Improved Survival of Periviable Infants after Alteration of the Threshold of Viability by the Neonatal Resuscitation Program 2015

 , ,
, ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
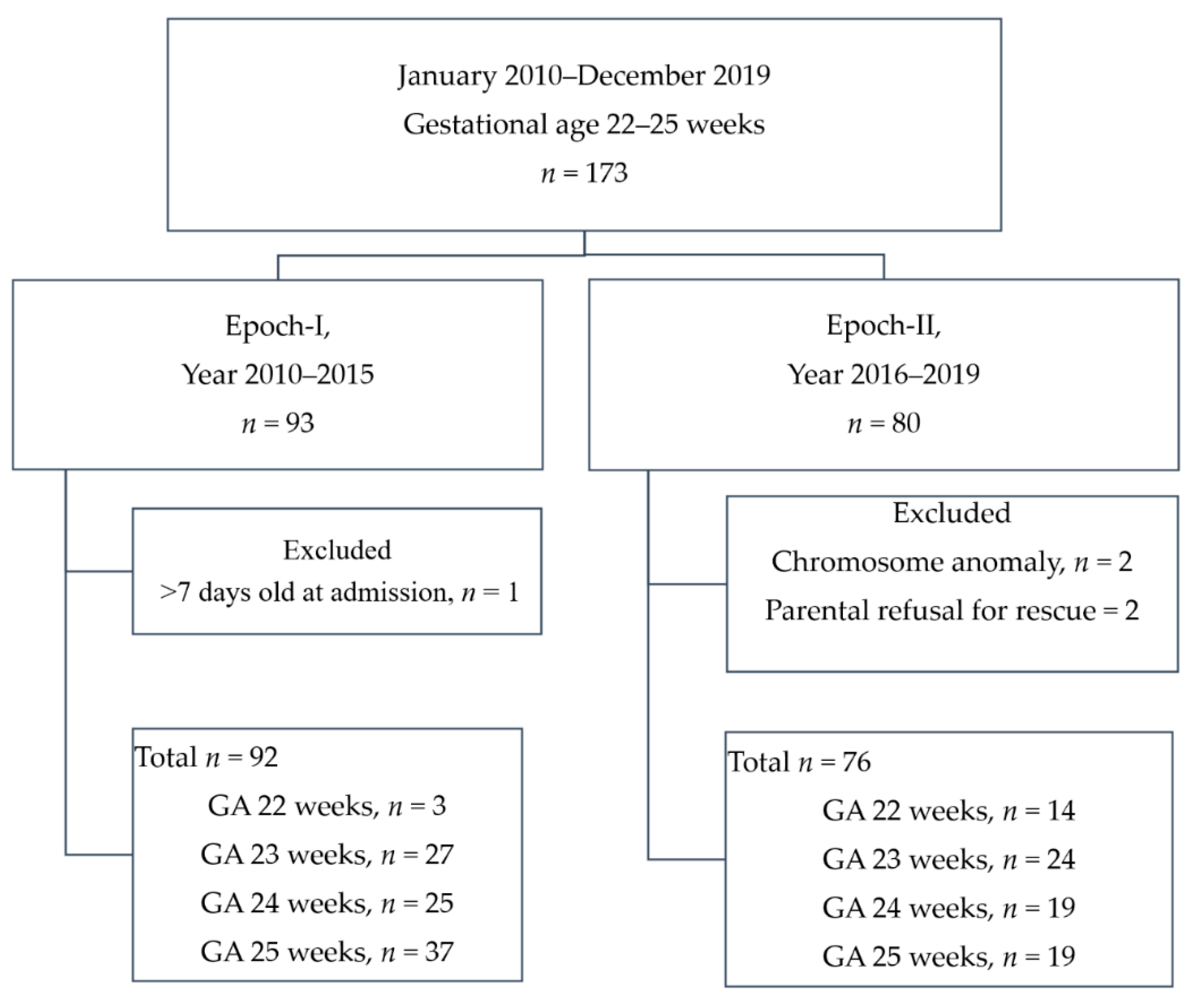
2.1. Study Design
2.2. Study Setting and Care Policies
2.2.1. Antenatal Counseling
2.2.2. Perinatal Management
2.2.3. Respiratory Management
2.2.4. Nutrition Management
2.2.5. Infection Control and Other Management
2.2.6. Discharge Policy and Post-Discharge Follow-Up Program
2.3. The Primary Outcome and Variable Definitions
2.4. Statistics Analysis
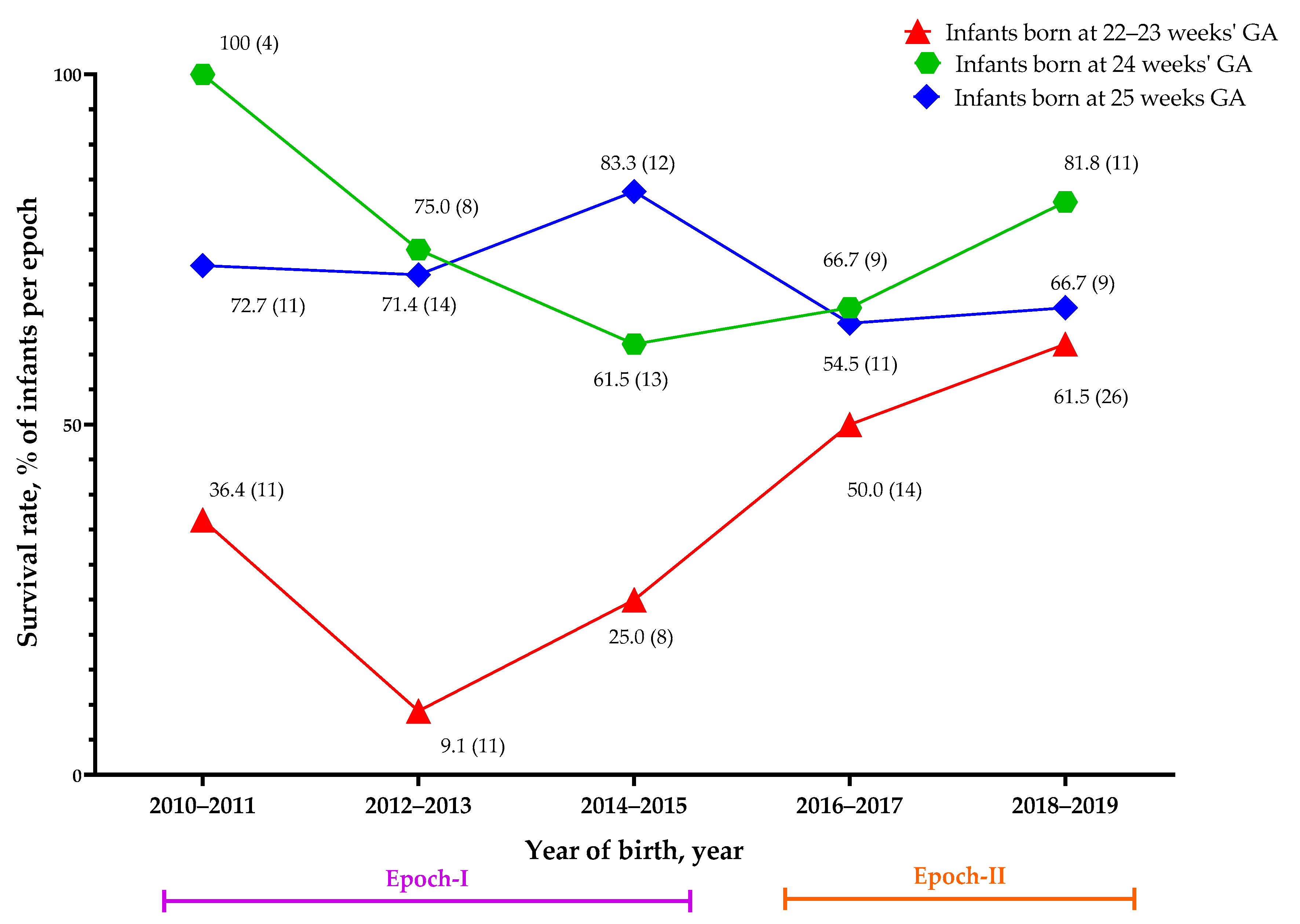
3. Results
4. Discussion
4.1. Survival Rate of Periviable Infants
4.2. Law, Guidelines, and the Debate of Ethics
4.3. Risk or Potential Factors Related to the Survival of Periviable Infants
4.4. Limitations and Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Barrington, K.J. Management during the first 72 h of age of the periviable infant: An evidence-based review. Semin. Perinatol. 2014, 38, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Patel, R.M.; Rysavy, M.A.; Bell, E.F.; Tyson, J.E. Survival of infants born at periviable gestational ages. Clin. Perinatol. 2017, 44, 287–303. [Google Scholar] [CrossRef] [PubMed]
- Falciglia, H.S.; Merkel, R.C.; Glover, V.; Hasselfeld, K.A.; Brady, W.K. The mortality of periviable and extremely premature infants and their impact on the overall neonatal mortality rate. Sci. Rep. 2020, 10, 2503. [Google Scholar] [CrossRef] [PubMed]
- American College of Obstetricians and Gynecologists; Society for Maternal-Fetal Medicine. Obstetric Care consensus No. 6: Periviable Birth. Obstet. Gynecol. 2017, 130, e187–e199. [Google Scholar] [CrossRef] [PubMed]
- American College of Obstetricians and Gynecologists and the Society for Maternal-Fetal Medicine; Ecker, J.L.; Kaimal, A.; Mercer, B.M.; Blackwell, S.C.; de Regnier, R.A.O.; Farrell, R.M.; Grobman, W.A.; Resnik, J.L.; Sciscione, A.C. #3: Periviable birth. Am. J. Obstet. Gynecol. 2015, 213, 604–614. [Google Scholar] [CrossRef]
- Raju, T.N.; Mercer, B.M.; Burchfield, D.J.; Joseph, G.F. Periviable birth: Executive summary of a Joint workshop by the eunice kennedy shriver national institute of child health and human development, society for maternal-fetal medicine, american academy of pediatrics, and american college of obstetricians and gynecologists. J. Perinatol. 2014, 34, 333–342. [Google Scholar] [CrossRef]
- Mehler, K.; Oberthuer, A.; Keller, T.; Becker, I.; Valter, M.; Roth, B.; Kribs, A. Survival Among Infants Born at 22 or 23 Weeks’ Gestation Following Active Prenatal and Postnatal Care. JAMA Pediatr. 2016, 170, 671. [Google Scholar] [CrossRef]
- Sharp, M.; French, N.; McMichael, J.; Campbell, C. Survival and neurodevelopmental outcomes in extremely preterm infants 22–24 weeks of gestation born in Western Australia. J. Paediatr. Child Health 2018, 54, 188–193. [Google Scholar] [CrossRef]
- Watkins, P.L.; Dagle, J.M.; Bell, E.F.; Colaizy, T.T. Outcomes at 18 to 22 Months of Corrected Age for Infants Born at 22 to 25 Weeks of Gestation in a Center Practicing Active Management. J. Pediatr. 2020, 217, 52–58. [Google Scholar] [CrossRef]
- Puia-Dumitrescu, M.; Younge, N.; Benjamin, D.K.; Lawson, K.; Hume, C.; Hill, K.; Mengistu, J.; Wilson, A.; Zimmerman, K.O.; Ahmad, K.; et al. Medications and in-hospital outcomes in infants born at 22–24 weeks of gestation. J. Perinatol. 2020, 40, 781–789. [Google Scholar] [CrossRef]
- Lorthe, E.; Torchin, H.; Delorme, P.; Ancel, P.Y.; Marchand-Martin, L.; Foix-L’Helias, L.; Benhammou, V.; Gire, C.; d’Ercole, C.; Winer, N.; et al. Preterm premature rupture of membranes at 22–25 weeks’ gestation: Perinatal and 2-year outcomes within a national population-based study (EPIPAGE-2). Am. J. Obstet. Gynecol. 2018, 219, 298.E1–298.E14. [Google Scholar] [CrossRef] [PubMed]
- Shafey, A.; Bashir, R.A.; Shah, P.; Synnes, A.; Yang, J.; Kelly, E.N. Canadian Neonatal Network and Canadian Neonatal Follow-Up Network Investigators Outcomes and resource usage of infants born at ≤25 weeks gestation in Canada. Paediatr. Child Health 2020, 25, 207–215. [Google Scholar] [CrossRef] [PubMed]
- Kono, Y.; Yonemoto, N.; Nakanishi, H.; Kusuda, S.; Fujimura, M. Changes in survival and neurodevelopmental outcomes of infants born at <25 weeks’ gestation: A retrospective observational study in tertiary centres in Japan. BMJ Paediatr. Open 2018, 2, e000211. [Google Scholar] [CrossRef] [PubMed]
- Kusuda, S.; Fujimura, M.; Sakuma, I.; Aotani, H.; Kabe, K.; Itani, Y.; Ichiba, H.; Matsunami, K.; Nishida, H.; Neonatal Research Network, Japan. Morbidity and mortality of infants with very low birth weight in Japan: Center variation. Pediatrics 2006, 118, e1130–e1138. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.-H.; Hsu, C.-H.; Tsou, K.-I.; Jim, W.-T. Outcomes and related factors in a cohort of infants born in Taiwan over a period of five years (2007–2011) with borderline viability. J. Formos. Med. Assoc. 2018, 117, 365–373. [Google Scholar] [CrossRef] [PubMed]
- Chirinian, N.; Uji, A.; Isayama, T.; Shah, V. Neonatal care in a Japanese NICU: Notes based on a site visit. Neonatal Netw. 2012, 31, 89–96. [Google Scholar] [CrossRef]
- Stoll, B.J.; Hansen, N.I.; Bell, E.F.; Walsh, M.C.; Carlo, W.A.; Shankaran, S.; Laptook, A.R.; Sanchez, P.J.; Van Meurs, K.P.; Wyckoff, M.; et al. Trends in care practices, morbidity, and mortality of extremely preterm neonates, 1993–2012. JAMA 2015, 314, 1039–1051. [Google Scholar] [CrossRef]
- Kusuda, S. More studies are needed to convince stakeholders of the value of resuscitating periviable infants. Acta Paediatr. 2019, 108, 1182–1183. [Google Scholar] [CrossRef]
- Ishii, N.; Kono, Y.; Yonemoto, N.; Kusuda, S.; Fujimura, M.; Neonatal Research Network, Japan. Outcomes of infants born at 22 and 23 weeks’ gestation. Pediatrics 2013, 132, 62–71. [Google Scholar] [CrossRef]
- Ministry of Justice (Taiwan). Criminal Code of the Republic of China, Article 288. Available online: https://law.moj.gov.tw/ENG/LawClass/LawSearchContent.aspx?pcode=C0000001&kw1=abortion (accessed on 8 August 2020).
- Wyckoff, M.H.; Aziz, K.; Escobedo, M.B.; Kapadia, V.S.; Kattwinkel, J.; Perlman, J.M.; Simon, W.M.; Weiner, G.M.; Zaichkin, J.G. Part 13: Neonatal Resuscitation: 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care (Reprint). Pediatrics 2015, 136, S196–S218. [Google Scholar] [CrossRef]
- Kattwinkel, J.; Perlman, J.M.; Aziz, K.; Colby, C.; Fairchild, K.; Gallagher, J.; Hazinski, M.F.; Halamek, L.P.; Kumar, P.; Little, G.; et al. Neonatal resuscitation: 2010 American heart association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Pediatrics 2010, 126, e1400–e1413. [Google Scholar] [CrossRef] [PubMed]
- Umbilical Cord Milking Procedure. Available online: http://nrn.shiga-med.ac.jp/milking/ (accessed on 10 August 2020).
- Meena, J.; Charles, M.V.; Ali, A.; Ramakrishnan, S.; Gosh, S.; Seetha, K.S. Utility of cord blood culture in early onset neonatal sepsis. Australas. Med. J. 2015, 8, 263–267. [Google Scholar] [CrossRef] [PubMed]
- SUPPORT Study Group of the Eunice Kennedy Shriver NICHD Neonatal Research Network. Target ranges of oxygen saturation in extremely preterm infants. N. Eng. J. Med. 2010, 362, 1959–1969. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.-C.; Chen, Y.-J.; Huang, C.-C.; Shieh, C.-C. Concentrated Preterm Formula as a Liquid Human Milk Fortifier at Initiation Stage in Extremely Low Birth Weight Preterm Infants: Short Term and 2-year Follow-up Outcomes. Nutrients 2020, 12, 2229. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, D.A.; Blackman, A.; Conaway, M.R.; Sinkin, R.A. Nonsterile glove use in addition to hand hygiene to prevent late-onset infection in preterm infants: Randomized clinical trial. JAMA Pediatr. 2014, 168, 909–916. [Google Scholar] [CrossRef] [PubMed]
- Red LED Light MK-02GX. Available online: http://redlight.jp/englishpage.html (accessed on 7 August 2020).
- Toyoshima, K.; Kawataki, M.; Ohyama, M.; Shibasaki, J.; Yamaguchi, N.; Hoshino, R.; Itani, Y.; Nakazawa, M. Tailor-made circulatory management based on the stress-velocity relationship in preterm infants. J. Formos. Med. Assoc. 2013, 112, 510–517. [Google Scholar] [CrossRef] [PubMed]
- Su, B.H.; Lin, H.Y.; Chiu, H.Y.; Tsai, M.L.; Chen, Y.T.; Lu, I.C. Therapeutic strategy of patent ductus arteriosus in extremely preterm infants. Pediatr. Neonatol. 2020, 61, 133–141. [Google Scholar] [CrossRef] [PubMed]
- Manzoni, P.; Stolfi, I.; Pugni, L.; Decembrino, L.; Magnani, C.; Vetrano, G.; Tridapalli, E.; Corona, G.; Giovannozzi, C.; Farina, D.; et al. A multicenter, randomized trial of prophylactic fluconazole in preterm neonates. N. Engl. J. Med. 2007, 356, 2483–2495. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.W.; Lin, Y.C.; Tu, Y.F.; Wang, S.T.; Huang, C.C.; Taiwan Premature Infant Developmental Collaborative Study Group. Isolated cystic periventricular leukomalacia differs from cystic periventricular leukomalacia with intraventricular hemorrhage in prevalence, risk factors and outcomes in preterm infants. Neonatology 2017, 111, 86–92. [Google Scholar] [CrossRef]
- Wang, L.W.; Lin, Y.C.; Wang, S.T.; Huang, C.C.; on behalf of the Taiwan Premature Infant Developmental Collaborative Study Group. Identifying Risk Factors Shared by Bronchopulmonary Dysplasia, Severe Retinopathy, and Cystic Periventricular Leukomalacia in Very Preterm Infants for Targeted Intervention. Neonatology 2018, 114, 17–24. [Google Scholar] [CrossRef]
- Chou, J.H.; Roumiantsev, S.; Singh, R. PediTools Electronic Growth Chart Calculators: Applications in Clinical Care, Research, and Quality Improvement. J. Med. Int. Res. 2020, 22, e16204. [Google Scholar] [CrossRef] [PubMed]
- El-Metwally, D.; Vohr, B.; Tucker, R. Survival and neonatal morbidity at the limits of viability in the mid 1990s: 22 to 25 weeks. J. Pediatr. 2000, 137, 616–622. [Google Scholar] [CrossRef] [PubMed]
- Merritt, T.A.; Boynton, B.R.; Hallman, M. Viability of infants born at 22 to 25 weeks’ gestation. N. Engl. J. Med. 1994, 330, 1234–1235. [Google Scholar] [PubMed]
- Su, B.H.; Hsieh, W.S.; Hsu, C.H.; Chang, J.H.; Lien, R.; Lin, C.H.; Premature Baby Foundation of Taiwan (PBFT). Neonatal outcomes of extremely preterm infants from taiwan: Comparison with Canada, Japan, and the USA. Pediatr. Neonatol. 2015, 56, 46–52. [Google Scholar] [CrossRef] [PubMed]
- The Comparison of Health Insurance Systems between Taiwan and Korea. Available online: http://www.airitilibrary.com/Publication/alDetailPrint?DocID=U0001-2408200714414000 (accessed on 12 August 2020).
- Lawrence, C.; Laventhal, N.; Fritz, K.A.; Carlos, C.; Famuyide, M.; Tonismae, T.; Hayslett, D.; Coleman, T.; Jain, M.; Edmonds, B.T.; et al. Ethical cultures in perinatal care: Do they exist? Correlation of provider attitudes with periviability practices at six centers. Am. J. Perinatol. 2020. [Google Scholar] [CrossRef] [PubMed]
- McAdams, R.M.; Erdenebileg, A.; Batra, M.; Gerelmaa, Z. Attitudes of healthcare providers towards non-initiation and withdrawal of neonatal resuscitation for preterm infants in Mongolia. J. Health Popul. Nutr. 2012, 30, 346–352. [Google Scholar] [CrossRef][Green Version]
- The Criterion for Accreditation of Tertiaryhospitals. Available online: https://dep.mohw.gov.tw/DOMA/lp-984-106.html (accessed on 12 August 2020).
- Carlo, W.A.; McDonald, S.A.; Fanaroff, A.A.; Vohr, B.R.; Stoll, B.J.; Ehrenkranz, R.A.; Andrews, W.W.; Wallace, D.; Das, A.; Bell, E.F.; et al. Association of antenatal corticosteroids with mortality and neurodevelopmental outcomes among infants born at 22 to 25 weeks’ gestation. JAMA 2011, 306, 2348–2358. [Google Scholar] [CrossRef] [PubMed]
- Ehret, D.E.Y.; Edwards, E.M.; Greenberg, L.T.; Bernstein, I.M.; Buzas, J.S.; Soll, R.F.; Horbar, J.D. Association of Antenatal Steroid Exposure with Survival among Infants Receiving Postnatal Life Support at 22 to 25 Weeks’ Gestation. JAMA Netw. Open 2018, 1, e183235. [Google Scholar] [CrossRef]
- Kyser, K.L.; Morriss, F.H., Jr.; Bell, E.F.; Klein, J.M.; Dagle, J.M. Improving survival of extremely preterm infants born between 22 and 25 weeks of gestation. Obstet. Gynecol. 2012, 119, 795–800. [Google Scholar] [CrossRef]
- Qiu, X.; Lodha, A.; Shah, P.S.; Sankaran, K.; Seshia, M.M.; Yee, W.; Jefferies, A.; Lee, S.K.; The Canadian Neonatal Network. Neonatal outcomes of small for gestational age preterm infants in Canada. Am. J. Perinatol. 2012, 29, 87–94. [Google Scholar] [CrossRef]
- Jensen, E.A.; Foglia, E.E.; Dysart, K.C.; Simmons, R.A.; Aghai, Z.H.; Cook, A.; Greenspan, J.S.; De Mauro, S.B. Adverse effects of small for gestational age differ by gestational week among very preterm infants. Arch. Dis. Child. Fetal Neonatal Ed. 2019, 104, F192–F198. [Google Scholar] [CrossRef] [PubMed]
- Rossi, R.M.; Hall, E.; DeFranco, E.A. Contemporary Trends in Cesarean Delivery Utilization for Live Births between 22 0/7 and 23 6/7 Weeks of Gestation. Obstet. Gynecol. 2019, 133, 451–458. [Google Scholar] [CrossRef] [PubMed]
- Malloy, M.H.; Doshi, S. Cesarean section and the outcome of very preterm and very low-birthweight infants. Clin. Perinatol. 2008, 35, 421–435. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| All Enrolled Infants | Epoch-I | Epoch-II | p Value | |
|---|---|---|---|---|
| Enrolled infants, N | 168 | 92 | 76 | |
| Sex, male | 96 (57.1) | 54 (58.7) | 42 (55.3) | 0.754 |
| Gestational age, weeks | 23.8 ± 1 | 24.0 ± 0.9 | 23.6 ± 1.0 | 0.002 |
| Body weight at birth, grams | 648 ± 122 | 681 ± 120 | 609 ± 112 | <0.001 |
| z score of body weight at birth | 0.12 ± 0.98 | 0.01 ± 0.99 | −0.29 ± 0.93 | 0.048 |
| small for gestational age | 18 (10.7) | 6 (6.5) | 12 (15.8) | 0.078 |
| Maternal condition | ||||
| Maternal age, years | 31.6 ± 5.3 | 31.3 ± 5.0 | 31.9 ± 5.7 | 0.519 |
| Multiple pregnancy | 77 (45.8) | 27 (29.3) | 50 (65.8) | <0.001 |
| Antenatal steroid therapy | 147 (87.5) | 78 (84.8) | 69 (90.8) | 0.349 |
| Gestational diabetes mellitus | 7 (4.2) | 4 (4.3) | 3 (3.9) | 1.000 |
| Maternal pre-eclampsia | 23 (13.7) | 9 (9.8) | 14 (18.4) | 0.119 |
| PPROM | 62 (36.9) | 33 (35.9) | 29 (38.2) | 0.872 |
| Perinatal condition and treatment | ||||
| Inborn | 152 (90.5) | 84 (91.3) | 68 (89.5) | 0.794 |
| Cesarean section | 82 (48.8) | 45 (48.9) | 37 (48.7) | 1.000 |
| Apgar score at 5 min | 6 (5–8) | 7 (5–8) | 6 (5–7) | 0.409 |
| 1 Body temperature at admission, °C | 35.4 ± 1.2 | 35.4 ± 1.0 | 35.4 ± 1.3 | 0.869 |
| Hypothermia 1 at admission | 135 (80.4) | 77 (83.7%) | 58 (76.3) | 0.248 |
| Blood pH at admission | 7.21 ± 0.15 | 7.22 ± 0.12 | 7.20 ± 0.17 | 0.512 |
| Blood sugar at admission, mg/dL | 93.3 ± 35.2 | 95.6 ± 35.7 | 90.4 ± 34.8 | 0.343 |
| Early-onset sepsis | 17 (10.1) | 5 (5.5) | 12 (16.0) | 0.038 |
| Surfactant-treated RDS | 105 (62.5) | 54 (58.7) | 51 (67.1) | 0.337 |
| Survival or mortality variable | ||||
| Survived to discharge | 103 (61.3) | 53 (57.6) | 50 (65.8) | 0.340 |
| PMA at discharge of survivor, weeks | 41.5 ± 7.0 | 40.5 ± 8.0 | 42.7 ± 5.4 | 0.109 |
| Mortality in the first month of life, n (% of all mortality cases) | 56 (86.2) | 34 (87.2) | 22 (84.6) | 1.000 |
| Postnatal age of mortality, days | 4.0 (2.5–18.5) | 4.0 (3–19) | 4.0 (2–11) | 0.595 |
| OR | 95% CI for OR | p Value | ||
|---|---|---|---|---|
| Lower | Upper | |||
| Basic Information | ||||
| Sex, male (ref. F) | 0.916 | 0.488 | 1.717 | 0.784 |
| Gestational age, Weeks | 1.654 | 1.197 | 2.285 | 0.002 |
| Birth BW, 100 g | 1.691 | 1.269 | 2.252 | <0.001 |
| z score of birth BW | 1.324 | 0.951 | 1.844 | 0.096 |
| SGA (ref. no) | 0.273 | 0.097 | 0.77 | 0.014 |
| Epoch of birth, II (ref. I) | 1.415 | 0.754 | 2.654 | 0.279 |
| Maternal condition | ||||
| Maternal Age | 1.01 | 0.953 | 1.071 | 0.735 |
| Antenatal steroid (ref. no) | 1.894 | 0.755 | 4.752 | 0.173 |
| Antenatal MgSO4 (ref. no) | 1.21 | 0.546 | 2.682 | 0.638 |
| Gestational DM (ref. no) | 1.607 | 0.303 | 8.538 | 0.578 |
| Preeclampsia (ref. no) | 0.349 | 0.141 | 0.861 | 0.022 |
| PPROM (ref. no) | 0.897 | 0.472 | 1.704 | 0.740 |
| Chorioamnionitis (ref. no) | 1.029 | 0.402 | 2.638 | 0.952 |
| Perinatal condition and treatment | ||||
| Inborn (ref. no) | 2.011 | 0.62 | 6.526 | 0.245 |
| Cesarean section (ref. no) | 0.587 | 0.314 | 1.099 | 0.096 |
| Apgar at 5 min | 1.309 | 1.113 | 1.539 | 0.001 |
| Hypothermia (ref. no) | 0.529 | 0.229 | 1.224 | 0.137 |
| Blood pH, (ref. lowest level 1) | 1.860 | 1.205 | 2.87 | 0.005 |
| Blood sugar, mg/dL | 0.997 | 0.988 | 1.006 | 0.485 |
| Early onset sepsis (ref. no) | 0.505 | 0.184 | 1.386 | 0.185 |
| Therapeutic surfactant therapy (ref. no) | 0.265 | 0.129 | 0.545 | <0.001 |
| Covariates | OR | 95% CI for OR | p Value | R Square | |
|---|---|---|---|---|---|
| Lower | Upper | 0.348 | |||
| Epoch | |||||
| II (2016–2019) | 2.602 | 1.170 | 5.789 | 0.019 | |
| I (2010–2015; reference) | |||||
| Antenatal steroid therapy | |||||
| Yes | 2.137 | 0.676 | 6.759 | 0.196 | |
| No (reference) | |||||
| Gestational age, weeks | 1.884 | 1.244 | 2.852 | 0.003 | |
| SGA | |||||
| Yes | 0.154 | 0.044 | 0.541 | 0.004 | |
| No (reference) | |||||
| Sex | |||||
| Female | 0.953 | 0.438 | 2.075 | 0.904 | |
| Male (reference) | |||||
| Cesarean section | |||||
| Yes | 0.417 | 0.186 | 0.934 | 0.033 | |
| No (reference) | |||||
| Hypothermia at admission | |||||
| Yes | 0.518 | 0.19 | 1.414 | 0.199 | |
| No (reference) | |||||
| Blood pH at birth (binned value) 1 | 1.94 | 1.156 | 3.255 | 0.012 | |
| Therapeutic surfactant therapy | |||||
| Yes | 0.306 | 0.133 | 0.705 | 0.005 | |
| No (reference) | |||||
| Adjusted OR 1 | 95% C.I. for aOR | p Value | ||
|---|---|---|---|---|
| Lower | Upper | |||
| GA 25 W | 1.314 | 0.275 | 6.285 | 0.732 |
| GA 24 W | 1.299 | 0.255 | 6.610 | 0.753 |
| GA 23 W | 10.314 | 2.430 | 43.774 | 0.002 |
| GA 22 W | NA | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Y.-J.; Yu, W.-H.; Chen, L.-W.; Huang, C.-C.; Kang, L.; Lin, H.-S.; Iwata, O.; Kato, S.; Hussein, M.H.; Lin, Y.-C. Improved Survival of Periviable Infants after Alteration of the Threshold of Viability by the Neonatal Resuscitation Program 2015. Children 2021, 8, 23. https://doi.org/10.3390/children8010023
Chen Y-J, Yu W-H, Chen L-W, Huang C-C, Kang L, Lin H-S, Iwata O, Kato S, Hussein MH, Lin Y-C. Improved Survival of Periviable Infants after Alteration of the Threshold of Viability by the Neonatal Resuscitation Program 2015. Children. 2021; 8(1):23. https://doi.org/10.3390/children8010023
Chicago/Turabian StyleChen, Yen-Ju, Wen-Hao Yu, Li-Wen Chen, Chao-Ching Huang, Lin Kang, Hui-Shan Lin, Osuke Iwata, Shin Kato, Mohamed Hamed Hussein, and Yung-Chieh Lin. 2021. "Improved Survival of Periviable Infants after Alteration of the Threshold of Viability by the Neonatal Resuscitation Program 2015" Children 8, no. 1: 23. https://doi.org/10.3390/children8010023
APA StyleChen, Y.-J., Yu, W.-H., Chen, L.-W., Huang, C.-C., Kang, L., Lin, H.-S., Iwata, O., Kato, S., Hussein, M. H., & Lin, Y.-C. (2021). Improved Survival of Periviable Infants after Alteration of the Threshold of Viability by the Neonatal Resuscitation Program 2015. Children, 8(1), 23. https://doi.org/10.3390/children8010023