
Respiratory Failure in an Extremely Premature Neonate with COVID-19

 ,
,
Abstract
1. Introduction
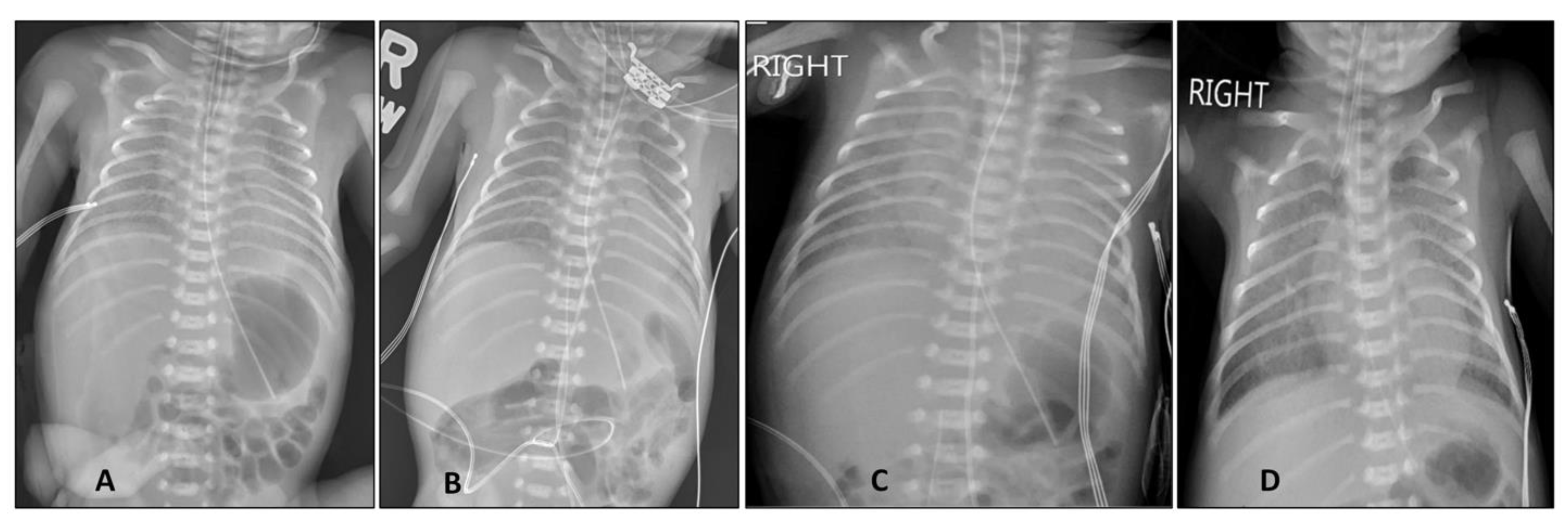
2. Case Report
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lambert, H.; Gupte, J.; Fletcher, H.; Hammond, L.; Lowe, N.; Pelling, M.; Raina, N.; Shahid, T.; Shanks, K. COVID-19 as a global challenge: Towards an inclusive and sustainable future. Lancet Planet Health 2020, 4, e312–e314. [Google Scholar] [CrossRef]
- Chen, H.; Guo, J.; Wang, C.; Luo, F.; Yu, X.; Zhang, W.; Li, J.; Zhao, D.; Xu, D.; Gong, Q.; et al. Clinical characteristics and intrauterine vertical transmission potential of COVID-19 infection in nine pregnant women: A retrospective review of medical records. Lancet 2020, 395, 809–815. [Google Scholar] [CrossRef]
- Dong, L.; Tian, J.; He, S.; Zhu, C.; Wang, J.; Liu, C.; Yang, J. Possible Vertical Transmission of SARS-CoV-2 From an Infected Mother to Her Newborn. JAMA J. Am. Med. Assoc. 2020, 323, 1846–1848. [Google Scholar] [CrossRef] [PubMed]
- Fenizia, C.; Biasin, M.; Cetin, I.; Vergani, P.; Mileto, D.; Spinillo, A.; Gismondo, M.R.; Perotti, F.; Callegari, C.; Mancon, A.; et al. Analysis of SARS-CoV-2 vertical transmission during pregnancy. Nat. Commun. 2020, 11, 5128. [Google Scholar] [CrossRef]
- Alzamora, M.C.; Paredes, T.; Caceres, D.; Webb, C.M.; Valdez, L.M.; La Rosa, M. Severe COVID-19 during Pregnancy and Possible Vertical Transmission. Am. J. Perinatol. 2020, 37, 861–865. [Google Scholar] [PubMed]
- Demirjian, A.; Singh, C.; Tebruegge, M.; Herbert, R.; Draz, N.; Mirfenderesky, M.; Jones, V.; Hinstridge, P.; Seneviratne, R.; Myers, R.; et al. Probable Vertical Transmission of SARS-CoV-2 Infection. Pediatr. Infect. Dis. J. 2020, 39, e257–e260. [Google Scholar] [CrossRef] [PubMed]
- Kirtsman, M.; Diambomba, Y.; Poutanen, S.M.; Malinowski, A.K.; Vlachodimitropoulou, E.; Parks, W.T.; Erdman, L.; Morris, S.K.; Shah, P.S. Probable congenital SARS-CoV-2 infection in a neonate born to a woman with active SARS-CoV-2 infection. CMAJ 2020, 192, E647–E650. [Google Scholar] [CrossRef]
- Zamaniyan, M.; Ebadi, A.; Aghajanpoor, S.; Rahmani, Z.; Haghshenas, M.; Azizi, S. Preterm delivery, maternal death, and vertical transmission in a pregnant woman with COVID-19 infection. Prenat. Diagn. 2020, 40, 1759–1761. [Google Scholar] [CrossRef]
- Fenton, T.R.; Kim, J.H. A systematic review and meta-analysis to revise the Fenton growth chart for preterm infants. BMC Pediatrics 2013, 13, 59. [Google Scholar] [CrossRef]
- Attaway, A.H.; Scheraga, R.G.; Bhimraj, A.; Biehl, M.; Hatipoglu, U. Severe covid-19 pneumonia: Pathogenesis and clinical management. BMJ 2021, 372, n436. [Google Scholar] [CrossRef]
- Tom, M.R.; Mina, M.J. To Interpret the SARS-CoV-2 Test, Consider the Cycle Threshold Value. Clin. Infect. Dis. 2020, 71, 2252–2254. [Google Scholar] [CrossRef]
- Piersigilli, F.; Carkeek, K.; Hocq, C.; Van Grambezen, B.; Hubinont, C.; Chatzis, O.; Van der Linden, D.; Danhaive, O. COVID-19 in a 26-week preterm neonate. Lancet Child Adolesc Health. 2020, 4, 476–478. [Google Scholar] [CrossRef]
- Ramakrishnan, S.; Nicolau, D.V., Jr.; Langford, B.; Mahdi, M.; Jeffers, H.; Mwasuku, C.; Krassowska, K.; Fox, R.; Binnian, I.; Glover, V.; et al. Inhaled budesonide in the treatment of early COVID-19 (STOIC): A phase 2, open-label, randomised controlled trial. Lancet Respir. Med. 2021. [Google Scholar] [CrossRef]
- Narang, S.; Roy, J.; Stevens, T.P.; Butler-O’Hara, M.; Mullen, C.A.; D’Angio, C.T. Risk factors for umbilical venous catheter-associated thrombosis in very low birth weight infants. Pediatr. Blood Cancer 2009, 52, 75–79. [Google Scholar] [CrossRef] [PubMed]
- Veldman, A.; Nold, M.F.; Michel-Behnke, I. Thrombosis in the critically ill neonate: Incidence, diagnosis, and management. Vasc Health Risk Manag. 2008, 4, 1337–1348. [Google Scholar] [PubMed]
- Rodríguez, C.; Luque, N.; Blanco, I.; Sebastian, L.; Barberà, J.A.; Peinado, V.I.; Tura-Ceide, O. Pulmonary Endothelial Dysfunction and Thrombotic Complications in Patients with COVID-19. Am. J. Respir. Cell Mol. Biol. 2021, 64, 407–415. [Google Scholar] [CrossRef] [PubMed]
- Vivanti, A.J.; Vauloup-Fellous, C.; Prevot, S.; Zupan, V.; Suffee, C.; Do Cao, J.; Benachi, A.; De Luca, D. Transplacental transmission of SARS-CoV-2 infection. Nat Commun. 2020, 11, 3572. [Google Scholar] [CrossRef] [PubMed]
- Muhidin, S.; Behboodi Moghadam, Z.; Vizheh, M. Analysis of Maternal Coronavirus Infections and Neonates Born to Mothers with 2019-nCoV; a Systematic Review. Arch. Acad. Emerg. Med. 2020, 8, e49. [Google Scholar]
- Dumitriu, D.; Emeruwa, U.N.; Hanft, E.; Liao, G.V.; Ludwig, E.; Walzer, L.; Arditi, B.; Saslaw, M.; Andrikopoulou, M.; Scripps, T.; et al. Outcomes of Neonates Born to Mothers with Severe Acute Respiratory Syndrome Coronavirus 2 Infection at a Large Medical Center in New York City. JAMA Pediatrics 2021, 175, 157–167. [Google Scholar] [CrossRef]
- Kimberlin, D.W.; Puopolo, K.M. Balancing Risks in the Time of COVID-19. JAMA Pediatrics 2021, 175, 129–130. [Google Scholar] [CrossRef]
- Li, M.; Chen, L.; Zhang, J.; Xiong, C.; Li, X. The SARS-CoV-2 receptor ACE2 expression of maternal-fetal interface and fetal organs by single-cell transcriptome study. PLoS ONE 2020, 15, e0230295. [Google Scholar]
- Wyckoff, A.S. AAP issues guidance on infants born to mothers with suspected or confirmed COVID-19. Am. Acad. Pediatrics 2020, 29. Available online: https://www.aappublications.org/news/2020/04/02/infantcovidguidance040220 (accessed on 14 March 2021).


{kind=link}
| Day after Birth | Specimen | SARS-CoV-2 Result | Ct Value (S Gene) | Ct Value (ORF1ab Gene) |
|---|---|---|---|---|
| Day 1 (24 h) | Nasopharyngeal | Positive | 17 | 17 |
| Day 2 (48 h) * | Nasopharyngeal | Positive | ||
| Day 14 | Nasopharyngeal | Positive | 27 | 27 |
| Day 22 | Nasopharyngeal | Positive | 31 | 30 |
| Day 30 | Nasopharyngeal | Positive | 31 | 33 |
| Day 30 | Endotracheal | Positive | 33 | ND |
| Day 42 | Nasopharyngeal | Positive | 28 | 28 |
| Day 50 | Nasopharyngeal | Negative | ND | ND |
| Day 57 | Nasopharyngeal | Negative | ND | ND |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kumar, V.H.S.; Prasath, A.; Blanco, C.; Kenney, P.O.; Ostwald, C.M.; Meyer, T.S.; Clementi, C.F.; Maciejewski, R.; Wilby, M.T.; Reynolds, A.M.; et al. Respiratory Failure in an Extremely Premature Neonate with COVID-19. Children 2021, 8, 477. https://doi.org/10.3390/children8060477
Kumar VHS, Prasath A, Blanco C, Kenney PO, Ostwald CM, Meyer TS, Clementi CF, Maciejewski R, Wilby MT, Reynolds AM, et al. Respiratory Failure in an Extremely Premature Neonate with COVID-19. Children. 2021; 8(6):477. https://doi.org/10.3390/children8060477
Chicago/Turabian StyleKumar, Vasantha H. S., Arun Prasath, Clariss Blanco, Patrick O. Kenney, Christina M. Ostwald, Tracy S. Meyer, Cara F. Clementi, Richard Maciejewski, Mark T. Wilby, Anne Marie Reynolds, and et al. 2021. "Respiratory Failure in an Extremely Premature Neonate with COVID-19" Children 8, no. 6: 477. https://doi.org/10.3390/children8060477
APA StyleKumar, V. H. S., Prasath, A., Blanco, C., Kenney, P. O., Ostwald, C. M., Meyer, T. S., Clementi, C. F., Maciejewski, R., Wilby, M. T., Reynolds, A. M., Hpa, N. J., & Yu, K. O. A. (2021). Respiratory Failure in an Extremely Premature Neonate with COVID-19. Children, 8(6), 477. https://doi.org/10.3390/children8060477