
Children’s Views and Experiences of Treatment Adherence and Parent/Child Co-Management in Eczema: A Qualitative Study

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
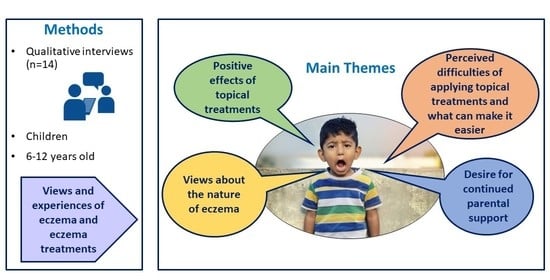
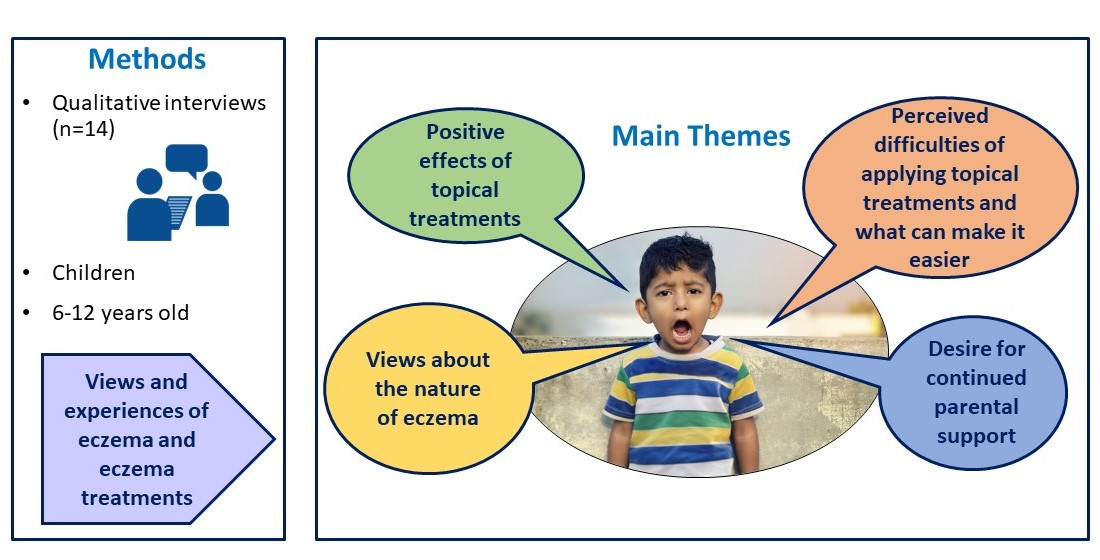
2.1. Study Design
2.2. Participants and Recruitment Procedures
2.3. Organising Qualitative Interviews
2.4. Conducting Qualitative Interviews with Child Participants
| About eczema |
|
| About eczema treatments |
|
| About eczema information |
|



2.5. Data Analysis
2.6. Reflexivity
3. Results
3.1. Participant Characteristics
3.2. Key Themes
3.2.1. Views about the Nature of Eczema
- “Eczema is like on/off, on/off”
“Parent: I would say rather than it being a cycle that’s repeated, it’s more dependent on the weather.C11: No. No, it’s a straight line.Interviewer: What did you mean by ‘it’s a line’?C11: That it doesn’t happen every single day, so it’s a new line. It’s a new time.”(C11, 6-year-old girl, mild eczema)
“It keeps going up and down, so it has its times. It’s either the back of my knees because it’s quite sweaty and it’s quite itchy and everything, it doesn’t crack up like my hands and feet does, it’s just like little bits. So, it’s just quite flaky underneath, but then just sometimes underneath my knees flare up a lot, but then my hands get a lot better. So, it’s like on/off, on/off.”(C13, 12-year-old boy, moderate eczema)
- “I want to find a solution to make my eczema go away”
“Some of my friends are saying that some of their relatives are having eczema, and just talking all about them, and saying that their eczema has gone away. Then that makes me feel kind of bad because some people’s eczema has gone away and mine hasn’t.”(C6, 8-year-old girl, severe eczema)
“I would like to find a solution to put it all away, but that’s probably not going to happen, but it would be nice to have it gone. I’ve heard people saying they grow out of it, but I haven’t had that.”(C13, 12-year-old boy, moderate eczema)
“It’s not too bad if you use the right cream and if you look after your eczema then it doesn’t really affect you much but if you don’t do anything about it then it can get worse.”(C9, 12-year-old girl, moderate eczema)
“Most nights I was staying up all night, trying to slow down the sweating and everything. Now it’s been only one night every month or something, so it’s been a lot better. I think now it’s just because I’ve been taking care of myself a lot better. I’m bigger, I can look after myself a lot more now”(C13, 12-year-old boy, moderate eczema)
- “Things that make my eczema worse”
“In the daytime, if it’s really hot…sometimes, it starts to get a rash down my arms and it starts to itch a bit more, so I just go inside and get cold water, piece of paper towel on it. Then it starts to ease up a bit more”(C12, 11-year-old boy, moderate eczema)
“It just becomes itchy whenever it wants. It has a mind of its own. It’s normally more like on the weekends when it’s really sunny and I’ve spent quite a lot of time on the trampoline.”(C3, 9-year-old girl, mild eczema)
3.2.2. Positive Effects of Topical Treatments
- “My creams soothe the itch and pain”
“Kind of annoying because it gets in the way and kind of disturbs you when you’re trying to get to sleep, but it does get better when I just treat it and things like that, like once I put my—bought some cream and it feels better once I put that on.”(C5, 9-year-old girl, mild eczema)
“Dry skin… it always itches all the time…I don’t like it…Itching it, but it’s really hard to stop itching it because in bed I scratch my feet sometimes, and then if I see scratches on them, and then when I put it [emollient] on it goes away…It helps—it helps your eczema and your dry skin.”(C4, 7-year-old boy, moderate eczema)
“C11: It basically stops me scratching when I have the cream on.Parent: Is that because it reminds you that you shouldn’t scratch?C11: No, I can’t scratch because it’s too slippery.”(C11, 6-year-old girl, mild eczema)
“I feel happy and it’s helping me and then, when you go to bed or you’re awake, you don’t scratch that much because you have cream on it and when you have cream on it, you might not like the feel of the cream, so you stop itching it until the cream dries in.”(C14, 7-year-old girl, severe eczema)
3.2.3. Perceived Difficulties of Applying Topical Treatments and What Can Make It Easier
- “I find it difficult applying creams at school”
“Because I don’t use it anywhere else than my house I don’t mind. If I had to use it at school or something I wouldn’t want to use it… I don’t really like to use this one as much because it takes quite a long time to soak and because I normally wear trousers or shorts to school I can’t really get it there.”(C1, 8-year-old girl, severe eczema)
“Sometimes bring cream down with me and we keep it in the [school] office and then I go and put it on when I need it… It’s okay but it kind of is—gets in the way of me missing out parts of my lessons.”(C5, 9-year-old girl, mild eczema)
“I get to school, I go into my classroom, then I sit down at my table and then I—and then we take the register. Then I start to get itchy so then I open the cupboard, sit down and put my cream on. Then I get back to my table. Because I sit right near the medical cupboard, I just get—I get my cream and I put it on wherever it’s itchy I normally just hide behind my table…I normally just go down here. Nobody can see me.”(C3, 9-year-old girl, mild eczema)
“I just start doing my work and then it makes me distracted and then I don’t feel like I’ve got to scratch.”(C14, 7-year-old girl, severe eczema)
“I sometimes—like at school I put my cardigan on so I can’t [scratch]… It’s more itchy when it’s really hot, because like in my classroom it’s really hot. It’s more—it doesn’t happen when I’m cool, and my gym’s really cool.”(C3, 9-year-old girl, mild eczema)
“It feels quite dry sometimes, and sometimes I’m really itchy at school, and the carpet sometimes makes my legs quite itchy. I tell my teacher, but she says that I should tell her later, so she doesn’t really help…To stop myself from itching, that’s very hard.”(C6, 8-year-old girl, severe eczema)
“If I’m on the other side of the room and I need to go up and get my cream, nobody looks at me then; it’s only after swimming when people look at me. After swimming at school they ask me; why do I have to put my cream on? I just find it really annoying… I don’t really like to put it on in front of people, but I kind of have to.”(C3, 9-year-old girl, mild eczema)
- “Putting on creams is frustrating and slow”
“Sometimes you just forget. It might be not having the time because we had lots of summer exams so we had to do lots of revision so I barely had any time.”(C9, 12-year-old girl, moderate eczema)
“I’d probably want to wait for the [emollient] kind of cream to soak in first and then put on sun cream but in the mornings I often don’t have time for that so I just want to put on one and go.”(C1, 8-year-old girl, severe eczema)
“It’s quite greasy, so it’s hard to work with iPads, TV remotes and everything like that …the cream doesn’t go straight after you’ve rubbed it in. So if you touch it, it’s all greasy and everything….it takes a good 10, 15 min to dry off, so it’s quite annoying.”(C13, 12-year-old boy, moderate eczema)
- “I don’t like how the cream feels on my skin”
“That one’s okay because it’s not so thick, but that one [emollient ointment]…I stick to things sometimes…If I’m just like in my pants and like someone’s doing my cream, it’s like I stick to the towel.”(C1, 8-year-old girl, severe eczema)
“C8: I just didn’t like the feel of it on my arms; it was quite heavy and greasy.Interviewer: What about the other cream that you liked?C8: It was nice and light, isn’t it?”(C8, 12-year-old boy, moderate eczema)
“I like that [steroid cream] helps my eczema, but sometimes it’s quite stingy when I put it on, and then sometimes I rub it off because it’s quite itchy.”(C6, 8-year-old girl, severe eczema)
- “Making treatment times easier”
“Dad gets the [emollient] and my [topical corticosteroid] and just gives me a massage into all the other places. I get special treatment every night!… It becomes one of those things at night, a massage parlour. He lies down, hands one after the other. Totally pampered.”(C12, 11-year-old boy, moderate eczema)
“I do know more what to do now than when I was six or something, because now I’ve actually got into the routine of it so I know how to do it all.”(C13, 12-year-old boy, moderate eczema)
“I just put it in my room so when I wake up I can see it and then it just sort of reminds me”(C4, 7-year-old boy, moderate eczema)
3.2.4. Desire for Continued Parental Support with Eczema Management
- “Sometimes I feel able to put my own cream on”
“Usually when I’m itching my arms Mum tells me to go put it on. The rest of the time I usually forget.”(C4, 7-year-old boy, moderate eczema)
“When it starts to flake up and it’s getting more dry skin underneath my nose, then mum just realises, and she says just to put some cream on.”(C12, 11-year-old boy, moderate eczema)
“My mum helps me with my back because I can’t reach my back so… I remember when she was doing it when I was in Year 1, but from Year 2 onwards I did it on my own….I put this on my whole body before I go to school, because that sometimes stops me itching as much. Sometimes, not all the time because I am known as the scratcher because I always scratch! My mum does my back, but I do everything else.”(C3, 9-year-old girl, mild eczema)
- “I can do it when I want to”
“I know what cream I can use, and I don’t have to wait for Mummy to be free.”(C6, 8-year-old girl, severe eczema)
“It’s better because you haven’t got a certain time to do it. So when you’ve got some spare time, you can actually do it then, rather than stopping doing something you want to do…Mum says right, it’s got to be done by a certain time, so that gives me time to finish what I’m doing and then I can do it.”(C13, 12-year-old boy, moderate eczema)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Weidinger, S.; Novak, N. Atopic dermatitis. Lancet 2016, 387, 1109–1122. [Google Scholar] [CrossRef]
- Zuberbier, T.; Orlow, S.J.; Paller, A.S.; Taïeb, A.; Allen, R.; Hernanz-Hermosa, J.M.; Ocampo-Candiani, J.; Cox, M.; Langeraar, J.; Simon, J.C. Patient perspectives on the management of atopic dermatitis. J. Allergy Clin. Immunol. 2006, 118, 226–232. [Google Scholar] [CrossRef] [PubMed]
- Williams, H.; Stewart, A.; von Mutius, E.; Cookson, W.; Anderson, H.R.; Asthma, I.S. Is eczema really on the increase worldwide? J. Allergy Clin. Immunol. 2008, 121, 947–954.e15. [Google Scholar] [CrossRef] [PubMed]
- Chamlin, S.L. The psychosocial burden of childhood atopic dermatitis. Dermatol. Ther. 2006, 19, 104–107. [Google Scholar] [CrossRef]
- Chamlin, S.L.; Frieden, I.J.; Williams, M.L.; Chren, M.M. Effects of atopic dermatitis on young American children and their families. Pediatrics 2004, 114, 607–611. [Google Scholar] [CrossRef] [PubMed]
- Abuabara, K.; Margolis, D.J. Do children really outgrow their eczema, or is there more than one eczema? J. Allergy Clin. Immunol. 2013, 132, 1139–1140. [Google Scholar] [CrossRef] [PubMed]
- Langan, S.M.; Irvine, A.D.; Weidinger, S. Atopic dermatitis. Lancet 2020, 396, 345–360. [Google Scholar] [CrossRef]
- NICE. Atopic eczema in under 12s: Diagnosis and managemen. In Excellence NNIfHaC; NICE: London, UK, 2007. [Google Scholar]
- Krejci-Manwaring, J.; Tusa, M.G.; Carroll, C.; Camacho, F.; Kaur, M.; Carr, D.; Fleischer Jr, A.B.; Balkrishnan, R.; Feldman, S.R. Stealth monitoring of adherence to topical medication: Adherence is very poor in children with atopic dermatitis. J. Am. Acad. Dermatol. 2007, 56, 211–216. [Google Scholar] [CrossRef] [PubMed]
- Leventhal, H.; Diefenbach, M.; Leventhal, E.A. Illness cognition: Using common sense to understand treatment adherence and affect cognition interactions. Cogn. Ther. Res. 1992, 16, 143–163. [Google Scholar] [CrossRef]
- Horne, R.; Weinman, J. Self-regulation and self-management in asthma: Exploring the role of illness perceptions and treatment beliefs in explaining non-adherence to preventer medication. Psychol. Health 2002, 17, 17–32. [Google Scholar] [CrossRef]
- Horne, R.; Chapman, S.C.; Parham, R.; Freemantle, N.; Forbes, A.; Cooper, V. Understanding patients’ adherence-related beliefs about medicines prescribed for long-term conditions: A meta-analytic review of the Necessity-Concerns Framework. PLoS ONE 2013, 8, e80633. [Google Scholar] [CrossRef]
- Walker, C.; Papadopoulos, L.; Hussein, M. Paediatric eczema and psychosocial morbidity: How does eczema interact with parents’ illness beliefs? J. Eur. Acad. Dermatol. Venereol. 2007, 21, 63–67. [Google Scholar] [CrossRef] [PubMed]
- Walker, C.; Papadopoulos, L.; Lipton, M.; Hussein, M. The importance of children’s illness beliefs: The Children’s Illness Perception Questionnaire (CIPQ) as a reliable assessment tool for eczema and asthma. Psychol. Health Med. 2006, 11, 100–107. [Google Scholar] [CrossRef]
- Capozza, K.; Schwartz, A. Does it work and is it safe? Parents’ perspectives on adherence to medication for atopic dermatitis. Pediatr. Dermatol. 2019, 37, 58–61. [Google Scholar] [CrossRef] [PubMed]
- Ellis, R.M.; Koch, L.H.; McGuire, E.; Williams, J.V. Potential barriers to adherence in pediatric dermatology. Pediatr. Dermatol. 2011, 28, 242–244. [Google Scholar] [CrossRef]
- Sokolova, A.; Smith, S.D. Factors contributing to poor treatment outcomes in childhood atopic dermatitis. Australas. J. Dermatol. 2015, 56, 252–257. [Google Scholar] [CrossRef] [PubMed]
- Teasdale, E.; Muller, I.; Sivyer, K.; Ghio, D.; Greenwell, K.; Wilczynska, S.; Roberts, A.; Ridd, M.J.; Francis, N.; Yardley, L.; et al. Views and experiences of managing eczema: Systematic review and thematic synthesis of qualitative studies. Br. J. Dermatol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Hanghøj, S.; Boisen, K.A. Self-reported barriers to medication adherence among chronically ill adolescents: A systematic review. J. Adolesc. Health 2014, 54, 121–138. [Google Scholar] [CrossRef] [PubMed]
- Holley, S.; Morris, R.; Knibb, R.; Latter, S.; Liossi, C.; Mitchell, F.; Roberts, G. Barriers and facilitators to asthma self-management in adolescents: A systematic review of qualitative and quantitative studies. Pediatr. Pulmonol. 2017, 52, 430–442. [Google Scholar] [CrossRef] [PubMed]
- KyngAs, H.A.; Kroll, T.; Duffy, M.E. Compliance in adolescents with chronic diseases: A review. J Adolesc Health 2000, 26, 379–388. [Google Scholar] [CrossRef] [PubMed]
- Iio, M.; Hamaguchi, M.; Nagata, M.; Yoshida, K. Stressors of School-age Children with Allergic Diseases: A Qualitative Study. J. Pediatr. Nurs. 2018, 42, e73–e78. [Google Scholar] [CrossRef] [PubMed]
- Roje, M.; Rezo, I.; Flander, G.B. Quality of life and psychosocial needs of children suffering from chronic skin diseases. Alcohol. Psychiatry Res. 2016, 52, 133–148. [Google Scholar] [CrossRef][Green Version]
- Xie, Q.-W.; Chan, C.L.-W.; Chan, C.H.-Y. The wounded self—lonely in a crowd: A qualitative study of the voices of children living with atopic dermatitis in Hong Kong. Health Soc. Care Community 2020, 28, 862–873. [Google Scholar] [CrossRef]
- Wake, E.V.; Batchelor, J.; Lawton, S.; Thomas, K.S.; Harrison, E.F.; Cowdell, F.C.; UK Dermatology Clinical Trials Network’s CLOTHES Trial Team Williams; Llewellyn, J.; Dean, T.; Grundy, J. The views of children and young people on the use of silk garments for the treatment of eczema: A nested qualitative study within the CLOTHing for the relief of Eczema Symptoms (CLOTHES) randomized controlled trial. Br. J. Dermatol. 2018, 178, 183–190. [Google Scholar] [CrossRef] [PubMed]
- Ghio, D.; Muller, I.; Greenwell, K.; Roberts, A.; McNiven, A.; Langan, S.M.; Santer, M. “It’s like the bad guy in a movie who just doesn’t die”: A qualitative exploration of young people’s adaptation to eczema and implications for self-care. Br. J. Dermatol. 2020, 182, 112–118. [Google Scholar] [CrossRef]
- Kosse, R.C.; Bouvy, M.L.; Daanen, M.; de Vries, T.W.; Koster, E.S. Adolescents, perspectives on atopic dermatitis treatment-experiences, preferences, and beliefs. JAMA Dermatol. 2018, 154, 824–827. [Google Scholar] [CrossRef]
- Wales, S.; Nadew, K.; Crisp, J. Parents’ and school-aged children’s views on managing treatment adherence in asthma or diabetes. Neonatal Paediatr. Child Health Nurs. 2007, 10, 26–30. [Google Scholar]
- Heath, G.; Farre, A.; Shaw, K. Parenting a child with chronic illness as they transition into adulthood: A systematic review and thematic synthesis of parents’ experiences. Patient Educ. Couns. 2017, 100, 76–92. [Google Scholar] [CrossRef] [PubMed]
- Sivyer, K.; Teasdale, E.; Greenwell, K.; Steele, M.; Ghio, D.; Ridd, M.J.; Roberts, A.; Chalmers, J.R.; Lawton, S.; Langan, S.M.; et al. Supporting parents and carers to manage and co-manage their child’s eczema: Intervention planning and optimisation for Eczema Care Online for Families. Manuscript in preparation.
- ECO. Eczema Care Online (ECO) Website 2020. Available online: https://www.nottingham.ac.uk/eco/ (accessed on 21 November 2020).
- England. PH. National General Practice Profiles 2018. Available online: https://fingertips.phe.org.uk/profile/general-practice/data (accessed on 14 January 2018).
- Hagger, M.S.; Orbell, S. A Meta-Analytic Review of the Common-Sense Model of Illness Representations. Psychol. Health 2003, 18, 141–184. [Google Scholar] [CrossRef]
- Docherty, S.; Sandelowski, M. Focus on qualitative methods: Interviewing children. Res. Nurs. Health 1999, 22, 177–185. [Google Scholar] [CrossRef]
- Madden, L.; Shilling, V.; Woolfall, K.; Sowden, E.; Smyth, R.L.; Williamson, P.R.; Young, B. Questioning assent: How are children’s views included as families make decisions about clinical trials? Child CareHealth Dev. 2016, 42, 900–908. [Google Scholar] [CrossRef] [PubMed]
- Clark, A.; Moss, P. Listening to Young Children: The Mosaic Approach; Jessica Kingsley Publishers: London, UK, 2011. [Google Scholar]
- Kellett, M. Empowering children and young people as researchers: Overcoming barriers and building capacity. Child Indic. Res. 2011, 4, 205–219. [Google Scholar] [CrossRef]
- Mandell, N. The least-adult role in studying children. J. Contemp. Ethnogr. 1988, 16, 433–467. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Ghio, D.; Greenwell, K.; Muller, I.; Roberts, A.; McNiven, A.; Santer, M. Psychosocial needs of adolescents and young adults with eczema: A secondary analysis of qualitative data to inform a behaviour change intervention. Br. J. Health Psychol. 2021, 26, 214–231. [Google Scholar] [CrossRef] [PubMed]
- Alanne, S.; Laitinen, K.; Paavilainen, E. Living Ordinary Family Life with an Allergic Child—The Mother’s Perspective. J. Pediatr. Nurs. 2014, 29, 679–687. [Google Scholar] [CrossRef] [PubMed]
- Cheung, W.K.; Lee, R.L. Children and adolescents living with atopic eczema: An interpretive phenomenological study with Chinese mothers. J. Adv. Nurs. 2012, 68, 2247–2255. [Google Scholar] [CrossRef] [PubMed]
- Fenerty, S.D.; O’Neill, J.L.; Gustafson, C.J.; Feldman, S.R. Maternal adherence factors in the treatment of pediatric atopic dermatitis. JAMA Dermatol. 2013, 149, 229–231. [Google Scholar] [CrossRef]
- Powell, K.; Le Roux, E.; Banks, J.P.; Ridd, M.J. Developing a written action plan for children with eczema: A qualitative study. Br. J. Gen. Pract. 2018, 68, e81–e89. [Google Scholar] [CrossRef]
- Santer, M.; Burgess, H.; Yardley, L.; Ersser, S.J.; Lewis-Jones, S.; Muller, I.; Hugh, C.; Little, P. Managing childhood eczema: Qualitative study exploring carers’ experiences of barriers and facilitators to treatment adherence. J. Adv. Nurs. 2013, 69, 2493–2501. [Google Scholar] [CrossRef] [PubMed]
- Santer, M.; Muller, I.; Yardley, L.; Lewis-Jones, S.; Ersser, S.; Little, P. Parents’ and carers’ views about emollients for childhood eczema: Qualitative interview study. BMJ Open 2016, 6, e011887. [Google Scholar] [CrossRef] [PubMed]
- Teasdale, E.J.; Muller, I.; Santer, M. Carers’ views of topical corticosteroid use in childhood eczema: A qualitative study of online discussion forums. Br. J. Dermatol. 2017, 176, 1500–1507. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Veenje, S.; Osinga, H.; Antonescu, I.; Bos, B.; de Vries, T.W. Focus group parental opinions regarding treatment with topical corticosteroids on children with atopic dermatitis. Allergol. Immunopathol. 2018, 47, 166–171. [Google Scholar] [CrossRef] [PubMed]
- Pound, P.; Britten, N.; Morgan, M.; Yardley, L.; Pope, C.; Daker-White, G.; Campbell, R. Resisting medicines: A synthesis of qualitative studies of medicine taking. Soc. Sci. Med. 2005, 61, 133–155. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, B.C.; Harris, I.B.; Beckman, T.J.; Reed, D.A.; Cook, D.A. Standards for reporting qualitative research: A synthesis of recommendations. Acad. Med. 2014, 89, 1245–1251. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Number of Interviewees | |
|---|---|
| Child gender | |
| Female | 9 |
| Male | 5 |
| Child age | |
| 6 years | 2 |
| 7 years | 2 |
| 8 years | 2 |
| 9 years | 2 |
| 10 years | 2 |
| 11 years | 1 |
| 12 years | 3 |
| Eczema severity 1 | |
| mild | 5 |
| moderate | 6 |
| severe | 3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Teasdale, E.; Sivyer, K.; Muller, I.; Ghio, D.; Roberts, A.; Lawton, S.; Santer, M. Children’s Views and Experiences of Treatment Adherence and Parent/Child Co-Management in Eczema: A Qualitative Study. Children 2021, 8, 158. https://doi.org/10.3390/children8020158
Teasdale E, Sivyer K, Muller I, Ghio D, Roberts A, Lawton S, Santer M. Children’s Views and Experiences of Treatment Adherence and Parent/Child Co-Management in Eczema: A Qualitative Study. Children. 2021; 8(2):158. https://doi.org/10.3390/children8020158
Chicago/Turabian StyleTeasdale, Emma, Katy Sivyer, Ingrid Muller, Daniela Ghio, Amanda Roberts, Sandra Lawton, and Miriam Santer. 2021. "Children’s Views and Experiences of Treatment Adherence and Parent/Child Co-Management in Eczema: A Qualitative Study" Children 8, no. 2: 158. https://doi.org/10.3390/children8020158
APA StyleTeasdale, E., Sivyer, K., Muller, I., Ghio, D., Roberts, A., Lawton, S., & Santer, M. (2021). Children’s Views and Experiences of Treatment Adherence and Parent/Child Co-Management in Eczema: A Qualitative Study. Children, 8(2), 158. https://doi.org/10.3390/children8020158