
Interleukin-2 Receptor as a Marker of Oxidative Stress in Paediatric Patients with Chronic Kidney Disease or Hypertension

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kattoor, A.J.; Pothineni, N.V.K.; Palagiri, D.; Mehta, J.L. Oxidative stress in atherosclerosis. Curr. Atheroscler. Rep. 2017, 19, 42. [Google Scholar] [CrossRef] [PubMed]
- Szczurek, W.; Szyguła-Jurkiewicz, B. Oxidative stress and inflammatory markers—The future of heart failure diagnostics? Kardiochir. Torakochirurgia Pol. 2015, 12, 145–149. [Google Scholar] [CrossRef] [PubMed]
- Chaudhary, P.; Janmeda, P.; Docea, A.O.; Yeskaliyeva, B.; Abdull Razis, A.F.; Modu, B.; Calina, D.; Sharifi-Rad, J. Oxidative stress, free radicals and antioxidants: Potential crosstalk in the pathophysiology of human diseases. Front. Chem. 2023, 11, 1158198. [Google Scholar] [CrossRef] [PubMed]
- Libby, P. Inflammation in atherosclerosis. Arterioscler. Thromb. Vasc. Biol. 2012, 32, 2045–2051. [Google Scholar] [CrossRef]
- Fayad, Z.A.; Amirbekian, V.; Toussaint, J.F.; Fuster, V. Identification of interleukin-2 for imaging atherosclerotic inflammation. Eur. J. Nucl. Med. Mol. Imaging 2006, 33, 111–116. [Google Scholar] [CrossRef]
- Simon, A.D.; Yazdani, S.; Wang, W.; Schwartz, A.; Rabbani, L.E. Elevated plasma levels of interleukin-2 and soluble IL-2 receptor in ischemic heart disease. Clin. Cardiol. 2001, 24, 253–256. [Google Scholar] [CrossRef]
- Hong, Y.M. Atherosclerotic cardiovascular disease beginning in childhood. Korean Circ. J. 2010, 40, 1–9. [Google Scholar] [CrossRef]
- Kotur-Stevuljević, J.; Peco-Antić, A.; Spasić, S.; Stefanović, A.; Paripović, D.; Kostić, M.; Vasić, D.; Vujović, A.; Jelić-Ivanović, Z.; Spasojević-Kalimanovska, V.; et al. Hyperlipidemia, oxidative stress, and intima media thickness in children with chronic kidney disease. Pediatr. Nephrol. 2013, 28, 295–303. [Google Scholar] [CrossRef]
- Ece, A.; Gürkan, F.; Kervancioğlu, M.; Kocamaz, H.; Güneş, A.; Atamer, Y.; Selek, S. Oxidative stress, inflammation and early cardiovascular damage in children with chronic renal failure. Pediatr. Nephrol. 2006, 21, 545–552. [Google Scholar] [CrossRef]
- Drożdż, D.; Kwinta, P.; Sztefko, K.; Kordon, Z.; Drożdż, T.; Łątka, M.; Miklaszewska, M.; Zachwieja, K.; Rudziński, A.; Pietrzyk, J.A. Oxidative stress biomarkers and left ventricular hypertrophy in children with chronic kidney disease. Oxid. Med. Cell Longev. 2016, 2016, 7520231. [Google Scholar] [CrossRef]
- Bujanowicz, A.; Skrzypczyk, P. Immunological mechanisms of arterial damage in pediatric patients with primary hypertension. Cent. Eur. J. Immunol. 2023, 48, 150–157. [Google Scholar] [CrossRef] [PubMed]
- Calcaterra, V.; Regalbuto, C.; Porri, D.; Pelizzo, G.; Mazzon, E.; Vinci, F.; Zuccotti, G.; Fabiano, V.; Cena, H. Inflammation in Obesity-Related Complications in Children: The Protective Effect of Diet and Its Potential Role as a Therapeutic Agent. Biomolecules 2020, 10, 1324. [Google Scholar] [CrossRef] [PubMed]
- Correia-Costa, L.; Sousa, T.; Morato, M.; Cosme, D.; Afonso, J.; Areias, J.C.; Schaefer, F.; Guerra, A.; Afonso, A.C.; Azevedo, A.; et al. Oxidative stress and nitric oxide are increased in obese children and correlate with cardiometabolic risk and renal function. Br. J. Nutr. 2016, 116, 805–815. [Google Scholar] [CrossRef] [PubMed]
- Hertiš Petek, T.; Homšak, E.; Svetej, M.; Marčun Varda, N. Metabolic Syndrome, Inflammation, Oxidative Stress, and Vitamin D Levels in Children and Adolescents with Obesity. Int. J. Mol. Sci. 2024, 25, 10599. [Google Scholar] [CrossRef]
- Codazzi, V.; Frontino, G.; Galimberti, L.; Giustina, A.; Petrelli, A. Mechanisms and risk factors of metabolic syndrome in children and adolescents. Endocrine 2024, 84, 16–28. [Google Scholar] [CrossRef]
- Močnik, M.; Golob Jančič, S.; Marčun Varda, N. Liver and kidney ultrasound elastography in children and young adults with hypertension or chronic kidney disease. Pediatr. Nephrol. 2023, 38, 3379–3387. [Google Scholar] [CrossRef]
- Lurbe, E.; Agabiti-Rosei, E.; Cruickshank, J.K.; Dominiczak, A.; Erdine, S.; Hirth, A.; Invitti, C.; Litwin, M.; Mancia, G.; Pall, D.; et al. 2016 European Society of Hypertension guidelines for the management of high blood pressure in children and adolescents. J. Hypertens. 2016, 34, 1887–1920. [Google Scholar] [CrossRef]
- Akern. In Bodygram Plus Software Guide; Akern s.r.l.: Florence, Italy, 2016.
- Marčun Varda, N.; Golob Jančič, S.; Močnik, M. Obesity and body composition in relation to liver and kidney ultrasound elastography in paediatric patients with either hypertension or chronic kidney disease. Children 2023, 11, 18. [Google Scholar] [CrossRef]
- Ding, R.; Gao, W.; Ostrodci, D.H.; He, Z.; Song, Y.; Ma, L.; Liang, C.; Wu, Z. Effect of interleukin-2 level and genetic variants on coronary artery disease. Inflammation 2013, 36, 1225–1231. [Google Scholar] [CrossRef]
- Elkind, M.S.; Rundek, T.; Sciacca, R.R.; Ramas, R.; Chen, H.J.; Boden-Albala, B.; Rabbani, L.; Sacco, R.L. Interleukin-2 levels are associated with carotid artery intima-media thickness. Atherosclerosis 2005, 180, 181–187. [Google Scholar] [CrossRef]
- Malek, T.R.; Castro, I. Interleukin-2 receptor signaling: At the interface between tolerance and immunity. Immunity 2010, 33, 153–165. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Rickert, M.; Garcia, K.C. Structure of the quaternary complex of interleukin-2 with its alpha, beta, and gammac receptors. Science 2005, 310, 1159–1163. [Google Scholar] [CrossRef] [PubMed]
- Durda, P.; Sabourin, J.; Lange, E.M.; Nalls, M.A.; Mychaleckyj, J.C.; Jenny, N.S.; Li, J.; Walston, J.; Harris, T.B.; Psaty, B.M.; et al. Plasma levels of soluble interleukin-2 receptor α: Associations with clinical cardiovascular events and genome-wide association scan. Arterioscler. Thromb. Vasc. Biol. 2015, 35, 2246–2253. [Google Scholar] [CrossRef]
- Teraura, H.; Kotani, K.; Minami, T.; Takeshima, T.; Shimooki, O.; Kajii, E. The serum concentration of soluble interleukin-2 receptor in patients with Kawasaki disease. Ann. Clin. Biochem. 2017, 54, 209–213. [Google Scholar] [CrossRef]
- Bien, E.; Balcerska, A. Serum soluble interleukin 2 receptor alpha in human cancer of adults and children: A review. Biomarkers 2008, 13, 1–26. [Google Scholar] [CrossRef]
- Al-Rawi, K.F.; Ali, H.H.; Guma, M.A.; Mohammed Aldahham, B.J.; Tuleab Alaaraji, S.F.; Al-Ani, O.; Tariq Ali, A. Relationship between IL-2, IL-17 concentrations, and serum creatinine levels in men with chronic kidney diseases. Rep. Biochem. Mol. Biol. 2022, 10, 664–674. [Google Scholar] [CrossRef]
- Silverstein, D.M. Inflammation in chronic kidney disease: Role in the progression of renal and cardiovascular disease. Pediatr. Nephrol. 2009, 24, 1445–1452. [Google Scholar] [CrossRef]
- Zwolińska, D.; Medyńska, A.; Szprynger, K.; Szczepańska, M. Serum concentration of IL-2, IL-6, TNF-alpha and their soluble receptors in children on maintenance hemodialysis. Nephron 2000, 86, 441–446. [Google Scholar] [CrossRef]
- Nairn, J.; Hodge, G.; Henning, P. Intracellular cytokines in peripheral blood leucocytes in children with chronic renal failure. Pediatr. Nephrol. 2006, 21, 251–256. [Google Scholar] [CrossRef]
- Eder, K.; Baffy, N.; Falus, A.; Fulop, A.K. The major inflammatory mediator interleukin-6 and obesity. Inflamm. Res. 2009, 58, 727–736. [Google Scholar] [CrossRef]
- Fain, J.N. Release of interleukins and other inflammatory cytokines by human adipose tissue is enhanced in obesity and primarily due to the nonfat cells. Vitam. Horm. 2006, 74, 443–477. [Google Scholar] [CrossRef] [PubMed]
- Jonas, M.I.; Kurylowicz, A.; Bartoszewicz, Z.; Lisik, W.; Jonas, M.; Wierzbicki, Z.; Chmura, A.; Pruszczyk, P.; Puzianowska-Kuznicka, M. Interleukins 6 and 15 levels are higher in subcutaneous adipose tissue, but obesity is associated with their increased content in visceral fat depots. Int. J. Mol. Sci. 2015, 16, 25817–25830. [Google Scholar] [CrossRef] [PubMed]
- Tuomisto, K.; Jousilahti, P.; Havulinna, A.S.; Borodulin, K.; Männistö, S.; Salomaa, V. Role of inflammation markers in the prediction of weight gain and development of obesity in adults—A prospective study. Metabol. Open 2019, 3, 100016. [Google Scholar] [CrossRef] [PubMed]
- Kochumon, S.; Al Madhoun, A.; Al-Rashed, F.; Thomas, R.; Sindhu, S.; Al-Ozairi, E.; Al-Mulla, F.; Ahmad, R. Elevated adipose tissue associated IL-2 expression in obesity correlates with metabolic inflammation and insulin resistance. Sci. Rep. 2020, 10, 16364. [Google Scholar] [CrossRef]
- van der Zalm, I.J.B.; van der Valk, E.S.; Wester, V.L.; Nagtzaam, N.M.A.; van Rossum, E.F.C.; Leenen, P.J.M.; Dik, W.A. Obesity-associated T-cell and macrophage activation improve partly after a lifestyle intervention. Int. J. Obes. 2020, 44, 1838–1850. [Google Scholar] [CrossRef]
- Schmidt, F.M.; Weschenfelder, J.; Sander, C.; Minkwitz, J.; Thormann, J.; Chittka, T.; Mergl, R.; Kirkby, K.C.; Faßhauer, M.; Stumvoll, M.; et al. Inflammatory cytokines in general and central obesity and modulating effects of physical activity. PLoS ONE 2015, 10, e0121971. [Google Scholar] [CrossRef]
- Vargas, R.; Ryder, E.; Diez-Ewald, M.; Mosquera, J.; Durán, A.; Valero, N.; Pedreañez, A.; Peña, C.; Fernández, E. Increased C-reactive protein and decreased Interleukin-2 content in serum from obese individuals with or without insulin resistance: Associations with leukocyte count and insulin and adiponectin content. Diabetes Metab. Syndr. 2016, 10, S34–S41. [Google Scholar] [CrossRef]
- Meijer, K.; de Vries, M.; Al-Lahham, S.; Bruinenberg, M.; Weening, D.; Dijkstra, M.; Kloosterhuis, N.; van der Leij, R.J.; van der Want, H.; Kroesen, B.J.; et al. Human primary adipocytes exhibit immune cell function: Adipocytes prime inflammation independent of macrophages. PLoS ONE 2011, 6, e17154. [Google Scholar] [CrossRef]
- Aygun, A.D.; Gungor, S.; Ustundag, B.; Gurgoze, M.K.; Sen, Y. Proinflammatory cytokines and leptin are increased in serum of prepubertal obese children. Mediators Inflamm. 2005, 2005, 180–183. [Google Scholar] [CrossRef]
- Dogan, Y.; Akarsu, S.; Ustundag, B.; Yilmaz, E.; Gurgoze, M.K. Serum IL-1beta, IL-2, and IL-6 in insulin-dependent diabetic children. Mediators Inflamm. 2006, 2006, 59206. [Google Scholar] [CrossRef]
- Utsal, L.; Tillmann, V.; Zilmer, M.; Mäestu, J.; Purge, P.; Jürimäe, J.; Saar, M.; Lätt, E.; Maasalu, K.; Jürimäe, T. Elevated serum IL-6, IL-8, MCP-1, CRP, and IFN-γ levels in 10- to 11-year-old boys with increased BMI. Horm. Res. Paediatr. 2012, 78, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Rosa, J.S.; Heydari, S.; Oliver, S.R.; Flores, R.L.; Pontello, A.M.; Ibardolaza, M.; Galassetti, P.R. Inflammatory cytokine profiles during exercise in obese, diabetic, and healthy children. J. Clin. Res. Pediatr. Endocrinol. 2011, 3, 115–121. [Google Scholar] [CrossRef] [PubMed]
- Mihuta, M.S.; Paul, C.; Borlea, A.; Roi, C.M.; Velea-Barta, O.A.; Mozos, I.; Stoian, D. Unveiling the Silent Danger of Childhood Obesity: Non-Invasive Biomarkers Such as Carotid Intima-Media Thickness, Arterial Stiffness Surrogate Markers, and Blood Pressure Are Useful in Detecting Early Vascular Alterations in Obese Children. Biomedicines 2023, 11, 1841. [Google Scholar] [CrossRef] [PubMed]
- Savant, J.D.; Furth, S.L.; Meyers, K.E. Arterial stiffness in children: Pediatric measurement and considerations. Pulse 2014, 2, 69–80. [Google Scholar] [CrossRef]

{kind=link}
| Variable | CKD Group (N = 46) MW | HTN Group (N = 50) MW | Control Group (N = 33) | KW |
|---|---|---|---|---|
| IL-2Rα (pg/mL) | 232 (118) p = 0.160 | 147 (35) p < 0.001 | 295 (172) | p< 0.001 |
| Overweight/Obesity (N = 51) | Normal Weight (N = 78) | Comparison (MW) | ||
| IL-2Rα (pg/mL) | 162 (119) | 286.5 (186) | p< 0.001 | |
| Anthropometric Measurements, Body Composition, Blood Pressure, Elastography Measurements | Laboratory Measurements | ||
|---|---|---|---|
| Variable | IL-2Rα | Variable | IL-2Rα |
| Age | r = −0.188 p = 0.038 | AST | r = 0.047 p = 0.606 |
| Height | r = −0.256 p = 0.004 | ALT | r = −0.178 p = 0.049 |
| Weight | r = −0.447 p < 0.001 | GGT | r = −0.265 p = 0.003 |
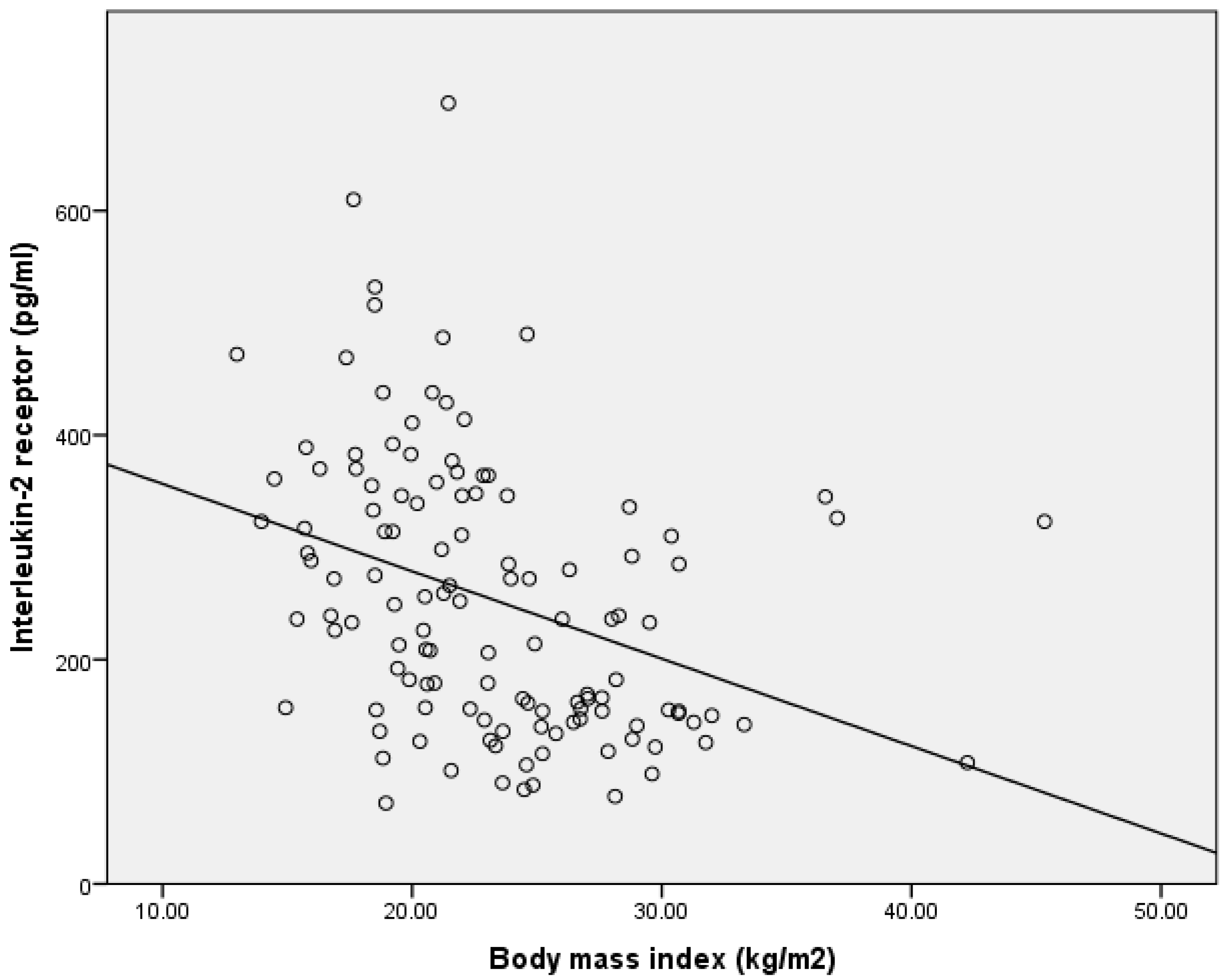
| BMI | r = −0.443 p < 0.001 | Urea | r = 0.182 p = 0.044 |
| Waist circumference | r = −0.477 p < 0.001 | Creatinine | r = 0.045 p = 0.623 |
| Hip circumference | r = −0.441 p < 0.001 | Cystatin C | r = 0.288 p = 0.002 |
| FFM | r = −0.335 p < 0.001 | Urate | r = −0.199 p = 0.039 |
| TBW | r = −0.316 p = 0.001 | Total cholesterol | r = −0.013 p = 0.889 |
| ECW | r = −0.284 p = 0.003 | LDL | r = −0.060 p = 0.515 |
| BCM | r = −0.350 p < 0.001 | HDL | r = 0.203 p = 0.027 |
| FM | r = −0.484 p < 0.001 | Triglycerides | r = −0.220 p = 0.016 |
| PA | r = −0.307 p = 0.001 | Vitamin D | r = 0.116 p = 0.210 |
| Systolic pressure | r = −0.442 p < 0.001 | Homocysteine | r = −0.086 p = 0.367 |
| Diastolic pressure | r = −0.142 p = 0.117 | Urinary albumin/creatinine | r = 0.318 p = 0.001 |
| Pulse wave velocity | r = −0.047 p = 0.661 | ||
| Liver elastography | r = −0.184 p = 0.041 | ||
| Left kidney elastography | r = −0.355 p < 0.001 | ||
| Right kidney elastography | r = −0.292 p = 0.001 | ||
| Dependent Variable | Beta Coefficient | Significance |
|---|---|---|
| Systolic pressure | −2.748 | 0.011 |
| Diastolic pressure | +0.050 | 0.973 |
| Creatinine | +0.468 | 0.488 |
| Cystatin C | +204.676 | 0.021 |
| Urinary albumin/creatinine | +0.077 | 0.894 |
| Body mass index | −4.946 | 0.040 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marčun Varda, N.; Močnik, M.; Filipič, M.; Homšak, E.; Svetej, M.; Golob Jančič, S. Interleukin-2 Receptor as a Marker of Oxidative Stress in Paediatric Patients with Chronic Kidney Disease or Hypertension. Children 2025, 12, 569. https://doi.org/10.3390/children12050569
Marčun Varda N, Močnik M, Filipič M, Homšak E, Svetej M, Golob Jančič S. Interleukin-2 Receptor as a Marker of Oxidative Stress in Paediatric Patients with Chronic Kidney Disease or Hypertension. Children. 2025; 12(5):569. https://doi.org/10.3390/children12050569
Chicago/Turabian StyleMarčun Varda, Nataša, Mirjam Močnik, Martina Filipič, Evgenija Homšak, Mateja Svetej, and Sonja Golob Jančič. 2025. "Interleukin-2 Receptor as a Marker of Oxidative Stress in Paediatric Patients with Chronic Kidney Disease or Hypertension" Children 12, no. 5: 569. https://doi.org/10.3390/children12050569
APA StyleMarčun Varda, N., Močnik, M., Filipič, M., Homšak, E., Svetej, M., & Golob Jančič, S. (2025). Interleukin-2 Receptor as a Marker of Oxidative Stress in Paediatric Patients with Chronic Kidney Disease or Hypertension. Children, 12(5), 569. https://doi.org/10.3390/children12050569