
Telomere Length and Emotional and Behavioral Problems in Children from the Prospective Birth Cohort INfancia y Medio Ambiente (INMA) Study

 ,
,  ,
,  ,
,  , , ,
, , , 
Abstract
1. Introduction
2. Materials and Methods
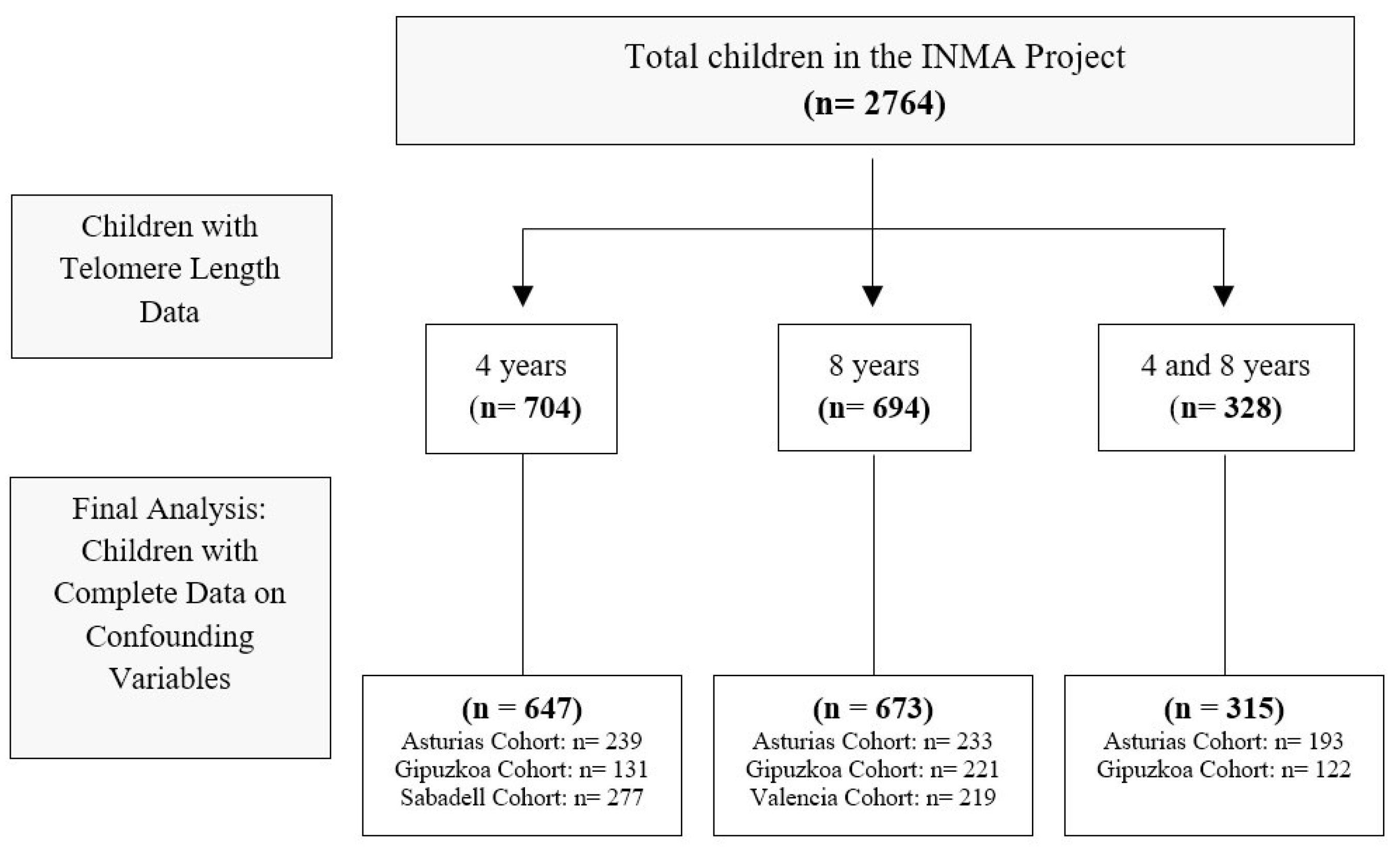
2.1. Study Design and Population
2.2. Study Variables
2.2.1. Telomere Length
2.2.2. Emotional and Behavioral Problems
2.2.3. Covariates
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| TL | telomere length |
| INMA | INfancia y Medio Ambiente (Childhood and Environment) |
| qPCR | quantitative polymerase chain reaction |
| T | telomere |
| S | single-copy gene |
| T/S | ratio of telomere copy number to the number of single-copy genes |
| ICC | intraclass correlation coefficients |
| SDQ | Strengths and Difficulties Questionnaire |
| BMI | body mass index |
| IQR | interquartile range |
| ZINB | zero-inflated negative binomial |
| NB | negative binomial |
| OR | odds ratio |
| IRR | incidence rate ratios |
| y | years |
| CBCL | Child Behavior Checklist |
| DNA | deoxyribonucleic acid |
References
- Sahin, E.; Colla, S.; Liesa, M.; Moslehi, J.; Müller, F.L.; Guo, M.; Cooper, M.; Kotton, D.; Fabian, A.J.; Walkey, C.; et al. Telomere dysfunction induces metabolic and mitochondrial compromise. Nature 2011, 470, 359–365. [Google Scholar] [CrossRef] [PubMed]
- O’Sullivan, R.J.; Karlseder, J. Telomeres: Protecting chromosomes against genome instability. Nat. Rev. Mol. Cell Biol. 2010, 11, 171–181. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Zhan, Y.; Pedersen, N.L.; Fang, F.; Hägg, S. Telomere Length and All-Cause Mortality: A Meta-analysis. Ageing Res. Rev. 2018, 48, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Codd, V.; Wang, Q.; Allara, E.; Musicha, C.; Kaptoge, S.; Stoma, S.; Jiang, T.; Hamby, S.E.; Braund, P.S.; Bountziouka, V.; et al. Polygenic basis and biomedical consequences of telomere length variation. Nat. Genet. 2021, 53, 1425–1433. [Google Scholar] [CrossRef]
- López-Otín, C.; Blasco, M.A.; Partridge, L.; Serrano, M.; Kroemer, G. Hallmarks of aging: An expanding universe. Cell 2023, 186, 243–278. [Google Scholar] [CrossRef]
- Powell, T.R.; De Jong, S.; Breen, G.; Lewis, C.M.; Dima, D. Telomere length as a predictor of emotional processing in the brain. Hum. Brain Mapp. 2019, 40, 1750–1759. [Google Scholar] [CrossRef]
- Epel, E.S. Telomeres in a Life-Span Perspective: A New “Psychobiomarker”? Curr. Dir. Psychol. Sci. 2009, 18, 6–10. [Google Scholar] [CrossRef]
- Achenbach, T.M.; Ivanova, M.Y.; Rescorla, L.A.; Turner, L.V.; Althoff, R.R. Internalizing/Externalizing Problems: Review and Recommendations for Clinical and Research Applications. J. Am. Acad. Child. Adolesc. Psychiatry 2016, 55, 647–656. [Google Scholar] [CrossRef]
- Aymerich, C.; Pedruzo, B.; Pacho, M.; Herrero, J.; Laborda, M.; Bordenave, M.; de Pablo, G.S.; Sesma, E.; Fernández-Rivas, A.; Catalan, A.; et al. Relationship between elimination disorders and internalizing-externalizing problems in children: A systematic review and meta-analysis. JCPP Adv. 2023, 3, e12185. [Google Scholar] [CrossRef]
- Vasileva, M.; Graf, R.K.; Reinelt, T.; Petermann, U.; Petermann, F. Research review: A meta-analysis of the international prevalence and comorbidity of mental disorders in children between 1 and 7 years. J. Child. Psychol. Psychiatry 2021, 62, 372–381. [Google Scholar] [CrossRef]
- Malouff, J.M.; Schutte, N.S. A meta-analysis of the relationship between anxiety and telomere length. Anxiety Stress Coping 2017, 30, 264–272. [Google Scholar] [CrossRef] [PubMed]
- Shalev, I.; Moffitt, T.E.; Braithwaite, A.W.; Danese, A.; Fleming, N.I.; Goldman-Mellor, S.; Harrington, H.L.; Houts, R.M.; Israel, S.; Poulton, R.; et al. Internalizing disorders and leukocyte telomere erosion: A prospective study of depression, generalized anxiety disorder and post-traumatic stress disorder. Mol. Psychiatry 2014, 19, 1163–1170. [Google Scholar] [CrossRef] [PubMed]
- Ridout, K.K.; Ridout, S.J.; Price, L.H.; Sen, S.; Tyrka, A.R. Depression and telomere length: A meta-analysis. J. Affect. Disord. 2016, 191, 237–247. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, C.H.; Epel, E.; Adler, N.; Bush, N.R.; Obradovic, J.; Lin, J.; Blackburn, E.; Stamperdahl, J.L.; Boyce, W.T. Autonomic and adrenocortical reactivity and buccal cell telomere length in kindergarten children. Psychosom. Med. 2011, 73, 533–540. [Google Scholar] [CrossRef]
- Wade, M.; Fox, N.A.; Zeanah, C.H.; Nelson, C.A.; Drury, S.S. Telomere Length and Psychopathology: Specificity and Direction of Effects Within the Bucharest Early Intervention Project. J. Am. Acad. Child. Adolesc. Psychiatry 2020, 59, 140–148.e3. [Google Scholar] [CrossRef]
- Robinson, O.; Lau, C.E.; Joo, S.; Andrusaityte, S.; Borras, E.; de Prado-Bert, P.; Chatzi, L.; Keun, H.C.; Grazuleviciene, R.; Gutzkow, K.B.; et al. Associations of four biological age markers with child development: A multi-omic analysis in the European HELIX cohort. Elife 2023, 12, e85104. [Google Scholar] [CrossRef]
- Wojcicki, J.M.; Heyman, M.B.; Elwan, D.; Shiboski, S.; Lin, J.; Blackburn, E.; Epel, E. Telomere length is associated with oppositional defiant behavior and maternal clinical depression in Latino preschool children. Transl. Psychiatry 2015, 5, e581. [Google Scholar] [CrossRef]
- Tien, J.; Lewis, G.D.; Liu, J. Prenatal risk factors for internalizing and externalizing problems in childhood. World J. Pediatr. 2020, 16, 341–355. [Google Scholar] [CrossRef]
- Kovess-Masfety, V.; Husky, M.M.; Keyes, K.; Hamilton, A.; Pez, O.; Bitfoi, A.; Carta, M.G.; Goelitz, D.; Kuijper, R.; Otten, R.; et al. Comparing the prevalence of mental health problems in children 6–11 across Europe. Soc. Psychiatry Psychiatr. Epidemiol. 2016, 51, 1093–1103. [Google Scholar] [CrossRef]
- Guxens, M.; Ballester, F.; Espada, M.; Fernández, M.F.; Grimalt, J.O.; Ibarluzea, J.; Olea, N.; Rebagliato, M.; Tardón, A.; Torrent, M.; et al. Cohort Profile: The INMA—INfancia y Medio Ambiente—(Environment and Childhood) Project. Int. J. Epidemiol. 2012, 41, 930–940. [Google Scholar] [CrossRef]
- Cawthon, R.M. Telomere length measurement by a novel monochrome multiplex quantitative PCR method. Nucleic. Acids Res. 2009, 37, e21. [Google Scholar] [CrossRef] [PubMed]
- Hellemans, J.; Mortier, G.; De Paepe, A.; Speleman, F.; Vandesompele, J. QBase Relative Quantification Framework and Software for Management and Automated Analysis of Real-Time Quantitative PCR Data. Genome Biol. 2007, 8, R19. [Google Scholar] [CrossRef] [PubMed]
- Telomere Research Network. Study Design & Analysis. Available online: https://trn.tulane.edu/resources/study-design-analysis/ (accessed on 10 June 2025).
- Verhulst, S. Improving comparability between qPCR-based telomere studies. Mol. Ecol. Resour. 2020, 20, 11–13. [Google Scholar] [CrossRef]
- Goodman, R. The Strengths and Difficulties Questionnaire: A research note. J. Child. Psychol. Psychiatry. 1997, 38, 581–586. [Google Scholar] [CrossRef]
- Rodríguez-Hernández, P.; Betancort, M.; de la Fuente, J.M.; Calpena, E.; Martín, A.; Rodríguez, R. Psychometric properties of the parent and teacher versions of the Strengths and Difficulties Questionnaire (SDQ) in a Spanish sample. Int. J. Clin. Health Psychol. 2012, 12, 265–279. [Google Scholar]
- Demanelis, K.; Jasmine, F.; Chen, L.S.; Chernoff, M.; Tong, L.; Delgado, D.; Zhang, C.; Shinkle, J.; Sabarinathan, M.; Lin, H.; et al. Determinants of telomere length across human tissues. Science 2020, 369, eaaz6876. [Google Scholar] [CrossRef]
- Likhar, A.; Baghel, P.; Patil, M. Early Childhood Development and Social Determinants. Cureus 2022, 14, e29500. [Google Scholar] [CrossRef]
- Ferschmann, L.; Bos, M.G.N.; Herting, M.M.; Mills, K.L.; Tamnes, C.K. Contextualizing adolescent structural brain development: Environmental determinants and mental health outcomes. Curr. Opin. Psychol. 2022, 44, 170–176. [Google Scholar] [CrossRef]
- Zuur, A.F.; Saveliev, A.A.; Ieno, E.N. Zero Inflated Models and Generalized Linear Mixed Models with R; Highland Statistics Ltd.: Newburgh, UK, 2012; p. 324. (Highland Statistics Ltd. book series). [Google Scholar]
- Wolkowitz, O.M.; Mellon, S.H.; Epel, E.S.; Lin, J.; Dhabhar, F.S.; Su, Y.; Reus, V.I.; Rosser, R.; Burke, H.M.; Kupferman, E.; et al. Leukocyte Telomere Length in Major Depression: Correlations with Chronicity, Inflammation and Oxidative Stress—Preliminary Findings. PLoS ONE 2011, 6, e17837. [Google Scholar] [CrossRef]
- Phillips, A.C.; Robertson, T.; Carroll, D.; Der, G.; Shiels, P.G.; McGlynn, L.; Benzeval, M. Do symptoms of depression predict telomere length? Evidence from the west of Scotland twenty-07 study. Psychosom. Med. 2013, 75, 288–296. [Google Scholar] [CrossRef]
- Martens, D.S.; Van Der Stukken, C.; Derom, C.; Thiery, E.; Bijnens, E.M.; Nawrot, T.S. Newborn Telomere Length Predicts Later Life Telomere Length: Tracking Telomere Lengthfrom Birth to Child- and Adulthood. EBioMedicine 2021, 63, 103164. [Google Scholar] [CrossRef] [PubMed]
- Martens, D.S.; Janssen, B.G.; Bijnens, E.M.; Clemente, D.B.P.; Vineis, P.; Plusquin, M.; Nawrot, T.S. Association of Parental Socioeconomic Status and Newborn TelomereLength. JAMA Netw. Open 2020, 3, e204057. [Google Scholar] [CrossRef]

{kind=link}
| Study Variables | Measures at 4 y (n = 647) | Measures at 8 y (n = 673) | Measures at Both 4 y and 8 y (n = 315) |
|---|---|---|---|
| Cohort, n (%) | |||
| Asturias | 240 (37.1) | 234 (34.8) | 193 (61.3) |
| Gipuzkoa | 131 (20.2) | 220 (32.7) | 122 (38.7) |
| Sabadell | 277 (42.7) | - | - |
| Valencia | - | 219 (32.5) | - |
| Mother characteristics | |||
| Age, median (IQR) | 31.0 (29.0–34.0) | 31.0 (29.0–34.0) | 32.0 (30.0–35.0) |
| Educational Level, n (%) | |||
| Primary or less | 120 (18.5) | 122 (18.1) | 47 (14.9) |
| Secondary | 274 (42.3) | 273 (40.6) | 125 (39.7) |
| University | 254 (39.2) | 278 (41.3) | 143 (45.4) |
| Preconceptional BMI, median (IQR) | 22.9 (20.8–25.6) | 22.7 (20.7–25.6) | 22.8 (20.6–25.3) |
| Smoking during pregnancy, n (%) | |||
| Yes | 166 (25.6) | 200 (29.7) | 81 (25.7) |
| No | 482 (74.4) | 473 (70.3) | 234 (74.3) |
| Children characteristics | |||
| Sex, n (%) | |||
| Males | 331 (51.1) | 347 (51.6) | 163 (51.7) |
| Females | 317 (48.9) | 326 (48.4) | 152 (48.3) |
| BMI at 4 years, median (IQR) | 15.9 (15.2–16.9) | - | 16.1 (15.3–17.2) |
| BMI at 8 years, median (IQR) | 16.7 (15.4–18.5) | 17.0 (15.7–18.8) | 17.0 (15.7–18.9) |
| Leukocyte Telomere Length | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| 4 Years (n = 647) a | 8 Years (n = 673) b | Change 4–8 Years (n = 315) c | |||||||
| Emotional and Behavioral Problems at 8 Years | Estimate (95% CI) | p-Value | I2 (%) | Estimate (95% CI) | p-Value | I2 (%) | Estimate (95% CI) | p-Value | I2 (%) |
| Internalizing problems a | |||||||||
| Count (OR) | 0.92 (0.54; 1.55) | 0.753 | 34.1 | 0.72 (0.29; 1.82) | 0.418 | 0.0 | 0.34 (0.06; 2.10) | 0.263 | 0.0 |
| IRR | 1.02 (0.95; 1.09) | 0.635 | 30.3 | 1.01 (0.95; 1.08) | 0.663 | 0.0 | 1.06 (0.94; 1.19) | 0.315 | 38.6 |
| Externalizing problems (IRR) | 0.97 (0.92; 1.03) | 0.317 | 37.4 | 1.03 (0.99; 1.09) | 0.146 | 4.0 | 0.98 (0.87; 1.11) | 0.784 | 49.1 |
| Total score (IRR) | 0.99 (0.94; 1.03) | 0.582 | 48.2 | 1.03 (0.98; 1.08) | 0.232 | 30.3 | 0.98 (0.87; 1.11) | 0.818 | 48.2 |
| Leukocyte Telomere Length | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| 4 Years (n = 317) a | 8 Years (n = 326) b | Change 4–8 Years (n = 152) c | |||||||
| Emotional and Behavioral Problems at 8 Years | Estimate (95% CI) | p-Value | I2 (%) | Estimate (95% CI) | p-Value | I2 (%) | Estimate (95% CI) | p-Value | I2 (%) |
| Internalizing problems a | |||||||||
| Count (OR) | 0.88 (0.47; 1.63) | 0.679 | 45.8 | 1.64 (0.60; 4.45) | 0.330 | 33.1 | 0.87 (0.25; 3.00) | 0.826 | 0.0 |
| IRR | 0.90 (0.70; 1.16) | 0.414 | 82.0 | 1.08 (0.98; 1.19) | 0.113 | 32.6 | 0.98 (0.84; 1.16) | 0.880 | 47.0 |
| Externalizing problems (IRR) | 0.93 (0.86; 1.01) | 0.093 | 38.0 | 1.05 (0.94; 1.20) | 0.324 | 63.5 | 0.96 (0.84; 1.10) | 0.565 | 43.4 |
| Total score (IRR) | 0.91 (0.78; 1.07) | 0.261 | 78.3 | 1.07 (0.95; 1.21) | 0.289 | 67.5 | 0.97 (0.80; 1.16) | 0.720 | 63.7 |
| Leukocyte Telomere Length | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| 4 Years (n = 330) a | 8 Years (n = 347) b | Change 4–8 Years (n = 163) c | |||||||
| Emotional and Behavioral Problems at 8 Years | Estimate (95% CI) | p-Value | I2 (%) | Estimate (95% CI) | p-Value | I2 (%) | Estimate (95% CI) | p-Value | I2 (%) |
| Internalizing problems a | |||||||||
| Count (OR) | 1.15 (0.73; 1.78) | 0.541 | 0.0 | 0.85 (0.47; 1.52) | 0.586 | 0.0 | 1.00 (0.48; 2.10) | 0.999 | 0.0 |
| IRR | 1.01 (0.98; 1.20) | 0.100 | 0.0 | 0.96 (0.88; 1.05) | 0.416 | 0.0 | 1.10 (0.94; 1.31) | 0.230 | 0.0 |
| Externalizing problems (IRR) | 1.04 (0.97; 1.11) | 0.258 | 0.0 | 1.02 (0.96; 1.09) | 0.444 | 0.0 | 1.01 (0.90; 1.14) | 0.817 | 0.0 |
| Total score (IRR) | 1.06 (0.99; 1.13) | 0.079 | 0.0 | 1.00 (0.94; 1.06) | 0.936 | 0.0 | 1.05 (0.93; 1.17) | 0.428 | 0.0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Campos-Sánchez, I.; Navarrete-Muñoz, E.M.; Barber-Valles, J.X.; Martens, D.S.; Riaño-Galán, I.; Irizar, A.; Llop, S.; Guxens, M.; Rodríguez-Dehli, C.; Babarro, I.; et al. Telomere Length and Emotional and Behavioral Problems in Children from the Prospective Birth Cohort INfancia y Medio Ambiente (INMA) Study. Children 2025, 12, 875. https://doi.org/10.3390/children12070875
Campos-Sánchez I, Navarrete-Muñoz EM, Barber-Valles JX, Martens DS, Riaño-Galán I, Irizar A, Llop S, Guxens M, Rodríguez-Dehli C, Babarro I, et al. Telomere Length and Emotional and Behavioral Problems in Children from the Prospective Birth Cohort INfancia y Medio Ambiente (INMA) Study. Children. 2025; 12(7):875. https://doi.org/10.3390/children12070875
Chicago/Turabian StyleCampos-Sánchez, Irene, Eva María Navarrete-Muñoz, Josep Xavier Barber-Valles, Dries S. Martens, Isolina Riaño-Galán, Amaia Irizar, Sabrina Llop, Mónica Guxens, Cristina Rodríguez-Dehli, Izaro Babarro, and et al. 2025. "Telomere Length and Emotional and Behavioral Problems in Children from the Prospective Birth Cohort INfancia y Medio Ambiente (INMA) Study" Children 12, no. 7: 875. https://doi.org/10.3390/children12070875
APA StyleCampos-Sánchez, I., Navarrete-Muñoz, E. M., Barber-Valles, J. X., Martens, D. S., Riaño-Galán, I., Irizar, A., Llop, S., Guxens, M., Rodríguez-Dehli, C., Babarro, I., Lozano, M., Vrijheid, M., Nawrot, T., & Valera-Gran, D. (2025). Telomere Length and Emotional and Behavioral Problems in Children from the Prospective Birth Cohort INfancia y Medio Ambiente (INMA) Study. Children, 12(7), 875. https://doi.org/10.3390/children12070875