CrossRef]
- Pica, R. Physical fitness and the early childhood curriculum. YC Young Child. 2006, 61, 12. [Google Scholar]
- Tyler, R. Basic principles of curriculum and instruction. In The Curriculum Studies Reader; Flinders, D.J., Thornton, S.J., Eds.; Routledge: London, UK, 2008. [Google Scholar]
- Oh, S.H. The latest trend in measuring infant physical activity. Proc. Korean Soc. Early Child. Phys. Educ. 2006, 7–14. Available online: https://kiss.kstudy.com/thesis/thesis-view.asp?key=2633857 (accessed on 25 November 2006).
- Cadenas-Sanchez, C.; Intemann, T.; Labayen, I.; Peinado, A.B.; Vidal-Conti, J.; Sanchis-Moysi, J.; Moliner-Urdiales, D.; Rodriguez Perez, M.A.; Cañete Garcia-Prieto, J.; Fernández-Santos, J.D.R.; et al. Physical fitness reference standards for preschool children: The PREFIT project. J. Sci. Med. Sport 2019, 22, 430–437. [Google Scholar] [CrossRef]
- California Department of Education. FITNESSGRAM Performance Standards, 2015–16 HFZ Charts. Available online: www.cde.ca.gov/ta/tg/pf/documents/pft15hfzstd.pdf (accessed on 10 May 2020).
- Kim, E.J.; Ahn, N.Y. The Effect of Home-Based Physical Activities on Physical Fitness in Children. Korean J. Growth Dev. 2018, 26, 119–129. [Google Scholar] [CrossRef]
- Ministry of Education. PAPS (PAPS: Physical Activity Promotion System); Ministry of Education: Sejong, Korea, 2009.
- Korea Disease Control and Prevention Agency. 2007 Korean National Growth Charts for children and adolescents; Commentary; Korea Disease Control and Prevention Agency: Cheongju-si, Korea, 2007.
- Henry, C. Basal metabolic rate studies in humans: Measurement and development of new equations. Public Health Nutr. 2005, 8, 1133–1152. [Google Scholar] [CrossRef]
- Sinaga, K.P.; Yang, M. Unsupervised K-means clustering algorithm. IEEE Access 2020, 8, 80716–80727. [Google Scholar] [CrossRef]
- MacQueen, J. Some methods for classification and analysis of multivariate observations. In Proceedings of the Fifth Berkeley Symposium on Mathematical Statistics and Probability, Oakland, CA, USA, 1 January 1967; Volume 1, pp. 281–297. [Google Scholar]
- Velicer, W.F.; Redding, C.A.; Anatchkova, M.D.; Fava, J.L.; Prochaska, J.O. Identifying cluster subtypes for the prevention of adolescent smoking acquisition. Addict. Behav. 2007, 32, 228–247. [Google Scholar] [CrossRef]
- Jeon, Y.; Eom, K. Role of physique and physical fitness in the balance of Korean national snowboard athletes. J. Exerc. Sci. Fit. 2021, 19, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Çetin, E. Is there a gender difference for agility in children age 7–12 years? Int. J. Acad. Res. 2013, 5, 487–490. [Google Scholar] [CrossRef]
- Hariadi, I.; Fadhli, N.R.; Yudasmara, D.S. In Relationship Between Body Mass Index (BMI) with Agility of Elementary School Children. In Proceedings of the 2nd International Conference on Sports Sciences and Health 2018 (2nd ICSSH 2018), Dordrecht, The Netherlands, February 2019; Atlantis Press: Dordrecht, The Netherlands, 2019; pp. 98–101. [Google Scholar] [CrossRef]
- Goodway, J.D.; Ozmun, J.C.; Gallahue, D.L. Understanding Motor Development: Infants, Children, Adolescents, Adults, 8th ed.; Jones & Bartlett Learning: Burlington, MA, USA, 2019. [Google Scholar]
- Wrotniak, B.H.; Epstein, L.H.; Dorn, J.M.; Jones, K.E.; Kondilis, V.A. The relationship between motor proficiency and physical activity in children. Pediatrics 2006, 118, e1758–e1765. [Google Scholar] [CrossRef] [PubMed]
- Landy, J.; Burridge, K. 50 Simple Things You Can Do to Raise a Child who is Physically Fit; Macmillan: London, UK, 1997. [Google Scholar]
- Arnold, B.L.; Schmitz, R.J. Examination of balance measures produced by the biodex stability system. J. Athl. Train. 1998, 33, 323. [Google Scholar] [PubMed]
- Cratty, B.J.; Martin, M.M. Perceptual-Motor Efficiency in Children: The Measurement and Improvement of Movement Attributes; Lea & Febiger: Palo Alto, CA, USA, 1969. [Google Scholar]
- McGraw, B.; McClenaghan, B.A.; Williams, H.G.; Dickerson, J.; Ward, D.S. Gait and postural stability in obese and nonobese prepubertal boys. Arch. Phys. Med. Rehabil. 2000, 81, 484–489. [Google Scholar] [CrossRef]
- Ridgway, C.L.; Brage, S.; Anderssen, S.A.; Sardinha, L.B.; Andersen, L.B.; Ekelund, U. Do physical activity and aerobic fitness moderate the association between birth weight and metabolic risk in youth?: The European Youth Heart Study. Diabetes Care 2011, 34, 187–192. [Google Scholar] [CrossRef]
- Hohenadel, M.G.; Hollstein, T.; Thearle, M.; Reinhardt, M.; Piaggi, P.; Salbe, A.D.; Krakoff, J. A low resting metabolic rate in late childhood is associated with weight gain in adolescence. Metab. Clin. Exp. 2019, 93, 68–74. [Google Scholar] [CrossRef]
- Webb, P. Energy expenditure and fat-free mass in men and women. Am. J. Clin. Nutr. 1981, 34, 1816–1826. [Google Scholar] [CrossRef] [PubMed]
- Nobre, I.G.; Moura-dos-Santos, M.A.; Nobre, G.G.; dos Santos, R.M.; da Costa Ribeiro, I.; Santos, G.C.J.; da Fonseca, E.V.d.S.; de Oliveira, T.L.P.S.; E Silva, W.T.F.; Nazare, J.-A. The mediation effect of anthropometry and physical fitness on the relationship between birthweight and basal metabolic rate in children. J. Dev. Orig. Health Dis. 2020, 11, 640–647. [Google Scholar] [CrossRef] [PubMed]
- Korea Institute of Sport Science. Developing Standard Training Guidelines for Each Athlete’s Growth Stage; Korea Institute of Sport Science: Seoul, Korea, 2005. [Google Scholar]
- Cole, S.Z.; Lanham, J.S. Failure to thrive: An update. Am. Fam. Physician 2011, 83, 829–834. [Google Scholar] [PubMed]


{kind=link}
| Cluster No. | n | % | Muscular Endurance | Muscular Strength (Left) | Muscular Strength (Right) | Flexibility | Agility | Power | Balance (Left) | Balance (Right) | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Total | 1 | 1242 | 28.2% | 41.73 ± 17.14 | 6.86 ± 1.65 | 7.30 ± 1.71 | 27.29 ± 7.04 | 13.3 ± 1.35 | 18.35 ± 3.92 | 48.37 ± 15.10 | 50.20 ± 14.31 |
| 2 | 1406 | 31.9% | 41.29 ± 17.58 | 10.51 ± 1.71 | 10.96 ± 1.71 | 29.36 ± 7.15 | 13.07 ± 1.43 | 19.6 ± 3.96 | 42.39 ± 17.85 | 43.54 ± 17.83 | |
| 3 | 210 | 4.80% | 16.63 ± 16.35 | 5.52 ± 2.14 | 5.74 ± 2.22 | 24.66 ± 7.76 | 18.15 ± 3.20 | 12.28 ± 3.65 | 14.97 ± 14.28 | 15.87 ± 14.82 | |
| 4 | 1552 | 35.2% | 24.50 ± 15.89 | 7.20 ± 2.00 | 7.64 ± 2.00 | 26.83 ± 7.72 | 13.88 ± 1.36 | 16.18 ± 3.59 | 18.11 ± 12.91 | 18.68 ± 13.26 | |
| Male | 1 | 610 | 26.7% | 42.53 ± 17.06 | 7.41 ± 1.59 | 7.86 ± 1.65 | 25.97 ± 7.26 | 13.02 ± 1.30 | 19.03 ± 4.01 | 45.83 ± 16.00 | 47.71 ± 15.17 |
| 2 | 732 | 32.0% | 42.80 ± 17.13 | 11.18 ± 1.62 | 11.55 ± 1.63 | 28.15 ± 7.00 | 12.75 ± 1.28 | 20.31 ± 4.09 | 39.76 ± 18.11 | 40.15 ± 18.36 | |
| 3 | 105 | 4.60% | 14.84 ± 14.44 | 6.10 ± 2.16 | 6.10 ± 2.31 | 23.86 ± 7.77 | 18.24 ± 3.74 | 12.22 ± 4.03 | 13.78 ± 14.24 | 13.59 ± 12.21 | |
| 4 | 838 | 36.7% | 25.53 ± 16.44 | 7.72 ± 1.98 | 8.11 ± 2.01 | 25.53 ± 7.67 | 13.58 ± 1.31 | 16.6 ± 3.7 | 15.82 ± 10.90 | 16.75 ± 12.08 | |
| Female | 1 | 632 | 29.7% | 0.97 ± 17.21 | 6.33 ± 1.52 | 6.77 ± 1.59 | 28.56 ± 6.58 | 13.58 ± 1.35 | 17.69 ± 3.71 | 50.82 ± 13.75 | 52.62 ± 13.00 |
| 2 | 674 | 31.7% | 39.64 ± 17.93 | 9.79 ± 1.50 | 10.32 ± 1.57 | 30.67 ± 7.07 | 13.43 ± 1.50 | 18.82 ± 3.68 | 45.25 ± 17.12 | 47.22 ± 16.48 | |
| 3 | 105 | 4.90% | 18.43 ± 17.95 | 4.93 ± 1.96 | 5.38 ± 2.09 | 25.45 ± 7.71 | 18.07 ± 2.56 | 12.34 ± 3.25 | 16.16 ± 14.28 | 18.15 ± 16.79 | |
| 4 | 714 | 33.6% | 23.29 ± 15.14 | 6.59 ± 1.85 | 7.09 ± 1.84 | 28.36 ± 7.50 | 14.23 ± 1.33 | 15.68 ± 3.39 | 20.8 ± 14.49 | 20.94 ± 14.20 |
| Cluster 1 | Cluster 2 | Cluster 3 | Cluster 4 | Total | Chi-Square | p | |||
|---|---|---|---|---|---|---|---|---|---|
| Gender | M | 610 (26.7) | 732 (32) | 105 (4.6) | 838 (36.7) | 2285 (100) | 6.894 | 0.075 | |
| F | 632 (29.7) | 674 (31.7) | 105 (4.9) | 714 (33.6) | 2125 (100) | ||||
| Physical Development | M | Underweight | 20 (37) | 2 (3.7) | 7 (13) | 25 (46.3) | 54 (100) | 83.511 | 0.000 |
| Normal | 514 (30.3) | 525 (30.9) | 66 (3.9) | 593 (34.9) | 1698 (100) | ||||
| Overweight | 44 (15.5) | 110 (38.9) | 13 (4.6) | 116 (41) | 283 (100) | ||||
| Obese | 32 (12.8) | 95 (38) | 19 (7.6) | 104 (41.6) | 250 (100) | ||||
| F | Underweight | 21 (32.3) | 8 (12.3) | 7 (10.8) | 29 (44.6) | 65 (100) | 88.522 | 0.000 | |
| Normal | 536 (34.2) | 492 (31.4) | 61 (3.9) | 478 (30.5) | 1567 (100) | ||||
| Overweight | 55 (16.4) | 114 (33.9) | 24 (7.1) | 143 (42.6) | 336 (100) | ||||
| Obese | 20 (12.7) | 60 (38.2) | 13 (8.3) | 64 (40.8) | 157 (100) | ||||
| Total | 119 (2.7) | 3265 (74) | 619 (14) | 407 (9.2) | 4410 (100) | ||||
| Total | Male | Female | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | F | p | Mean | SD | F | p | Mean | SD | F | p | ||
| Height | Cluster 1 | 117.30 | 4.31 | 124.247 | <0.001 | 117.75 | 4.37 | 77.066 | <0.001 | 116.86 | 4.22 | 50.582 | <0.001 |
| Cluster 2 | 120.53 | 4.71 | 121.30 | 4.51 | 119.71 | 4.80 | |||||||
| Cluster 3 | 116.62 | 6.26 | 117.90 | 6.20 | 115.35 | 6.10 | |||||||
| Cluster 4 | 118.38 | 5.00 | 118.89 | 4.90 | 117.78 | 5.04 | |||||||
| Total | 118.68 | 4.98 | 119.31 | 4.92 | 118.00 | 4.96 | |||||||
| Weight | Cluster 1 | 21.99 | 3.22 | 115.906 | <0.001 | 22.32 | 3.36 | 65.423 | <0.001 | 21.67 | 3.04 | 49.691 | <0.001 |
| Cluster 2 | 24.66 | 4.37 | 25.25 | 4.41 | 24.03 | 4.25 | |||||||
| Cluster 3 | 23.37 | 5.49 | 24.18 | 6.07 | 22.55 | 4.73 | |||||||
| Cluster 4 | 23.62 | 4.49 | 23.98 | 4.69 | 23.21 | 4.22 | |||||||
| Total | 23.48 | 4.31 | 23.95 | 4.49 | 22.98 | 4.05 | |||||||
| Total | Male | Female | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | F | p | Mean | SD | F | p | Mean | SD | F | p | |
| Cluster 1 | 975.17 | 68.37 | 102.678 | <0.001 | 1012.75 | 60.57 | 73.579 | <0.001 | 938.90 | 54.50 | 52.214 | <0.001 |
| Cluster 2 | 1027.04 | 86.89 | 1068.11 | 76.36 | 982.44 | 74.84 | ||||||
| Cluster 3 | 995.58 | 106.48 | 1041.33 | 106.34 | 949.84 | 85.17 | ||||||
| Cluster 4 | 1006.40 | 87.52 | 1041.39 | 82.18 | 965.33 | 74.88 | ||||||
| Total | 1003.67 | 85.80 | 1042.30 | 79.26 | 962.13 | 72.09 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, E.; Won, Y.; Shin, J. Analysis of Children’s Physical Characteristics Based on Clustering Analysis. Children 2021, 8, 485. https://doi.org/10.3390/children8060485
Kim E, Won Y, Shin J. Analysis of Children’s Physical Characteristics Based on Clustering Analysis. Children. 2021; 8(6):485. https://doi.org/10.3390/children8060485
Chicago/Turabian StyleKim, Eunjung, Yumi Won, and Jieun Shin. 2021. "Analysis of Children’s Physical Characteristics Based on Clustering Analysis" Children 8, no. 6: 485. https://doi.org/10.3390/children8060485
APA StyleKim, E., Won, Y., & Shin, J. (2021). Analysis of Children’s Physical Characteristics Based on Clustering Analysis. Children, 8(6), 485. https://doi.org/10.3390/children8060485