Influence of Physical Activity in Children and Adolescents with Cerebral Palsy: A Systematic Review

 , , , and
, , , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Design
2.2. Sources of Information
2.3. Selection Criteria
- The inclusion criteria contemplated empirical studies or interventions focused on PA, published in any language, whose sample is composed of persons with CP between the ages of 0 and 20 years. Also included were studies that analyzed factors that influence the practice of PA, as well as those that presented methodologies or tools aimed at promoting PA and its benefits.
- On the other hand, the exclusion criteria discarded those articles derived directly from the inclusion criteria, studies published after 2024, synthesis studies, those comparing people with CP to people without disabilities or other disabilities, reliability studies of research instruments, and those in which the age of the participants was not accurately specified.
3. Results
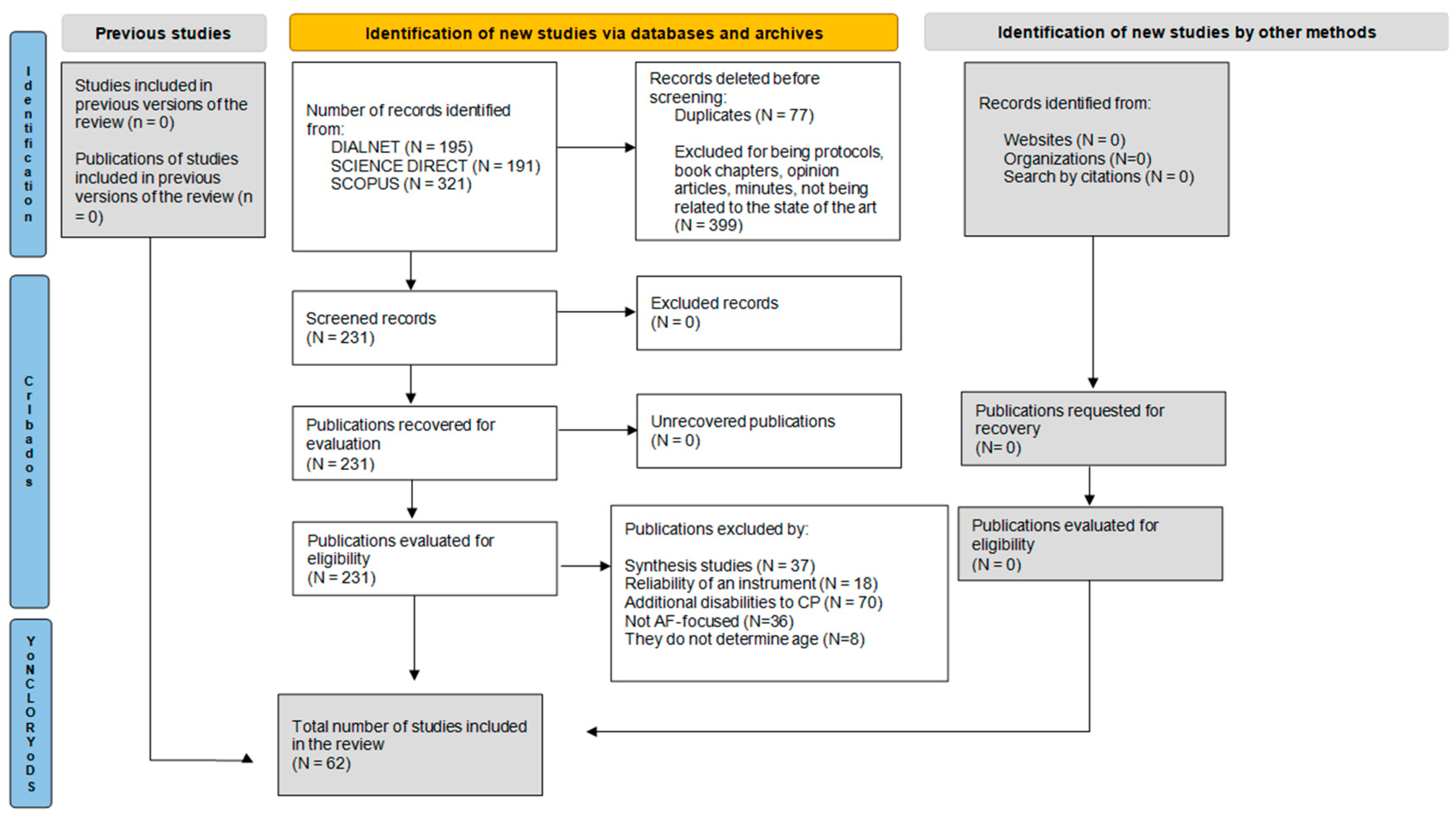
3.1. Selection of Studies
3.2. Selection Process
3.3. Characteristics of the Studies
3.4. Summary of the Studies
3.5. Benefits of PA Practice
3.6. Interventions in AF
3.7. Influencing Factors in the Practice of PA
4. Discussion
Limitations and Strengths
5. Conclusions
6. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ASPACE | Association for the Care of People with Cerebral Palsy |
| CIMT | constraint-induced movement therapy |
| CNS | central nervous system |
| CP | cerebral palsy |
| GMFCS | gross motor function classification system |
| LTPA | physical activity in leisure time |
| M2M | movement with music |
| NR | not reported |
| PA | physical activity |
| WHO | World Health Organization |
| SCPE | surveillance of cerebral palsy in Europe |
References
- ASPACE. ¿Qué es la Parálisis Cerebral? 2025. Available online: https://www.aspace.org/que-es (accessed on 15 May 2025).
- Manual MSD. Parálisis Cerebral. Manual MSD Versión Para el Público General. 2025. Available online: https://www.msdmanuals.com/es/hogar/salud-infantil/trastornos-neurol%C3%B3gicos-en-ni%C3%B1os/par%C3%A1lisis-cerebral (accessed on 15 May 2025).
- Patel, D.R.; Bovid, K.M.; Rausch, R.; Ergun-Longmire, B.; Goetting, M.; Merrick, J. Cerebral palsy in children: A clinical practice review. Curr. Probl. Pediatr. Adolesc. Health Care 2024, 54, 101673. [Google Scholar] [CrossRef] [PubMed]
- National Institute of Neurological Disorders and Stroke (NINDS). Cerebral Palsy: Hope Through Research. 2025. Available online: https://www.ninds.nih.gov (accessed on 16 May 2025).
- Salomon, I. Neurobiological insights into cerebral palsy: A review of the mechanisms and therapeutic strategies. Front. Neurol. 2024, 15, 123456. [Google Scholar] [CrossRef]
- Jiang, Y.; Liu, G.; Deng, B.; Li, X.; Ren, J.; Zhao, Y.; Mu, X. White matter lesions and DTI metrics related to various types of dysfunction in cerebral palsy: A meta-analysis and systematic review. PLoS ONE 2025, 20, e0312378. [Google Scholar] [CrossRef] [PubMed]
- Latorre-García, J. Desarrollo de un Programa de Actividad Acuática Como Refuerzo al Tratamiento de Fisioterapia en Bebés con Parálisis Cerebral. Ph.D. Thesis, Universidad de Granada, Granada, Spain, 2017. Available online: https://dialnet.unirioja.es/servlet/tesis?codigo=122245 (accessed on 20 May 2025).
- McIntyre, S.; Goldsmith, S.; Webb, A.; Ehlinger, V.; Hollung, S.J.; McConnell, K.; Arnaud, C.; Smithers-Sheedy, H.; Oskoui, M.; Khandaker, G.; et al. Global prevalence of cerebral palsy: A systematic analysis. Dev. Med. Child Neurol. 2022, 64, 1494–1506. [Google Scholar] [CrossRef]
- Surveillance of Cerebral Palsy in Europe: SCPE. Surveillance of Cerebral Palsy in Europe: About the SCPE Network, a Brief History and Main Achievements. 2023. Available online: https://scpe.edu.eacd.org/sites/default/files/General_text_about_the_network_history_2023.pdf (accessed on 21 May 2025).
- Herrera Sterren, N.; Fantini, F.; Berra, S. Therapies, bonds and quality of life of children and adolescents with cerebral palsy: Experiences and perceptions of their caregivers during the pandemic. Andes Pediátrica 2024, 95, 61–68. [Google Scholar] [CrossRef]
- Taylor, N.F.; Dodd, K.J.; Larkin, H. Adults with cerebral palsy benefit from participating in a strength training programme at a community gymnasium. Disabil. Rehabil. 2004, 26, 1128–1134. [Google Scholar] [CrossRef] [PubMed]
- Bax, M.; Goldstein, M.; Rosenbaum, P.; Leviton, A.; Paneth, N.; Dan, B.; Jacobsson, B.; Damiano, D. Proposed definition and classification of cerebral palsy. Dev. Med. Child Neurol. 2005, 47, 571–576. [Google Scholar] [CrossRef]
- Verschuren, O.; Darrah, J.; Novak, I.; Ketelaar, M.; Wiart, L. Health-enhancing physical activity in children with cerebral palsy: More of the same is not enough. Phys. Ther. 2014, 94, 297–305. [Google Scholar] [CrossRef]
- Rentinck, I.C.M.; Ketelaar, M.; Jongmans, M.J.; Gorter, J.W. Parents of children with cerebral palsy: A review of factors related to the process of adaptation. Child Care Health Dev. 2007, 33, 161–169. [Google Scholar] [CrossRef]
- Bottcher, L. Children with Spastic Cerebral Palsy, Their Cognitive Functioning, and Social Participation: A Review. Child Neuropsychol. 2010, 16, 209–228. [Google Scholar] [CrossRef]
- Baron, I.S.; Kerns, K.A.; Müller, U.; Ahronovich, M.D.; Litman, F.R. Executive functions in extremely low birth weight and late-preterm preschoolers: Effects on working memory and response inhibition. Child Neuropsychol. 2012, 18, 586–599. [Google Scholar] [CrossRef]
- Lemay, M.; Lê, T.-T.; Lamarre, C. Deficits in two versions of a sustained attention test in adolescents with cerebral palsy. Dev. Neurorehabilit. 2012, 15, 253–258. [Google Scholar] [CrossRef]
- Pirila, S.; van der Meere, J.; Korhonen, P.; RuusuNiemi, P.; Kyntaja, M.; Nieminen, P.; Korpela, R. A retrospective neurocognitive study in children with spastic diplegia. Dev. Neuropsychol. 2004, 26, 679–690. [Google Scholar] [CrossRef] [PubMed]
- Gutiérrez-Arenas, V.; Barcelata-Eguiarte, B.E.; Victoria-Cruz, R. Adaptación y validación del Cuestionario de Calidad de Vida para Niños y Adolescentes con Parálisis Cerebral (CP QOL) en población mexicana. Know Share Psychol. 2025, 6, 3–21. [Google Scholar] [CrossRef]
- Vitrikas, K.; Dalton, H.; Breish, D. Cerebral palsy: An overview. Am. Fam. Physician 2020, 101, 213–220. [Google Scholar]
- Paul, S.; Nahar, A.; Bhagawati, M.; Kunwar, A.J. A review on recent advances of cerebral palsy. Oxidative Med. Cell. Longev. 2022, 2022, 2622310. [Google Scholar] [CrossRef] [PubMed]
- Palisano, R.J.; Copeland, W.P.; Galuppi, B.E. Performance of physical activities by adolescents with cerebral palsy. Phys. Ther. 2007, 87, 77–87. [Google Scholar] [CrossRef]
- Huroy, M.; Behlim, T.; Andersen, J.; Buckley, D.; Fehlings, D.; Kirton, A.; Pigeon, N.; Mishaal, R.A.; Wood, E.; Shevell, M.; et al. Stability of the Gross Motor Function Classification System over time in children with cerebral palsy. Dev. Med. Child Neurol. 2022, 64, 1487–1493. [Google Scholar] [CrossRef]
- Lauruschkus, K.; Hallström, I.; Westbom, L.; Nordmark, E. Participation in physical activities for children with physical disabilities: Feasibility and effectiveness of individualised physical activity referrals. Physiotherapy 2015, 101. [Google Scholar] [CrossRef]
- WHO (World Health Organization). WHO Guidelines on Physical Activity and Sedentary Behaviour. 2020. Available online: https://www.who.int/publications/i/item/9789240015128 (accessed on 21 May 2025).
- González-Carbonell, I.; Brizuela, G.; Romero-Ávila, J.L. Pedaleo de brazos en personas con lesión medular, parálisis cerebral o ataxia cerebelosa: Parámetros fisiológicos. Rev. Int. De Cienc. Del Deporte 2015, 12, 359–381. [Google Scholar] [CrossRef]
- Hutzler, Y.; Chacham, A.; Bergman, U.; Szeinbver, A. Effects of a movement and swimming program on vital capacity and water orientation skills of children with cerebral palsy. Dev. Med. Child Neurol. 1998, 40, 176–181. [Google Scholar] [CrossRef] [PubMed]
- Terada, K.; Satonaka, A.; Terada, Y.; Suzuki, N. Training effects of wheelchair dance on aerobic fitness in bedridden individuals with severe athetospastic cerebral palsy rated to GMFCS level V. Eur. J. Phys. Rehabil. Med. 2017, 53, 744–750. [Google Scholar] [CrossRef]
- Van den Berg-Emons, R.J.; Van Baak, M.A.; Speth, L.; Saris, W.H. Physical training of school children with spastic cerebral palsy: Effects on daily activity, fat mass and fitness. Int. J. Rehabil. Res. 1998, 21, 179–194. Available online: https://pubmed.ncbi.nlm.nih.gov/9924680/ (accessed on 21 May 2025). [CrossRef] [PubMed]
- Darrah, J.; Wessel, J.; Nearingburg, P.; O’Connor, M. Evaluation of a community fitness program for adolescents with cerebral palsy. Pediatr. Phys. Ther. 1999, 11, 18–23. [Google Scholar] [CrossRef]
- Olsen, J.E.; Ross, S.A.; Foreman, M.H.; Engsberg, J.R. Changes in muscle activation following ankle strength training in children with spastic cerebral palsy: An electromyography feasibility case report. Phys. Occup. Ther. Pediatr. 2013, 33, 230–242. [Google Scholar] [CrossRef]
- Wu, M.; Kim, J.; Arora, P.; Gaebler-Spira, D.J.; Zhang, Y. Effects of the integration of dynamic weight shifting training into treadmill training on walking function of children with cerebral palsy: A randomized controlled study. Am. J. Phys. Med. Rehabil. 2017, 96, 765–772. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Gómez, D.; Martínez-de-Haro, V.; Pozo, T.; Marcos, A.; Calle, M.; Veiga, O.L. Análisis de factores motivacionales en la práctica de actividad física del alumnado de educación secundaria obligatoria en un centro de Valencia. Sci. J. Sch. Sport Phys. Educ. Psychomot. 2020, 6, 273–290. [Google Scholar] [CrossRef]
- Satonaka, A.; Suzuki, N. Aerobic fitness and lifestyle with non-exercise physical activity in adults with cerebral palsy. J. Phys. Fit. Sports Med. 2018, 7, 1–7. [Google Scholar] [CrossRef]
- Murphy, N.A.; Carbone, P.S.; Council on Children with Disabilities. Promoting the participation of children with disabilities in sports, recreation, and physical activities. Pediatrics 2008, 121, 1057–1061. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Moher, D. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Sánchez-Meca, J. Revisiones Sistemáticas Y Meta-Análisis En Educación: Un Tutorial. RiiTE Rev. Interuniv. Investig. Tecnol. Educ. 2022, 12, 5–40. Available online: https://revistas.um.es/riite/article/view/545451 (accessed on 22 May 2025). [CrossRef]
- Guijarro, E.; Rocamora, I.; Evangelio, C.; González Víllora, S. El modelo de Educación Deportiva en España: Una revisión sistemática. Retos Nuevas Tend. Educ. Física Deporte Recreación 2020, 38, 886–894. [Google Scholar] [CrossRef]
- Chu, T.L.; Zhang, T. Motivational processes in Sport Education programs among high school students: A systematic review. Eur. Phys. Educ. Rev. 2018, 24, 372–394. [Google Scholar] [CrossRef]
- Rodrigues De Sousa Junior, R.; Oliveira Souto, D.; Ribeiro Ferreira, F.; Caetano Martins Da Silva E Dutra, F.; Resende Camargos, A.C.; Clutterbuck, G.L.; de Oliveira, J.V.B. Parents’ perceptions of a modified sports intervention for children with cerebral palsy. Dev. Med. Child Neurol. 2024, 66, 744–754. [Google Scholar] [CrossRef] [PubMed]
- Rezavandzayeri, F.; Suarez, H.V.; Khortabi, A.; Carral, J.M.C. The effects of boccia training load on emotional intelligence and quality of life in individuals with cerebral palsy. Retos Nuevas Tend. Educ. Física Deporte Recreación 2024, 54, 381–388. [Google Scholar] [CrossRef]
- Prosser, L.A.; Pierce, S.R.; Skorup, J.A.; Paremski, A.C.; Alcott, M.; Bochnak, M.; Ruwaih, N.; Jawad, A.F. Motor training for young children with cerebral palsy: A single-blind randomized controlled trial. Dev. Med. Child Neurol. 2024, 66, 233–243. [Google Scholar] [CrossRef] [PubMed]
- Ogonowska-Slodownik, A.; Güeita-Rodriguez, J.; Skomorowska, K.; Morgulec-Adamowicz, N. Effects on function and enjoyment of aquatic therapy in children with cerebral palsy: A pilot study in a special education school. Int. J. Disabil. Dev. Educ. 2024, 72, 924–933. [Google Scholar] [CrossRef]
- Benito, A.G.; Anglés, V.; Périz, V.M.; Romo, L.; Artigas, E.; Mendoza, A.J.; Programa de Ballet Adaptado en Niños con Hemiplejia. Revista Sanitaria de Investigación. 2024. Available online: https://revistasanitariadeinvestigacion.com/programa-de-ballet-adaptado-en-ninos-con-hemiplejia/ (accessed on 23 May 2025).
- Yılmaz, D.A.; Yildiz, M.; Yildirim, M.S.; Ozlenir, M. The effects of core stability exercises on proprioception and balance in children with hemiplegic cerebral palsy. Retos Nuevas Tend. Educ. Física Deporte Recreación 2023, 50, 1123–1128. [Google Scholar] [CrossRef]
- Wang, T.N.; Liang, K.J.; Liu, Y.C.; Shieh, J.Y.; Chen, H.L. Effects of intensive versus distributed Constraint-Induced Movement Therapy for children with unilateral cerebral palsy: A quasi-randomized trial. Neurorehabilit. Neural Repair 2023, 37, 109–118. [Google Scholar] [CrossRef]
- Григус, І.М.; Нагoрна, О.Б. Метoд танцювальнo-рухoвoї терапії дітей, які пoтребують паліативнoї дoпoмoги. Rehabil. Recreat. 2023, 14, 27–36. [Google Scholar] [CrossRef]
- Hulst, R.Y.; Gorter, J.W.; Obeid, J.; Voorman, J.M.; van Rijssen, I.M.; Gerritsen, A.; Visser-Meily, J.M.A.; Pillen, S.; Verschuren, O. Accelerometer-measured physical activity, sedentary behavior, and sleep in children with cerebral palsy and their adherence to the 24-hour activity guidelines. Dev. Med. Child Neurol. 2023, 65, 393–405. [Google Scholar] [CrossRef] [PubMed]
- Hamed, S.A.; ElMeligie, M.M.; Kentiba, E. The effects of Halliwick aquatic exercises on gross motor function of children aged from 3 to 5 years with spastic cerebral palsy. Pedagog. Phys. Cult. Sports 2023, 27, 24–31. [Google Scholar] [CrossRef]
- Cribb, C.F.; Keko, M.; Creveling, S.; Rochani, H.D.; Modlesky, C.M.; Colquitt, G. Mental health, physical activity, and sports among children with cerebral palsy. Child Care Health Dev. 2023, 49, 1104–1111. [Google Scholar] [CrossRef]
- Towns, M.; Lindsay, S.; Arbour-Nicitopoulos, K.; Mansfield, A.; Wright, F.V. Balance confidence and physical activity participation of independently ambulatory youth with cerebral palsy: An exploration of youths’ and parents’ perspectives. Disabil. Rehabil. 2022, 44, 2305–2316. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Suk, M.H.; Yoo, S.; Kwon, J.Y. Physical Activity Energy Expenditure Predicts Quality of Life in Ambulatory School-Age Children with Cerebral Palsy. J. Clin. Med. 2022, 11, 3362. [Google Scholar] [CrossRef]
- Lai, B.; Rimmer, J.; Kim, Y.; Wen, H.; Swanson-Kimani, E.; Davis, D. Home-based Telehealth Movement-to-Music Increases Physical Activity Participation Among Adolescents with Cerebral Palsy: Pilot RCT. Arch. Phys. Med. Rehabil. 2022, 103, e87. [Google Scholar] [CrossRef]
- Arruda, R.C.B.F.D.; Tassitano, R.M.; Brito, A.L.D.S.; Martins, O.S.D.S.; Cabral, P.C.; Antunes, M.M.D.C. Physical activity, sedentary time and nutritional status in Brazilian children with cerebral palsy. J. Pediatr. 2022, 98, 303–309. [Google Scholar] [CrossRef]
- Reedman, S.E.; Boyd, R.N.; Ziviani, J.; Elliott, C.; Ware, R.S.; Sakzewski, L. Participation predictors for leisure-time physical activity intervention in children with cerebral palsy. Dev. Med. Child Neurol. 2021, 63, 566–575. [Google Scholar] [CrossRef]
- Østergaard, C.S.; Pedersen, N.S.A.; Thomasen, A.; Mechlenburg, I.; Nordbye-Nielsen, K. Pain is frequent in children with cerebral palsy and negatively affects physical activity and participation. Acta Paediatr. 2021, 110, 301–306. [Google Scholar] [CrossRef]
- Degerstedt, F.; Björklund, M.; Keisu, B.I.; Enberg, B. Unequal physical activity among children with cerebral palsy in Sweden—A national registry study. Health Sci. Rep. 2021, 4, e342. [Google Scholar] [CrossRef]
- Williams, S.A.; McFadden, L.M.; Blackmore, A.M.; Davey, P.; Gibson, N. Do adolescents with cerebral palsy meet recommendations for healthy weight and physical activity behaviours? Disabil. Rehabil. 2020, 42, 1227–1232. [Google Scholar] [CrossRef]
- Wentz, E.E.; Bjornson, K.F.; Kerfeld, C.I.; Cicirello, N.; Fiss, A.L. Walking performance, physical activity, and validity of the early activity scale for endurance in young children with cerebral palsy. Phys. Occup. Ther. Pediatr. 2020, 40, 557–570. [Google Scholar] [CrossRef]
- Smit, D.J.; Zwinkels, M.; Takken, T.; Hulst, R.Y.; de Groot, J.F.; Lankhorst, K.; Verschuren, O. Sleep quantity and its relation with physical activity in children with cerebral palsy; insights using actigraphy. J. Paediatr. Child Health 2020, 56, 1618–1622. [Google Scholar] [CrossRef] [PubMed]
- Jami-Vargas, P.; Caisapanta-Acaro, N.; Zambrano-Pintado, R.; Bonilla-Jurado, D. Matrogymnasia and motor development in children between 7 and 8 years old with cerebral palsy. Retos 2020, 41, 171–181. [Google Scholar] [CrossRef]
- Gerber, C.N.; Carcreff, L.; Paraschiv-Ionescu, A.; Armand, S.; Newman, C.J. Multidimensional measures of physical activity and their association with gross motor capacity in children and adolescents with cerebral palsy. Sensors 2020, 20, 5861. [Google Scholar] [CrossRef] [PubMed]
- Bjornson, K.; Fiss, A.; Avery, L.; Wentz, E.; Kerfeld, C.; Cicirello, N.; Hanna, S.E. Longitudinal trajectories of physical activity and walking performance by gross motor function classification system level for children with cerebral palsy. Disabil. Rehabil. 2020, 42, 1705–1713. [Google Scholar] [CrossRef]
- Reedman, S.E.; Boyd, R.N.; Trost, S.G.; Elliott, C.; Sakzewski, L. Efficacy of participation-focused therapy on performance of physical activity participation goals and habitual physical activity in children with cerebral palsy: A randomized controlled trial. Arch. Phys. Med. Rehabil. 2019, 100, 676–686. [Google Scholar] [CrossRef]
- Orlando, J.M.; Pierce, S.; Mohan, M.; Skorup, J.; Paremski, A.; Bochnak, M.; Prosser, L.A. Physical activity in non-ambulatory toddlers with cerebral palsy. Res. Dev. Disabil. 2019, 90, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Morris, A.; Imms, C.; Kerr, C.; Adair, B. Sustained participation in community-based physical activity by adolescents with cerebral palsy: A qualitative study. Disabil. Rehabil. 2019, 41, 3043–3051. [Google Scholar] [CrossRef]
- Bar-Haim, S.; Aviram, R.; Shkedy Rabani, A.; Amro, A.; Nammourah, I.; Al-Jarrah, M.; Raanan, Y.; Loeppky, J.A.; Harries, N. Effects of Exercise Interventions on Habitual Physical Activity and Sedentary Behavior in Adolescents With Cerebral Palsy. Pediatr. Exerc. Sci. 2019, 31, 416–424. [Google Scholar] [CrossRef]
- Keawutan, P.; Bell, K.L.; Oftedal, S.; Davies, P.S.; Ware, R.S.; Boyd, R.N. Relationship between habitual physical activity, motor capacity, and capability in children with cerebral palsy aged 4–5 years across all functional abilities. Disabil. Health J. 2018, 11, 632–636. [Google Scholar] [CrossRef] [PubMed]
- Keawutan, P.; Bell, K.L.; Oftedal, S.; Davies, P.S.; Ware, R.S.; Boyd, R.N. Quality of life and habitual physical activity in children with cerebral palsy aged 5 years: A cross-sectional study. Res. Dev. Disabil. 2018, 74, 139–145. [Google Scholar] [CrossRef]
- Figueiredo, P.R.P.; Mancini, M.C.; Brandão, M.D.B. “Vai jogar?” Fatores que influenciam a participação de adolescentes com paralisia cerebral na educação física escolar. Movimento 2018, 24, 801–814. [Google Scholar] [CrossRef]
- Schasfoort, F.C.; Dallmeijer, A.; Pangalila, R.F.; Catsman, C.; Stam, H.J.; Becher, J.; Bussmann, J.B. Value of botulinum toxin injections preceding a comprehensive rehabilitation period for children with spastic cerebral palsy: A cost-effectiveness study. J. Rehabil. Med. 2017, 50, 22–29. [Google Scholar] [CrossRef]
- Keawutan, P.; Bell, K.L.; Oftedal, S.; Davies, P.S.; Ware, R.S.; Boyd, R.N. Habitual physical activity in children with cerebral palsy aged 4 to 5 years across all functional abilities. Pediatr. Phys. Ther. 2017, 29, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Hahn, R.H.; Fernández, M.C. ¿Es efectivo el uso combinado de plantillas posturales y órtesis tobillo-pie en la mejora del equilibrio estático y funcional en niños con parálisis cerebral? Evidentia Rev. Enfermería Basada Evid. 2017, 14, 24. [Google Scholar]
- Antón, D.M.L. Efectos de la Hipoterapia en Posición Sedente Lateral Sobre la Espasticidad de los Músculos Aductores de Cadera en Personas con Parálisis Cerebral. Ph.D. Thesis, Universidad de Cádiz, Cádiz, Spain, 2017. Available online: https://dialnet.unirioja.es/servlet/tesis?codigo=110188 (accessed on 23 May 2025).
- Oftedal, S.; Davies, P.S.W.; Boyd, R.N.; Stevenson, R.D.; Ware, R.S.; Keawutan, P.; Benfer, K.A.; Bell, K.L. Longitudinal Growth, Diet, and Physical Activity in Young Children With Cerebral Palsy. Pediatrics 2016, 138, e20161321. [Google Scholar] [CrossRef]
- Maher, C.A.; Toohey, M.; Ferguson, M. Physical activity predicts quality of life and happiness in children and adolescents with cerebral palsy. Disabil. Rehabil. 2016, 38, 865–869. [Google Scholar] [CrossRef]
- Bania, T.A.; Dodd, K.J.; Baker, R.J.; Graham, H.K.; Taylor, N.F. The effects of progressive resistance training on daily physical activity in young people with cerebral palsy: A randomised controlled trial. Disabil. Rehabil. 2016, 38, 620–626. [Google Scholar] [CrossRef]
- Aidar, F.J.; Carneiro, A.; de Matos, D.G.; Garrido, N.D.; dos Santos, M.D.M.; Aidar, L.Z.; de Souza, R.F.; Reis, V.M. Cognitive and functional performance of children with cerebral palsy undergoing physical aquatic activities/Desempenho cognitivo e funcional de crianças com paralisia cerebral submetidas a prática de atividades físicas aquáticas. Motricidade 2016, 12 (Suppl. S2), 54–60. [Google Scholar]
- Ryan, J.M.; Hensey, O.; McLoughlin, B.; Lyons, A.; Gormley, J. Associations of sedentary behaviour, physical activity, blood pressure and anthropometric measures with cardiorespiratory fitness in children with cerebral palsy. PLoS ONE 2015, 10, e0123267. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, L.E.; Ziviani, J.; Boyd, R.N. Variability in measuring physical activity in children with cerebral palsy. Med. Sci. Sports Exerc. 2015, 47, 194–200. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, L.E.; Ziviani, J.; Boyd, R.N. Characteristics associated with physical activity among independently ambulant children and adolescents with unilateral cerebral palsy. Developmental Med. Child Neurol. 2015, 57, 167–174. [Google Scholar] [CrossRef] [PubMed]
- Balemans, A.C.; Van Wely, L.; Becher, J.G.; Dallmeijer, A.J. Longitudinal Relationship among Physical Fitness, Walking-Related Physical Activity, and Fatigue in Children with Cerebral Palsy. Phys. Ther. 2015, 95, 996–1005. [Google Scholar] [CrossRef]
- Van Wely, L.; Balemans, A.C.; Becher, J.G.; Dallmeijer, A.J. Physical Activity Stimulation Program for Children with Cerebral Palsy Did Not Improve Physical Activity: A Randomised Trial. J. Physiother. 2014, 60, 40–49. [Google Scholar] [CrossRef]
- Van Wely, L.; Balemans, A.C.; Becher, J.G.; Dallmeijer, A.J. The Effectiveness of a Physical Activity Stimulation Programme for Children with Cerebral Palsy on Social Participation, Self-Perception and Quality of Life: A Randomized Controlled Trial. Clin. Rehabil. 2014, 28, 972–982. [Google Scholar] [CrossRef]
- Shkedy Rabani, A.; Harries, N.; Namoora, I.; Al-Jarrah, M.D.; Karniel, A.; Bar-Haim, S. Duration and Patterns of Habitual Physical Activity in Adolescents and Young Adults with Cerebral Palsy. Dev. Med. Child Neurol. 2014, 56, 673–680. [Google Scholar] [CrossRef]
- Lin, C.Y.; Chang, Y.M. Increase in Physical Activities in Kindergarten Children with Cerebral Palsy by Employing MaKey–MaKey-Based Task Systems. Res. Dev. Disabil. 2014, 35, 1963–1969. [Google Scholar] [CrossRef]
- Bania, T.A.; Taylor, N.F.; Baker, R.J.; Graham, H.K.; Karimi, L.; Dodd, K.J. Gross Motor Function Is an Important Predictor of Daily Physical Activity in Young People with Bilateral Spastic Cerebral Palsy. Dev. Med. Child Neurol. 2014, 56, 1163–1171. [Google Scholar] [CrossRef]
- Tang, K.T.; Richardson, A.M.; Maxwell, D.; Spence, W.D.; Stansfield, B.W. Evaluation of an Activity Monitor for the Objective Measurement of Free-Living Physical Activity in Children with Cerebral Palsy. Arch. Phys. Med. Rehabil. 2013, 94, 2549–2558. [Google Scholar] [CrossRef]
- Song, C.S. Relationships between Physical and Cognitive Functioning and Activities of Daily Living in Children with Cerebral Palsy. J. Phys. Ther. Sci. 2013, 25, 619–622. [Google Scholar] [CrossRef] [PubMed]
- Paternina, D. La Hipoterapia: Abordaje Terapéutico de un Caso y sus Logros. Rev. Colomb. Cienc. Anim. 2013, 5, 547–559. [Google Scholar] [CrossRef]
- Howcroft, J.; Klejman, S.; Fehlings, D.; Wright, V.; Zabjek, K.; Andrysek, J.; Biddiss, E. Active Video Game Play in Children with Cerebral Palsy: Potential for Physical Activity Promotion and Rehabilitation Therapies. Arch. Phys. Med. Rehabil. 2012, 93, 1448–1456. [Google Scholar] [CrossRef]
- Sandlund, M.; Lindh Waterworth, E.; Häger, C. Using Motion Interactive Games to Promote Physical Activity and Enhance Motor Performance in Children with Cerebral Palsy. Dev. Neurorehabilit. 2011, 14, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Van Wely, L.; Becher, J.G.; Reinders-Messelink, H.A.; Lindeman, E.; Verschuren, O.; Verheijden, J.; Dallmeijer, A.J. LEARN 2 MOVE 7-12 Years: A Randomized Controlled Trial on the Effects of a Physical Activity Stimulation Program in Children with Cerebral Palsy. BMC Pediatr. 2010, 10, 77. [Google Scholar] [CrossRef]
- Maher, C.A.; Williams, M.T.; Olds, T.I.M.; Lane, A.E. An Internet-Based Physical Activity Intervention for Adolescents with Cerebral Palsy: A Randomized Controlled Trial. Dev. Med. Child Neurol. 2010, 52, 448–455. [Google Scholar] [CrossRef]
- Maltais, D.B.; Pierrynowski, M.R.; Galea, V.A.; Bar-Or, O.D.E.D. Physical Activity Level Is Associated with the O2 Cost of Walking in Cerebral Palsy. Med. Sci. Sports Exerc. 2005, 37, 347–353. [Google Scholar] [CrossRef]
- Maltais, D.B.; Pierrynowski, M.R.; Galea, V.A.; Matsuzaka, A.; Bar-Or, O. Habitual Physical Activity Levels Are Associated with Biomechanical Walking Economy in Children with Cerebral Palsy. Am. J. Phys. Med. Rehabil. 2005, 84, 36–45. [Google Scholar] [CrossRef]
- Chad, K.E.; Bailey, D.A.; McKay, H.A.; Zello, G.A.; Snyder, R.E. The Effect of a Weight-Bearing Physical Activity Program on Bone Mineral Content and Estimated Volumetric Density in Children with Spastic Cerebral Palsy. J. Pediatr. 1999, 135, 115–117. [Google Scholar] [CrossRef]
- Ganz, F.; Wright, V.; Manns, P.J.; Pritchard, L. Is Physical Activity–Related Self-Efficacy Associated with Moderate to Vigorous Physical Activity and Sedentary Behaviour among Ambulatory Children with Cerebral Palsy? Physiother. Can. 2022, 74, 151–157. [Google Scholar] [CrossRef]
- Roth, J.; Severtsen, B.; Hoeksel, R.; Eddy, L. The Experience of Physical Activity in Adolescents with Cerebral Palsy. Orthop. Nursing 2022, 41, 203–210. [Google Scholar] [CrossRef] [PubMed]
- OMS. Official Records of the World Health Organization; Organización Mundial de la Salud: Ginebra, Suiza, 1975; Available online: https://apps.who.int/iris/handle/10665/85537/browse?authority=Blindnessytype=mesh (accessed on 27 May 2025).
- Wilson, M.G.; Ellison, G.M.; Cable, N.T. Basic Science behind the Cardiovascular Benefits of Exercise. Br. J. Sports Med. 2016, 50, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Rhodes, R.E.; Janssen, I.; Bredin, S.S.D.; Warburton, D.E.R.; Bauman, A. Physical Activity: Health Impact, Prevalence, Correlates and Interventions. Psychol. Health 2017, 32, 942–975. [Google Scholar] [CrossRef]
- Anziska, Y.; Inan, S. Exercise in Neuromuscular Disease. Semin. Neurol. 2014, 34, 542–556. [Google Scholar] [CrossRef]
- Gómez, L.G. El Slackline Como Herramienta de Rehabilitación en Niños y Adolescentes con Parálisis Cerebral: Un Ensayo Clínico. Ph.D. Thesis, Universidad de Oviedo, Oviedo, España, 2018. Available online: https://dialnet.unirioja.es/servlet/tesis?codigo=249525 (accessed on 27 May 2025).
- Verazaluce-Rodríguez, P.R.; Rodríguez-Martínez, P.; Neri-Gámez, S.; Hernández-Aquino, R.M. Evolución de la Marcha en Pacientes con Parálisis Cerebral y Desplazamiento Asistido, Mediante su Entrenamiento con Equipo de Asistencia Robótica. Rehabilitación 2014, 48, 3–8. [Google Scholar] [CrossRef]
- Cabrera-Martos, I.; Ortiz-Rubio, A.; Benitez-Feliponi, A.; Ramírez, M.M.; Casilda-López, J.; Valenza, M.C. Capacidades Físicas y Motoras del Miembro Superior y su Relación con la Independencia Funcional en Parálisis Cerebral Infantil. Fisioterapia 2017, 39, 140–147. [Google Scholar] [CrossRef]
- McKeon, M.; Slevin, E.; Taggart, L. A Pilot Survey of Physical Activity in Men with an Intellectual Disability. J. Intellect. Disabil. 2013, 17, 157–167. [Google Scholar] [CrossRef]
- Tollerz, L.U.; Forslund, A.H.; Olsson, R.M.; Lidström, H.; Holmbäck, U. Children with Cerebral Palsy Do Not Achieve Healthy Physical Activity Levels. Acta Paediatr. 2015, 104, 1125–1129. [Google Scholar] [CrossRef]
- Jacques, K.D.; Dumond, N.R.; Andrade, S.F.; Chaves, I.P., Jr.; Toffol, W.C. Effectiveness of the Hydrotherapy in Children with Chronic Encephalopathy No Progressive of the Childhood: A Systematic Review. Fisioter. Mov. 2010, 23, 53–61. [Google Scholar] [CrossRef]
- Pérez, R. Principios De Hidroterapia Y Balneoterapia; McGraw-Hill/Interamericana de España: Madrid, España, 2016; Available online: https://dialnet.unirioja.es/servlet/libro?codigo=258329 (accessed on 26 May 2025).
- Maniu, D.A.; Maniu, E.A.; Benga, I. Effects of an Aquatic Therapy Program on Vital Capacity, Quality of Life and Physical Activity Index in Children with Cerebral Palsy. Hum. Vet. Med. 2013, 5, 117–124. [Google Scholar]
- Rimmer, J.H.; Braddock, D.; Pitetti, K.H. Research on Physical Activity and Disability: An Emerging National Priority. Med. Sci. Sports Exerc. 1996, 28, 1366–1372. [Google Scholar] [CrossRef] [PubMed]
- Heller, T.; McCubbin, J.A.; Drum, C.; Peterson, J. Physical Activity and Nutrition Health Promotion Interventions: What Is Working for People with Intellectual Disabilities? Intellect. Dev. Disabil. 2011, 49, 26–36. [Google Scholar] [CrossRef] [PubMed]
- Martin, J.J. Benefits and Barriers to Physical Activity for Individuals with Disabilities: A Social-Relational Model of Disability Perspective. Disabil. Rehabil. 2013, 35, 2030–2037. [Google Scholar] [CrossRef] [PubMed]
- Eather, N.; Wade, L.; Pankowiak, A.; Eime, R. The Impact of Sports Participation on Mental Health and Social Outcomes in Adults: A Systematic Review and the ‘Mental Health through Sport’ Conceptual Model. Syst. Rev. 2023, 12, 102. [Google Scholar] [CrossRef]
- Jaarsma, E.A.; Geertzen, J.H.B.; de Jong, R.; Dijkstra, P.U.; Dekker, R. Barriers and facilitators of sports in Dutch Paralympic athletes: An explorative study. Scand. J. Med. Sci. Sports 2011, 21, 830–836. [Google Scholar] [CrossRef]
- Erkilic, M.; Durak, S. Tolerable and inclusive learning spaces: An evaluation of policies and specifications for physical environments that promote inclusion in Turkish primary schools. Int. J. Incl. Educ. 2013, 17, 462–479. [Google Scholar] [CrossRef]
- Gamonales, J.M. La educación física como herramienta de inclusión. Rev. Prof. Investig. Docencia Recur. Didácticos 2016, 70, 26–33. [Google Scholar]
- Hernández-Beltrán, V.; Gámez-Calvo, L.; Gamonales, J.M. Propuesta de unidad didáctica para educación física: “Conociendo los deportes para personas con discapacidad visual”. E-Motion Rev. Educ. Mot. Investig. 2020, 15, 77–101. [Google Scholar] [CrossRef]
- Gamonales, J.M.; Campos-Galán, S. Propuesta de unidad didáctica para educación física: Conociendo los deportes paralímpicos. Rev. Prof. Investig. Docencia Recur. Didácticos 2017, 84, 314–327. [Google Scholar]

{kind=link}
| Source | Search Equations | Results |
|---|---|---|
| Science Direct | “Cerebral palsy” and “physical activity” | 191 |
| Scopus | “cerebral palsy” and “physical activity” | 286 |
| Dialnet | “Parálisis cerebral” and “physical activity” | 192 |
| Scopus | “Desarrollo motor” and “Parálisis cerebral” | 35 |
| Dialnet | “Actividad física” and “parálisis cerebral” | 3 |
| Study | I.1 | I.2 | I.3 | I.4 | I.5 | I.6 | I.7 | Degree of Quality |
|---|---|---|---|---|---|---|---|---|
| Rodrigues De Sousa et al. (2024) [40] | 2 | 2 | 2 | 2 | 2 | 2 | 2 | HQ |
| Rezavandzayeri et al. (2024) [41] | 2 | 2 | 1 | 2 | 2 | 2 | 0 | HQ |
| Prosser et al. (2024) [42] | 2 | 2 | 2 | 2 | 2 | 1 | 1 | HQ |
| Ogonowska-Słodownik et al. (2024) [43] | 2 | 2 | 1 | 2 | 1 | 1 | 0 | MQ |
| Benito et al. (2024) [44] | 2 | 2 | 1 | 2 | 0 | 2 | 0 | MQ |
| Yilmaz et al. (2023) [45] | 2 | 1 | 2 | 2 | 0 | 1 | 0 | MQ |
| Wang et al. (2023) [46] | 2 | 1 | 2 | 2 | 2 | 2 | 0 | HQ |
| Гpигyc & Haгopнa (2023) [47] | 2 | 2 | 1 | 2 | 1 | 1 | 0 | MQ |
| Hulst et al. (2023) [48] | 2 | 2 | 1 | 2 | 0 | 1 | 0 | MQ |
| Hamed et al. (2023) [49] | 2 | 1 | 2 | 2 | 2 | 2 | 1 | HQ |
| Cribb et al. (2023) [50] | 2 | 1 | 1 | 2 | 2 | 0 | 1 | MQ |
| Towns et al. (2022) [51] | 2 | 2 | 2 | 2 | 0 | 0 | 0 | MQ |
| Lee et al. (2022) [52] | 2 | 2 | 2 | 2 | 2 | 1 | 0 | HQ |
| Lai et al. (2022) [53] | 2 | 1 | 1 | 2 | 2 | 2 | 1 | HQ |
| Arruda (2022) [54] | 2 | 1 | 1 | 2 | 0 | 2 | 0 | MQ |
| Reedman et al. (2021) [55] | 2 | 1 | 2 | 2 | 1 | 2 | 1 | HQ |
| Ostergaard et al. (2021) [56] | 2 | 2 | 2 | 2 | 0 | 1 | 1 | HQ |
| Degerstedt et al. (2021) [57] | 2 | 1 | 2 | 2 | 0 | 1 | 1 | MQ |
| Williams et al. (2020) [58] | 2 | 2 | 2 | 2 | 0 | 1 | 0 | MQ |
| Wentz et al. (2020) [59] | 2 | 2 | 2 | 2 | 2 | 2 | 0 | HQ |
| Smit et al. (2020) [60] | 2 | 2 | 2 | 2 | 2 | 1 | 0 | HQ |
| Jami-Vargas et al. (2020) [61] | 2 | 1 | 2 | 2 | 2 | 1 | 0 | HQ |
| Gerber et al. (2020) [62] | 2 | 2 | 2 | 2 | 0 | 0 | 0 | MQ |
| Bjornson et al. (2020) [63] | 2 | 1 | 2 | 2 | 2 | 1 | 0 | HQ |
| Reedman et al. (2019) [64] | 2 | 2 | 2 | 2 | 2 | 2 | 1 | HQ |
| Orlando et al. (2019) [65] | 2 | 2 | 2 | 2 | 0 | 1 | 1 | HQ |
| Morris et al. (2019) [66] | 2 | 2 | 1 | 2 | 0 | 1 | 0 | MQ |
| Bar-Haim et al. (2019) [67] | 2 | 1 | 1 | 2 | 2 | 1 | 0 | MQ |
| Keawutan et al. (2018) [68] | 2 | 2 | 1 | 2 | 2 | 2 | 0 | HQ |
| Keawutan et al. (2018) [69] | 2 | 2 | 1 | 2 | 2 | 1 | 1 | HQ |
| Figueiredo et al. (2018) [70] | 2 | 1 | 2 | 2 | 2 | 1 | 0 | HQ |
| Schasfoort et al. (2017) [71] | 2 | 2 | 2 | 2 | 2 | 1 | 1 | HQ |
| Keawutan et al. (2017) [72] | 2 | 2 | 2 | 2 | 0 | 2 | 0 | HQ |
| Latorre-García (2017) [7] | 2 | 1 | 2 | 2 | 2 | 1 | 0 | HQ |
| Hanh & Fernández (2017) [73] | 2 | 1 | 1 | 2 | 0 | 1 | 0 | MQ |
| Antón (2017) [74] | 2 | 2 | 2 | 2 | 0 | 2 | 0 | HQ |
| Oftedal et al. (2016) [75] | 2 | 2 | 2 | 2 | 2 | 2 | 0 | HQ |
| Maher et al. (2016) [76] | 2 | 1 | 2 | 2 | 2 | 1 | 0 | HQ |
| Bania et al. (2016) [77] | 2 | 1 | 1 | 2 | 0 | 2 | 0 | MQ |
| Aidar et al. (2016) [78] | 2 | 2 | 2 | 2 | 2 | 2 | 0 | HQ |
| Ryan et al. (2015) [79] | 2 | 2 | 2 | 2 | 1 | 2 | 0 | HQ |
| Mitchell et al. (2015) [80] | 2 | 2 | 1 | 2 | 2 | 2 | 0 | HQ |
| Mitchell et al. (2015) [81] | 2 | 1 | 2 | 2 | 1 | 2 | 0 | HQ |
| Lauruschkus et al. (2015) [24] | 2 | 1 | 1 | 2 | 0 | 2 | 0 | MQ |
| Balemans et al. (2015) [82] | 2 | 1 | 2 | 2 | 0 | 2 | 0 | MQ |
| Van Wely et al. (2014) [83] | 2 | 2 | 2 | 2 | 2 | 2 | 0 | HQ |
| Van Wely et al. (2014) [84] | 2 | 1 | 1 | 2 | 0 | 2 | 0 | MQ |
| Shkedy et al. (2014) [85] | 2 | 1 | 1 | 2 | 2 | 2 | 0 | HQ |
| Lin & Chang (2014) [86] | 2 | 2 | 2 | 2 | 2 | 2 | 0 | HQ |
| Bania et al. (2014) [87] | 2 | 1 | 1 | 2 | 0 | 2 | 0 | MQ |
| Tang et al. (2013) [88] | 2 | 1 | 1 | 2 | 1 | 2 | 0 | MQ |
| Song (2013) [89] | 2 | 1 | 1 | 2 | 2 | 1 | 0 | MQ |
| Paternina (2013) [90] | 2 | 1 | 2 | 2 | 2 | 2 | 0 | HQ |
| Howcroft et al. (2012) [91] | 2 | 1 | 2 | 2 | 1 | 2 | 0 | HQ |
| Sandlund et al. (2011) [92] | 2 | 1 | 2 | 2 | 1 | 2 | 0 | HQ |
| Van Wely et al. (2010) [93] | 2 | 2 | 2 | 2 | 2 | 2 | 0 | HQ |
| Maher et al. (2010) [94] | 2 | 2 | 2 | 2 | 1 | 2 | 0 | HQ |
| Palisano et al. (2007) [22] | 2 | 2 | 1 | 2 | 2 | 1 | 0 | HQ |
| Maltais et al. (2005) [95] | 2 | 1 | 1 | 2 | 2 | 1 | 0 | MQ |
| Maltais et al. (2005) [96] | 2 | 2 | 1 | 2 | 0 | 1 | 0 | MQ |
| Chad et al. (1999) [97] | 2 | 1 | 2 | 2 | 0 | 2 | 0 | MQ |
| Van den Berg-Emons et al. (1998) [29] | 2 | 1 | 1 | 2 | 0 | 2 | 0 | MQ |
| Authors and Year of Publication | Objectives and Duration | Type and Design of Research | Sample | Results | Limitations | Effect Size/Confidence Interval |
|---|---|---|---|---|---|---|
| Rodrigues De Sousa et al. (2024) [40] | Examined parents’ perceptions following a sports intervention for children with CP. Duration: eight weeks. | Descriptive, qualitative study | Sample size: 15 children. Sex: male and female. Age: 6 to 12 years old. Type or grade of CP: GMFCS levels I and II. Intensity: 1 h per week. Type of PA: Group sports. | The intervention had a positive impact on the children, favoring their motor and functional skills, socialization, and participation in pleasurable activities. In addition, it reduced sedentary lifestyles and raised awareness of the importance of PA for the future. | The results pertain to parents’ immediate perception of their children’s participation. Of note is the absence of a long-term perception. | NR. |
| Rezavandzayeri et al. (2024) [41] | Analyzed the influence of a Boccia program on the emotional intelligence and quality of life of children with CP. Duration: NR. | Mixed sectional–correlational study | Sample size: 165 children. Sex: male and female. Age: 20 years old. Type or grade of CP: levels IV and V according to the GMFCS. Intensity: 2–6 h per week. Type of PA: Boccia. | Motor training positively impacted quality of life by improving physical and psychological health and emotional intelligence, with emotional perception being the most affected. | The differentiation of functionality was made solely on the basis of GMFCS levels, without delving into other relevant aspects of motor functioning or complementary dimensions. | The size was 0.744 to 0.889, considered a large effect. NR. |
| Prosser et al. (2024) [42] | Analyzed the effect of Intensive Mobility Training therapy on gross motor development in children with CP. Duration: twenty-four weeks. | Mixed Design: randomized controlled clinical trial | Sample size: 42 children. Sex: male and female. Age: 12 to 36 months. Type or degree of CP: levels I, II, III, and IV of GMFCS. Intensity: three sessions per week. Type of PA: iMOVE. | Individuals improved their gross motor skills, postural control, and participation in daily activities. Intensive therapy could be considered a more effective program than standard care for gross motor development. | The physicians in charge of performing the intervention were leaders in the area, which may make the comparison greater than in other centers. | The effect size was 1.3 points, with a 95% confidence interval. |
| Ogonowska-Słodownik et al. (2024) [43] | Analyzed the functionality and enjoyment of children with CP after participating in aquatic PA. Duration: NR. | Mixed | Sample size: 10 children. Sex: male and female Age: 9- and 10-year-old PC. Type or degree of CP: GMFCS levels II to IV. Intensity: NR. Type of PA: aquatic therapy. | The children who participated showed improvements in their level of performance, mental adaptation, and balance control in the water. In addition, their feelings of enjoyment and motivation increased. | The sample size was small and the study was conducted only with the population of a single center. | NR. |
| Benito et al. (2024) [44] | Evaluated the effect of an adapted ballet program on children with hemiplegic CP. Duration: nine months. | Longitudinal experimental study | Sample size: 15 children. Sex: NR. Age: 7 to 10 years old. Type or degree of CP: level I in GMFCS. Intensity: 2/3 sessions per week. Type of PA: Adapted ballet. | The intervention showed a positive impact on balance, body symmetry, and active participation. The program produced physical, emotional, and social benefits. | NR. | NR. |
| Yilmaz et al. (2023) [45] | Analyzed the influence of stabilization physical exercises on balance and proprioception. Duration: twelve months. | Mixed experimental design | Sample size: 20 children. Sex: male and female. Age: 4 to 12 years. Type or degree of CP: levels I and II on the GMFCS. Intensity: NR. Type of PA: core stability exercises. | The exercises had a positive impact on proprioception, balance, and trunk involvement. These improvements positively influence their postural control and quality of life. | NR. | NR. |
| Wang et al. (2023) [46] | Analyzed the efficacy of constraint-induced movement therapy (CIMT) in children with CP. Duration: thirty-six hours. | Mixed randomized trial | Sample size: 50 children. Sex: NR. Age: 4 to 12 years. Type or degree of CP: unilateral CP. Intensity: 2 sessions per week. Type of PA: movement therapy with restriction. | Following the program, improvements in children’s gross psychomotor skills were identified. Some individuals showed improved use of the affected arm at 8 weeks. The intensity of the intervention intervened positively in motor rehabilitation. | The sample size was small and the intervention lasted 8 weeks, so the long-term effects could not be observed. | NR. |
| Гpигyc & Haгopнa (2023) [47] | Evaluated the effectiveness of dance and movement therapy in children and adolescents in palliative care. Duration: two years. | Qualitative, descriptive | Sample size: 12 children. Sex: male and female. Age: 8 to 12 years. Type or grade of CP: levels IV and V of the GMFCS. Intensity: NR. Type of PA: dance. | Participation had a positive impact on individuals in three areas: participation in PA, context (more favorable for the child), and body structure–function (physical well-being and motor control). | The study was conducted at a single center and with a small sample size. | NR. |
| Hulst et al. (2023) [48] | Evaluated physical activity during the 24-hour daily cycle and PA guidelines in children with cerebral palsy. Duration: seven days. | Mixed NR | Sample size: 54 children. Sex: male and female Age: 3 to 12 years. Type or degree of CP: levels I, II, and III according to the GMFCS. Intensity: 744.2 min/day. Type of PA: NR. | Low rates related to sleep, PA, and sedentary lifestyles seek to promote a call for improving healthy lifestyles and reducing negative health issues. | NR. | NR. |
| Hamed et al. (2023) [49] | Analyzed the effectiveness of aquatic physical activity on the gross motor skills of children with CP. Duration: twelve weeks. | Mixed randomized, controlled trial | Sample size: 34 individuals. Sex: NR. Age: 3 to 5 years. Type or degree of CP: spastic CP. Intensity: three weekly sessions. Type of PA: “10 steps” therapy. | After the intervention, a positive impact was observed on the Gross Motor Function Measure scores: posture, balance, and mobility. | The intervention had a short duration (12 weeks). The continuity of the progress was not analyzed once the intervention was completed. | NR. Ninety-five percent confidence interval. |
| Cribb et al. (2023) [50] | To identify the associations between PA practice and mental health in children with CP. Duration: NR. | Quantitative, cross-sectional | Sample size: 458. Sex: NR. Age: 6 to 17 years. Type or degree of CP: NR. Intensity: NR. Type of PA: NR. | Individuals with CP are more likely to present mental health disorders, anxiety, depression, and conduct disorders. PA significantly reduces risk factors. | The information is collected through interviews conducted with parents and caregivers, so there may be biases in memory or perception. | NR. Ninety-five percent confidence interval. |
| Towns et al. (2022) [51] | Analyzed the balance confidence of children with CP. Duration: NR. | Descriptive, qualitative study | Sample size: eight children. Sex: male and female. Age: 9 to 17 years. Type or degree of CP: levels I and II of the GMFCS. Intensity: NR. Type of PA: NR. | Young people are concerned about losing their balance during PA. Loss of balance causes embarrassment and frustration, rather than fear. Social factors can make an environment pleasant when confidence in balance is low. | NR. | NR. |
| Lee et al. (2022) [52] | Analyzed the relationship between habitual PA and its relationship with the quality of life in children with CP. Duration: seven days. | Mixed | Sample size: 46 children. Sex: male and female. Age: 7.48 average age. Type or degree of CP: levels I, II, and III of the GMFCS. Intensity: NR. Type of PA: regular PA. | Energy expenditure can be used as an indicator to look at PA and quality of life in children with CP. In addition, it can be used as a biomarker of these two characteristics. | The small number of children and the specific characteristics make it impossible to generalize the results. | NR. |
| Lai et al. (2022) [53] | Analyzed the effectiveness of movement with music (M2M) with the aim of increasing physical activity in leisure time (LTPA). Duration: four weeks. | Mixed | Sample size: 58 children. Sex: male and female. Age: 10 to 19 years. Type or degree of CP: CP. Intensity: three sessions per week. Type of PA: M2M. | Efficacy in the inclusion of an M2M project as there is an increase in LTPA in children with CP. | The study used a small sample; the implementation would need to be analyzed in a larger trial. | They identify an effect size of 0.17. NR. |
| Arruda (2022) [54] | To evaluate the sedentary behavior and PA of children with CP and their relationship with body composition. Duration: seven days. | Mixed NR | Sample size: 53 children. Sex: male and female. Age: 2 to 10 years. Type or degree of CP: dyskinetic CP. Intensity: mild, moderate, and vigorous. Type of PA: regular PA. | Children with dyskinetic CP practiced more PA and were less sedentary than spastic children. Children with more severe CP had a delay in growth that led to less physical activity. | NR. | NR. |
| Reedman et al. (2021) [55] | Determined the predictors that improve the participation of children with CP in PA during their free time using Participate CP. Duration: eight weeks. | Mixed randomized, controlled trial with a waiting list | Sample size: 33 children. Sex: male and female. Age: 8 to 12 years. Type or degree of CP: CP. Intensity: 1 h per week. Type of PA: Leisure time physical activity participate in CP. | Children with intrinsic motivation from the beginning improved more. Those who met the treatment objectives achieved greater participation during PA. | Small sample. | NR. Ninety-five percent confidence interval. |
| Ostergaard et al. (2021) [56] | To identify the level of pain in children with CP and its relationship with participation in leisure PA. Duration: one year. | Mixed cross-sectional study | Sample size: 960 children. Sex: male and female. Age: 2 to 11 years. Type or degree of CP: levels I, II, III, IV, and V of the GMFCS. Intensity: NR. Type of PA: leisure PA. | A large percentage of children with CP have pain, which influences leisure PA. Interventions to reduce pain are important, as they help to reduce pain and favor the practice of PA. | NR. | NR. Ninety-five percent confidence interval. |
| Degerstedt et al. (2021) [57] | Analyzed the influence of sex, country, and functional factors on leisure PA practice in children with CP in Sweden. Duration: one year. | Mixed cross-sectional study | Sample size: 1935 children. Sex: male and female. Age: 6 to 18 years. Type or degree of CP: CP. Intensity: NR. Type of PA: NR. | Children born in Sweden were more likely to perform PA than those born outside Europe. Boys with CP performed more leisure PA than girls. | NR. | NR. Ninety-five percent confidence interval. |
| Williams et al. (2020) [58] | To describe the energy expenditure, body composition, and nutritional intake produced via PA in adolescents with PC. Duration: NR. | Mixed cross-sectional study | Sample size: 12 children. Sex: male and female. Age: 12 to 19 years. Type or degree of CP: children with CP at GMFCS levels II, III, IV, and V. Intensity: moderate to vigorous. Type of PA: adapted PA. | Adolescents with CP may have a high percentage of fat and high levels of sedentary and moderate to vigorous PA. It is important to monitor body fat percentage in adolescents with CP as it tends to be high, even though some have a level within their healthy range. | NR. | NR. |
| Wentz et al. (2020) [59] | Analyzed gait and PA in children with CP while considering gross motor function, age, and geographical location to assess the validity of the Early Activity Scale for Endurance. Duration: seven days. | Mixed prospective cohort study | Sample size: 79 children. Sex: male and female. Age: 11 years. Type or degree of CP: children with CP at levels I, II III, IV, and V of the GMFCS. Intensity: moderate to vigorous. Type of PA: regular PA. | Only the different levels of gross motor function marked significant differences in gait and moderate to vigorous PA. | The sample size, being so small, means that not as much data comes out as could exist. | NR. |
| Smit et al. (2020) [60] | Analyzed sleep and the relationship between its quality, PA, and sedentary behavior in children and adolescents with CP. Duration: seven days. | Mixed cross-sectional study | Sample size: 36 children. Sex: male and female. Age: 15 years. Type or degree of CP: children with spastic CP at levels I, II, III, and IV of the GMFCS. Intensity: NR. Type of PA: NR. | Children with CP have a recommended sleep duration and this is a factor that is related to the sedentary nature of children. | Little research based on different measures of sleep quality and quantity. | NR. |
| Jami-Vargas et al. (2020) [61] | To improve the development of gross motor skills in children with CP using the Matrogymnastics method. Duration: NR. | Mixed, descriptive | Sample size: 16 children. Sex: male and female. Age: 7 years. Type or degree of CP: PCI. Intensity: NR. Type of PA: matrogymnasia. | Matrogymnasia is an effective tool for the motor development of children, adding the participation of parents so that the exercise continues at home. | Longitudinal study, because after the study period, it is not clear whether the effects have been maintained or not. | NR. |
| Gerber et al. (2020) [62] | Analyzed the PA and gross motor skills of children and adolescents with CP and tried to understand their relationship. Duration: NR. | Qualitative clinical trial | Sample size: 25 children. Sex: male and female. Age: 8 to 20 years. Type or degree of CP: GMFCS level I, II, and III. Intensity: NR. Type of PA: NR. | The children spent 90% of their time sitting or passive and most of them had difficulty performing PA beyond 3 min. We did not see a strong relationship between motor ability and performance, but we did observe that a certain level of motor ability is necessary for PA performance. | There is no software that allows routine data analysis by healthcare providers who are not trained in clinical settings. | NR. |
| Bjornson et al. (2020) [63] | Analyzed the trajectories for the development of AF and walking function in children with CP. Duration: NR. | Mixed longitudinal study | Sample size: 79 children. Sex: male and female. Age: 3 to 12 years old. Type or degree of CP: children with CP of GMFCS levels I, II, III, IV, and V. Intensity: NR. Type of PA: marching. | The children did not reflect plateaus in PA or gait according to functional level; however, they showed a decrease in the quantity and quality of PA from 3 to 12 years of age. | NR. | NR. |
| Reedman et al. (2019) [64] | To determine the efficacy of a participation-based therapy to improve performance and satisfaction with free and habitual PA. Duration: twelve weeks. | Mixed | Sample size: 37 children. Sex: male and female. Age: 10 years old. Type or degree of CP: levels I, II, and III according to the GMFCS. Intensity: Light, moderate, and vigorous. Type of PA: Habitual PA. | Positive results were observed in increasing the performance of leisure PA goals by reducing barriers influencing participation. | The program did not produce changes in the average habitual PA. | NR. Ninety-five percent confidence interval. |
| Orlando et al. (2019) [65] | Analyzed self-initiated PA and its relationship with gross motor skills and the participation of children with CP. Duration: seven days. | Mixed NR | Sample size: 20 children. Sex: male and female. Age: 1–3 years. Type or degree of CP: non-ambulatory CP. Intensity: slight, moderate, and vigorous. Type of PA: NR. | The results showed non-significant values in the performance of games on the ground in gross motor skills and participation. | Independently measure PA, participation, and gross motor skills. | NR. |
| Morris et al. (2019) [66] | To determine the facilitators that promote PA in adolescents with CP. Duration: NR. | Mixed inductive, thematic study | Sample size: 15 children. Sex: male and female. Age: 12 to 18 years old. Type or degree of CP: children with CP at levels I, II, III, IV, and V according to the GMFCS. Intensity: NR. Type of PA: recreational. | They drew seven ideas: start, want to succeed, sense of belonging, the importance of the coach, endorsement to continue, support, and being passionate. These were synthesized into the Framework for Sustained Engagement. | NR. | NR. |
| Bar-Haim et al. (2019) [67] | Analyzed the changes in habitual PA and motor skills after the exercises. Duration: twelve weeks. | Mixed NR | Sample size: 54 children. Gender: male and female. Age: 12 to 20 years old. Type or degree of CP: bilateral spastic CP of GMFCS levels II and III. Intensity: Moderate to vigorous. Type of PA: Habitual PA. | Motor capacity improves after the interventions by seeing a growth in habitual PA. Intervention based on progressive group resistance training produces improvements in habitual PA, improving the social interaction and motivation that joint training brings. | NR. | NR. |
| Keawutan et al. (2018) [68] | Analyzed the relationship between habitual physical activity, sedentary behavior, and motor skills in children with CP. Duration: seven days. | Mixed cross-sectional study | Sample size: 67 children. Sex: male and female. Age: 4 to 5 years old. Type or degree of CP: PCI classified according to the GMFCS. Intensity: Light, moderate, and vigorous. Type of PA: Habitual PA. | Gross motor skills and ability are influenced by habitual PA and sedentary lifestyles. | Those children with progressive disorders were not included. | NR. |
| Keawutanet et al. (2018) [69] | Evaluated the quality of life in 5-year-old children with CP and related it to PA. Duration: seven days. | Mixed cross-sectional study | Sample size: 58 children. Sex: male and female. Age: 5 years. Type or degree of CP: levels I, II, III, IV, and V of the GMFCS. Intensity: Light, moderate, and vigorous. Type of PA: NR. | Children who engage in PA have a better quality of life than those who do not, due to the feelings of emotional well-being, self-esteem, and control of motor function that PA produces. | The habitual PA was not related to the quality of life reported by the parents. | NR. Ninety-five percent confidence interval. |
| Figueiredo et al. (2018) [70] | Analyzed the factors that influence the participation in PA among students with CP. Duration: NR. | Qualitative NR | Sample size: 10 people. Sex: male and female. Age: 12 to 14 years. Type or degree of CP: levels I to IV on the GMFCS. Intensity: NR. Type of PA: Team sports and recreational activities. | Personal and environmental factors, the attitudes of teachers, monitors, peers, and the variety of materials have a positive or negative influence on these 3 categories: “There is no way I can participate” (1), “I participate when” (2) and “It would be easier if” (3). | Unique perspective from the viewpoint of teenagers, without considering other agents in the environment. | NR. |
| Schasfoort et al. (2017) [71] | Evaluated the treatment with botulinum toxin and its combination with intensive physiotherapy. Duration: six months. | Mixed NR | Sample size: 65 children. Sex: male and female. Age: 4 to 12 years old. Type or degree of CP: CP. Intensity: NR. Type of PA: therapeutic and functional. | Combination treatment is not cost-effective when seeking to improve gross motor skills, PA levels, and quality of life. | NR. | NR. Ninety-five percent confidence interval. Intervalo de confianza del 95%. |
| Keawutan et al. (2017) [72] | Analyzed the PA of children aged 4 to 5 years with CP and sedentary behavior. Duration: seven days. | Mixed comparative analysis | Sample size: 7 children. Sex: male and female. Age: 4 to 5 years. Type or degree of CP: children with ambulatory and non-ambulatory CP. Intensity: light, moderate, and vigorous. Type of PA: NR. | Children spend a large part of their time in inactivity. Interventions are needed to reduce sedentary lifestyles and increase habitual PA. | Little basis of interventions to reduce sedentary behavior and promote PA. | NR. |
| Latorre-García (2017) [7] | Analyzed the relationship between water-based PA and motor development in children with CP. Duration: twelve weeks. | Mixed conceptual and experimental bibliography | Sample size: 12 children. Sex: male and female. Age: between 14 and 36 months. Type or degree of CP: CP. Intensity: two times per week. Moderate. Type of PA: Aquatic. | Infants with PCI were able to develop gross motor skills. They also strengthened others such as balance, coordination, motor learning, muscle tone, and endurance. | The presented study spans from September 2013 to December 2016. Although it continues to this day, no data is presented. | NR. |
| Hanh & Fernández (2017) [73] | Evaluated the effect of using postural insoles and ankle–foot orthoses on static and functional balance in children with CP. Duration: six weeks. | Mixed | Sample size: 20 children. Sex: male and female. Age: 4 to 12 years old. Type or degree of CP: spastic diplegic CP and levels I and II of the GMFCS. Intensity: NR. Type of PA: functional and balance. | The use of such supports improves balance and reduces anteroposterior and mediolateral sway. | NR. | NR. |
| Antón (2017) [74] | Analyzed whether hippotherapy produces long-term benefits in muscle spasticity. Duration: eight weeks. | Mixed NR | Sample size: 44 children. Sex: male and female. Age: 8–9 years Type or degree of CP: NR. Intensity: two per week. Type of PA: hippotherapy. | Children benefited from hip abductor strengthening following hippotherapy. | The intervention program lasts 12 weeks. | NR. |
| Oftedal et al. (2016) [75] | To describe the relationship between height, growth velocity, habitual PA, energy intake, and sedentary lifestyle. Duration: two years. | Mixed longitudinal study with mixed effects regression models | Sample size: 175 children. Sex: male and female. Age: 18 months to 5 years. Type or degree of CP: children with levels I, II, III, IV, and V according to the GMFCS. Intensity: Light, moderate, and vigorous. Type of PA: habitual PA. | Functional status and gestational age are two factors to take into account when assessing the growth of children. Increasing active time and PA is effective in improving growth and health. | NR. | NR. |
| Maher et al. (2016) [76] | Analyzed the relationships between PA and quality of life with the health and happiness of young people with CP. Duration: NR. | Mixed cross-sectional study | Sample size: 70 children. Sex: male and female. Age: 13 years and 11 months. Type or degree of CP: levels I, II, III, IV, and V children according to the GMFCS. Intensity: light, moderate, and vigorous. Type of PA: recreational and outdoor. | A positive relationship was found between PA, quality of life, and happiness. PA has potential benefits for improving the well-being of young people. PA is a predictor of children’s quality of life, health, and happiness. | Lack of clinical services and interventions aimed at increasing PA in children with CP. | NR. |
| Bania et al. (2016) [77] | Analyzed whether individualized resistance training increases the daily PA of children with CP. Duration: twelve weeks. | Mixed cross-sectional study | Sample size: 36 children. Sex: male and female. Age: 13 years and 11 months. Type or degree of CP: children with bilateral spastic CP. Intensity: three per week. Moderate and high. Type of PA: progressive resistance PA. | Resistance training can improve muscle strength, but it does not increase PA practice. Other strategies are needed to address low levels of PA. | Lack of strategies to address the low daily PA in young people with CP. | NR. |
| Aidar et al. (2016) [78] | Analyzed social function and aquatic PA in children with CP using the Pediatric Disability Assessment Inventory. Duration: twelve weeks. | Mixed NR | Sample size: 21 children. Sex: male and female. Age: 6 to 12 years. Type or degree of CP: CP. Intensity: 2–3 per week. Slight and moderate. Type of PA: aquatic. | The practice of aquatic exercises improved motor skills and, in a transversal way, social function, thus promoting the independence of the child with CP. | NR. | NR. |
| Ryan et al. (2015) [79] | To relate sedentary behavior, PA, and cardiorespiratory fitness in children with CP. Duration: seven days. | Mixed cross-sectional study | Sample size: 55 children. Sex: male and female. Age: 6 to 17 years. Type or degree of CP: Children with unilateral CP. Type of PA: habitual and spontaneous PA. Children with ambulatory CP of levels I and II of the GMFCS. Intensity: Light, moderate, and vigorous. | Vigorous activity is related to cardiorespiratory fitness in children with CP, but not light or moderate activity. Children with CP have low levels of cardiorespiratory fitness, central adiposity, and high blood pressure. | The cross-sectional design does not allow for establishing causal relationships. | NR. |
| Mitchell et al. (2015) [80] | Analyzed the PA and the proportion obtained by performing 60 min of moderate to vigorous PA daily in children and adolescents with CP. Duration: seven days. | Mixed cross-sectional study | Sample size: 102 children. Sex: male and female. Age: 11 years old. Type or degree of CP: children with unilateral CP of GMFCS levels I and II. Intensity: Light, moderate, and vigorous Type of PA: Habitual PA. | A high percentage of children with unilateral CP do not perform the recommended amount of PA to meet health recommendations. | Only children with unilateral CP were selected. | NR. |
| Mitchell et al. (2015) [81] | Analyzed the influence of physical, personal, and environmental characteristics on the practice of PA in children with unilateral CP. Duration: seven days. | Mixed cross-sectional study | Sample size: 102 children. Sex: male and female. Age: 8 to 17 years. Type or degree of CP: children with unilateral CP independent of GMFCS levels I and II. Intensity: Light, moderate, and vigorous. Type of PA: habitual and spontaneous PA. | Young age, gender, greater walking endurance, and greater participation in the home and community are factors that influence the PA of children with CP. | Only children with independent unilateral CP were selected. | NR. |
| Lauruschkus et al. (2015) [24] | Analyzed the experiences of children with CP, participation in PA, and the facilitators and barriers. Duration: twelve weeks. | Mixed Exploratory analysis study | Sample size: 16 children. Sex: male and female. Age: 8 to 11 years. Type or degree of CP: CP. Intensity: slight and moderate. Type of PA: individual. | Facilitators are summarized as: enjoying the feeling, being able, feeling connected, being aware that it is good for me, children want to be physically active, they want to have fun and enjoy the feeling of speed and doing new activities that encourage participation. Barriers are fatigue and accessibility to some activities or places. | The study could have been improved by asking the children about the physical activities they enjoy. | NR. |
| Balemans et al. (2015) [82] | Investigated the changes in physical fitness and PA levels related to walking and fatigue in children. Duration: one year. | Mixed analysis of a randomized, controlled trial | Sample size: 46 children. Sex: male and female. Age: 7 to 13 years. Type or degree of CP: children with bilateral and unilateral CP. Intensity: slight and moderate. Type of PA: walking. | In children with bilateral CP, there is a positive relationship between physical fitness and gait-related PA, whereas in unilateral CP, there was no connection. | The random coefficient regression analysis cannot be used to establish a causal relationship. | NR. |
| Van Wely et al. (2014) [83] | Analyzed the effectiveness of a 6- month PA program on social participation, self-perception, and quality of life. Duration: six months. | Mixed multicenter controlled trial with blinded allocation and evaluations | Sample size: 49 children. Sex: male and female. Age: 7 to 13 years. Type or degree of CP: children with spastic CP. Intensity: slight and moderate. Type of PA: habitual PA. | The intervention had positive benefits on social participation in domestic life at 12 months, not at 6 months. No relationship was found with social participation in recreation, leisure, self-perception, and quality of life. | NR. | NR. |
| Van Wely et al. (2014) [84] | Analyzed whether a 6-month PA program produces benefits in the child with CP. Duration: six months. | Mixed | Sample size: 49 children. Sex: male and female. Age: 7 to 13 years. Type or degree of CP: spastic CP and GMFCS severity I, II, and III. Intensity: mild and moderate. Type of PA: regular PA. | The program combining PA, counseling, and home therapy was not effective in children with CP. There was a trend of improvement in the children’s attitudes, clinically irrelevant, not for 6 months, but for 12 months. | Examined each variable of the population that intervenes separately to understand its influence. | NR. |
| Shkedy et al. (2014) [85] | Analyzed the duration and indicators of PA in the population in the Middle East. Duration: seven days. | Mixed NR | Sample size: 222 children Sex: male and female. Age: 16 years old. Type or degree of CP: children with bilateral CP of GMFCS levels II, III, and IV. Intensity: Light, moderate, and vigorous. Type of PA: regular PA. | The Mann–Whitney U test showed that there were differences in gross motor function and lower walking, standing, and sedentary activity at higher GMFCS levels. | Limited control over participant compliance may have resulted in some records being defective. | NR. |
| Lin & Chang (2014) [86] | Analyzed whether the Makey Makey program is useful for developing an intervention project. Duration: four weeks. | Mixed NR | Sample size: 1 girl. Sex: female. Age: 5 years and 9 months. Type or degree of CP: convulsive CP. Intensity: Three per week. Mild and moderate. Type of AF: Makey Makey. | Useful tools to motivate and improve children’s motor skills. Helen, a child who could not stretch her arm, improved her ability to extend it and pick up objects from a table with it. Each time she did so, she received a stimulus given by the program, which encouraged her intrinsic motivation. | This approach could have been used to receive interactive feedback independent of physical disabilities. | NR. |
| Bania et al. (2014) [87] | Analyzed daily PA levels in adolescents with CP and tried to show factors that help predict these levels. Duration: seven days. | Mixed. cross-sectional study | Sample size: 45 children. Sex: male and female. Age: 15 to 20 years. Type or degree of CP: children with bilateral spastic CP of GMFCS levels II and III. Intensity: light, moderate, and vigorous. Type of PA: habitual PA. | Adolescents and young adults with bilateral spastic CP who can walk with difficulty have reduced PA. Gross motor function is a predictor of daily PA. | The number of variables was limited by the sample and its size. | NR. |
| Tang et al. (2013) [88] | To evaluate the use of an activity monitor to observe PA in children with mobility problems due to CP. Duration: seven days. | Mixed evaluation study | Sample size: 15 children. Sex: male and female. Age: 5 to 17 years old. Type or degree of CP: children with ambulatory CP. Intensity: light, moderate, and vigorous. Type of PA: regular PA. | The activity monitor made it possible to analyze the sitting and upright postural states and the importance of taking into account the degree of severity according to the time and type of steps taken (walking, tiptoeing). PA in leisure time showed improvements. | NR. | NR. |
| Song (2013) [89] | Analyzed the relationship between physical, cognitive function, and daily PA in children with CP. Duration: NR. | Mixed NR | Sample size: 78 children. Sex: male and female. Age: 1 to 43 months. Type or degree of CP: CP. Intensity: NR. Type of PA: regular PA. | Physical and cognitive functions change whether the person can stand with assistance or without assistance. Age did not have a great influence. Cognitive function is related to physical function. Daily PA was affected by each type of CP. | Cognitive and physical impairments are not included in the examination and evaluation of CP. | NR. |
| Paternina (2013) [90] | Evaluated hippotherapy as a therapeutic alternative. Duration: twelve weeks. | Qualitative NR | Sample size: one person. Sex: female. Age: 4 years and 7 months. Type or degree of CP: dyskinetic CP. Intensity: Two per week. Mild and moderate. Type of PA: Hippotherapy. | Positive impact on the child’s development, mainly in gross motor skills and functional independence. The child developed skills in the right arm that she did not have before. | There is no assessment of basic devices that influence cognitive development such as visual acuity and hearing. | NR. |
| Howcroft et al. (2012) [91] | Analyzed the potential of active video games to promote PA and rehabilitation therapies in children with CP. Duration: eight weeks. | Mixed single-group experimental study | Sample size: 17 children. Sex: male and female. Age: 9 years. Type or degree of CP: CP. Intensity: Three per week. Thirty min. Moderate. Type of PA: dances and sports. | Moderate levels of PA were seen during dance and boxing practice. Angular velocities and accelerations were significant in the dominant arm. High levels of enjoyment. Positive tool to encourage light and moderate PA. | The small base of studies on variation in individual movements and playing styles. | NR. |
| Sandlund et al. (2011) [92] | Analyzed the practice of low-cost interactive games as a home-based intervention for children with CP. Duration: eight weeks. | Qualitative exploratory analysis | Sample size: 14 children. Gender: male and female. Age: 6 to 16 years old. Type or degree of CP: CP. Intensity: Two per week. Thirty–forty-five min. Light and moderate. Type of PA: Interactive movement games. | Motivation and practice compliance were high. PA increased during the intervention. Children’s physical performance improved. | More specific analysis of motor functions. | NR. |
| Van Wely et al. (2010) [93] | Analyzed the LEARN 2 MOVE 7–12 as a program to improve PA based on physical training and lifestyle. Duration: six weeks. | Mixed | Sample size: 50 children. Sex: male and female. Age: 7 to 12 years. Type or degree of CP: children with GMFCS levels I, II, and III spastic CP. Intensity: mild to moderate. Type of PA: habitual PA. | Lifestyle change and physiotherapeutic interventions improve physical training and PA in children with CP. | The effects obtained from the intervention cannot be related to a specific element. | NR. |
| Maher et al. (2010) [94] | Analyzed a PA-based intervention using the internet for 8 weeks in adolescents with CP. Duration: twelve weeks. | Mixed | Sample size: 72 children. Sex: male and female. Age: 12 to 16 years old. Type or degree of CP: unilateral and bilateral CP of levels I, II, and III of the GMFCS. Intensity: moderate. Type of PA: remote PA. | Short-term improvements in PA and knowledge were seen. Not comparable to face-to-face PA. | In order to present the results, it has focused on the best evidence. | NR. |
| Palisano et al. (2007) [22] | Analyzed PA from the point of view of adolescents with CP. Duration: NR. | Qualitative descriptive study | Sample size: 156 children. Sex: male and female. Age: 11 to 17 years old. Type or degree of CP: children with CP of GMFCS levels I, II, III, IV, and V. Intensity: slight and moderate. Type of PA: daily and recreational PA. | The performance of adolescents in PA with CP changed according to the degree of GMFCS. Depending on the level, there were greater difficulties in performing PA. | Lack of collaborative work between therapists and PA teachers working in clinical settings to carry out fitness programs. | NR. |
| Maltais et al. (2005) [95] | Analyzed the relationship between PA levels and oxygen costs during walking. Duration: NR. | Mixed NR | Sample size: 11 children. Sex: male and female. Age: 10 to 16 years old. Type or degree of CP: mild CP. Intensity: low and moderate. Type of PA: regular PA and walking. | Those with a low PA level had a higher oxygen cost when walking. | Lack of interventions to analyze whether interventions aimed at reducing the cost of oxygen improve the level of PA and vice versa. | NR. |
| Maltais et al. (2005) [96] | Analyzed the relationship between habitual PA and the biomechanical economy of treadmill walking. Duration: NR. | Mixed controlled trial | Sample size: 11 children. Sex: male and female. Age: 10 to 16 years. Type or degree of CP: mild CP. Intensity: NR. Type of PA: habitual PA and walking. | Those who possessed a high biomechanical gait economy on the treadmill were more physically active. Treadmill speed affected gait biomechanics, but not time. | NR. | NR. |
| Chad et al. (1999) [97] | Analyzed the effect of a weight-bearing PA program on bone content and bone density in children with CP. Duration: twenty-four weeks. | Mixed experimental study | Sample size: 18 children. Gender: male and female. Age: 9 years old. Type or degree of CP: spastic CP. Intensity: moderate and high. Type of PA: weight-bearing PA. | The intervention produced improvements in bone mineral accumulation. Minimal loading period positively affects patients osteogenically. | NR. | NR. |
| Van den Berg-Emons et al. (1998) [29] | Analyzed the influence of 9-month PA programs on the daily PA, fat, and physical fitness of children. Duration: twelve weeks. | Mixed controlled trial | Sample size: 20 children. Sex: male and female. Age: 9 years old. Type or degree of CP: spastic CP. Intensity: moderate and high. Type of PA: endurance, strength, and mobility training. | Aerobic training has a limited effect on PA in children with CP but slows deterioration and muscle strength. The training improves maximal aerobic power. | NR. | NR. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Andrés-Pérez, F.; Bru-Luna, L.M.; Hidalgo-Fuentes, S.; Llamas-Salguero, F.; Martí-Vilar, M. Influence of Physical Activity in Children and Adolescents with Cerebral Palsy: A Systematic Review. Children 2025, 12, 853. https://doi.org/10.3390/children12070853
Andrés-Pérez F, Bru-Luna LM, Hidalgo-Fuentes S, Llamas-Salguero F, Martí-Vilar M. Influence of Physical Activity in Children and Adolescents with Cerebral Palsy: A Systematic Review. Children. 2025; 12(7):853. https://doi.org/10.3390/children12070853
Chicago/Turabian StyleAndrés-Pérez, Faustino, Lluna Maria Bru-Luna, Sergio Hidalgo-Fuentes, Fátima Llamas-Salguero, and Manuel Martí-Vilar. 2025. "Influence of Physical Activity in Children and Adolescents with Cerebral Palsy: A Systematic Review" Children 12, no. 7: 853. https://doi.org/10.3390/children12070853
APA StyleAndrés-Pérez, F., Bru-Luna, L. M., Hidalgo-Fuentes, S., Llamas-Salguero, F., & Martí-Vilar, M. (2025). Influence of Physical Activity in Children and Adolescents with Cerebral Palsy: A Systematic Review. Children, 12(7), 853. https://doi.org/10.3390/children12070853