
Variability of Prognostic Results Based on Biological Parameters in Sickle Cell Disease Cohort Studies in Children: What Should Clinicians Know?

Abstract
1. Introduction
2. Methods
2.1. Literature Search
2.2. Illustration of the Impact on Results of the Methods Selected
2.2.1. Study Population
2.2.2. Statistical Methodology
3. Results
3.1. Literature Search
3.2. Collection and Statistical Analyses of Biological Parameter in Cohort Studies
- −
- either once during the follow-up: either at a fixed age range (which depended on the study), or at the last follow-up;
- −
- or several times: either all values during the follow-up or at a fixed range of ages.
3.3. Illustration of the Impact on Results of the Methods Selected
 ), in green, when the square is to the left of the line and as a risk factor (
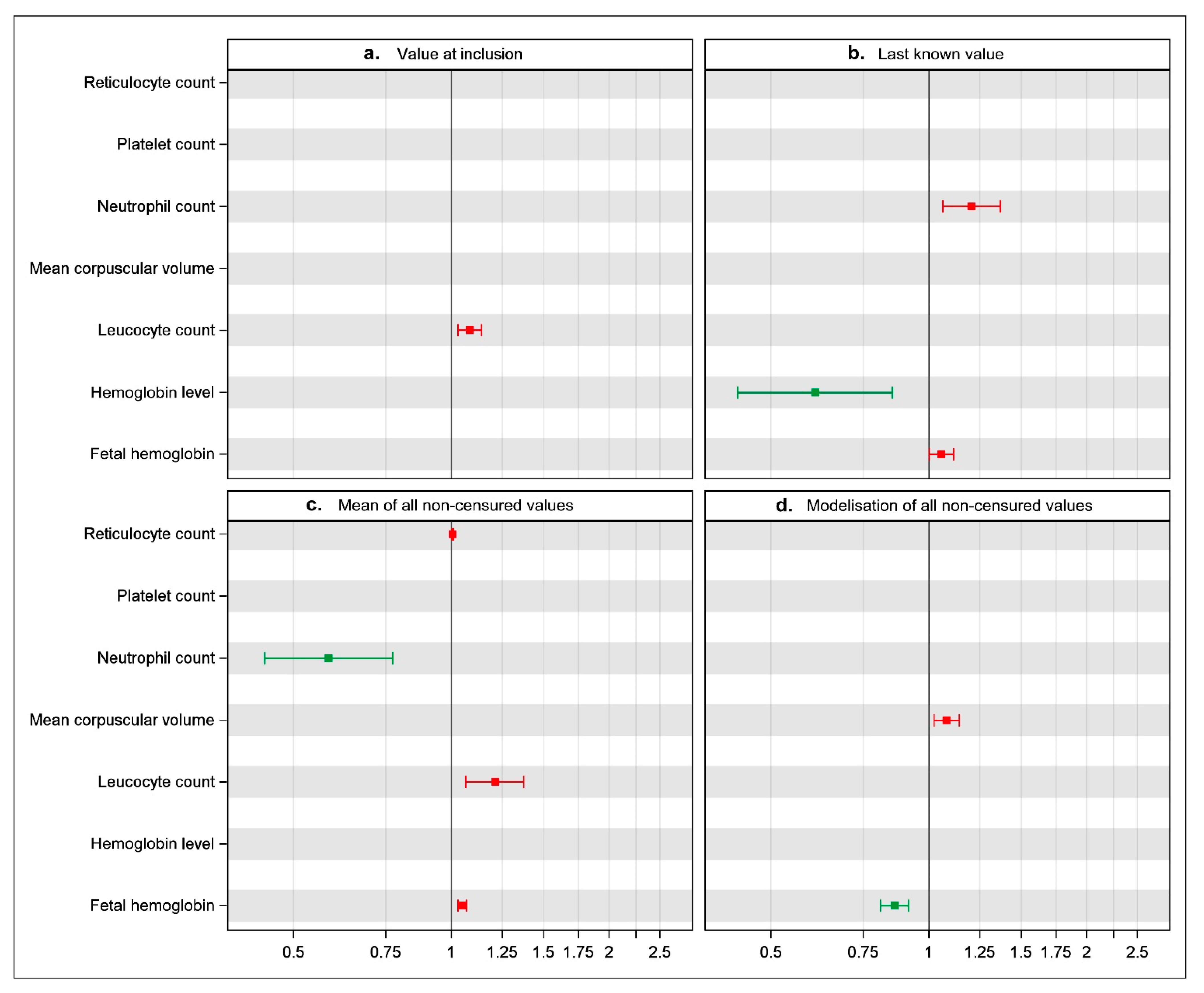
), in green, when the square is to the left of the line and as a risk factor ( ) in red when it is to the right. Stepwise selection is a statistical method in which statistically significant prognostic variables are selected using an automated procedure to build a multivariable model. When this procedure is applied, only variables with a 5% level of significance are captured.
) in red when it is to the right. Stepwise selection is a statistical method in which statistically significant prognostic variables are selected using an automated procedure to build a multivariable model. When this procedure is applied, only variables with a 5% level of significance are captured.- −
- If we considered the single value at the inclusion of the study (panel a), we found that only the leukocyte count was associated with a higher risk of CV (HR 1.11 (1.03–1.15)). The six other biological parameters were not associated with the occurrence of CV.
- −
- If we considered the single last known value (panel b), we found that only the neutrophil count and the HbF level were associated with a higher risk of CV (respectively, (HR 1.20 (1.07–1.35) and 1.13 (1.10–1.19))) whereas the hemoglobin level was inversely associated with the risk of CV (HR 0.62 (0.39–0.86)). The four other biological parameters were not found to be significantly associated with the occurrence of CV.
- −
- If we considered the mean of all non-censured values (panel c), we found that the neutrophil count was inversely associated with the occurrence of CV (HR 0.59 (0.27–0.79)), whereas the reticulocyte count, the leukocyte count and the HbF level were associated with a higher risk of CV (respectively, (HR 1.02 (1.01–1.03)), (HR 1.22 (1.07–1.36)) and (HR 1.08 (1.04–1.10))). The three other biological parameters were not found to be significantly associated with the occurrence of CV.
- −
- Last, if we performed a modelization of all non-censured values (panel d), we found this time the mean corpuscular volume to be associated with the occurrence of CV (HR 1.08 (1.02–1.15)), whereas the HbF level was inversely associated with risk of CV (HR 0.87 (0.82–0.92)). The five other biological parameters were not found to be significantly correlated with the occurrence of CV.
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rees, D.C.; Gibson, J.S. Biomarkers in sickle cell disease. Br. J. Haematol. 2012, 156, 433–445. [Google Scholar] [CrossRef]
- Platt, O.S.; Brambilla, D.J.; Rosse, W.F.; Milner, P.F.; Castro, O.; Steinberg, M.H.; Klug, P.P. Mortality in sickle cell disease. Life expectancy and risk factors for early death. N. Engl. J. Med. 1994, 330, 1639–1644. [Google Scholar] [CrossRef] [PubMed]
- Platt, O.S.; Thorington, B.D.; Brambilla, D.J.; Milner, P.F.; Rosse, W.F.; Vichinsky, E.; Kinney, T.R. Pain in sickle cell disease. Rates and risk factors. N. Engl. J. Med. 1991, 325, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Miller, S.T.; Sleeper, L.A.; Pegelow, C.H.; Enos, L.E.; Wang, W.C.; Weiner, S.J.; Wethers, D.L.; Smith, J.; Kinney, T.R. Prediction of adverse outcomes in children with sickle cell disease. N. Engl. J. Med. 2000, 342, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Castro, O.; Brambilla, D.J.; Thorington, B.; Reindorf, C.A.; Scott, R.B.; Gillette, P.; Vera, J.C.; Levy, P.S. The acute chest syndrome in sickle cell disease: Incidence and risk factors. The Cooperative Study of Sickle Cell Disease. Blood 1994, 84, 643–649. [Google Scholar] [CrossRef]
- Bernaudin, F.; Verlhac, S.; Arnaud, C.; Kamdem, A.; Chevret, S.; Hau, I.; Coïc, L.; Leveillé, E.; LeMarchand, E.; Lesprit, E.; et al. Impact of early transcranial Doppler screening and intensive therapy on cerebral vasculopathy outcome in a newborn sickle cell anemia cohort. Blood 2011, 117, 1130–1140, quiz 1436. [Google Scholar] [CrossRef] [PubMed]
- Ohene-Frempong, K.; Weiner, S.J.; Sleeper, L.A.; Miller, S.T.; Embury, S.; Moohr, J.W.; Wethers, D.L.; Pegelow, C.H.; Gill, F.M. Cerebrovascular accidents in sickle cell disease: Rates and risk factors. Blood 1998, 91, 288–294. [Google Scholar]
- Kato, G.J.; Wang, Z.; Machado, R.F.; Blackwelder, W.C.; Vi, J.G.T.; Hazen, S.L. Endogenous nitric oxide synthase inhibitors in sickle cell disease: Abnormal levels and correlations with pulmonary hypertension, desaturation, haemolysis, organ dysfunction and death. Br. J. Haematol. 2009, 145, 506–513. [Google Scholar] [CrossRef] [PubMed]
- Sommet, J.; Alberti, C.; Couque, N.; Verlhac, S.; Haouari, Z.; Mohamed, D.; François, M.; Missud, F.; Holvoet, L.; Elmaleh-Bergès, M.; et al. Clinical and haematological risk factors for cerebral macrovasculopathy in a sickle cell disease newborn cohort: A prospective study. Br. J. Haematol. 2016, 172, 966–977. [Google Scholar] [CrossRef] [PubMed]
- Bernaudin, F.; Verlhac, S.; Chevret, S.; Torres, M.; Coic, L.; Arnaud, C.; Kamdem, A.; Hau, I.; Neonato, M.G.; Delacourt, C. G6PD deficiency, absence of alpha-thalassemia, and hemolytic rate at baseline are significant independent risk factors for abnormally high cerebral velocities in patients with sickle cell anemia. Blood 2008, 112, 4314–4317. [Google Scholar] [CrossRef]
- Meier, E.R.; Fasano, R.M.; Estrada, M.; He, J.; Luban, N.L.; McCarter, R. Early Reticulocytosis and Anemia Are Associated with Abnormal and Conditional Transcranial Doppler Velocities in Children with Sickle Cell Anemia. J. Pediatr. 2016, 169, 227–231.e1. [Google Scholar] [CrossRef] [PubMed]
- Hankins, J.S.; McCarville, M.B.; Rankine-Mullings, A.; Reid, M.E.; Lobo, C.L.; Moura, P.G.; Ali, S.; Soares, D.P.; Aldred, K.; Jay, D.W.; et al. Prevention of conversion to abnormal transcranial Doppler with hydroxyurea in sickle cell anemia: A Phase III international randomized clinical trial. Am. J. Hematol. 2015, 90, 1099–1105. [Google Scholar] [CrossRef] [PubMed]
- Tsiatis, A.A.; DeGruttola, V.; Wulfsohn, M.S. Modeling the relationship of survival to longitudinal data measured with error. Applications to survival and CD4 counts in patients with AIDS. J. Am. Stat. Assoc. 1995, 90, 27–37. [Google Scholar] [CrossRef]
- Diggle, P.J.; Sousa, I.; Chetwynd, A.G. Joint modelling of repeated measurements and time-to-event outcomes: The fourth Armitage lecture. Stat. Med. 2008, 27, 2981–2998. [Google Scholar] [CrossRef] [PubMed]
- Curtis, S.A.; Danda, N.; Etzion, Z.; Cohen, H.W.; Billett, H.H. Longitudinal Analysis of Patient Specific Predictors for Mortality in Sickle Cell Disease. PLoS ONE 2016, 11, e0164743. [Google Scholar] [CrossRef] [PubMed]
- Maitra, P.; Caughey, M.; Robinson, L.; Desai, P.C.; Jones, S.; Nouraie, M.; Gladwin, M.T.; Hinderliter, A.; Cai, J.; Ataga, K.I. Risk factors for mortality in adult patients with sickle cell disease: A meta-analysis of studies in North America and Europe. Haematologica 2017, 102, 626–636. [Google Scholar] [CrossRef]
- Bailey, K.; Morris, J.S.; Thomas, P.; Serjeant, G.R. Fetal haemoglobin and early manifestations of homozygous sickle cell disease. Arch. Dis. Child. 1992, 67, 517–520. [Google Scholar] [CrossRef][Green Version]
- Estepp, J.H.; Smeltzer, M.P.; Kang, G.; Li, C.; Wang, W.C.; Abrams, C.; Aygun, B.; Ware, R.E.; Nottage, K.; Hankins, J.S. A Clinically Meaningful Fetal Hemoglobin Threshold for Children with Sickle Cell Anemia During Hydroxyurea Therapy. Am. J. Hematol. 2017, 92, 1333–1339. [Google Scholar] [CrossRef]
- Koshy, M.; Entsuah, R.; Koranda, A.; Kraus, A.P.; Johnson, R.; Bellvue, R.; Flournoy-Gill, Z.; Levy, P. Leg ulcers in patients with sickle cell disease. Blood 1989, 74, 1403–1408. [Google Scholar] [CrossRef]
- Nolan, V.G.; Adewoye, A.H.; Baldwin, C.T.; Wang, L.; Ma, Q.; Wyszynski, D.F.; Farrell, J.J.; Sebastiani, P.; Farrer, L.A.; Steinberg, M.H. Sickle cell leg ulcers: Associations with haemolysis and SNPs in Klotho, TEK and genes of the TGF-beta/BMP pathway. Br. J. Haematol. 2006, 133, 570–578. [Google Scholar] [CrossRef]
- Dallman, P.R.; Siimes, M.A. Percentile curves for hemoglobin and red cell volume in infancy and childhood. J. Pediatr. 1979, 94, 26–31. [Google Scholar] [CrossRef]
- Swaanenburg, J.C.; Rutten, W.P.; Holdrinet, A.C.; van Strik, R. The determination of reference values for hematologic parameters using results obtained from patient populations. Am. J. Clin. Pathol. 1987, 88, 182–191. [Google Scholar] [CrossRef]
- WHO Multicentre Growth Reference Study Group. WHO Child Growth Standards based on length/height, weight and age. Acta Paediatr. Oslo Nor. 1992, 450 (Suppl 2006), 76–85. [Google Scholar] [CrossRef]
- Thiébaut, R.; Chêne, G.; Jacqmin-Gadda, H.; Morlat, P.; Mercié, P.; Dupon, M.; Neau, D.; Ramaroson, H.; Dabis, F.; Salamon, R.; et al. Time-updated CD4+ T lymphocyte count and HIV RNA as major markers of disease progression in naive HIV-1-infected patients treated with a highly active antiretroviral therapy: The Aquitaine cohort, 1996–2001. J. Acquir. Immune Defic. Syndr. 1999, 33, 380–386. [Google Scholar] [CrossRef]
- Dafni, U.G.; Tsiatis, A.A. Evaluating surrogate markers of clinical outcome when measured with error. Biometrics 1998, 54, 1445–1462. [Google Scholar] [CrossRef] [PubMed]
- Bycott, P.; Taylor, J. A comparison of smoothing techniques for CD4 data measured with error in a time-dependent Cox proportional hazards model. Stat. Med. 1998, 17, 2061–2077. [Google Scholar] [CrossRef]
- Ibrahim, J.G.; Chu, H.; Chen, L.M. Basic concepts and methods for joint models of longitudinal and survival data. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2010, 28, 2796–2801. [Google Scholar] [CrossRef]
- Andrinopoulou, E.-R.; Rizopoulos, D.; Jin, R.; Bogers, A.J.J.C.; Lesaffre, E.; Takkenberg, J.J.M. An introduction to mixed models and joint modeling: Analysis of valve function over time. Ann. Thorac. Surg. 2012, 93, 1765–1772. [Google Scholar] [CrossRef] [PubMed]
- Garre, F.G.; Zwinderman, A.H.; Geskus, R.B.; Sijpkens, Y.W.J.; van Leven, T.K. A joint latent class changepoint model to improve the prediction of time to graft failure. Front. Public Health 2008, 171, 299–308. [Google Scholar] [CrossRef]
- Daher-Abdi, Z.; Essig, M.; Rizopoulos, D.; Le Meur, Y.; Prémaud, A.; Woillard, J.-B.; Rerolle, J.-P.; Marquet, P.; Rousseau, A. Impact of longitudinal exposure to mycophenolic acid on acute rejection in renal-transplant recipients using a joint modeling approach. Pharmacol. Res. 2013, 72, 52–60. [Google Scholar] [CrossRef] [PubMed]
- Ioannidis, J.P.A.; Greenland, S.; Hlatky, M.A.; Khoury, M.J.; MacLeod, M.R.; Moher, D.; Schulz, K.F.; Tibshirani, R. Increasing value and reducing waste in research design, conduct, and analysis. Lancet Lond. Engl. 2014, 383, 166–175. [Google Scholar] [CrossRef]
- Altman, D.G.; Moher, D. Importance of Transparent Reporting on Health Research. In Guidelines for Reporting Health Research: A User’s Manual, 1st ed.; John Wiley & Sons: Hoboken, NJ, USA, 2014. [Google Scholar]


{kind=link}
| N = 16 | |
|---|---|
| Region | |
| North America | 8 |
| Europe | 7 |
| Africa | 1 |
| SCD clinical event studied | |
| Neurological complications * | 10 |
| Vaso-occlusive crises | 2 |
| Acute chest syndrome | 1 |
| Nutrition and growth | 2 |
| Pulmonary arterial hypertension | 1 |
| Alloimmunization | 1 |
| Retinopathy | 1 |
| Hemolysis | 1 |
| Mortality | 1 |
| Number of included patients (n = 16) | |
| Median (Q1; Q3) | 184 (102; 376) |
| (Min-Max) | (24; 1041) |
| Age at study inclusion (years) (n = 9) | |
| Median (Q1; Q3) | 2.3 (0.8; 11.8) |
| (Min-Max) | (0.3; 17.0) |
| Follow-up in years (n = 10) | |
| Median (Q1; Q3) | 6.0 (2.0; 11.5) |
| (Min-Max) | (2.5; 6.7) |
| Laboratory Parameter | Hemoglobin | Reticulocyte Count | Leukocyte Count | Fetal Hemoglobin | ||||
|---|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | n | % | |
| Methods used for data collection | 16 | 14 | 14 | 11 | ||||
| One value per patient | 7 | (44) | 7 | (50) | 6 | (43) | 5 | (46) |
| At fixed age | 7 | 6 | 6 | 4 | ||||
| Last known value | 0 | 1 | 0 | 1 | ||||
| Several values per patient | 6 | (37) | 5 | (36) | 6 | (43) | 4 | (36) |
| All values during follow-up | 3 | 3 | 3 | 2 | ||||
| Values measured at fixed range of age | 3 | 2 | 3 | 2 | ||||
| NR | 3 | (19) | 2 | (14) | 2 | (14) | 2 | (18) |
| Methods used for data modelling | 15 | 13 | 12 | 11 | ||||
| One value per patient * | 8 | (53) | 8 | (61) | 5 | (42) | 5 | (45) |
| Several values per patient | 5 | (33) | 4 | (31) | 5 | (42) | 4 | (36) |
| 1 | ||||||||
| - Values were summarized as means ** | 4 | 3 | 4 | 3 | ||||
| - All values were modelled *** | 1 | 1 | 1 | 1 | ||||
| NR | 2 | (13) | 1 | (8) | 2 | (16) | 2 | (18) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sommet, J.; Roux, E.L.; Koehl, B.; Haouari, Z.; Mohamed, D.; Baruchel, A.; Benkerrou, M.; Alberti, C. Variability of Prognostic Results Based on Biological Parameters in Sickle Cell Disease Cohort Studies in Children: What Should Clinicians Know? Children 2021, 8, 143. https://doi.org/10.3390/children8020143
Sommet J, Roux EL, Koehl B, Haouari Z, Mohamed D, Baruchel A, Benkerrou M, Alberti C. Variability of Prognostic Results Based on Biological Parameters in Sickle Cell Disease Cohort Studies in Children: What Should Clinicians Know? Children. 2021; 8(2):143. https://doi.org/10.3390/children8020143
Chicago/Turabian StyleSommet, Julie, Enora Le Roux, Bérengère Koehl, Zinedine Haouari, Damir Mohamed, André Baruchel, Malika Benkerrou, and Corinne Alberti. 2021. "Variability of Prognostic Results Based on Biological Parameters in Sickle Cell Disease Cohort Studies in Children: What Should Clinicians Know?" Children 8, no. 2: 143. https://doi.org/10.3390/children8020143
APA StyleSommet, J., Roux, E. L., Koehl, B., Haouari, Z., Mohamed, D., Baruchel, A., Benkerrou, M., & Alberti, C. (2021). Variability of Prognostic Results Based on Biological Parameters in Sickle Cell Disease Cohort Studies in Children: What Should Clinicians Know? Children, 8(2), 143. https://doi.org/10.3390/children8020143