Body Posture Defects and Body Composition in School-Age Children



Abstract
1. Introduction
2. Material and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Czaprowski, D.; Stoliński, Ł.; Tyrakowski, M.; Kozinoga, M.; Kotwicki, T. Non-structural misalignments of body posture in the sagittal plane. Scoliosis Spinal Disord. 2018, 13, 1–14. [Google Scholar] [CrossRef]
- Wilczyński, J.; Bieniek, K. Canonical correlations between somatic features and postural stability in children aged 10–12. Med. Stud. 2019, 35, 93–99. [Google Scholar] [CrossRef]
- Domagalska-Szopa, M.; Szopa, A. Postural orientation and standing postural alignment in ambulant children with bilateral cerebral palsy. Clin. Biomech. 2017, 16, 22–27. [Google Scholar]
- Binkley, T.; Specker, B. The negative effect of sitting time on bone is mediated by lean mass in pubertal children. J. Musculoskelet. Neuronal Interact. 2016, 16, 18–23. [Google Scholar] [PubMed]
- Calloni, S.F.; Huisman, T.A.; Poretti, A. Back pain and scoliosis in children: When to image, what to consider. Neuroradiol. J. 2017, 30, 393–404. [Google Scholar] [PubMed]
- Clark, E.M.; Taylor, H.J.; Harding, I.; Hutchinson, J.; Nelson, I.; Deanfield, J.; Ness, A.; Tobias, J.H.; Nelson, I. Association Between Components of Body Composition and Scoliosis: A Prospective Cohort Study Reporting Differences Identifiable Before the Onset of Scoliosis. J. Bone Miner. Res. 2014, 29, 1729–1736. [Google Scholar] [CrossRef] [PubMed]
- Dayer, R.; Haumont, T.; Belaieff, W. Idiopathic scoliosis: Etiological concepts and hypotheses. J. Child. Orthop. 2013, 7, 11–16. [Google Scholar] [PubMed]
- Girardo, M.; Bettini, N.; Dema, E.; Cervellati, S. The role of melatonin in the pathogenesis of adolescent idiopathic scoliosis (AIS). Eur. Spine J. 2011, 20, 68–74. [Google Scholar]
- Goodbody, C.M.; Asztalos, I.B.; Sankar, W.N.; Flynn, J.M. It’s not just the big kids: Both high and low BMI impact bracing success for adolescent idiopathic scoliosis. J. Child. Orthop. 2016, 10, 395–404. [Google Scholar]
- Stolinski, L.; Kozinoga, M.; Czaprowski, D.; Tyrakowski, M.; Cerny, P.; Suzuki, N.; Kotwicki, T. Two-dimensional digital photography for child body posture evaluation: Standardized technique, reliable parameters and normative data for age 7–10 years. Scoliosis Spinal Disord. 2017, 12, 38. [Google Scholar] [CrossRef]
- Drerup, B.; Ellger, B.; zu Meyer Bentrup, F.M.; Hierholzer, E. Functional rasterstereographic images. A new method for biomechanical analysis of skeletal geometry. Orthopäde 2001, 30, 242–250. [Google Scholar] [CrossRef] [PubMed]
- Harzmann, H.C. Optischer Gipsabdruckhilftbei der Rückenanalyse. Süddeutscher Orthopädenkongress. Kongressausgabe 1999, 2, 15. [Google Scholar]
- Grant, C.A.; Newell, N.; Izatt, M.T. A comparison of vertebral venous networks in adolescent idiopathic scoliosis patients and healthy controls. Surg. Radiol. Anat. 2017, 39, 281–291. [Google Scholar] [CrossRef] [PubMed]
- Hedberg-Oldfors, C.; Darin, N.; Olsson Engman, M. A new early-onset neuromuscular disorder associated with kyphoscoliosis peptidase (KY) deficiency. Eur. J. Hum. Genet. 2016, 24, 1771–1777. [Google Scholar] [CrossRef]
- Högler, W.; Baumann, U.; Kelly, D. Endocrine and bone metabolic complications in chronic liver disease and after liver transplantation in children. J. Pediatr. Gastroenterol. Nutr. 2012, 54, 313–321. [Google Scholar] [CrossRef]
- Kim, H.Y.; Cha, Y.-H.; Chun, Y.S.; Shin, H.S. Correlation of the torsion values measured by rotational profile, kinematics, and CT study in CP patients. Gait Posture 2017, 57, 241–245. [Google Scholar] [CrossRef]
- Ludwig, O.; Hammes, A.; Kelm, J.; Schmitt, E. Assessment of the posture of adolescents in everyday clinical practice: Intra-rater and inter-rater reliability and validity of a posture index. J. Bodyw. Mov. Ther. 2016, 20, 761–766. [Google Scholar] [CrossRef]
- Margalit, A.; Mckean, G.; Constantine, A.; Thompson, C.B.; Lee, R.J.; Sponseller, P.D. Body Mass Hides the Curve. J. Pediatr. Orthop. 2017, 37, e255–e260. [Google Scholar] [CrossRef] [PubMed]
- Monticone, M.; Ambrosini, E.; Cazzaniga, D.; Rocca, B.; Motta, L.; Cerri, C.; Brayda-Bruno, M.; Lovi, A. Adults with idiopathic scoliosis improve disability after motor and cognitive rehabilitation: Results of a randomised controlled trial. Eur. Spine J. 2016, 25, 3120–3129. [Google Scholar] [CrossRef]
- Neiva, P.D.; Kirkwood, R.N.; Mendes, P.L.; Zabjek, K.; Becker, H.G.; Mathur, S. Postural disorders in mouth breathing children: A systematic review. Braz. J. Phys. Ther. 2017, 22, 7–19. [Google Scholar] [CrossRef]
- Oishi, S.N.; Agranovich, O.; Pajardi, G.E. Treatment of the Upper Extremity Contracture/Deformities. J. Pediatr. Orthop. 2017, 37, S9–S15. [Google Scholar] [CrossRef] [PubMed]
- Porte, M.; Patte, K.; Dupeyron, A. Exercise therapy in the treatment of idiopathic adolescent scoliosis: Is it useful? Arch Pediatr. 2016, 23, 624–628. [Google Scholar] [CrossRef] [PubMed]
- Putzier, M.; Groß, C.; Zahn, R.K. Characteristics of neuromuscular scoliosis. Orthopade 2016, 45, 500–508. [Google Scholar] [CrossRef] [PubMed]
- Senthil, P.; Sudhakar, S.; Porcelvan, S. Implication of Posture Analysing Software to Evaluate the Postural Changes after Corrective Exercise Strategy on Subjects with Upper Body Dysfunction-A Randomized Controlled Trial. J. Clindiagn. Res. 2017, 11, YC01–YC04. [Google Scholar] [CrossRef]
- Tam, E.M.; Liu, Z.; Lam, T.P. Lower Muscle Mass and Body Fat in Adolescent Idiopathic Scoliosis Are Associated with Abnormal Leptin Bioavailability. Spine 2016, 41, 940–946. [Google Scholar] [CrossRef]
- Tarrant, R.C.; Queally, J.M.; Moore, D.P.; Kiely, P.J. Prevalence and impact of low body mass index on outcomes in patients with adolescent idiopathic scoliosis: A systematic review. Eur. J. Clinnutr. 2018, 12. [Google Scholar] [CrossRef]
- Wang, W.; Wang, Z.; Zhu, Z. Body composition in males with adolescent idiopathic scoliosis: A case-control study with dual-energy X-ray absorptiometry. BMC Musculoskelet Disord. 2016, 29, 107. [Google Scholar] [CrossRef]
- Weiss, H.R. Current knowledge on physiotherapy for scoliosis. Orthopade 2016, 45, 549–550. [Google Scholar] [CrossRef]
- Araújo, F.; Simões, A.D.G.A.; Silva, P.; Alegrete, N.; Lucas, R. Sagittal standing posture and relationships with anthropometrics and body composition during childhood. Gait Posture 2019, 73, 45–51. [Google Scholar] [CrossRef]
- Wyszyńska, J.; Podgórska-Bednarz, J.; Drzał-Grabiec, J. Analysis of Relationship between the Body Mass Composition and Physical Activity with Body Posture in Children. Biomed. Res. Int. 2016, 2016, 185167. [Google Scholar] [CrossRef]
- Rusek, W.; Baran, J.; Leszczak, J.; Adamczyk, M.; Weres, A.; Baran, R.; Inglot, G.; Pop, T. The Influence of Body Mass Composition on the Postural Characterization of School-Age Children and Adolescents. Biomed. Res. Int. 2018, 14, 9459014. [Google Scholar] [CrossRef] [PubMed]
- Barczyk, K.; Skolimowski, T.; Anwajler, J.; Chamela-Bilińska, D. Somatic features and parameters of anterior-posterior spinal curvature in 7-year-olds with particular posture types. Ortop. Traumatol. Rehabil. 2005, 7, 555–562. [Google Scholar] [PubMed]
- Lin, M.; Liu, Z.; Liu, G.; Zhao, S.; Li, C.; Chen, W. Identification of novel FBN1 variations implicated in congenital scoliosis. J. Hum. Genet. 2019, 65, 221–230. [Google Scholar] [CrossRef] [PubMed]
- Burwell, R.G.; Dangerfield, P.H. Etiologic theories of idiopathic scoliosis: Neurodevelopmental concepts to be evaluated. Stud. Heal. Technol. Inform. 2002, 91, 15–19. [Google Scholar]
- Kuznia, A.L.; Hernandez, A.K.; Lee, L.U. Adolescent Idiopathic Scoliosis: Common Questions and Answers. Am. Fam. Phys. 2020, 101, 19–23. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
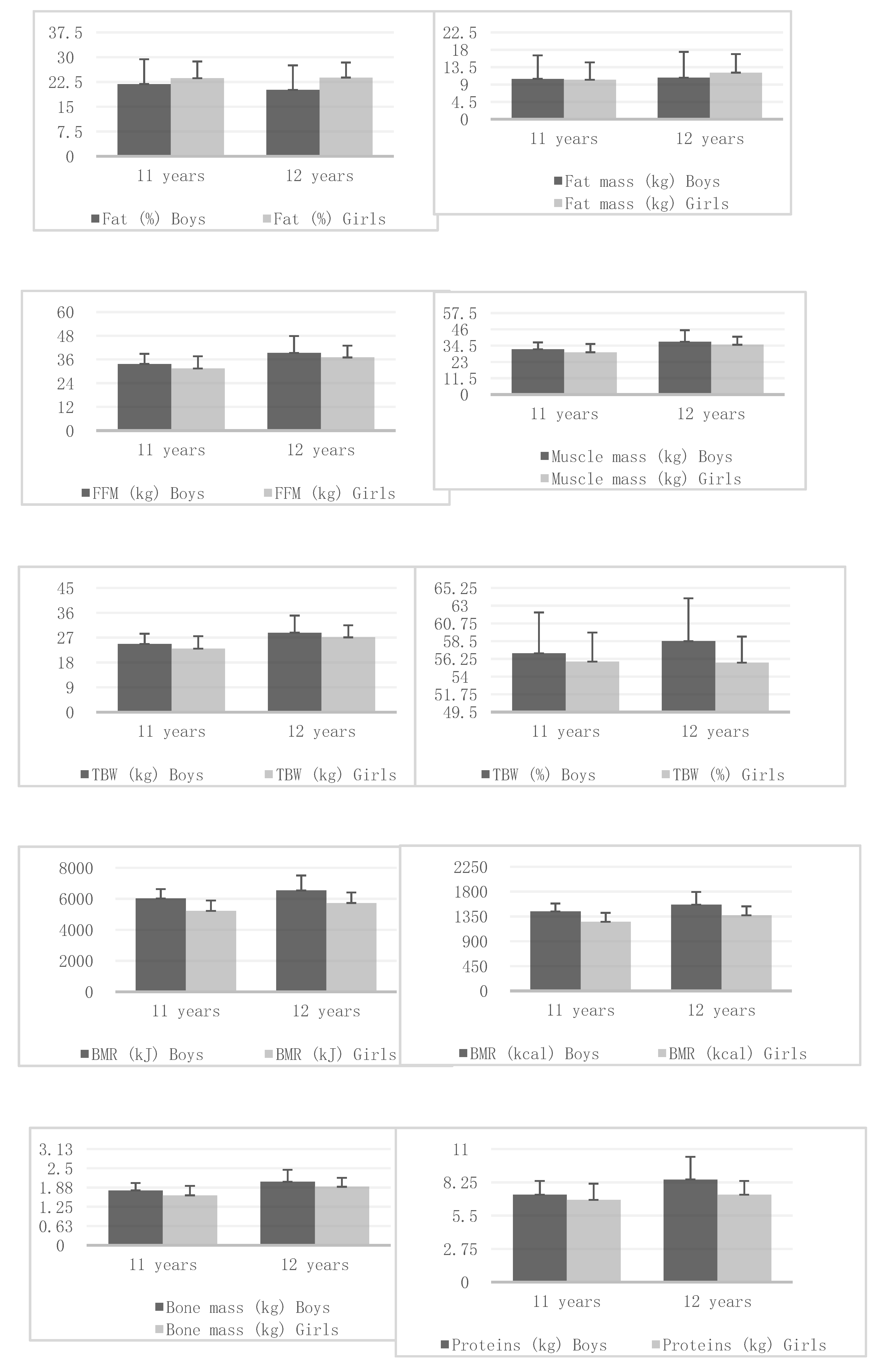
| Variables | Age | Boys/Girls | X | SD | Mann–Whitney U Test | Student’s t-Test |
|---|---|---|---|---|---|---|
| Body height (cm) | 11 | Boys | 151.44 | 5.49 | Z = 1.877 p = 0.060 | t = 1.673 p = 0.097 |
| Girls | 149.35 | 8.23 | ||||
| 12 | Boys | 158.18 | 8.71 | Z = 0.886 p = 0.375 | t = −0.768 p = 0.444 | |
| Girls | 159.24 | 6.63 | ||||
| Body mass (kg) | 11 | Boys | 44.19 | 10.56 | Z = 1.420 p = 0.155 | t = 1.386 p = 0.168 |
| Girls | 41.66 | 10.23 | ||||
| 12 | Boys | 50.08 | 13.72 | Z = 0.114 p = 0.908 | t = 0.446 p = 0.656 | |
| Girls | 49.11 | 10.34 | ||||
| Fat (%) | 11 | Boys | 21.85 | 7.5 | Z = 2.225 p = 0.026 | t = −1.626 p = 0.106 |
| Girls | 23.65 | 5.06 | ||||
| 12 | Boys | 20.1 | 7.43 | Z = 3.993 p = 0.000 | t = −3.371 p = 0.001 | |
| Girls | 23.82 | 4.55 | ||||
| Fat mass (kg) | 11 | Boys | 10.46 | 6.07 | Z = 0.568 p = 0.569 | t = 0.245 p = 0.806 |
| Girls | 10.23 | 4.49 | ||||
| 12 | Boys | 10.75 | 6.7 | Z = 2.600 p = 0.009 | t = −1.271 p = 0.206 | |
| Girls | 12.07 | 4.81 | ||||
| FFM (kg) | 11 | Boys | 33.72 | 5.11 | Z = 2.561 p = 0.010 | t = 2.334 p = 0.021 |
| Girls | 31.42 | 6.16 | ||||
| 12 | Boys | 39.33 | 8.49 | Z = 1.333 p = 0.182 | t = 1.749 p = 0.083 | |
| Girls | 37.04 | 5.94 | ||||
| Muscle mass (kg) | 11 | Boys | 31.9 | 4.92 | Z = 2.467 p = 0.0136 | t = 2.229 p = 0.027 |
| Girls | 29.8 | 5.85 | ||||
| 12 | Boys | 37.28 | 8.1 | Z = 1.288 p = 0.197 | t = 1.707 p = 0.090 | |
| Girls | 35.15 | 5.65 | ||||
| BMI | 11 | Boys | 19.13 | 3.76 | Z = 0.739 p = 0.459 | t = 1.046 p = 0.297 |
| Girls | 18.48 | 3.26 | ||||
| 12 | Boys | 19.77 | 4.1 | Z = 0.345 p = 0.729 | t = 0.797 p = 0.426 | |
| Girls | 19.25 | 3.28 | ||||
| TBW (kg) | 11 | Boys | 24.69 | 3.75 | Z = 2.554 p = 0.010 | t = 2.334 p = 0.021 |
| Girls | 23 | 4.52 | ||||
| 12 | Boys | 28.79 | 6.22 | Z = 1.331 p = 0.183 | t = 1.754 p = 0.082 | |
| Girls | 27.11 | 4.35 | ||||
| TBW (%) | 11 | Boys | 56.96 | 5.18 | Z = 1.965 p = 0.049 | t = 1.358 p = 0.176 |
| Girls | 55.9 | 3.69 | ||||
| 12 | Boys | 58.49 | 5.45 | Z = 4.024 p = 0.000 | t = 3.375 p = 0.001 | |
| Girls | 55.77 | 3.31 | ||||
| BMR (kJ) | 11 | Boys | 6029.91 | 597.4 | Z = 6.367 p < 0.001 | t = 7.255 p < 0.001 |
| Girls | 5220.55 | 674.44 | ||||
| 12 | Boys | 6538.84 | 970.67 | Z = 5.021 p < 0.001 | t = 5.393 p < 0.001 | |
| Girls | 5733.16 | 678.25 | ||||
| BMR (kcal) | 11 | Boys | 1441.17 | 142.78 | Z = 6.195 p < 0.001 | t = 7.036 p < 0.001 |
| Girls | 1252.75 | 162.54 | ||||
| 12 | Boys | 1562.82 | 231.99 | Z = 5.021 p < 0.001 | t = 5.394 p < 0.001 | |
| Girls | 1370.25 | 162.11 | ||||
| Bone mass (kg) | 11 | Boys | 1.78 | 0.24 | Z = 3.580 p = 0.001 | t = 3.291 p = 0.001 |
| Girls | 1.62 | 0.31 | ||||
| 12 | Boys | 2.06 | 0.39 | Z = 2.227 p = 0.025 | t = 2.588 p = 0.010 | |
| Girls | 1.9 | 0.29 | ||||
| Proteins (kg) | 11 | Boys | 7.23 | 1.13 | Z = 2.270 p = 0.023 | t = 2.014 p = 0.046 |
| Girls | 6.8 | 1.34 | ||||
| 12 | Boys | 8.48 | 1.88 | Z = 1.114 p = 0.265 | t = 1.550 p = 0.124 | |
| Girls | 7.23 | 1.13 |
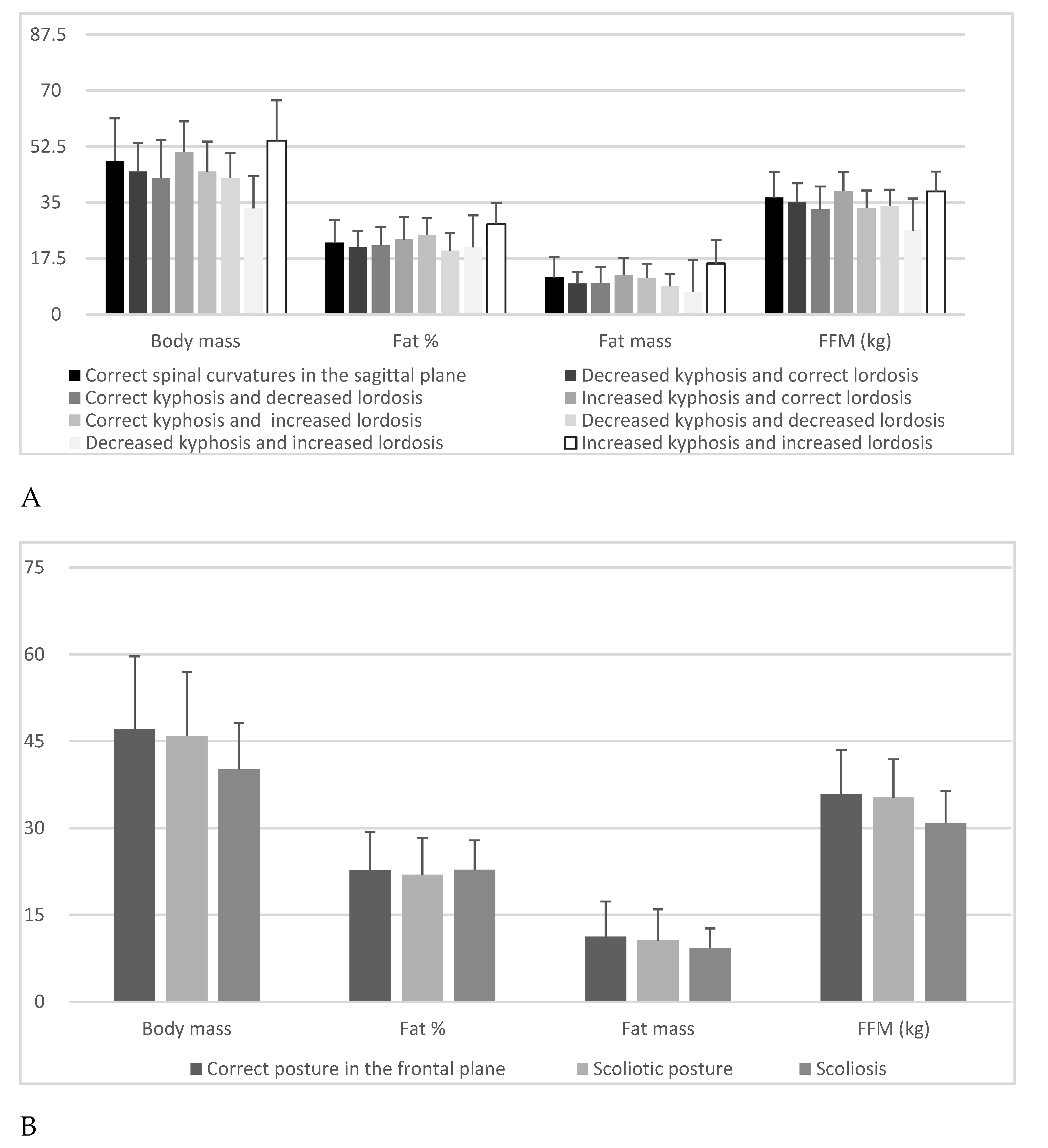
| Variables | N; % | Body Mass (kg) | Fat (%) | Fat Mass (kg) | FFM (kg) | ||||
|---|---|---|---|---|---|---|---|---|---|
| X; SD | Kruskal–Wallis Test | X; SD | Kruskal–Wallis Test | X; SD | Kruskal–Wallis Test | X; SD | Kruskal–Wallis Test | ||
| Correct spinal curvatures in the sagittal plane | 106% 41.08 | 48.00 ± 13.29 | H = 22.81 p = 0.001 | 22.46 ± 7.02 | H = 20.28 p = 0.005 | 11.50 ± 6.42 | H = 20.49 p = 0.004 | 36.50 ± 8.03 | H = 21.648 p = 0.002 |
| Decreased kyphosis and correct lordosis | 40% 15.50 | 44.62 ± 8.98 | 21.02 ± 5.03 | 9.62 ± 3.71 | 35.00 ± 5.97 | ||||
| Correct kyphosis and decreased lordosis | 24% 9.30 | 42.58 ± 11.89 | 21.58 ± 5.82 | 9.75 ± 5.07 | 32.84 ± 7.14 | ||||
| Increased kyphosis and correct lordosis | 17% 6.59 | 50.79 ± 9.53 | 23.42 ± 7.05 | 12.29 ± 5.24 | 38.50 ± 5.93 | ||||
| Correct kyphosis and increased lordosis | 22% 8.53 | 44.64 ± 9.39 | 24.74 ± 5.29 | 11.40 ± 4.44 | 33.24 ± 5.48 | ||||
| Decreased kyphosis and decreased lordosis | 32% 12.40 | 42.63 ± 7.86 | 19.94 ± 5.55 | 8.77 ± 3.75 | 33.87 ± 5.12 | ||||
| Decreased kyphosis and increased lordosis | 4% 1.55 | 33.18 ± 6.16 | 20.93 ± 3.41 | 6.98 ± 1.79 | 26.20 ± 4.84 | ||||
| Increased kyphosis and increased lordosis | 13% 5.04 | 54.31 ± 12.60 | 28.16 ± 6.62 | 15.90 ± 7.37 | 38.41 ± 6.24 | ||||
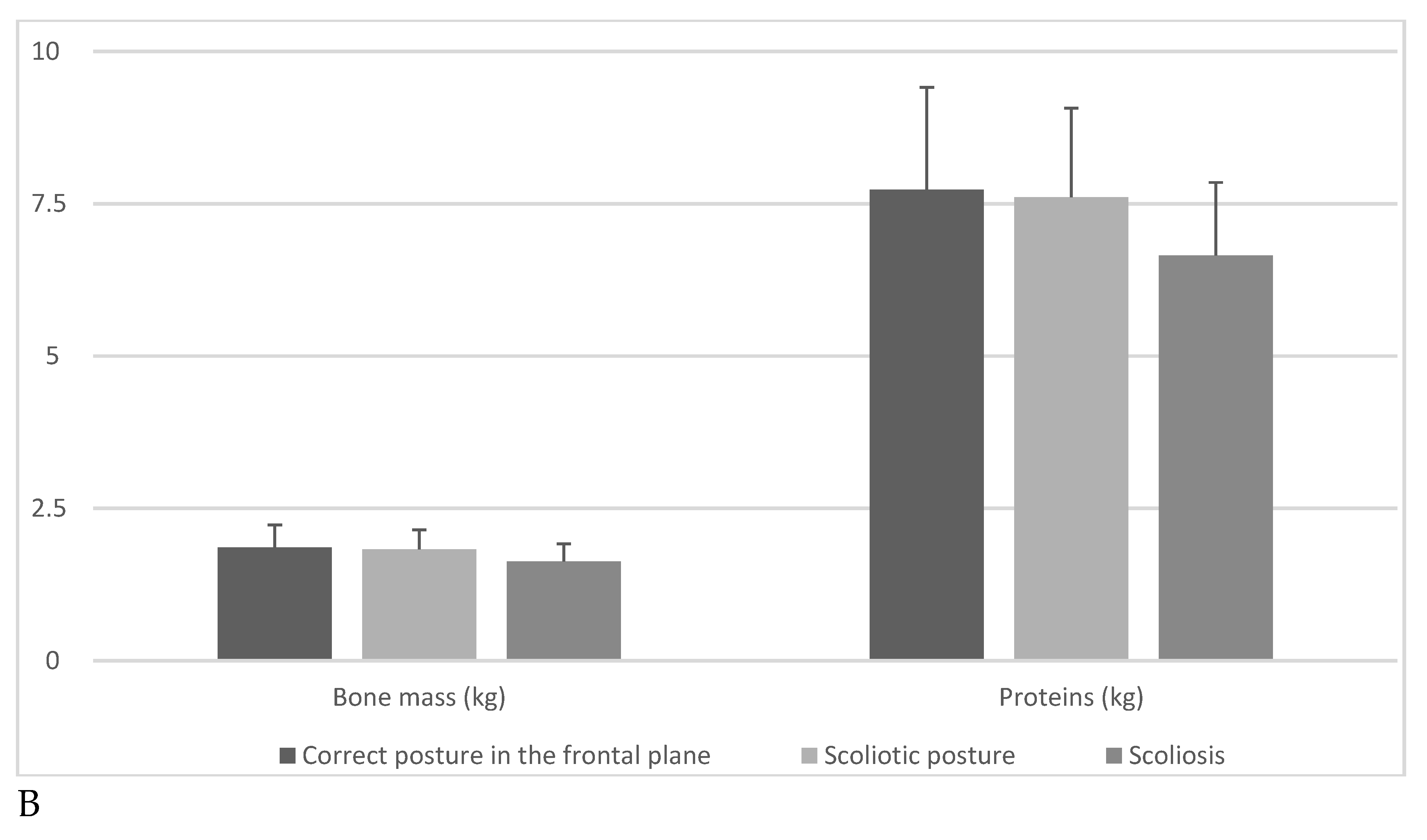
| Correct posture in the frontal plane | 116% 44.96 | 47.06 ± 12.58 | H = 2.252 p = 0.324 | 22.77 ± 6.58 | H = 1.055 p = 0.589 | 11.28 ± 6.04 | H = 1.005 p = 0.604 | 35.78 ± 7.67 | H = 3.011 p = 0.221 |
| Scoliotic posture | 134% 51.94 | 45.86 ± 11.04 | 21.95 ± 6.40 | 10.61 ± 5.33 | 35.25 ± 6.61 | ||||
| Scoliosis | 8% 3.10 | 40.14 ± 7.99 | 22.78 ± 5.08 | 9.31 ± 3.34 | 30.83 ± 5.60 | ||||
| Variables | N; % | Muscle Mass (kg) | BMI | TBW (kg) | TBW (%) | ||||
|---|---|---|---|---|---|---|---|---|---|
| X; SD | Kruskal–Wallis Test | X; SD | Kruskal–Wallis Test | X; SD | Kruskal–Wallis Test | X; SD | Kruskal–Wallis Test | ||
| Correct spinal curvatures in the sagittal plane | 106% 41.08 | 34.61 ± 7.65 | H = 21.907 p = 0.002 | 19.5 ± 4.08 | H = 18.397 p = 0.011 | 26.72 ± 5.88 | H = 21.668 p = 0.002 | 56.57 ± 4.91 | H = 20.247 p = 0.005 |
| Decreased kyphosis and correct lordosis | 40% 15.50 | 33.17 ± 5.69 | 18.3 ± 2.41 | 25.62 ± 4.36 | 57.85 ± 3.63 | ||||
| Correct kyphosis and decreased lordosis | 24% 9.30 | 31.12 ± 6.80 | 18.7 ± 3.56 | 24.05 ± 5.22 | 57.42 ± 4.28 | ||||
| Increased kyphosis and correct lordosis | 17% 6.59 | 36.51 ± 5.65 | 20.6 ± 3.31 | 28.20 ± 4.35 | 56.09 ± 5.14 | ||||
| Correct kyphosis and increased lordosis | 22% 8.53 | 31.39 ± 5.32 | 18.9 ± 3.26 | 24.33 ± 4.01 | 55.10 ± 3.88 | ||||
| Decreased kyphosis and decreased lordosis | 32% 12.40 | 32.09 ± 4.86 | 17.9 ± 2.66 | 24.79 ± 3.76 | 58.61 ± 4.08 | ||||
| Decreased kyphosis and increased lordosis | 4% 1.55 | 24.83 ± 4.62 | 15.2 ± 2.25 | 19.15 ± 3.55 | 57.83 ± 2.54 | ||||
| Increased kyphosis and increased lordosis | 13% 5.04 | 36.43 ± 5.93 | 21.6 ± 4.30 | 28.13 ± 4.57 | 52.62 ± 4.84 | ||||
| Correct posture in the frontal plane | 116% 44.96 | 33.92 ± 7.30 | H = 3.041 p = 0.218 | 19.4 ± 4.01 | H = 1.318 p = 0.517 | 26.19 ± 5.62 | H = 3.038 p = 0.218 | 56.51 ± 4.80 | H = 1.07 p = 0.598 |
| Scoliotic posture | 134% 51.94 | 33.40 ± 6.31 | 19.01 ± 3.31 | 25.80 ± 4.83 | 57.04 ± 4.51 | ||||
| Scoliosis | 8% 3.10 | 29.20 ± 5.31 | 17.54 ± 2.71 | 22.55 ± 4.11 | 56.4 ± 3.72 | ||||
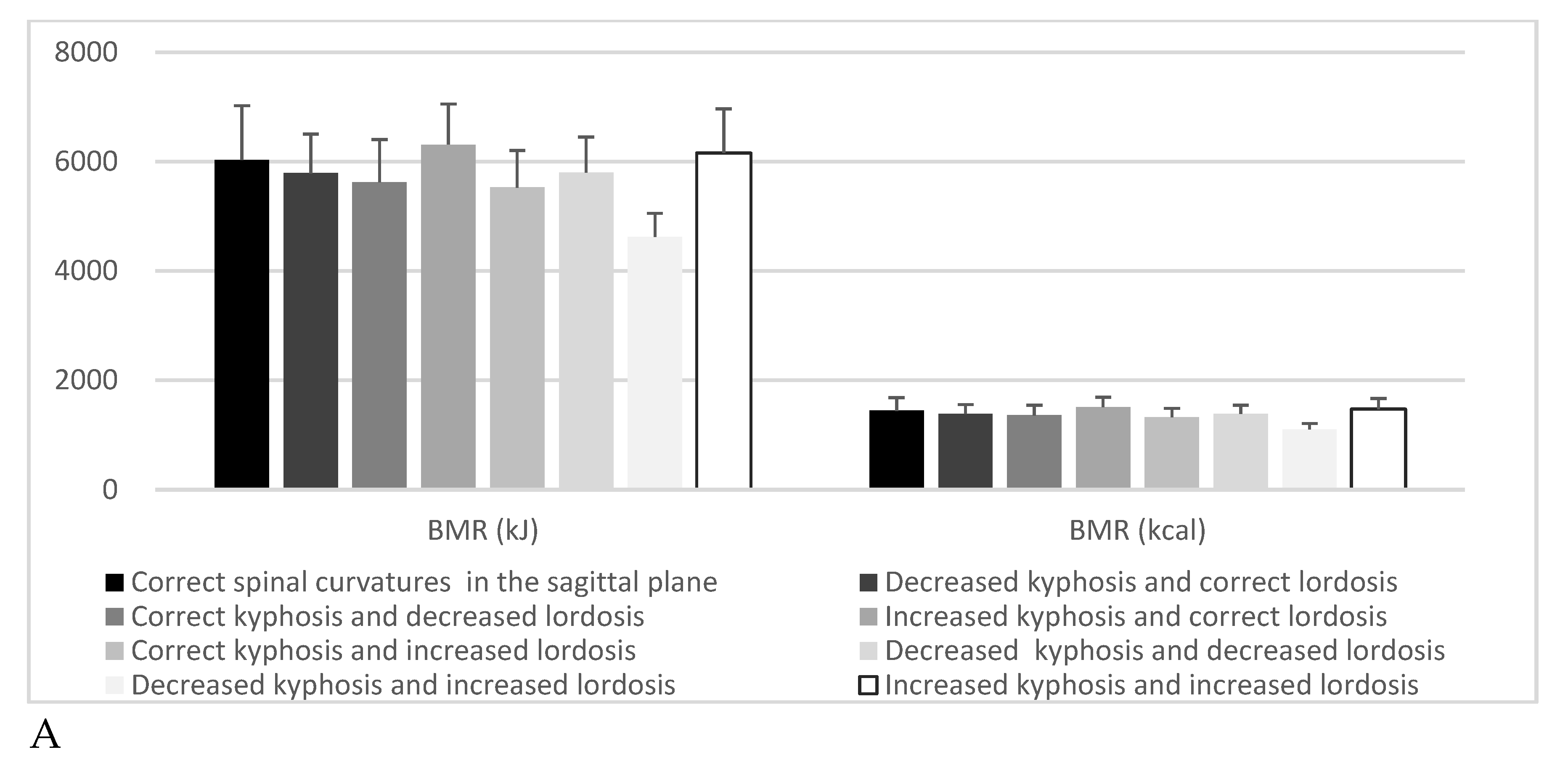
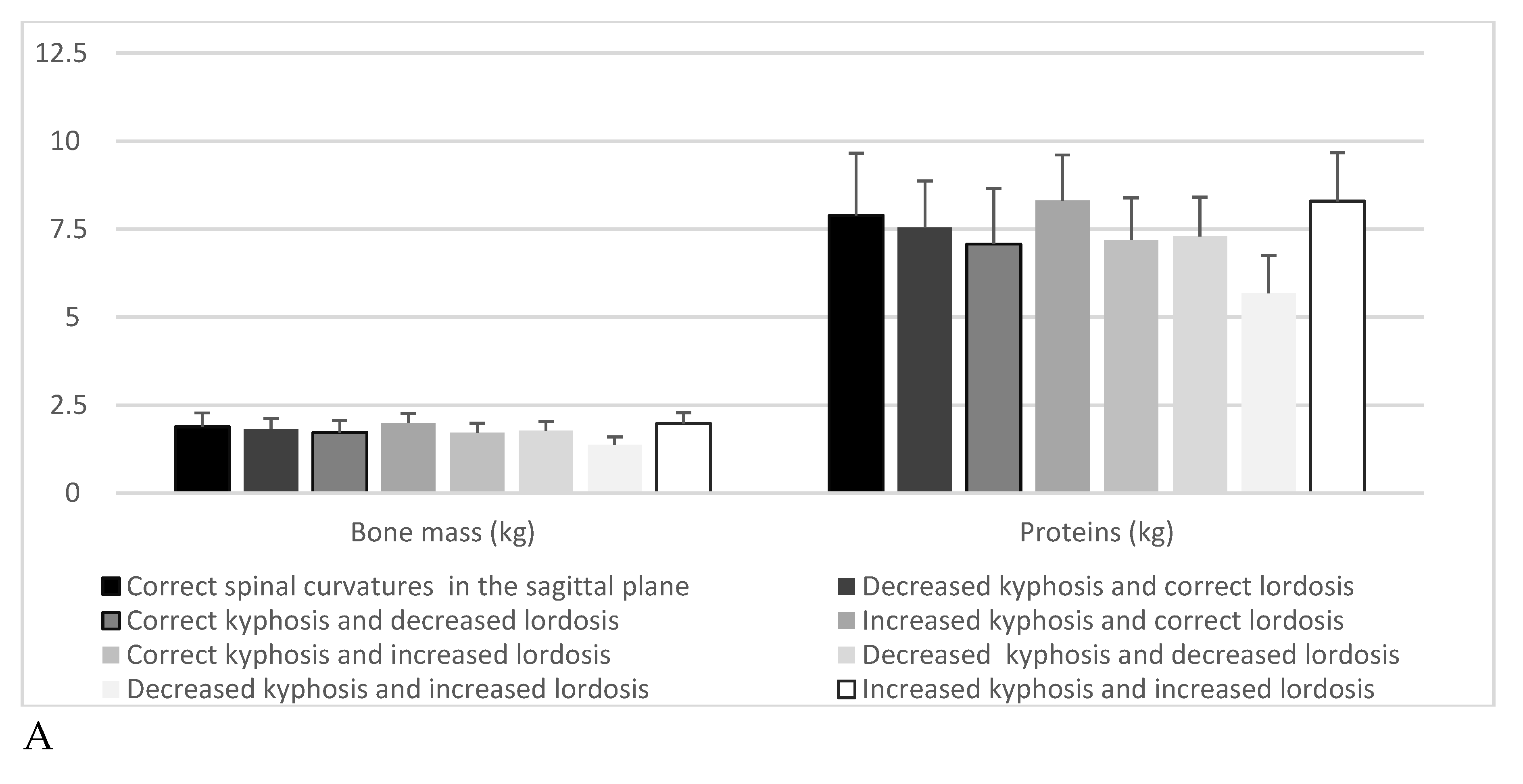
| Variables | N; % | BMR (kJ) | BMR (kcal) | Bone Mass (kg) | Proteins (kg) | ||||
|---|---|---|---|---|---|---|---|---|---|
| X; SD | Kruskal–Wallis Test | X; SD | Kruskal–Wallis Test | X; SD | Kruskal–Wallis Test | X; SD | Kruskal–Wallis Test | ||
| Correct spinal curvatures in the sagittal plane | 106% 41.08 | 6031.08 ± 992.07 | H = 23.04 p = 0.001 | 1441.46 ± 237.11 | H = 22.33 p = 0.002 | 1.89 ± 0.39 | H = 21.86 p = 0.002 | 7.89 ± 1.77 | H = 21.35 p = 0.003 |
| Decreased kyphosis and correct lordosis | 40% 15.50 | 5787.25 ± 715.35 | 1383.18 ± 170.99 | 1.83 ± 0.29 | 7.55 ± 1.32 | ||||
| Correct kyphosis and decreased lordosis | 24% 9.30 | 5625.00 ± 779.26 | 1356.92 ± 182.16 | 1.72 ± 0.35 | 7.08 ± 1.57 | ||||
| Increased kyphosis and correct lordosis | 17% 6.59 | 6310.00 ± 742.34 | 1508.1 ± 177.42 | 1.99 ± 0.28 | 8.31 ± 1.30 | ||||
| Correct kyphosis and increased lordosis | 22% 8.53 | 5525.55 ± 675.08 | 1320.6 ± 161.35 | 1.72 ± 0.27 | 7.19 ± 1.20 | ||||
| Decreased kyphosis and decreased lordosis | 32% 12.40 | 5799.13 ± 649.85 | 1386.0 ± 155.28 | 1.78 ± 0.26 | 7.30 ± 1.11 | ||||
| Decreased kyphosis and increased lordosis | 4% 1.55 | 4620.00 ± 433.80 | 1104.2 ± 103.66 | 1.38 ± 0.22 | 5.68 ± 1.07 | ||||
| Increased kyphosis and increased lordosis | 13% 5.04 | 6155.08 ± 807.30 | 1471.08 ± 192.93 | 1.98 ± 0.31 | 8.30 ± 1.37 | ||||
| Correct posture in the frontal plane | 116% 44.96 | 5948.72 ± 941.73 | H = 2.807 p = 0.245 | 1421.78 ± 225.08 | H = 2.755 p = 0.252 | 1.86 ± 0.37 | H = 2.853 p = 0.240 | 7.73 ± 1.68 | H = 3.065 p = 0.215 |
| Scoliotic posture | 134% 51.94 | 5860.98 ± 800.24 | 1403.06 ± 189.95 | 1.83 ± 0.32 | 7.61 ± 1.46 | ||||
| Scoliosis | 8% 3.10 | 5333.00 ± 792.07 | 1274.63 ± 189.31 | 1.63 ± 0.29 | 6.65 ± 1.20 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wilczyński, J.; Lipińska-Stańczak, M.; Wilczyński, I. Body Posture Defects and Body Composition in School-Age Children. Children 2020, 7, 204. https://doi.org/10.3390/children7110204
Wilczyński J, Lipińska-Stańczak M, Wilczyński I. Body Posture Defects and Body Composition in School-Age Children. Children. 2020; 7(11):204. https://doi.org/10.3390/children7110204
Chicago/Turabian StyleWilczyński, Jacek, Magdalena Lipińska-Stańczak, and Igor Wilczyński. 2020. "Body Posture Defects and Body Composition in School-Age Children" Children 7, no. 11: 204. https://doi.org/10.3390/children7110204
APA StyleWilczyński, J., Lipińska-Stańczak, M., & Wilczyński, I. (2020). Body Posture Defects and Body Composition in School-Age Children. Children, 7(11), 204. https://doi.org/10.3390/children7110204