
Improving Postoperative Pediatric Recovery by Efficient Recovery Room Care—A Comprehensive Review

Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Post-Anesthetic Recovery Room
3.1.1. Essential Infrastructure and Equipment
- Reliable access to oxygen, air, and vacuum systems.
- Tools and expertise for emergency airway management.
- Emergency medications and appropriately scaled dosing tools for pediatric use.
- Immediate access to diagnostic tools, including ultrasound and, where indicated, X-ray facilities.
- Facilities for blood gas analysis and access to clinical laboratories, with a blood bank available depending on the surgical procedures performed.
3.1.2. Trained Personnel and Operational Standards
- Staff thoroughly trained in pediatric care, trained in recognizing the age-specific needs of children [8], and adhering to established standards while utilizing structured care protocols and checklists.
- A clear communication hierarchy with accessible contact information for all relevant personnel [9].
3.1.3. Comprehensive Patient Monitoring
- Pulse oximetry: Mandatory for all patients, with both pre- and post-ductal measurements recommended for infants younger than four weeks.
- Carbon dioxide monitoring: This should be performed via nasal cannula or transcutaneously when an impaired neurological status is present, in order to accurately detect hypoventilation or apnea before desaturation occurs [13].
- Electrocardiographic (ECG) monitoring: Performed based on clinical risk factors. For heart rates exceeding 200 beats per minute, a 12-lead ECG is essential to ensure accurate rhythm differentiation.
- Blood pressure: Measured on admission, before transfer, and at regular intervals based on the patient’s clinical status.
- Temperature: Monitored at a minimum upon admission and before transfer.

| Postoperative Risk for | Risk Factors |
|---|---|
| Hypoglycemia in need of therapy for blood glucose values <60 mg/dL (<70 mg/dL in type 1 diabetes) |
○ Age < 12 months/weight for age <5th percentile developmental delay/failure to thrive ○ ASA status ≥ III ○ Long fasting times ○ Abdominal surgery ○ Metabolic disease ○ Low glycogen reserve (parenteral nutrition, liver disease, beta blockers, diabetic mother) |
| Hyperglycemia/ketoacidosis in need of therapy for blood glucose values > 220–250 mg/dL | ○ Type I diabetes |
Primary Objectives of Pediatric Recovery Care
- Stabilizing vital parameters.
- Providing effective pain management.
- Timely detection and treatment of complications after anesthesia.
- Minimizing emotional distress.
- Reducing and treating nausea and vomiting.
- Achieving an adequate level of consciousness.
- Ensuring that the level of required monitoring and support is compatible with the capabilities of the ward where further care will be provided.
Additional Influencing Factors
3.2. Airway and Respiration
Postoperative Residual Neuromuscular Blockade
3.3. Hypothermia
3.4. Postoperative Nausea and/or Vomiting (PO(N)V)
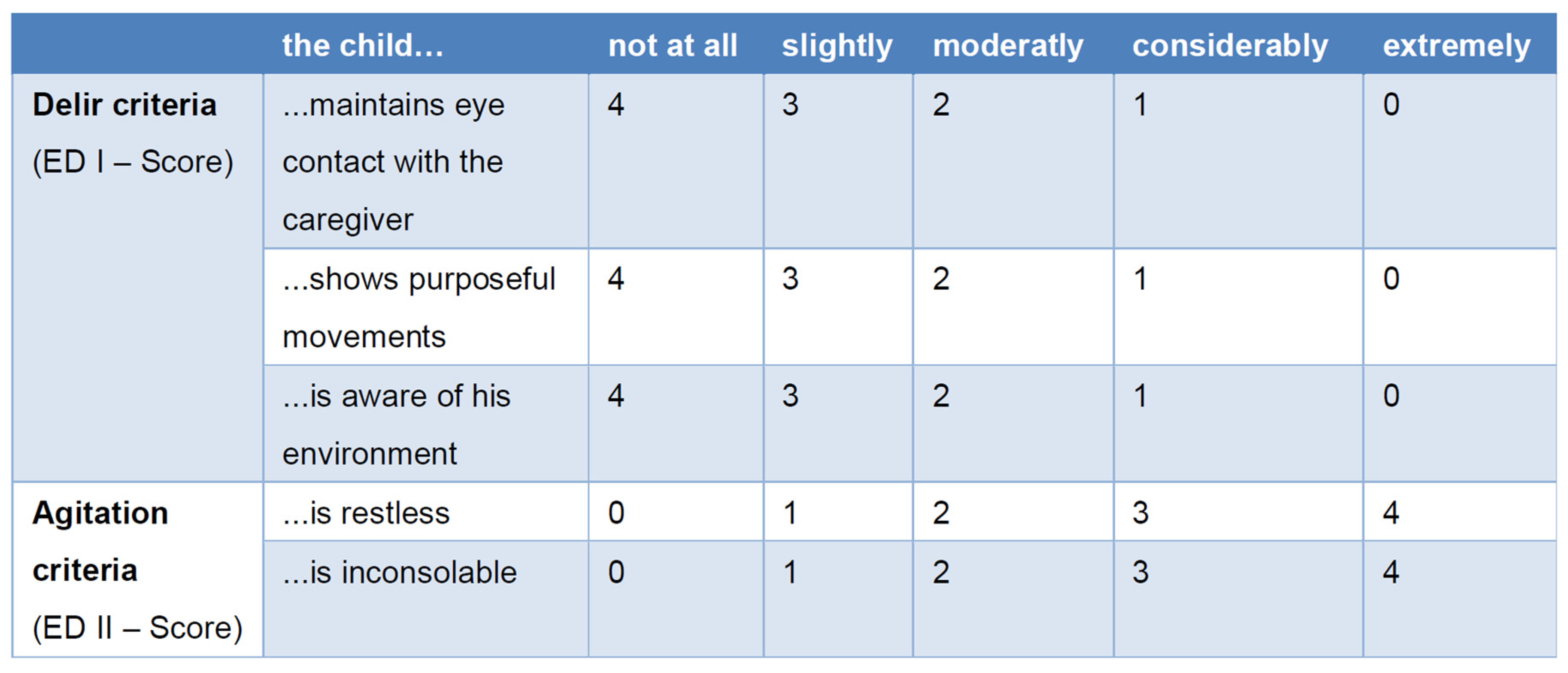
3.5. Emergence Delirium (ED)
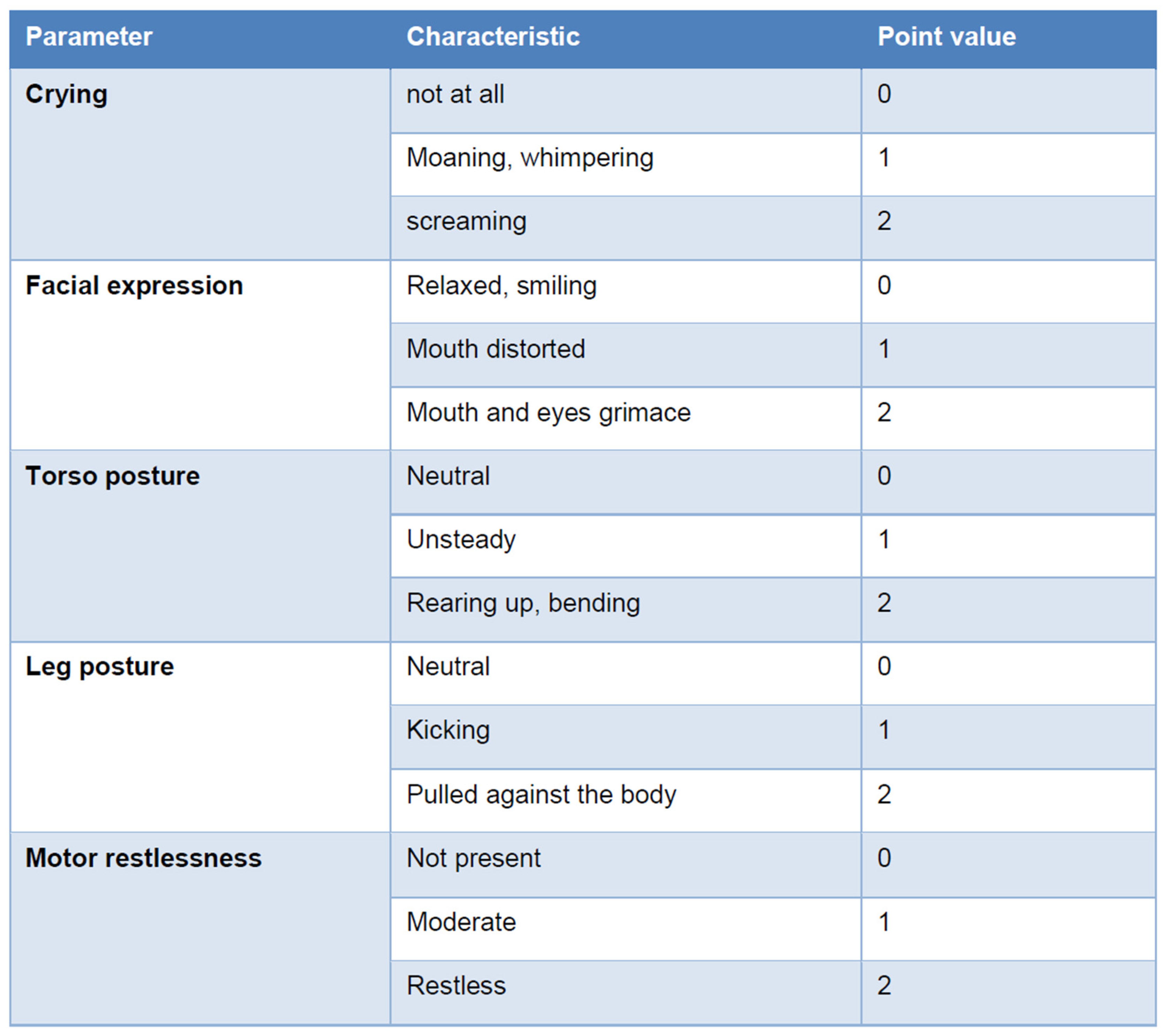
3.6. Pain Assessment and Pain Management
3.6.1. Prevention of Chronic Post-Surgical Pain (CPSP)
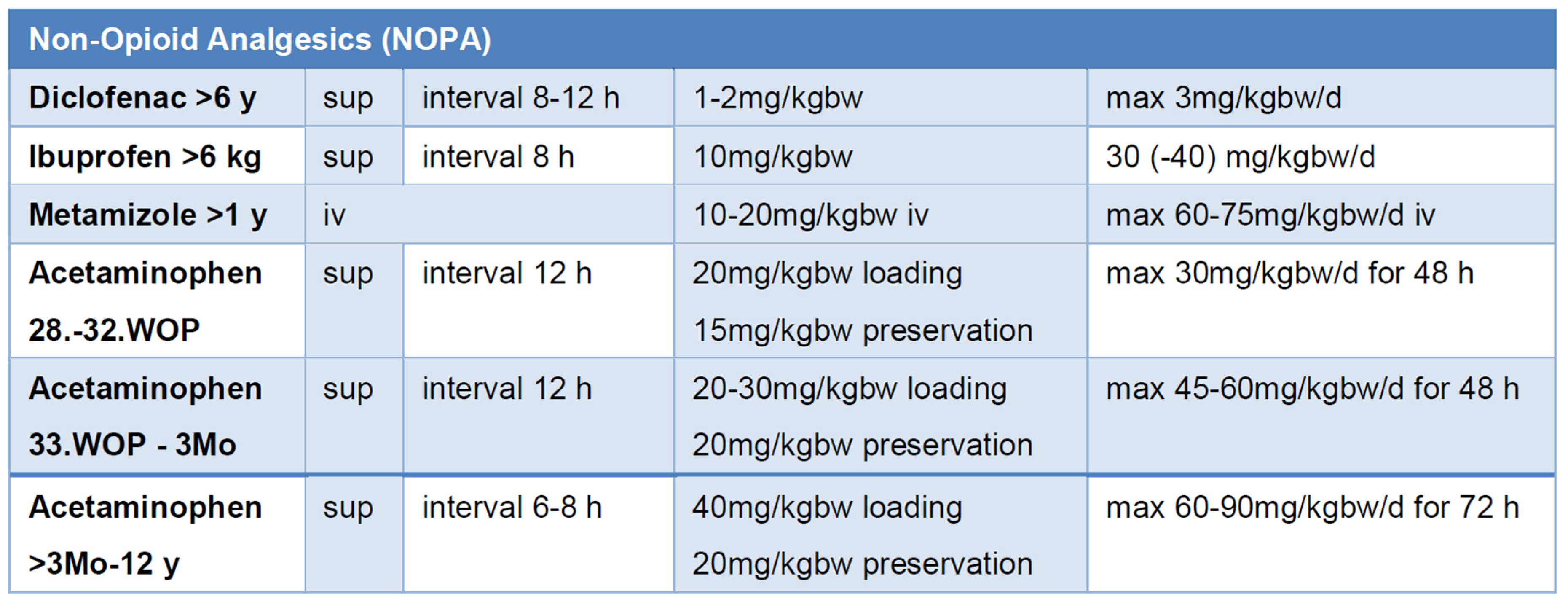
3.6.2. Non-Opioid Analgesics (NOPAs)
3.6.3. Opioids
3.6.4. Co-Analgesics
3.7. Early Postoperative Clear Fluid Intake
3.8. Discharge Criteria from Postoperative Recovery Room Care
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CHIPPS | Children’s and Infants’ Postoperative Pain Scale |
| CPSP | chronic post-surgical pain |
| ECG | electrocardiographic |
| ED | emergence delirium |
| EEG | electroencephalographic |
| LMA | laryngeal mask airway |
| NOPA | non-opioid analgesic |
| NSAID | nonsteroidal anti-inflammatory drugs |
| OSAS | obstructive sleep apnea syndrome |
| PO(N)V | postoperative nausea and/or vomiting |
| r-FLACC scale | revised Face, Legs, Activity, Cry, and Consolability scale |
References
- Murat, I.; Constant, I.; Maud’huy, H. Perioperative anaesthetic morbidity in children: A database of 24,165 anaesthetics over a 30-month period. Paediatr. Anaesth. 2004, 14, 158–166. [Google Scholar] [CrossRef] [PubMed]
- Khan, N.A.; Quan, H.; Bugar, J.M.; Lemaire, J.B.; Brant, R.; Ghali, W.A. Association of postoperative complications with hospital costs and length of stay in a tertiary care center. J. Gen. Intern. Med. 2006, 21, 177–180. [Google Scholar] [CrossRef]
- Story, D.A.; Leslie, K.; Myles, P.S.; Fink, M.; Poustie, S.J.; Forbes, A.; Yap, S.; Beavis, V.; Kerridge, R.; REASON Investigators, Australian and New Zealand College of Anaesthetists Trials Group. Complications and mortality in older surgical patients in Australia and New Zealand (the REASON study): A multicentre, prospective, observational study. Anaesthesia 2010, 65, 1022–1030. [Google Scholar] [CrossRef] [PubMed]
- Lloyd, C.; Proctor, L.; Au, M.; Story, D.; Edwards, S.; Ludbrook, G. Incidence of early major adverse events after surgery in moderate-risk patients: Early postoperative adverse events. Br. J. Anaesth. 2020, 124, e9–e10. [Google Scholar] [CrossRef] [PubMed]
- General Comment No. 15 (2013) on the Right of the Child to the Enjoyment of the Highest Attainable Standard of Health (Art. 24). Available online: https://digitallibrary.un.org/record/778524?ln=en&v=pdf (accessed on 21 March 2025).
- Available online: https://www.asahq.org/standards-and-practice-parameters/standards-for-postanesthesia-care (accessed on 21 January 2025).
- Sjoberg, C.; Ringdal, M.; Jildenstal, P. Postoperative Recovery in the Youngest: Beyond Technology. Children 2024, 11, 1021. [Google Scholar] [CrossRef]
- De Lourdes Levy, M.; Larcher, V.; Kurz, R.; Ethics Working Group of the Confederation of European Specialists in Paediatrics (CESP). Informed consent/assent in children. Statement of the Ethics Working Group of the Confederation of European Specialists in Paediatrics (CESP). Eur. J. Pediatr. 2003, 162, 629–633. [Google Scholar] [CrossRef]
- Olin, K.; Klinga, C.; Ekstedt, M.; Pukk-Harenstam, K. Exploring everyday work as a dynamic non-event and adaptations to manage safety in intraoperative anaesthesia care: An interview study. BMC Health Serv. Res. 2023, 23, 651. [Google Scholar] [CrossRef]
- Wensing, M. Implementation science in healthcare: Introduction and perspective. Z. Evid. Fortbild. Qual. Gesundhwes. 2015, 109, 97–102. [Google Scholar] [CrossRef]
- Proctor, E.K.; Powell, B.J.; McMillen, J.C. Implementation strategies: Recommendations for specifying and reporting. Implement. Sci. 2013, 8, 139. [Google Scholar] [CrossRef]
- Damschroder, L.J.; Aron, D.C.; Keith, R.E.; Kirsh, S.R.; Alexander, J.A.; Lowery, J.C. Fostering implementation of health services research findings into practice: A consolidated framework for advancing implementation science. Implement. Sci. 2009, 4, 50. [Google Scholar] [CrossRef]
- Klein, A.A.; Meek, T.; Allcock, E.; Cook, T.M.; Mincher, N.; Morris, C.; Nimmo, A.F.; Pandit, J.J.; Pawa, A.; Rodney, G.; et al. Recommendations for standards of monitoring during anaesthesia and recovery 2021: Guideline from the Association of Anaesthetists. Anaesthesia 2021, 76, 1212–1223. [Google Scholar] [CrossRef] [PubMed]
- Hoagland, M.; Duggar, B.; Hamrick, J.; Alonso, G.T.; Martin, L. Error traps in the perioperative management of children with type 1 diabetes. Paediatr. Anaesth. 2024, 34, 19–27. [Google Scholar] [CrossRef] [PubMed]
- Riegger, L.Q.; Leis, A.M.; Golmirzaie, K.H.; Malviya, S. Risk Factors for Intraoperative Hypoglycemia in Children: A Multicenter Retrospective Cohort Study. Anesth. Analg. 2021, 132, 1075–1083. [Google Scholar] [CrossRef] [PubMed]
- Sigurdsson, T.S.; Snaebjornsdottir, S.; Sigurdsson, M.I. Incidence of hypoglycaemia in fasting children after induction of anaesthesia for elective procedures: A descriptive observational study. Eur. J. Anaesthesiol. 2023, 40, 950–952. [Google Scholar] [CrossRef]
- Abraham, M.B.; Karges, B.; Dovc, K.; Naranjo, D.; Arbelaez, A.M.; Mbogo, J.; Javelikar, G.; Jones, T.W.; Mahmud, F.H. ISPAD Clinical Practice Consensus Guidelines 2022: Assessment and management of hypoglycemia in children and adolescents with diabetes. Pediatr. Diabetes 2022, 23, 1322–1340. [Google Scholar] [CrossRef]
- Sawada, A.; Kamada, Y.; Hayashi, H.; Ichinose, H.; Sumita, S.; Yamakage, M. Effect of Intraoperative Glucose Infusion on Catabolism of Adipose Tissue and Muscle Protein in Patients Anesthetized With Remifentanil in Combination With Sevoflurane During Major Surgery: A Randomized Controlled Multicenter Trial. Anesth. Analg. 2016, 123, 869–876. [Google Scholar] [CrossRef]
- Nishina, K.; Mikawa, K.; Maekawa, N.; Asano, M.; Obara, H. Effects of exogenous intravenous glucose on plasma glucose and lipid homeostasis in anesthetized infants. Anesthesiology 1995, 83, 258–263. [Google Scholar] [CrossRef]
- Sjoberg, C.; Ringdal, M.; Lundqvist, P.; Jildenstal, P. How to Achieve Highly Professional Care in the Postoperative Ward: The Care of Infants and Toddlers. J. PeriAnesthesia Nurs. 2024, 40, 95–99. [Google Scholar] [CrossRef]
- Baek, J.; Kim, Y.M. The Impact of Parental Presence on Emergence Delirium in Pediatric Patients After General Anesthesia: A Systematic Review and Meta-analysis. J. PeriAnesthesia Nurs. 2024, 39, 475–483. [Google Scholar] [CrossRef]
- Kain, Z.N.; Mayes, L.C.; Caldwell-Andrews, A.A.; Karas, D.E.; McClain, B.C. Preoperative anxiety, postoperative pain, and behavioral recovery in young children undergoing surgery. Pediatrics 2006, 118, 651–658. [Google Scholar] [CrossRef]
- Kain, Z.N.; Caldwell-Andrews, A.A.; Mayes, L.C.; Weinberg, M.E.; Wang, S.M.; MacLaren, J.E.; Blount, R.L. Family-centered preparation for surgery improves perioperative outcomes in children: A randomized controlled trial. Anesthesiology 2007, 106, 65–74. [Google Scholar] [CrossRef] [PubMed]
- Cote, C.J.; Zaslavsky, A.; Downes, J.J.; Kurth, C.D.; Welborn, L.G.; Warner, L.O.; Malviya, S.V. Postoperative apnea in former preterm infants after inguinal herniorrhaphy. A combined analysis. Anesthesiology 1995, 82, 809–822. [Google Scholar] [CrossRef] [PubMed]
- Welborn, L.G.; de Soto, H.; Hannallah, R.S.; Fink, R.; Ruttimann, U.E.; Boeckx, R. The use of caffeine in the control of post-anesthetic apnea in former premature infants. Anesthesiology 1988, 68, 796–798. [Google Scholar] [CrossRef]
- Schmidt, B.; Roberts, R.S.; Davis, P.; Doyle, L.W.; Barrington, K.J.; Ohlsson, A.; Solimano, A.; Tin, W.; Caffeine for Apnea of Prematurity Trial, G. Caffeine therapy for apnea of prematurity. N. Engl. J. Med. 2006, 354, 2112–2121. [Google Scholar] [CrossRef]
- Schmidt, B.; Roberts, R.S.; Davis, P.; Doyle, L.W.; Barrington, K.J.; Ohlsson, A.; Solimano, A.; Tin, W.; Caffeine for Apnea of Prematurity Trial, G. Long-term effects of caffeine therapy for apnea of prematurity. N. Engl. J. Med. 2007, 357, 1893–1902. [Google Scholar] [CrossRef]
- Patino, M.; Sadhasivam, S.; Mahmoud, M. Obstructive sleep apnoea in children: Perioperative considerations. Br. J. Anaesth. 2013, 111 (Suppl. S1), i83–i95. [Google Scholar] [CrossRef]
- Albornoz, A.E.; Rana, M.; Hayes, J.; Englesakis, M.; Tsang, M.; Amin, R.; Gilfoyle, E.; Petre, M.A.; Campisi, P.; Aoyama, K. Perioperative clinical practice recommendations for pediatric tonsillectomy: A systematic review. Can. J. Anaesth. 2024, 71, 187–200. [Google Scholar] [CrossRef] [PubMed]
- Webber, A.M.; Brennan, M. The high-risk pediatric patient for ambulatory surgery. Curr. Opin. Anaesthesiol. 2023, 36, 630–635. [Google Scholar] [CrossRef]
- Parry, M.; Glaisyer, H.R.; Bailey, P.M. Removal of LMA in children. Br. J. Anaesth. 1997, 78, 337–338. [Google Scholar] [CrossRef]
- Patterson, H.; Eady, J.; Sommerfield, A.; Sommerfield, D.; Hauser, N.; von Ungern-Sternberg, B.S. Patient positioning and its impact on perioperative outcomes in children: A narrative review. Paediatr. Anaesth. 2024, 34, 507–518. [Google Scholar] [CrossRef]
- Luedeke, C.M.; Rudolph, M.I.; Pulverenti, T.S.; Azimaraghi, O.; Grimm, A.M.; Jackson, W.M.; Jaconia, G.D.; Stucke, A.G.; Nafiu, O.O.; Karaye, I.M.; et al. Development and validation of a score for prediction of postoperative respiratory complications in infants and children (SPORC-C). Br. J. Anaesth. 2025, 134, 212–220. [Google Scholar] [CrossRef]
- Ledowski, T.; O’Dea, B.; Meyerkort, L.; Hegarty, M.; von Ungern-Sternberg, B.S. Postoperative Residual Neuromuscular Paralysis at an Australian Tertiary Children’s Hospital. Anesthesiol. Res. Pract. 2015, 2015, 410248. [Google Scholar] [CrossRef] [PubMed]
- von Ungern-Sternberg, B.S.; Hammer, J.; Schibler, A.; Frei, F.J.; Erb, T.O. Decrease of functional residual capacity and ventilation homogeneity after neuromuscular blockade in anesthetized young infants and preschool children. Anesthesiology 2006, 105, 670–675. [Google Scholar] [CrossRef] [PubMed]
- Lorinc, A.N.; Lawson, K.C.; Niconchuk, J.A.; Modes, K.B.; Moore, J.D.; Brenn, B.R. Residual Weakness and Recurarization After Sugammadex Administration in Pediatric Patients: A Case Series. A A Pract. 2020, 14, e01225. [Google Scholar] [CrossRef] [PubMed]
- Heier, T.; Caldwell, J.E. Impact of hypothermia on the response to neuromuscular blocking drugs. Anesthesiology 2006, 104, 1070–1080. [Google Scholar] [CrossRef]
- Bindu, B.; Bindra, A.; Rath, G. Temperature management under general anesthesia: Compulsion or option. J. Anaesthesiol. Clin. Pharmacol. 2017, 33, 306–316. [Google Scholar] [CrossRef]
- Bjertnaes, L.J.; Naesheim, T.O.; Reierth, E.; Suborov, E.V.; Kirov, M.Y.; Lebedinskii, K.M.; Tveita, T. Physiological Changes in Subjects Exposed to Accidental Hypothermia: An Update. Front. Med. 2022, 9, 824395. [Google Scholar] [CrossRef]
- Zanelli, S.; Buck, M.; Fairchild, K. Physiologic and pharmacologic considerations for hypothermia therapy in neonates. J. Perinatol. 2011, 31, 377–386. [Google Scholar] [CrossRef]
- Zhao, J.; Le, Z.; Chu, L.; Gao, Y.; Zhang, M.; Fan, J.; Ma, D.; Hu, Y.; Lai, D. Risk factors and outcomes of intraoperative hypothermia in neonatal and infant patients undergoing general anesthesia and surgery. Front. Pediatr. 2023, 11, 1113627. [Google Scholar] [CrossRef]
- Akin, A.; Esmaoglu, A.; Boyaci, A. Postoperative shivering in children and causative factors. Paediatr. Anaesth. 2005, 15, 1089–1093. [Google Scholar] [CrossRef]
- Nemeth, M.; Miller, C.; Brauer, A. Perioperative Hypothermia in Children. Int. J. Environ. Res. Public Health 2021, 18, 7541. [Google Scholar] [CrossRef] [PubMed]
- Laptook, A.R.; Salhab, W.; Bhaskar, B.; Neonatal Research, N. Admission temperature of low birth weight infants: Predictors and associated morbidities. Pediatrics 2007, 119, e643–e649. [Google Scholar] [CrossRef]
- Eberhart, L.H.; Morin, A.M.; Guber, D.; Kretz, F.J.; Schauffelen, A.; Treiber, H.; Wulf, H.; Geldner, G. Applicability of risk scores for postoperative nausea and vomiting in adults to paediatric patients. Br. J. Anaesth. 2004, 93, 386–392. [Google Scholar] [CrossRef]
- Edler, A.A.; Mariano, E.R.; Golianu, B.; Kuan, C.; Pentcheva, K. An analysis of factors influencing postanesthesia recovery after pediatric ambulatory tonsillectomy and adenoidectomy. Anesth. Analg. 2007, 104, 784–789. [Google Scholar] [CrossRef] [PubMed]
- Gan, T.J.; Belani, K.G.; Bergese, S.; Chung, F.; Diemunsch, P.; Habib, A.S.; Jin, Z.; Kovac, A.L.; Meyer, T.A.; Urman, R.D.; et al. Fourth Consensus Guidelines for the Management of Postoperative Nausea and Vomiting. Anesth. Analg. 2020, 131, 411–448. [Google Scholar] [CrossRef] [PubMed]
- Roher, K.; Fideler, F. Perioperative Complications in Pediatric Anesthesia. Anasthesiol. Intensiv. Notfallmed Schmerzther. 2022, 57, 563–576. [Google Scholar] [CrossRef]
- Cox, R.G. Alternative therapies and postoperative vomiting. Paediatr. Anaesth. 2016, 26, 782–783. [Google Scholar] [CrossRef]
- Abraham, J. Acupressure and acupuncture in preventing and managing postoperative nausea and vomiting in adults. J. Perioper. Pract. 2008, 18, 543–551. [Google Scholar] [CrossRef]
- Chauvin, C.; Schalber-Geyer, A.S.; Lefebvre, F.; Bopp, C.; Carrenard, G.; Marcoux, L.; Mayer, J.F.; Schwaab, C.; Joshi, G.P.; Diemunsch, P. Early postoperative oral fluid intake in paediatric day case surgery influences the need for opioids and postoperative vomiting: A controlled randomized trialdagger. Br. J. Anaesth. 2017, 118, 407–414. [Google Scholar] [CrossRef]
- Johns, D.E.; Gerling, V.; Pasker-de Jong, P.C. Ice pops in the recovery room: Effects on postoperative nausea and vomiting. Br. J. Anaesth. 2017, 118, 637–638. [Google Scholar] [CrossRef]
- Aldecoa, C.; Bettelli, G.; Bilotta, F.; Sanders, R.D.; Audisio, R.; Borozdina, A.; Cherubini, A.; Jones, C.; Kehlet, H.; MacLullich, A.; et al. European Society of Anaesthesiology evidence-based and consensus-based guideline on postoperative delirium. Eur. J. Anaesthesiol. 2017, 34, 192–214. [Google Scholar] [CrossRef]
- Voepel-Lewis, T.; Malviya, S.; Tait, A.R. A prospective cohort study of emergence agitation in the pediatric postanesthesia care unit. Anesth. Analg. 2003, 96, 1625–1630. [Google Scholar] [CrossRef]
- Vlajkovic, G.P.; Sindjelic, R.P. Emergence delirium in children: Many questions, few answers. Anesth. Analg. 2007, 104, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Ringblom, J.; Wahlin, I.; Proczkowska, M. A psychometric evaluation of the Pediatric Anesthesia Emergence Delirium scale. Paediatr. Anaesth. 2018, 28, 332–337. [Google Scholar] [CrossRef] [PubMed]
- Sikich, N.; Lerman, J. Development and psychometric evaluation of the pediatric anesthesia emergence delirium scale. Anesthesiology 2004, 100, 1138–1145. [Google Scholar] [CrossRef]
- Somaini, M.; Engelhardt, T.; Fumagalli, R.; Ingelmo, P.M. Emergence delirium or pain after anaesthesia—How to distinguish between the two in young children: A retrospective analysis of observational studies. Br. J. Anaesth. 2016, 116, 377–383. [Google Scholar] [CrossRef] [PubMed]
- Russell, P.S.S.; Mammen, P.M.; Shankar, S.R.; Viswanathan, S.A.; Rebekah, G.; Russell, S.; Earnest, R.; Chikkala, S.M. Pediatric Anesthesia Emergence Delirium Scale: A diagnostic meta-analysis. World J. Clin. Pediatr. 2022, 11, 196–205. [Google Scholar] [CrossRef]
- Locatelli, B.G.; Ingelmo, P.M.; Emre, S.; Meroni, V.; Minardi, C.; Frawley, G.; Benigni, A.; Di Marco, S.; Spotti, A.; Busi, I.; et al. Emergence delirium in children: A comparison of sevoflurane and desflurane anesthesia using the Paediatric Anesthesia Emergence Delirium scale. Paediatr. Anaesth. 2013, 23, 301–308. [Google Scholar] [CrossRef]
- Ringblom, J.; Wahlin, I.; Proczkowska, M.; Korhonen, L.; Arestedt, K. Measurement Properties of the Pediatric Anesthesia Emergence Delirium Scale: A Confirmatory Factor Analysis-Based Study. Paediatr. Anaesth. 2025, 35, 155–162. [Google Scholar] [CrossRef]
- Aono, J.; Mamiya, K.; Manabe, M. Preoperative anxiety is associated with a high incidence of problematic behavior on emergence after halothane anesthesia in boys. Acta Anaesthesiol. Scand. 1999, 43, 542–544. [Google Scholar] [CrossRef]
- Mason, K.P. Paediatric emergence delirium: A comprehensive review and interpretation of the literature. Br. J. Anaesth. 2017, 118, 335–343. [Google Scholar] [CrossRef] [PubMed]
- Muzzi, E.; Ronfani, L.; Bossini, B.; Lezcano, C.; Orzan, E.; Barbi, E. Effects of Intraoperative Auditory Stimulation on Pain and Agitation on Awakening After Pediatric Adenotonsillectomy: A Randomized Clinical Trial. JAMA Otolaryngol.-Head Neck Surg. 2021, 147, 638–645. [Google Scholar] [CrossRef]
- Xiao, Y.; Jin, X.; Zhang, Y.; Huang, T.; Zhou, L.; Gao, J. Efficacy of propofol for the prevention of emergence agitation after sevoflurane anaesthesia in children: A meta-analysis. Front. Surg. 2022, 9, 1031010. [Google Scholar] [CrossRef]
- Ng, K.T.; Sarode, D.; Lai, Y.S.; Teoh, W.Y.; Wang, C.Y. The effect of ketamine on emergence agitation in children: A systematic review and meta-analysis. Paediatr. Anaesth. 2019, 29, 1163–1172. [Google Scholar] [CrossRef]
- Zhao, N.; Zeng, J.; Fan, L.; Zhang, C.; Wu, Y.; Wang, X.; Gao, F.; Yu, C. The Effect of Alfentanil on Emergence Delirium Following General Anesthesia in Children: A Randomized Clinical Trial. Paediatr. Drugs 2022, 24, 413–421. [Google Scholar] [CrossRef] [PubMed]
- Kim, N.; Park, J.H.; Lee, J.S.; Choi, T.; Kim, M.S. Effects of intravenous fentanyl around the end of surgery on emergence agitation in children: Systematic review and meta-analysis. Paediatr. Anaesth. 2017, 27, 885–892. [Google Scholar] [CrossRef] [PubMed]
- Davies, L.; Qi, T.S.; Ng, A. Emergence delirium: An overview with an emphasis on the use of electroencephalography in its management. Anesth. Pain. Med. 2024, 19, S87–S95. [Google Scholar] [CrossRef]
- Petre, M.A.; Levin, D.N.; Englesakis, M.; Maynes, J.T.; Pechlivanoglou, P.; Aoyama, K. Dexmedetomidine vs. total intravenous anaesthesia in paediatric emergence delirium: A network meta-analysis. Eur. J. Anaesthesiol. 2021, 38, 1111–1123. [Google Scholar] [CrossRef]
- Koo, C.H.; Koo, B.W.; Han, J.; Lee, H.T.; Lim, D.; Shin, H.J. The effects of intraoperative magnesium sulfate administration on emergence agitation and delirium in pediatric patients: A systematic review and meta-analysis of randomized controlled trials. Paediatr. Anaesth. 2022, 32, 522–530. [Google Scholar] [CrossRef]
- Bernhart, K.; Becke-Jakob, K.; Lehmann, T.; Harnik, M.; Seiler, S.; Meissner, W.; Stuber, F.; Stamer, U.M. Analgesic use and favourable patient-reported outcome measures after paediatric surgery: An analysis of registry data. Br. J. Anaesth. 2023, 130, 74–82. [Google Scholar] [CrossRef]
- Buttner, W.; Finke, W.; Hilleke, M.; Reckert, S.; Vsianska, L.; Brambrink, A. Development of an observational scale for assessment of postoperative pain in infants. Anasthesiol Intensiv. Notfallmed Schmerzther 1998, 33, 353–361. [Google Scholar] [CrossRef]
- Malviya, S.; Voepel-Lewis, T.; Burke, C.; Merkel, S.; Tait, A.R. The revised FLACC observational pain tool: Improved reliability and validity for pain assessment in children with cognitive impairment. Paediatr. Anaesth. 2006, 16, 258–265. [Google Scholar] [CrossRef] [PubMed]
- Crellin, D.J.; Harrison, D.; Santamaria, N.; Babl, F.E. Systematic review of the Face, Legs, Activity, Cry and Consolability scale for assessing pain in infants and children: Is it reliable, valid, and feasible for use? Pain 2015, 156, 2132–2151. [Google Scholar] [CrossRef]
- Zielinski, J.; Morawska-Kochman, M.; Zatonski, T. Pain assessment and management in children in the postoperative period: A review of the most commonly used postoperative pain assessment tools, new diagnostic methods and the latest guidelines for postoperative pain therapy in children. Adv. Clin. Exp. Med. 2020, 29, 365–374. [Google Scholar] [CrossRef]
- Furuta, M.; Suzuki, Y.; Sun, N.; Aoyama, K. Chronic post-surgical pain in pediatric population. J. Anesth. 2022, 36, 785–786. [Google Scholar] [CrossRef] [PubMed]
- Rabbitts, J.A.; Fisher, E.; Rosenbloom, B.N.; Palermo, T.M. Prevalence and Predictors of Chronic Postsurgical Pain in Children: A Systematic Review and Meta-Analysis. J. Pain 2017, 18, 605–614. [Google Scholar] [CrossRef] [PubMed]
- Rosenbloom, B.N.; Frederiksen, S.D.; Wang, V.; Park, C.S.; Gordon, G.; Brar, G.; Rasic, N.; Stinson, J.N.; Birnie, K.A.; Rabbitts, J.A. Prognostic factors of chronic postsurgical pain in children and adolescents: A systematic review and meta-analysis. Reg. Anesth. Pain Med. 2025, 50, 144–152. [Google Scholar] [CrossRef]
- Ziesenitz, V.C.; Welzel, T.; van Dyk, M.; Saur, P.; Gorenflo, M.; van den Anker, J.N. Efficacy and Safety of NSAIDs in Infants: A Comprehensive Review of the Literature of the Past 20 Years. Paediatr. Drugs 2022, 24, 603–655. [Google Scholar] [CrossRef]
- Wong, I.; St John-Green, C.; Walker, S.M. Opioid-sparing effects of perioperative paracetamol and nonsteroidal anti-inflammatory drugs (NSAIDs) in children. Paediatr. Anaesth. 2013, 23, 475–495. [Google Scholar] [CrossRef]
- Messerer, B.; Grogl, G.; Stromer, W.; Jaksch, W. Pediatric perioperative systemic pain therapy: Austrian interdisciplinary recommendations on pediatric perioperative pain management. Schmerz 2014, 28, 43–64. [Google Scholar] [CrossRef]
- Birmingham, P.K.; Tobin, M.J.; Fisher, D.M.; Henthorn, T.K.; Hall, S.C.; Cote, C.J. Initial and subsequent dosing of rectal acetaminophen in children: A 24-h pharmacokinetic study of new dose recommendations. Anesthesiology 2001, 94, 385–389. [Google Scholar] [CrossRef] [PubMed]
- Lewis, S.R.; Nicholson, A.; Cardwell, M.E.; Siviter, G.; Smith, A.F. Nonsteroidal anti-inflammatory drugs and perioperative bleeding in paediatric tonsillectomy. Cochrane Database Syst. Rev. 2013, 2013, CD003591. [Google Scholar] [CrossRef] [PubMed]
- Ringsten, M.; Kredo, T.; Ebrahim, S.; Hohlfeld, A.; Bruschettini, M. Diclofenac for acute postoperative pain in children. Cochrane Database Syst. Rev. 2023, 12, CD015087. [Google Scholar] [CrossRef]
- Yoon, E.; Babar, A.; Choudhary, M.; Kutner, M.; Pyrsopoulos, N. Acetaminophen-Induced Hepatotoxicity: A Comprehensive Update. J. Clin. Transl. Hepatol. 2016, 4, 131–142. [Google Scholar] [CrossRef] [PubMed]
- Thibault, C.; Pelletier, E.; Nguyen, C.; Trottier, E.D.; Dore-Bergeron, M.J.; DeKoven, K.; Roy, A.M.; Piche, N.; Delisle, J.F.; Morin, C.; et al. The Three W’s of Acetaminophen In Children: Who, Why, and Which Administration Mode. J. Pediatr. Pharmacol. Ther. 2023, 28, 20–28. [Google Scholar] [CrossRef]
- Stamer, U.M.; Stammschulte, T.; Erlenwein, J.; Koppert, W.; Freys, S.; Meissner, W.; Ahrens, P.; Brede, E.M.; Lindig, M.; Dusch, M.; et al. Recommendations for the perioperative use of dipyrone: Expert recommendation of the working group on acute pain of the German Pain Society, the scientific working group on pain medicine of the German Society for Anesthesiology and Intensive Care Medicine and the surgical working group on acute pain of the German Society for Surgery with participation of representatives of the Drug Commission of the German Medical Association. Schmerz 2019, 33, 287–294. [Google Scholar] [CrossRef]
- Zahn, J.; Eberl, S.; Rodle, W.; Rascher, W.; Neubert, A.; Toni, I. Metamizole Use in Children: Analysis of Drug Utilisation and Adverse Drug Reactions at a German University Hospital between 2015 and 2020. Paediatr. Drugs 2022, 24, 45–56. [Google Scholar] [CrossRef]
- Sharp, D.; Jaffrani, A. A PRISMA Systematic Review on the Safety and Efficacy of Patient-Controlled Analgesia (PCA) in Pediatrics. J. Pediatr. Nurs. 2021, 61, 219–223. [Google Scholar] [CrossRef]
- Walker, S.M. Neonatal pain. Paediatr. Anaesth. 2014, 24, 39–48. [Google Scholar] [CrossRef]
- Schultz-Machata, A.M.; Becke, K.; Weiss, M. Nalbuphine in pediatric anesthesia. Anaesthesist 2014, 63, 135–143. [Google Scholar] [CrossRef]
- Aldamluji, N.; Burgess, A.; Pogatzki-Zahn, E.; Raeder, J.; Beloeil, H.; PROSPECT Working Group Collaborators. PROSPECT guideline for tonsillectomy: Systematic review and procedure-specific postoperative pain management recommendations. Anaesthesia 2021, 76, 947–961. [Google Scholar] [CrossRef] [PubMed]
- Jun, J.H.; Kim, K.N.; Kim, J.Y.; Song, S.M. The effects of intranasal dexmedetomidine premedication in children: A systematic review and meta-analysis. Can. J. Anaesth. 2017, 64, 947–961. [Google Scholar] [CrossRef] [PubMed]
- Burjek, N.E.; Hafeman, M.; Guthrie, D.; Desai, A.; Jin, Z.; Brockel, M.; Moore, R. Perioperative use of gabapentinoids in pediatric patients. Anesthesiol. Perioper. Sci. 2023, 1, 21. [Google Scholar] [CrossRef]
- Pillai Riddell, R.R.; Bucsea, O.; Shiff, I.; Chow, C.; Gennis, H.G.; Badovinac, S.; DiLorenzo-Klas, M.; Racine, N.M.; Ahola Kohut, S.; Lisi, D.; et al. Non-pharmacological management of infant and young child procedural pain. Cochrane Database Syst. Rev. 2023, 6, CD006275. [Google Scholar] [CrossRef]
- Vittinghoff, M.; Lonnqvist, P.A.; Mossetti, V.; Heschl, S.; Simic, D.; Colovic, V.; Dmytriiev, D.; Holzle, M.; Zielinska, M.; Kubica-Cielinska, A.; et al. Postoperative pain management in children: Guidance from the pain committee of the European Society for Paediatric Anaesthesiology (ESPA Pain Management Ladder Initiative). Paediatr. Anaesth. 2018, 28, 493–506. [Google Scholar] [CrossRef]
- Vittinghoff, M.; Lonnqvist, P.A.; Mossetti, V.; Heschl, S.; Simic, D.; Colovic, V.; Hozle, M.; Zielinska, M.; Maria, B.J.; Oppitz, F.; et al. Postoperative Pain Management in children: Guidance from the Pain Committee of the European Society for Paediatric Anaesthesiology (ESPA Pain Management Ladder Initiative) Part II. Anaesth. Crit. Care Pain Med. 2024, 43, 101427. [Google Scholar] [CrossRef]
- Fung, A.C.; Tsang, J.T.; Chung, P.H.; Kak-Yuen Wong, K. Does Chewing Gum Lead to Earlier Postoperative Gastrointestinal Recovery in Children? A Systematic Review and Meta-analysis. J. Pediatr. Surg. 2024, 59, 268–274. [Google Scholar] [CrossRef]
- Rafeeqi, T.; Pearson, E.G. Enhanced recovery after surgery in children. Transl. Gastroenterol. Hepatol. 2021, 6, 46. [Google Scholar] [CrossRef]
- Aldrete, J.A. The post-anesthesia recovery score revisited. J. Clin. Anesth. 1995, 7, 89–91. [Google Scholar] [CrossRef]
- Stein, A.L.; Baumgard, D.; Del Rio, I.; Tutiven, J.L. Updates in Pediatric Regional Anesthesia and Its Role in the Treatment of Acute Pain in the Ambulatory Setting. Curr. Pain. Headache Rep. 2017, 21, 11. [Google Scholar] [CrossRef]
- Finneran, J.J.t.; Ilfeld, B.M. Continuous peripheral nerve blocks for analgesia following painful ambulatory surgery: A review with focus on recent developments in infusion technology. Curr. Opin. Anaesthesiol. 2023, 36, 525–532. [Google Scholar] [CrossRef] [PubMed]
- Gurnaney, H.; Kraemer, F.W.; Maxwell, L.; Muhly, W.T.; Schleelein, L.; Ganesh, A. Ambulatory continuous peripheral nerve blocks in children and adolescents: A longitudinal 8-year single center study. Anesth. Analg. 2014, 118, 621–627. [Google Scholar] [CrossRef] [PubMed]
- Uffman, J.C.; Kim, S.S.; Quan, L.N.; Shelton, T.; Beltran, R.J.; Jatana, K.R.; Chiang, T.; Tobias, J.D. Adverse Events in Infants Less Than 6 Months of Age After Ambulatory Surgery and Diagnostic Imaging Requiring Anesthesia. Pediatr. Qual. Saf. 2022, 7, e574. [Google Scholar] [CrossRef] [PubMed]
- Kurth, C.D.; Tyler, D.; Heitmiller, E.; Tosone, S.R.; Martin, L.; Deshpande, J.K. National pediatric anesthesia safety quality improvement program in the United States. Anesth. Analg. 2014, 119, 112–121. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Korell, L.; Fideler, F. Improving Postoperative Pediatric Recovery by Efficient Recovery Room Care—A Comprehensive Review. Children 2025, 12, 568. https://doi.org/10.3390/children12050568
Korell L, Fideler F. Improving Postoperative Pediatric Recovery by Efficient Recovery Room Care—A Comprehensive Review. Children. 2025; 12(5):568. https://doi.org/10.3390/children12050568
Chicago/Turabian StyleKorell, Lisa, and Frank Fideler. 2025. "Improving Postoperative Pediatric Recovery by Efficient Recovery Room Care—A Comprehensive Review" Children 12, no. 5: 568. https://doi.org/10.3390/children12050568
APA StyleKorell, L., & Fideler, F. (2025). Improving Postoperative Pediatric Recovery by Efficient Recovery Room Care—A Comprehensive Review. Children, 12(5), 568. https://doi.org/10.3390/children12050568