
Association Between Carbohydrate Quality Index During Pregnancy and Risk for Large-for-Gestational-Age Neonates: Results from the BORN 2020 Study


 , , , and
, , , and 
Abstract
1. Introduction
2. Materials and Methods
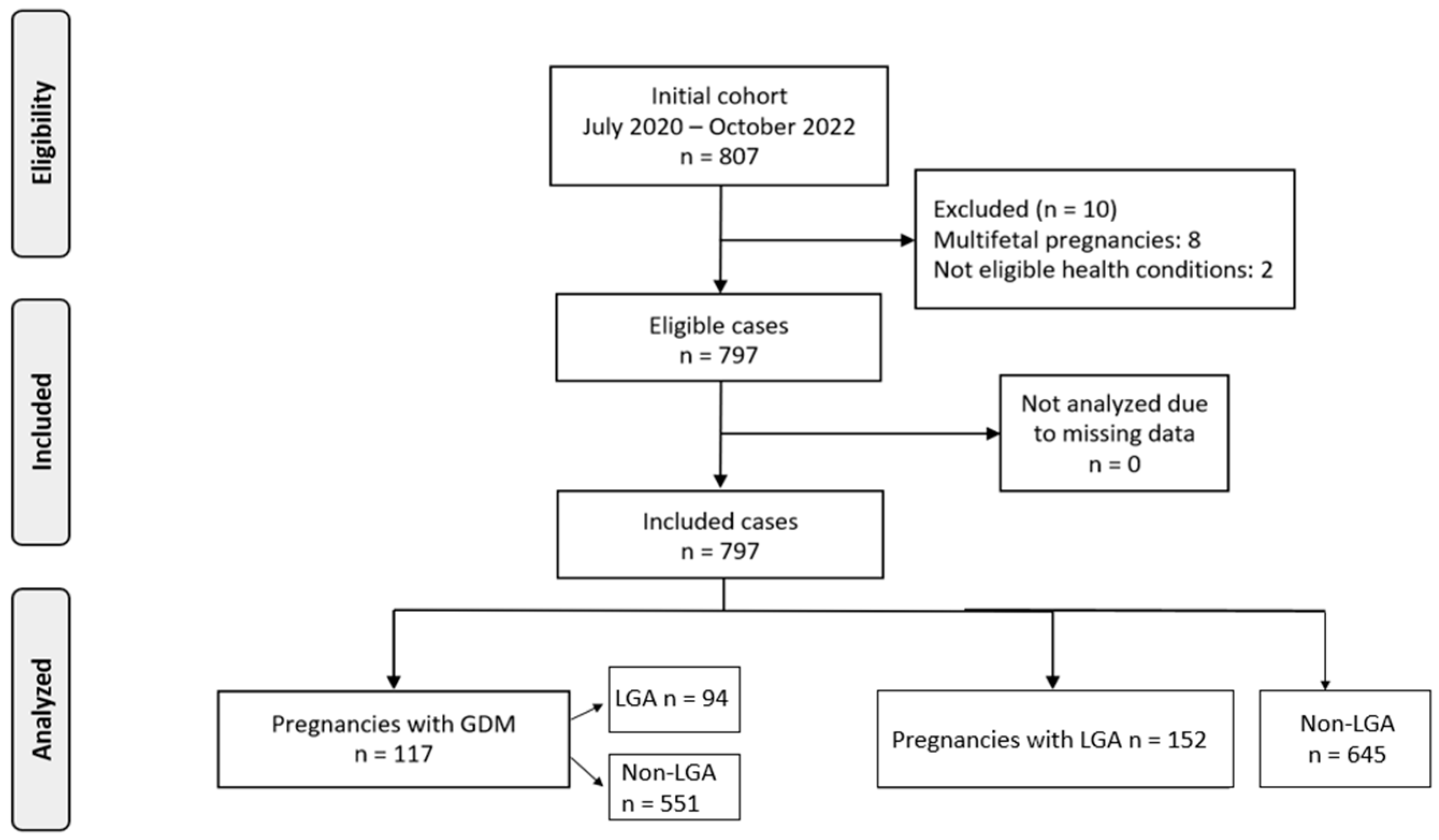
2.1. Study Design and Population
2.2. Dietary Assessment and Carbohydrate Quality Index
2.3. GDM Diagnosis
2.4. Outcome Ascertainment
2.5. Statistical Analysis
3. Results
4. Discussion
4.1. Primary Findings
4.2. Interpretation of the Findings
4.3. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hong, Y.H.; Lee, J.-E. Large for gestational age and obesity-related comorbidities. J. Obes. Metab. Syndr. 2021, 30, 124. [Google Scholar] [CrossRef] [PubMed]
- Ahlsson, F.; Gustafsson, J.; Tuvemo, T.; Lundgren, M. Females born large for gestational age have a doubled risk of giving birth to large for gestational age infants. Acta Paediatr. 2007, 96, 358–362. [Google Scholar] [CrossRef] [PubMed]
- Berntorp, K.; Anderberg, E.; Claesson, R.; Ignell, C.; Källén, K. The relative importance of maternal body mass index and glucose levels for prediction of large-for-gestational-age births. BMC Pregnancy Childbirth 2015, 15, 280. [Google Scholar] [CrossRef] [PubMed]
- Luoto, R.; Kinnunen, T.I.; Aittasalo, M.; Kolu, P.; Raitanen, J.; Ojala, K.; Mansikkamäki, K.; Lamberg, S.; Vasankari, T.; Komulainen, T. Primary prevention of gestational diabetes mellitus and large-for-gestational-age newborns by lifestyle counseling: A cluster-randomized controlled trial. PLoS Med. 2011, 8, e1001036. [Google Scholar] [CrossRef] [PubMed]
- Chawla, R.; Badon, S.E.; Rangarajan, J.; Reisetter, A.C.; Armstrong, L.L.; Lowe, L.P.; Urbanek, M.; Metzger, B.E.; Hayes, M.G.; Scholtens, D.M. Genetic risk score for prediction of newborn adiposity and large-for-gestational-age birth. J. Clin. Endocrinol. Metab. 2014, 99, E2377–E2386. [Google Scholar] [CrossRef] [PubMed]
- Boubred, F.; Pauly, V.; Romain, F.; Fond, G.; Boyer, L. The role of neighbourhood socioeconomic status in large for gestational age. PLoS ONE 2020, 15, e0233416. [Google Scholar] [CrossRef] [PubMed]
- Coustan, D.R.; Lowe, L.P.; Metzger, B.E.; Dyer, A.R. The Hyperglycemia and Adverse Pregnancy Outcome (HAPO) study: Paving the way for new diagnostic criteria for gestational diabetes mellitus. Am. J. Obstet. Gynecol. 2010, 202, 654.e1–654.e6. [Google Scholar] [CrossRef] [PubMed]
- Azoulay, L.; Bouvattier, C.; Christin-Maitre, S. Impact of intra-uterine life on future health. In Annales d’Endocrinologie; Elsevier: Amsterdam, The Netherlands, 2022. [Google Scholar]
- Gluckman, P.D.; Cutfield, W.; Hofman, P.; Hanson, M.A. The fetal, neonatal, and infant environments—The long-term consequences for disease risk. Early Hum. Dev. 2005, 81, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Sakuyama, H.; Katoh, M.; Wakabayashi, H.; Zulli, A.; Kruzliak, P.; Uehara, Y. Influence of gestational salt restriction in fetal growth and in development of diseases in adulthood. J. Biomed. Sci. 2016, 23, 12. [Google Scholar] [CrossRef] [PubMed]
- Öztürk, H.N.O.; Türker, P.F. Fetal programming: Could intrauterin life affect health status in adulthood? Obstet. Gynecol. Sci. 2021, 64, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Danley, S.; Laban, D. The Influence of Maternal Nutrition on Fetal Development and Birth Outcomes. World Sci. News 2025, 200, 63–102. [Google Scholar]
- Dhobale, M. Neurotrophic factors and maternal nutrition during pregnancy. Vitam. Horm. 2017, 104, 343–366. [Google Scholar] [PubMed]
- Sweeting, A.; Mijatovic, J.; Brinkworth, G.D.; Markovic, T.P.; Ross, G.P.; Brand-Miller, J.; Hernandez, T.L. The carbohydrate threshold in pregnancy and gestational diabetes: How low can we go? Nutrients 2021, 13, 2599. [Google Scholar] [CrossRef] [PubMed]
- Filardi, T.; Panimolle, F.; Crescioli, C.; Lenzi, A.; Morano, S. Gestational diabetes mellitus: The impact of carbohydrate quality in diet. Nutrients 2019, 11, 1549. [Google Scholar] [CrossRef] [PubMed]
- Zhang, R.; Han, S.; Chen, G.-C.; Li, Z.-N.; Silva-Zolezzi, I.; Parés, G.V.; Wang, Y.; Qin, L.-Q. Effects of low-glycemic-index diets in pregnancy on maternal and newborn outcomes in pregnant women: A meta-analysis of randomized controlled trials. Eur. J. Nutr. 2018, 57, 167–177. [Google Scholar] [CrossRef] [PubMed]
- Moses, R.G.; Casey, S.A.; Quinn, E.G.; Cleary, J.M.; Tapsell, L.C.; Milosavljevic, M.; Petocz, P.; Brand-Miller, J.C. Pregnancy and Glycemic Index Outcomes study: Effects of low glycemic index compared with conventional dietary advice on selected pregnancy outcomes. Am. J. Clin. Nutr. 2014, 99, 517–523. [Google Scholar] [CrossRef] [PubMed]
- Louie, J.C.Y.; Markovic, T.P.; Perera, N.; Foote, D.; Petocz, P.; Ross, G.P.; Brand-Miller, J.C. A randomized controlled trial investigating the effects of a low–glycemic index diet on pregnancy outcomes in gestational diabetes mellitus. Diabetes Care 2011, 34, 2341–2346. [Google Scholar] [CrossRef] [PubMed]
- Walsh, J.M.; McGowan, C.A.; Mahony, R.; Foley, M.E.; McAuliffe, F.M. Low glycaemic index diet in pregnancy to prevent macrosomia (ROLO study): Randomised control trial. BMJ 2012, 345, e5605. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Liu, Z.; Duan, B.; Zhang, Q.; Zhou, Z.; Liu, W. Effects of a low glycemic index or low glycemic load diet on pregnant women at high risk of gestational diabetes: A meta-analysis of randomized controlled trials. Nutr. Metab. Cardiovasc. Dis. 2023, 33, 2006–2018. [Google Scholar] [CrossRef] [PubMed]
- Schulz, R.; Slavin, J. Perspective: Defining carbohydrate quality for human health and environmental sustainability. Adv. Nutr. 2021, 12, 1108–1121. [Google Scholar] [CrossRef] [PubMed]
- Maghoul, A.; Khonsari, N.M.; Asadi, S.; Abdar, Z.E.; Ejtahed, H.-S.; Qorbani, M. Dietary carbohydrate quality index and cardio-metabolic risk factors. Int. J. Vitam. Nutr. Res. 2023, 94, 377–393. [Google Scholar] [CrossRef] [PubMed]
- Xue, L.; Chen, X.; Sun, J.; Fan, M.; Qian, H.; Li, Y.; Wang, L. Maternal dietary carbohydrate and pregnancy outcomes: Quality over quantity. Nutrients 2024, 16, 2269. [Google Scholar] [CrossRef] [PubMed]
- Apostolopoulou, A.; Tranidou, A.; Tsakiridis, I.; Magriplis, E.; Dagklis, T.; Chourdakis, M. Effects of Nutrition on Maternal Health, Fetal Development, and Perinatal Outcomes. Nutrients 2024, 16, 375. [Google Scholar] [CrossRef] [PubMed]
- Apostolopoulou, A.; Magriplis, E.; Tsekitsidi, E.; Oikonomidou, A.C.; Papaefstathiou, E.; Tsakiridis, I.; Dagklis, T.; Chourdakis, M. Development and validation of a short culture-specific food frequency questionnaire for Greek pregnant women and their adherence to the Mediterranean diet. Nutrition 2021, 90, 111357. [Google Scholar] [CrossRef] [PubMed]
- Tsagkari, A.; Pateras, K.; Ladopoulou, D.; Kornarou, E.; Vlachadis, N. Birthweight by gestational age reference centile charts for Greek neonates. medRxiv 2020. [Google Scholar] [CrossRef]
- Mao, K.; Gao, Y.; Li, S.; Chi, L. A retrospective cohort study on the influencing factors for macrosomia in singleton pregnancies. Medicine 2024, 103, e34743. [Google Scholar] [CrossRef] [PubMed]
- Jenabi, E.; Salehi, A.M.; Farashi, S.; Salimi, Z. The environmental risk factors associated with fetal macrosomia: An umbrella review. Pediatr. Neonatol. 2024, 65, 217–221. [Google Scholar] [CrossRef] [PubMed]
- Alfadhli, E.M. Maternal obesity influences birth weight more than gestational diabetes. BMC Pregnancy Childbirth 2021, 21, 111. [Google Scholar] [CrossRef] [PubMed]
- Song, X.; Shu, J.; Zhang, S.; Chen, L.; Diao, J.; Li, J.; Li, Y.; Wei, J.; Liu, Y.; Sun, M. Pre-pregnancy body mass index and risk of macrosomia and large for gestational age births with gestational diabetes mellitus as a mediator: A prospective cohort study in Central China. Nutrients 2022, 14, 1072. [Google Scholar] [CrossRef] [PubMed]
- Group, H.S.C.R. Hyperglycaemia and Adverse Pregnancy Outcome (HAPO) Study: Associations with maternal body mass index. BJOG Int. J. Obstet. Gynaecol. 2010, 117, 575–584. [Google Scholar]
- Fernández-González, E.; Martínez-González, M.Á.; Bes-Rastrollo, M.; Suescun-Elizalde, D.; Basterra-Gortari, F.J.; Santiago, S.; Gea, A. Association between pre-conceptional carbohydrate quality index and the incidence of gestational diabetes: The SUN cohort study. Br. J. Nutr. 2023, 129, 704–714. [Google Scholar] [CrossRef] [PubMed]
- Siargkas, A.; Tranidou, A.; Magriplis, E.; Tsakiridis, I.; Apostolopoulou, A.; Xenidis, T.; Pazaras, N.; Chourdakis, M.; Dagklis, T. Impact of Maternal Macronutrient Intake on Large for Gestational Age Neonates’ Risk Among Women with Gestational Diabetes Mellitus: Results from the Greek BORN2020 Cohort. Nutrients 2025, 17, 269. [Google Scholar] [CrossRef] [PubMed]
- Louie, J.C.Y.; Markovic, T.P.; Ross, G.P.; Foote, D.; Brand-Miller, J.C. Effect of a low glycaemic index diet in gestational diabetes mellitus on post-natal outcomes after 3 months of birth: A pilot follow-up study. Matern. Child Nutr. 2015, 11, 409–414. [Google Scholar] [CrossRef] [PubMed]
- Pittyanont, S.; Suriya, N.; Sirilert, S.; Tongsong, T. Comparisons of the Rates of Large-for-Gestational-Age Newborns between Women with Diet-Controlled Gestational Diabetes Mellitus and Those with Non-Gestational Diabetes Mellitus. Clin. Pract. 2024, 14, 536–545. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Variable | Non-LGA N = 645 | LGA N = 152 | p-Value | GDM Non-LGA N = 94 | GDM with LGA N = 23 | p Value |
|---|---|---|---|---|---|---|
| Maternal age | 32.41 (±4.97) | 32.4 (±4.48) | 0.98 | 34.39 (±4.72) | 33.17 (±3.2) | 0.24 |
| Maternal age > 35 | 191 (29.61%) | 46 (30.26%) | 0.95 | 44 (46.81%) | 7 (30.43%) | 0.24 |
| Weight | 63 (57, 72) | 66 (60, 77) | p < 0.001 *** | 64.5 (58.25, 78) | 68 (63.5, 80.5) | 0.16 |
| Height | 165 (161, 170) | 167 (162.75, 170) | 0.006 ** | 164.7 (±6.28) | 168.22 (±6.15) | 0.017 * |
| BMI before pregnancy | 22.7 (20.7, 25.8) | 23.8 (21.6, 27.42) | 0.004 ** | 23.55 (21.62, 28.43) | 24.7 (22.65, 28.75) | 0.45 |
| BMI before pregnancy > 25 | 196 (30.39%) | 64 (42.11%) | 0.007 ** | 36 (38.3%) | 10 (43.48%) | 0.83 |
| BMI before pregnancy > 30 | 76 (11.78%) | 24 (15.79%) | 0.23 | 21 (22.34%) | 4 (17.39%) | 0.81 |
| Parity 0 1 2 3 4 | 339 (52.56%) 234 (36.28%) 62 (9.61%) 8 (1.24%) 2 (0.31%) | 68 (44.74%) 63 (41.45%) 19 (12.5%) 2 (1.32%) 0 (0%) | 0.1 0.27 0.36 1 - | 52 (55.32%) 32 (34.04%) 9 (9.57%) 1 (1.06%) | 8 (34.78%) 12 (52.17%) 3 (13.04%) 0 (0%) | 0.13 0.17 0.91 - |
| Smoking | 69 (10.7%) | 12 (7.89%) | 0.38 | 18 (19.15%) | 3 (13.04%) | 0.7 |
| ART | 49 (7.6%) | 10 (6.58%) | 0.8 | 9 (9.57%) | 2 (8.7%) | 0.1 |
| Thyroid disease | 89 (13.8%) | 17 (11.18%) | 0.47 | 9 (9.57%) | 4 (17.39%) | 0.48 |
| GDM | 94 (14.57%) | 23 (15.13%) | 0.96 | 94 (100%) | 23 (100%) | - |
| CQI for LGA in Total Population | ||||||
|---|---|---|---|---|---|---|
| Models | Low | Moderate | High | |||
| aOR (95% CI) | p-Value | aOR (95% CI) | p-Value | p for Trend | ||
| Model 1 | reference | 1.6 (1.03, 2.5) | 0.037 * | 1.29 (0.81, 2.07) | 0.28 | 0.23 |
| Model 2 | reference | 1.57 (1.01, 2.46) | 0.046 * | 1.26 (0.78, 2.02) | 0.33 | 0.28 |
| Model 3 | reference | 1.58 (1.01, 2.47) | 0.044 * | 1.26 (0.79, 2.03) | 0.33 | 0.28 |
| Model 4 | reference | 1.7 (1.08, 2.72) | 0.023 * | 1.44 (0.86, 2.4) | 0.16 | 0.12 |
| CQI for LGA in GDM | ||||||
| Models | Low | Moderate | High | p for Trend | ||
| aOR (95% CI) | p-Value | aOR (95% CI) | p-Value | |||
| Model 1 | reference | 3.85 (0.72, 31.93) | 0.15 | 6.74 (1.32, 56.66) | 0.039 * | 0.041 * |
| Model 2 | reference | 3.81 (0.71, 32.02) | 0.15 | 6.64 (1.27, 57.48) | 0.044 * | 0.045 * |
| Model 3 | reference | 3.56 (0.65, 30.04) | 0.18 | 6.27 (1.2, 54.33) | 0.051 | 0.052 |
| Model 4 | reference | 1.9 (0.28, 18.14) | 0.53 | 3.05 (0.47, 30.22) | 0.28 | 0.3 |
| Variable | Tertile/Group | LGA | GDM with LGA | ||||
|---|---|---|---|---|---|---|---|
| aOR (95% CI) | p-Value | Power | aOR (95% CI) | p-Value | Power | ||
| Glycemic index (GI) | T2 (medium) | 0.95 (0.61, 1.5) | 0.85 | 0.135 | 0.76 (0.19, 2.76) | 0.68 | 0.552 |
| T3 (high) | 0.79 (0.49–1.28) | 0.36 | 0.994 | 0.45 (0.07, 2.15) | 0.34 | 1 | |
| Dietary fiber | T2 (medium) | 1.38 (0.87, 2.22) | 0.17 | 1 | 2.18 (0.43, 13.5) | 0.36 | 1 |
| T3 (high) | 1.25 (0.71, 2.2) | 0.43 | 0.994 | 3.15 (0.59, 20.6) | 0.19 | 1 | |
| Solid/Total carb ratio | T2 (medium) | 0.98 (0.62, 1.55) | 0.96 | 0.056 | 0.55 (0.13, 2.16) | 0.4 | 0.994 |
| T3 (high) | 1.24 (0.79, 1.95) | 0.34 | 0.992 | 0.66 (0.16, 2.48) | 0.55 | 0.87 | |
| Whole/Total grain ratio | T2 (medium) | 1.31 (0.83, 2.03) | 0.23 | 1 | 2.3 (0.49, 12.28) | 0.3 | 1 |
| T3 (high) | 1.21 (0.76, 1.91) | 0.41 | 0.969 | 2.29 (0.55, 11.38) | 0.27 | 1 | |
| Carbohydrate Quality Index in LGA | |||
|---|---|---|---|
| Low | Moderate | High | |
| Carbohydrate Intake (% E) | |||
| ≤40% | reference | reference | reference |
| 40–50% | 1.78 (0.83, 3.82), p = 0.14 | 1.18 (0.57, 2.46), p = 0.65 | 0.87 (0.4, 1.88), p = 0.73 |
| ≥50% | 4.25 (1.53, 11.67), p = 0.005 * | 1.63 (0.69, 3.81), p = 0.25 | 0.53 (0.16, 1.52), p = 0.26 |
| Carbohydrate Quality Index in GDM with LGA | |||
| Carbohydrate Intake (% E) | |||
| ≤40% | reference | reference | reference |
| 40–50% | 6.14 × 10−10 (-,-), p = 0.1 | - (-,-), p = 0.1 | 1.12 (0.11, 10.47), p = 0.92 |
| ≥50% | 0.01 (-,-), p = 0.1 | - (-,-), p = 0.1 | 4.05 (0.13, 165.61), p = 0.43 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tranidou, A.; Siargkas, A.; Tsakiridis, I.; Magriplis, E.; Apostolopoulou, A.; Chourdakis, M.; Dagklis, T. Association Between Carbohydrate Quality Index During Pregnancy and Risk for Large-for-Gestational-Age Neonates: Results from the BORN 2020 Study. Children 2025, 12, 955. https://doi.org/10.3390/children12070955
Tranidou A, Siargkas A, Tsakiridis I, Magriplis E, Apostolopoulou A, Chourdakis M, Dagklis T. Association Between Carbohydrate Quality Index During Pregnancy and Risk for Large-for-Gestational-Age Neonates: Results from the BORN 2020 Study. Children. 2025; 12(7):955. https://doi.org/10.3390/children12070955
Chicago/Turabian StyleTranidou, Antigoni, Antonios Siargkas, Ioannis Tsakiridis, Emmanouela Magriplis, Aikaterini Apostolopoulou, Michail Chourdakis, and Themistoklis Dagklis. 2025. "Association Between Carbohydrate Quality Index During Pregnancy and Risk for Large-for-Gestational-Age Neonates: Results from the BORN 2020 Study" Children 12, no. 7: 955. https://doi.org/10.3390/children12070955
APA StyleTranidou, A., Siargkas, A., Tsakiridis, I., Magriplis, E., Apostolopoulou, A., Chourdakis, M., & Dagklis, T. (2025). Association Between Carbohydrate Quality Index During Pregnancy and Risk for Large-for-Gestational-Age Neonates: Results from the BORN 2020 Study. Children, 12(7), 955. https://doi.org/10.3390/children12070955