
Can the Oxygen Saturation Index Predict Severe Bronchopulmonary Dysplasia?


 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Sample Size
2.2. Statistical Analysis
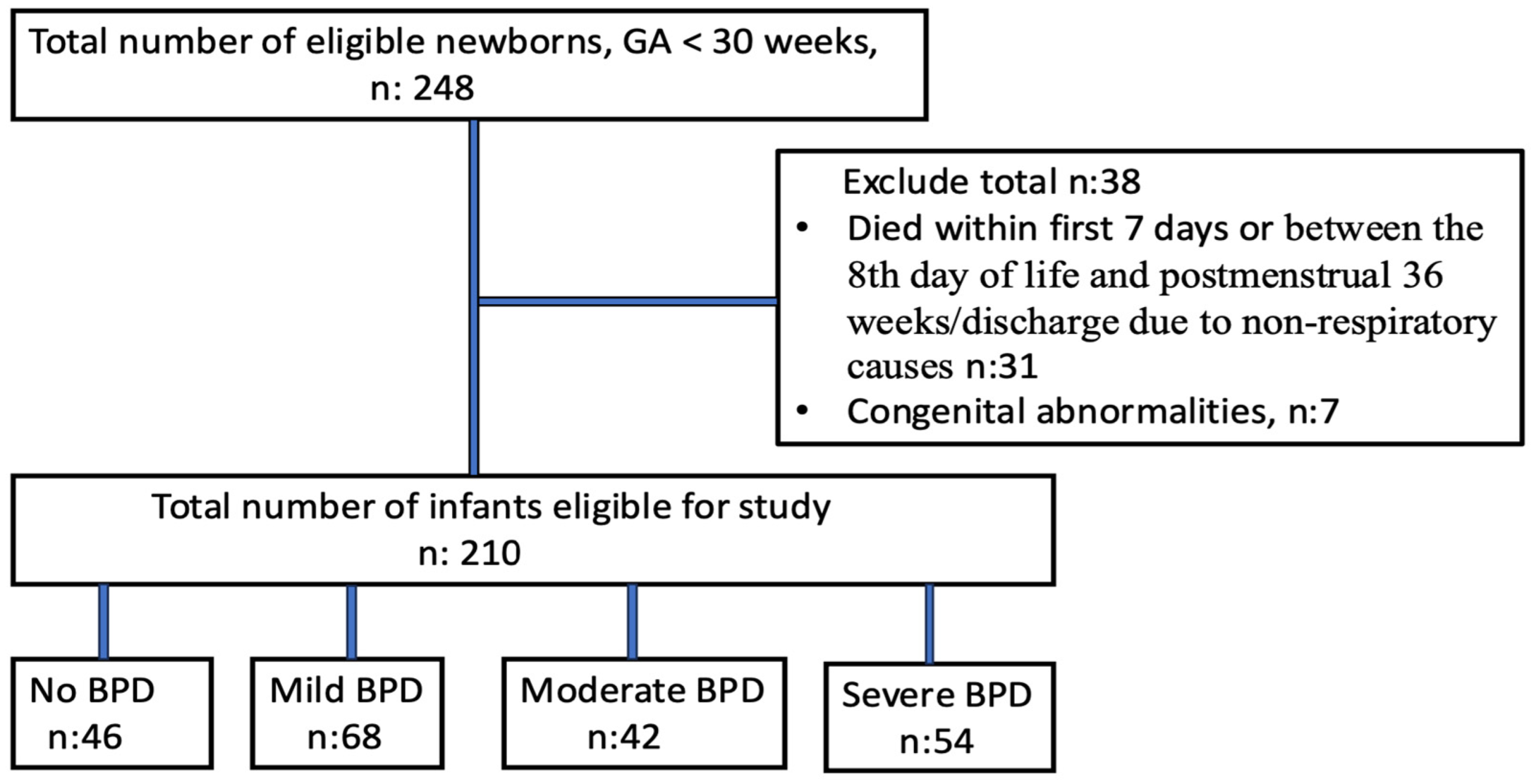
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| BPD | Bronchopulmonary dysplasia |
| OSI | Oxygen saturation index |
| FiO2 | Fraction of inspired oxygen |
| SpO2 | Oxygen saturation |
| MAP | Mean airway pressure |
| F | Gender |
| SGA | Small for gestational age |
| NEC | Necrotizing enterocolitis |
| HsPDA | Hemodynamically significant patent ductus arteriosus |
| IVH | Intraventricular hemorrhage |
| ROP | Retinopathy of prematurity |
References
- Stoll, B.J.; Hansen, N.I.; Bell, E.F.; Walsh, M.C.; Carlo, W.A.; Shankaran, S.; Laptook, A.R.; Sánchez, P.J.; Van Meurs, K.P.; Wyckoff, M.; et al. Eunice Kennedy Shriver National Institute of Child Health and Human Development Neonatal Research Network. Trends in Care Practices, Morbidity, and Mortality of Extremely Preterm Neonates, 1993–2012. JAMA 2015, 314, 1039–1051. [Google Scholar] [CrossRef] [PubMed]
- O’Reilly, M.; Sozo, F.; Harding, R. Impact of preterm birth and bronchopulmonary dysplasia on the developing lung: Long-term consequences for respiratory health. Clin. Exp. Pharmacol. Physiol. 2013, 40, 765–773. [Google Scholar] [CrossRef] [PubMed]
- Higgins, R.D.; Jobe, A.H.; Koso-Thomas, M.; Bancalari, E.; Viscardi, R.M.; Hartert, T.V.; Ryan, R.M.; Kallapur, S.G.; Steinhorn, R.H.; Konduri, G.G.; et al. Bronchopulmonary Dysplasia: Executive Summary of a Workshop. J. Pediatr. 2018, 197, 300–308. [Google Scholar] [CrossRef] [PubMed]
- Lal, C.V.; Ambalavanan, N. Biomarkers, Early Diagnosis, and Clinical Predictors of Bronchopulmonary Dysplasia. Clin. Perinatol. 2015, 42, 739–754. [Google Scholar] [CrossRef]
- van de Loo, M.; van Kaam, A.; Offringa, M.; Doyle, L.W.; Cooper, C.; Onland, W. Corticosteroids for the prevention and treatment of bronchopulmonary dysplasia: An overview of systematic reviews. Cochrane Database Syst. Rev. 2024, 4, CD013271. [Google Scholar] [CrossRef]
- Poets, C.F.; Lorenz, L. Prevention of bronchopulmonary dysplasia in extremely low gestational age neonates: Current evidence. Arch. Dis. Child. Fetal Neonatal Ed. 2018, 103, F285–F291. [Google Scholar] [CrossRef]
- Horbar, J.D.; Edwards, E.M.; Greenberg, L.T.; Morrow, K.A.; Soll, R.F.; Buus-Frank, M.E.; Buzas, J.S. Variation in Performance of Neonatal Intensive Care Units in the United States. JAMA Pediatr. 2017, 171, e164396. [Google Scholar] [CrossRef]
- Tan, Y.W.; Adamson, L.; Forster, C.; Davies, B.; Sharkey, D. Using serial oxygenation index as an objective predictor of survival for antenatally diagnosed congenital diaphragmatic hernia. J. Pediatr. Surg. 2012, 47, 1984–1989. [Google Scholar] [CrossRef]
- Muniraman, H.K.; Song, A.Y.; Ramanathan, R.; Fletcher, K.L.; Kibe, R.; Ding, L.; Biniwale, M. Evaluation of oxygen saturation index compared with oxygenation index in neonates with hypoxemic respiratory failure. JAMA Netw. Open 2019, 2, e191179. [Google Scholar] [CrossRef]
- Khalesi, N.; Choobdar, F.A.; Khorasani, M.; Sarvi, F.; Haghighi Aski, B.; Khodadost, M. Accuracy of oxygen saturation index in determining the severity of respiratory failure among preterm infants with respiratory distress syndrome. J. Matern. Fetal Neonatal Med. 2019, 34, 2334–2339. [Google Scholar] [CrossRef]
- Rawat, M.; Chandrasekharan, P.K.; Williams, A.; Gugino, S.; Koenigsknecht, C.; Swartz, D.; Ma, C.X.; Mathew, B.; Nair, J.; Lakshminrusimha, S. Oxygen saturation index and severity of hypoxic respiratory failure. Neonatology 2015, 107, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Thomas, N.J.; Shaffer, M.L.; Willson, D.F.; Shih, M.C.; Curley, M.A. Defining acute lung disease in children with the oxygenation saturation index. Pediatr. Crit. Care Med. 2010, 11, 12–17. [Google Scholar] [CrossRef]
- Thandaveshwara, D.; Chandrashekar Reddy, A.H.; Gopalakrishna, M.V.; Doreswamy, S.M. Saturation oxygenation pressure index: A non-invasive bedside measure for severity of respiratory disease in neonates on CPAP. Eur. J. Pediatr. 2021, 180, 1287–1292. [Google Scholar] [CrossRef]
- Doreswamy, S.M.; Chakkarapani, A.A.; Murthy, P. Saturation oxygen pressure index for assessment of pulmonary disease in neonates on non-invasive ventilation. Indian Pediatr. 2015, 52, 74–75. [Google Scholar] [PubMed]
- Bui-Binh-Bao, S.; Nguyen Thi, D.; Hoang Mai, L.; Do Ho Tinh, T.; Nguyen, T.T.B. Assessing hypoxic respiratory failure in mechanically ventilated neonates: A comparative study of oxygen saturation index and oxygenation index. PLoS ONE 2024, 19, e0304278. [Google Scholar] [CrossRef] [PubMed]
- Tsurukawa, S.; Zuiki, M.; Naito, Y.; Kitamura, K.; Matsumura, U.; Kanayama, T.; Ichise, E.; Horiguchi, G.; Teramukai, S.; Komatsu, H. Oxygenation saturation index in neonatal hypoxemic respiratory failure. Pediatr. Int. 2024, 66, e15753. [Google Scholar] [CrossRef]
- Khemani, R.G.; Rubin, S.; Belani, S.; Leung, D.; Erickson, S.; Smith, L.S.; Zimmerman, J.J.; Newth, C.J.L. Pulse oximetry vs. PaO2 metrics in mechanically ventilated children: Berlin definition of ARDS and mortality risk. Intensive Care Med. 2015, 41, 94–102. [Google Scholar] [CrossRef]
- Dargaville, P.A.; Aiyappan, A.; De Paoli, A.G.; Dalton, R.G.; Kuschel, C.A.; Kamlin, C.O.; Orsini, F.; Carlin, J.B.; Davis, P.G. Continuous positive airway pressure failure in preterm infants: Incidence, predictors, and consequences. Neonatology 2013, 104, 8–14. [Google Scholar] [CrossRef]
- Krishnegowda, S.; Doreswamy, S.M.; Thandaveshwar, D. Comprehensive, noninvasive saturation, oxygen, and pressure index: Does it reflect the severity of acute respiratory illness in neonates on continuous positive airway pressure? A prospective study. J. Clin. Neonatol. 2017, 6, 245. [Google Scholar] [CrossRef]
- Horn-Oudshoorn, E.J.J.; Vermeulen, M.J.; Crossley, K.J.; Cochius-den Otter, S.C.M.; Schnater, J.M.; Reiss, I.K.M.; DeKoninck, P.L.J. Oxygen Saturation Index in Neonates with a Congenital Diaphragmatic Hernia: A Retrospective Cohort Study. Neonatology 2022, 119, 111–118. [Google Scholar] [CrossRef]
- Htun, Z.T.; Schulz, E.V.; Desai, R.K.; Marasch, J.L.; McPherson, C.C.; Mastrandrea, L.D.; Jobe, A.H.; Ryan, R.M. Postnatal steroid management in preterm infants with evolving bronchopulmonary dysplasia. J. Perinatol. 2021, 41, 1783–1796. [Google Scholar] [CrossRef] [PubMed]
- Aziz, K.; Lee, H.C.; Escobedo, M.B.; Hoover, A.V.; Kamath-Rayne, B.D.; Kapadia, V.S.; Magid, D.J.; Niermeyer, S.; Schmölzer, G.M.; Szyld, E.; et al. Part 5: Neonatal Resuscitation 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Pediatrics 2021, 147 (Suppl. S1), e2020038505E. [Google Scholar] [CrossRef] [PubMed]
- Sweet, D.G.; Carnielli, V.P.; Greisen, G.; Hallman, M.; Klebermass-Schrehof, K.; Ozek, E.; Te Pas, A.; Plavka, R.; Roehr, C.C.; Saugstad, O.D.; et al. European Consensus Guidelines on the Management of Respiratory Distress Syndrome: 2022 Update. Neonatology 2023, 120, 3–23. [Google Scholar] [CrossRef]
- Glenski, J.A.; Marsh, H.M.; Hall, R.T. Calculation of mean airway pressure during mechanical ventilation in neonates. Crit. Care Med. 1984, 12, 642–644. [Google Scholar] [CrossRef]
- Chou, F.S.; Leigh, R.M.; Rao, S.S.; Narang, A.; Yeh, H.W. Oxygenation index in the first three weeks of life is a predictor of bronchopulmonary dysplasia grade in very preterm infants. BMC Pediatr. 2023, 23, 18. [Google Scholar] [CrossRef]
- Jobe, A.H.; Bancalari, E. Bronchopulmonary dysplasia. Am. J. Respir. Crit. Care Med. 2001, 163, 1723–1729. [Google Scholar] [CrossRef]
- Jensen, E.A. What is bronchopulmonary dysplasia and does caffeine prevent it? Semin. Fetal Neonatal Med. 2020, 25, 101176. [Google Scholar] [CrossRef] [PubMed]
- Sunil, B.; Nithya, E. Correlation of Oxygen Saturation Index and Oxygenation Index in Hypoxemic Respiratory Failure among Neonates. J. Clin. Diagn. Res. 2021, 15, SC06–SC08. [Google Scholar]
- Durlak, W.; Thébaud, B. BPD: Latest Strategies of Prevention and Treatment. Neonatology 2024, 121, 596–607. [Google Scholar] [CrossRef]
- Dini, G.; Ceccarelli, S.; Celi, F. Strategies for the prevention of bronchopulmonary dysplasia. Front. Pediatr. 2024, 12, 1439265. [Google Scholar] [CrossRef]
- Greenberg, R.G.; McDonald, S.A.; Laughon, M.M.; Tanaka, D.; Jensen, E.; Van Meurs, K.; Eichenwald, E.; Brumbaugh, J.E.; Duncan, A.; Walsh, M.; et al. Eunice Kennedy Shriver National Institute of Child Health and Human Development Neonatal Research Network. Online clinical tool to estimate risk of bronchopulmonary dysplasia in extremely preterm infants. Arch. Dis. Child. Fetal Neonatal Ed. 2022, 107, 638–643. [Google Scholar] [CrossRef] [PubMed]
- Kielt, M.J.; Logan, J.W.; Backes, C.H.; Conroy, S.; Reber, K.M.; Shepherd, E.G.; Nelin, L.D. Noninvasive Respiratory Severity Indices Predict Adverse Outcomes in Bronchopulmonary Dysplasia. J. Pediatr. 2022, 242, 129–136.e2. [Google Scholar] [CrossRef] [PubMed]
- Xing, W.; He, W.; Li, X.; Chen, J.; Cao, Y.; Zhou, W.; Shen, Q.; Zhang, X.; Ta, D. Early severity prediction of BPD for premature infants from chest X-ray images using deep learning: A study at the 28th day of oxygen inhalation. Comput. Methods Programs Biomed. 2022, 221, 106869. [Google Scholar] [CrossRef]
- Sharma, A.; Xin, Y.; Chen, X.; Sood, B.G. Early prediction of moderate to severe bronchopulmonary dysplasia in extremely premature infants. Pediatr. Neonatol. 2020, 61, 290–299. [Google Scholar] [CrossRef]
- Kostekci, Y.E.; Bakırarar, B.; Okulu, E.; Erdeve, O.; Atasay, B.; Arsan, S. An Early Prediction Model for Estimating Bronchopulmonary Dysplasia in Preterm Infants. Neonatology 2023, 120, 709–717. [Google Scholar] [CrossRef] [PubMed]
- Srivatsa, B.; Srivatsa, K.R.; Clark, R.H. Assessment of validity and utility of a bronchopulmonary dysplasia outcome estimator. Pediatr. Pulmonol. 2023, 58, 788–793. [Google Scholar] [CrossRef]
- Jung, Y.H.; Jang, J.; Kim, H.S.; Shin, S.H.; Choi, C.W.; Kim, E.K.; Kim, B.I. Respiratory severity score as a predictive factor for severe bronchopulmonary dysplasia or death in extremely preterm infants. BMC Pediatr. 2019, 19, 121. [Google Scholar]
- Di Fiore, J.M.; MacFarlane, P.M.; Martin, R.J. Intermittent Hypoxemia in Preterm Infants. Clin. Perinatol. 2019, 46, 553–565. [Google Scholar] [CrossRef]
- Jensen, E.A.; Whyte, R.K.; Schmidt, B.; Bassler, D.; Vain, N.E.; Roberts, R.S. Canadian Oxygen Trial Investigators. Association between Intermittent Hypoxemia and Severe Bronchopulmonary Dysplasia in Preterm Infants. Am. J. Respir. Crit. Care Med. 2021, 204, 1192–1199. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| N = 210 | |
|---|---|
| Gestational age (days) | 28.1 ± 2.9 |
| Birth weight (g), mean ± SD | 1105 ± 405 |
| Gender (F), n (%) | 107 (51.2) |
| Delivery mode (VD), n (%) | 68 (32.4) |
| SGA, n (%) | 23 (11.0) |
| Antenatal steroid, n (%) | 113 (53.8) |
| Chorioamnionitis, n (%) | 10 (4.8) |
| Delivery room intubation, n (%) | 122 (58.1) |
| IVH grade ≥2, n (%) | 26 (12.4) |
| NEC stage ≥2B, n (%) | 21 (10.0) |
| ROP (requiring treatment), n (%) | 21 (10.0) |
| HsPDA n (%) | 93 (44.3) |
| Late postnatal steroid, n (%) | 51 (24.3) |
| İnvasive mechanical ventilation duration (days) | 4 (0–21) |
| Non-invasive mechanical ventilation duration (days) | 28 (6–54) |
| BPD, n (%) | 164 (78.1) |
| Mild BPD, n (%) | 68 (32.3) |
| Moderate BPD, n (%) | 42 (20.0) |
| Severe BPD, n (%) | 54 (25.7) |
| Hospital stay (days), mean ± SD | 63 (37–103) |
| Infants Without Severe BPD (n = 156) | Infants with Severe BPD/Death (n = 54) | p | |
|---|---|---|---|
| Gestational age (days) | 29.0 ± 2.0 | 25.9 ± 3.4 | <0.001 |
| Birth weight (g), mean ± SD | 1273 ± 373 | 777 ± 232 | <0.001 |
| Gender (F), n (%) | 74 (49.6) | 33 (54.1) | 0.759 |
| Delivery mode (VD), n (%) | 47 (31.5) | 20 (32.8) | 0.160 |
| SGA, n (%) | 12 (8.1) | 11 (18.0) | 0.135 |
| Antenatal steroid, n (%) | 78 (52.3) | 34 (55.7) | 0.449 |
| Chorioamnionitis, n (%) | 4 (2.7) | 6 (9.8) | 0.022 |
| Delivery room intubation, n (%) | 67 (44.9) | 54 (88.5) | <0.001 |
| IVH grade ≥2, n (%) | 11 (7.4) | 15 (24.6) | <0.001 |
| NEC stage ≥2B, n (%) | 5 (3.4) | 15 (24.6) | <0.001 |
| ROP (requiring treatment), n (%) | 6 (4.0) | 15 (24.6) | <0.001 |
| HsPDA n (%) | 45 (30.2) | 47 (77.0) | <0.001 |
| Late postnatal steroid, n (%) | 15 (10.1) | 35 (57.4) | <0.001 |
| İnvasive mechanical ventilation duration (days), median (range min–max) | 4 (0– 101) | 9 (3–260) | <0.001 |
| Non-invasive mechanical ventilation duration (days), mean ± SD/median (range min–max) | 18 (3–115) | 31 (0–153) | <0.001 |
| Hospital stay (days), mean ± SD | 62.4 ± 36.7 | 112.5 ± 65.0 | <0.001 |
| OSI (Postnatal Days) | Infants Without Severe BPD | Infants with Severe BPD | p |
|---|---|---|---|
| 3 | 2.1 (1.3–2.4) | 2.7 (2.2–3.7) | 0.07 |
| 7 | 2.0 (1.1–2.2) | 2.6 (2.1–3.4) | 0.06 |
| 14 | 1.3 (0.9–2.2) | 4.9 (3.5–6.6) | <0.001 |
| 21 | 1.3 (0.9–1.9) | 3.5 (3.1–4.4) | <0.001 |
| 28 | 1.4 (0.8–1.9) | 2.8 (2.2–3.7) | <0.001 |
| Sensitivity | Specificity | PPV | NPV | AUC | Metric Score | ||
|---|---|---|---|---|---|---|---|
| OSI-14 | 3.6 | 89.09% | 81.05% | 73.13% | 92.77% | 0.93 | 1.7 |
| 3.4 | 87.27% | 82.11% | 73.85% | 91.76% | 0.93 | 1.69 | |
| 3.3 | 83.64% | 87.37% | 79.31% | 90.22% | 0.93 | 1.71 | |
| 3.2 | 83.64% | 89.47% | 82.14% | 90.43% | 0.93 | 1.73 | |
| 2.6 | 78.18% | 90.53% | 82.69% | 87.76% | 0.93 | 1.69 | |
| 2.5 | 74.55% | 94.74% | 89.13% | 86.54% | 0.93 | 1.69 | |
| OSI-21 | 2.8 | 80% | 90.59% | 83.33% | 88.51% | 0.92 | 1.71 |
| 2.9 | 80% | 91.76% | 85.11% | 88.64% | 0.92 | 1.72 | |
| 3 | 80% | 95.29% | 90.91% | 89.01% | 0.92 | 1.75 | |
| 3.1 | 76% | 96.47% | 92.68% | 87.23% | 0.92 | 1.72 | |
| Delivery room intubation | 2 | 94.55% | 54.84% | 42.62% | 96.59% | 0.75 | 1.49 |
| OSI-14 < 3.6 + OSI-21 < 3.0 + Delivery room intubation | 2 | 86% | 84.52% | 76.79% | 91.03% | 0.92 | 1.71 |
| 3 | 72% | 98.81% | 97.30% | 85.57% | 0.92 | 1.71 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ozdemir, H.; Gulcan Kersin, S.; Memisoglu, A.; Kandemir, I.; Bilgen, H.S. Can the Oxygen Saturation Index Predict Severe Bronchopulmonary Dysplasia? Children 2025, 12, 582. https://doi.org/10.3390/children12050582
Ozdemir H, Gulcan Kersin S, Memisoglu A, Kandemir I, Bilgen HS. Can the Oxygen Saturation Index Predict Severe Bronchopulmonary Dysplasia? Children. 2025; 12(5):582. https://doi.org/10.3390/children12050582
Chicago/Turabian StyleOzdemir, Hulya, Sinem Gulcan Kersin, Asli Memisoglu, Ibrahim Kandemir, and Hulya Selva Bilgen. 2025. "Can the Oxygen Saturation Index Predict Severe Bronchopulmonary Dysplasia?" Children 12, no. 5: 582. https://doi.org/10.3390/children12050582
APA StyleOzdemir, H., Gulcan Kersin, S., Memisoglu, A., Kandemir, I., & Bilgen, H. S. (2025). Can the Oxygen Saturation Index Predict Severe Bronchopulmonary Dysplasia? Children, 12(5), 582. https://doi.org/10.3390/children12050582