
Practice of Routine Monitoring of Gastric Residual in Preterm Infants: A Meta-Analysis Article

Abstract
1. Introduction
2. Materials and Methods
2.1. Protocol
2.2. Search Strategy
2.3. Study Selection
2.4. Population
2.5. Intervention
2.6. Comparator
2.7. Outcome
2.8. Inclusion and Exclusion Criteria
2.9. Data Collection and Analysis
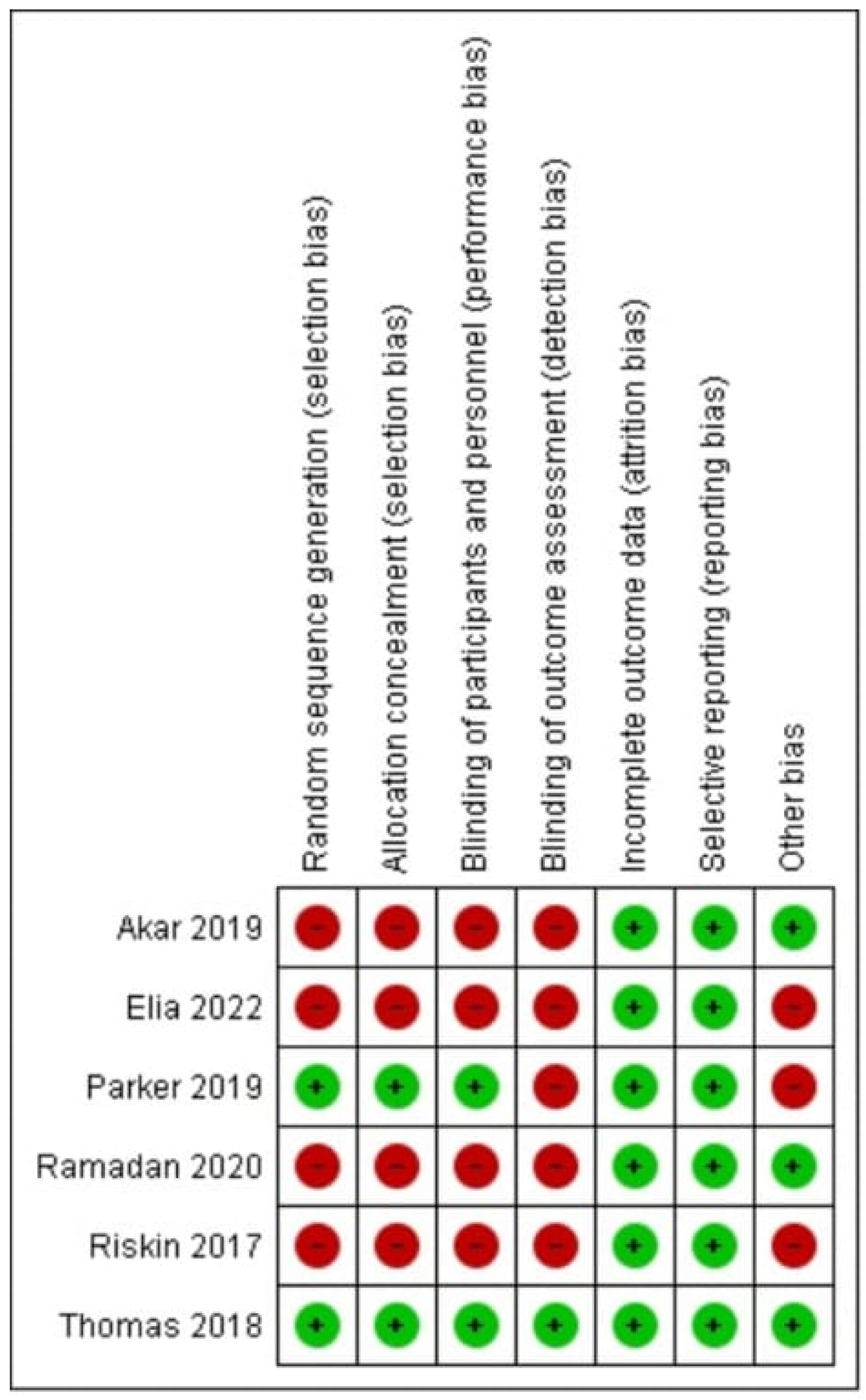
2.10. Assessment of Risk of Bias in Included Studies
2.11. Data Analysis
2.12. Statistical Analysis
2.13. Measures of Treatment
2.14. Assessment of Heterogeneity
2.15. Subgroup Analysis
3. Results
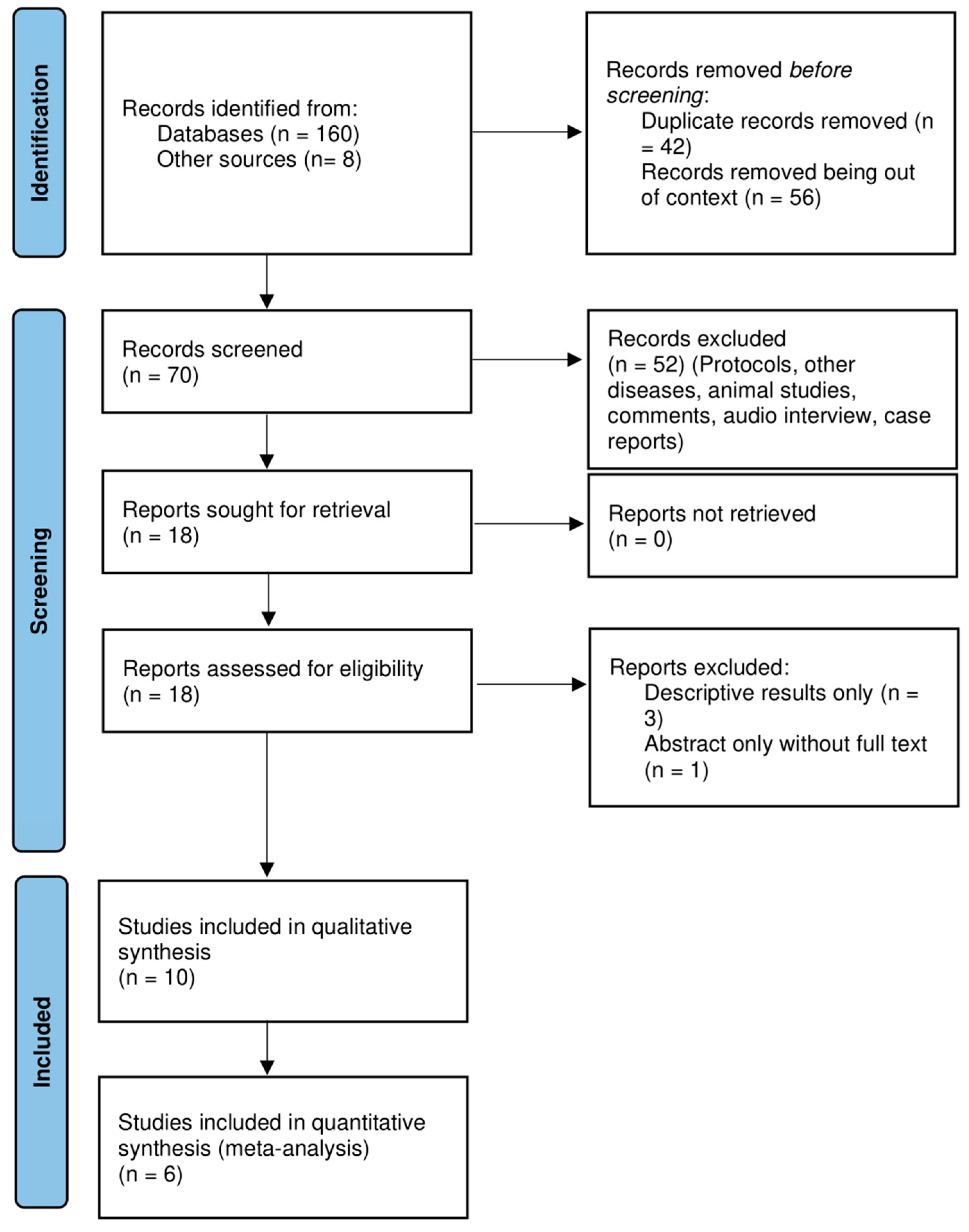
3.1. Study Search
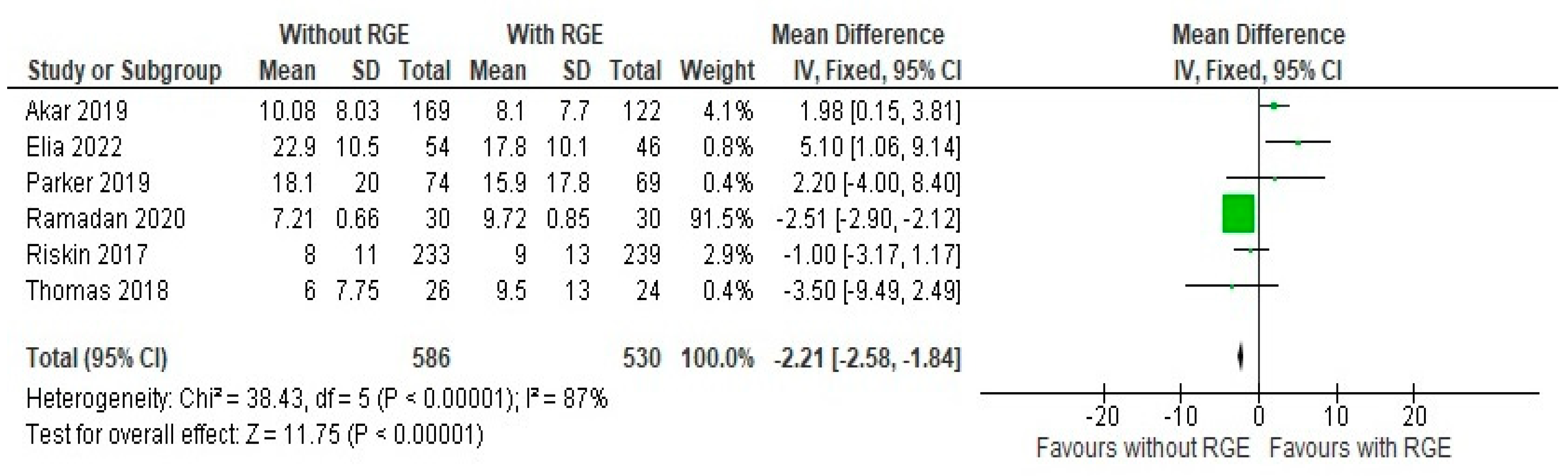
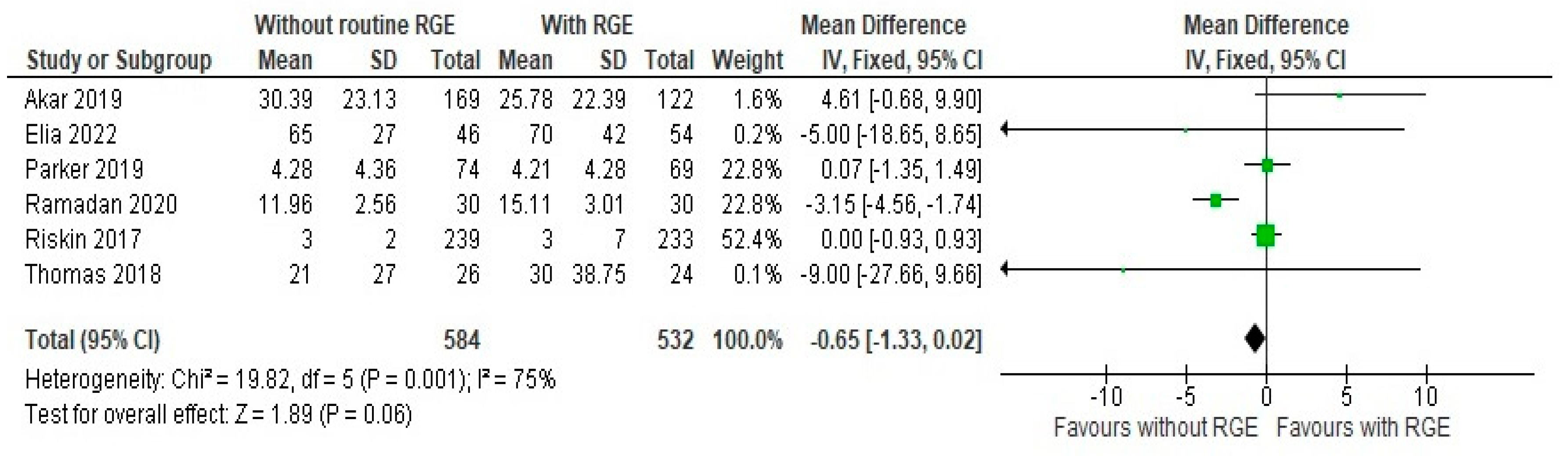
3.2. Primary Outcomes
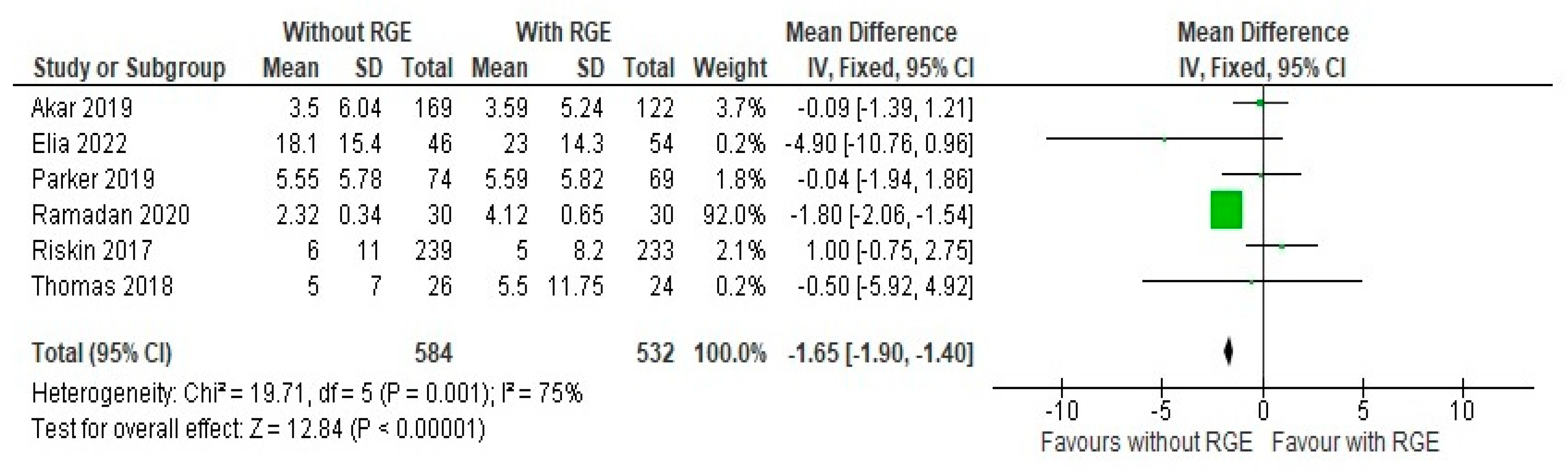
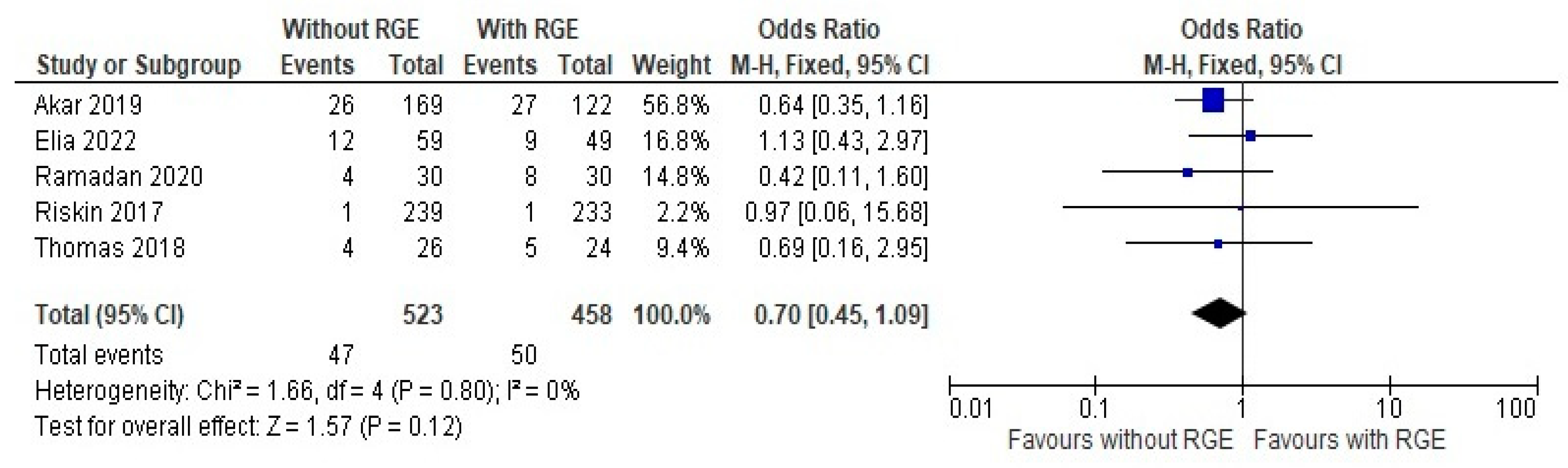
3.3. Secondary Outcomes
3.4. Other Outcomes
3.5. Subgroup Analysis
3.6. Sensitivity Analysis
4. Discussion
5. Limitations
6. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kumar, J.; Meena, J.; Mittal, P.; Shankar, J.; Kumar, P.; Shenoi, A. Routine prefeed gastric aspiration in preterm infants: A systematic review and meta-analysis. Eur. J. Pediatr. 2021, 180, 2367–2377. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.Y.; Xue, H.P.; Yuan, M.J.; Jin, Y.R.; Huang, C.X. Effects of ultrasound monitoring of gastric residual volume on feeding complications, caloric intake and prognosis of patients with severe mechanical ventilation. World J. Gastrointest. Surg. 2023, 15, 1719. [Google Scholar] [CrossRef] [PubMed]
- Yasuda, H.; Kondo, N.; Yamamoto, R.; Asami, S.; Abe, T.; Tsujimoto, H.; Kataoka, Y. Monitoring of gastric residual volume during enteral nutrition. Cochrane Database Syst. Rev. 2021, 9, CD013335. [Google Scholar] [CrossRef] [PubMed]
- Athalye-Jape, G.; Nettleton, M.; Lai, C.-T.; Nathan, E.; Geddes, D.; Simmer, K.; Patole, S. Composition of coloured gastric residuals in extremely preterm infants-a nested prospective observational study. Nutrients 2020, 12, 2585. [Google Scholar] [CrossRef]
- Gale, C.; Roberts, C.; Hardy, P.; CTU, N. The neoGASTRIC Trial: Avoiding Routine Gastric Residual Volume Measurement in Neonatal Critical Care: A Multi-Centre Randomised Controlled Trial Protocol. Available online: https://www.isrctn.com/ISRCTN16710849 (accessed on 1 March 2025).
- Makker, K.; Ji, Y.; Hong, X.; Wang, X. Antenatal and neonatal factors contributing to extra uterine growth failure (EUGR) among preterm infants in Boston Birth Cohort (BBC). J. Perinatol. 2021, 41, 1025–1032. [Google Scholar] [CrossRef]
- Hwang, H.S.; Chung, M.L. Risk Factors Contributing to Extrauterine Growth Restriction in Very Low Birth Weight Infants. Neonatal Med. 2024, 31, 31–37. [Google Scholar] [CrossRef]
- Moschino, L.; Duci, M.; Leon, F.F.; Bonadies, L.; Priante, E.; Baraldi, E.; Verlato, G. Optimizing nutritional strategies to prevent necrotizing enterocolitis and growth failure after bowel resection. Nutrients 2021, 13, 340. [Google Scholar] [CrossRef]
- Banait, N.; Basu, S.; Desai, P.; Dutta, S.; Kumar, A.; Kumar, J.; Shenoi, A.; Suryawanshi, P. Feeding of low birth weight neonates. J. Neonatol. 2020, 34, 28–51. [Google Scholar] [CrossRef]
- Abdul Hamid, H. Feeding Practices, Nutrition and Gastro-Oesophageal Reflux Disease (GORD) Among Newborn Infants in Neonatal Units. Doctor Thesis, University of Nottingham, Nottingham, UK, 2022. [Google Scholar]
- Tian, L.; Li, W.; Su, Y.; Gao, H.; Yang, Q.; Lin, P.; Wang, L.; Zeng, J.; Li, Y. Risk factors for central venous access device-related thrombosis in hospitalized children: A systematic review and meta-analysis. Thromb. Haemost. 2020, 121, 625–640. [Google Scholar] [CrossRef]
- Hamza, W.S.; Hamed, E.A.-T.M.; Alfadhli, M.A.; Ramadan, M.A.-M. A multidisciplinary intervention to reduce central line-associated bloodstream infection in pediatrics and neonatal intensive care units. Pediatr. Neonatol. 2022, 63, 71–77. [Google Scholar] [CrossRef]
- Mangalapally, N.; Patel, S.; Schofield, E.M.; Capriolo, C.D.; Davis, N.L.M. Impact of Routine Gastric Aspirate Monitoring on Very Low Birth Weight Early Preterm Infants. J. Pediatr. Gastroenterol. Nutr. 2023, 76, 517–522. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Moher, D. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Willhelm, C.; Girisch, W.; Gottschling, S.; Gräber, S.; Wahl, H.; Meyer, S. Systematic Cochrane Reviews in Neonatology: A Critical Appraisal. Pediatr. Neonatol. 2013, 54, 261–266. [Google Scholar] [CrossRef]
- Minozzi, S.; Dwan, K.; Borrelli, F.; Filippini, G. Reliability of the revised Cochrane risk-of-bias tool for randomised trials (RoB2) improved with the use of implementation instruction. J. Clin. Epidemiol. 2022, 141, 99–105. [Google Scholar] [CrossRef]
- Puhan, M.A.; Schünemann, H.J.; Murad, M.H.; Li, T.; Brignardello-Petersen, R.; Singh, J.A.; Kessels, A.G.; Guyatt, G.H. A GRADE Working Group approach for rating the quality of treatment effect estimates from network meta-analysis. BMJ 2014, 349, g5630. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; Sterne, J.A.C.; Higgins, J.P.T.; Egger, M. Investigating and dealing with publication bias and other reporting biases in meta-analyses of health research: A review. Res. Synth. Methods 2021, 12, 248–259. [Google Scholar] [CrossRef]
- Akar, S.; Turgut, M. Do we control gastric residuals unnecessarily in premature newborns? AGRA study: Avoidance of gastric residual aspiration. World J. Pediatr. Surg. 2020, 3, e000056. [Google Scholar] [CrossRef]
- Elia, S.; Ciarcià, M.; Miselli, F.; Bertini, G.; Dani, C. Effect of selective gastric residual monitoring on enteral intake in preterm infants. Ital. J. Pediatr. 2022, 48, 30. [Google Scholar] [CrossRef]
- Parker, L.A.; Weaver, M.; Torrazza, R.J.M.; Shuster, J.; Li, N.; Krueger, C.; Neu, J. Effect of gastric residual evaluation on enteral intake in extremely preterm infants: A randomized clinical trial. JAMA Pediatr. 2019, 173, 534–543. [Google Scholar] [CrossRef]
- Ramadan, O.; Rashad, H.; Darwish, M.; Dabash, S. Effect of non-aspirated gastric residual content on preterm infants’ health status. Int. J. Health Sci. 2022, 6, 6875–6887. [Google Scholar] [CrossRef]
- Riskin, A.; Cohen, K.; Kugelman, A.; Toropine, A.; Said, W.; Bader, D. The impact of routine evaluation of gastric residual volumes on the time to achieve full enteral feeding in preterm infants. J. Pediatr. 2017, 189, 128–134. [Google Scholar] [CrossRef] [PubMed]
- Thomas, S.; Nesargi, S.; Roshan, P.; Raju, R.; Mathew, S.; Rao, S. Gastric residual volumes versus abdominal girth measurement in assessment of feed tolerance in preterm neonates: A randomized controlled trial. Adv. Neonatal Care 2018, 18, E13–E19. [Google Scholar] [CrossRef] [PubMed]
- Patel, R.M.; Ferguson, J.; McElroy, S.J.; Khashu, M.; Caplan, M.S. Defining necrotizing enterocolitis: Current difficulties and future opportunities. Pediatr. Res. 2020, 88, 10–15. [Google Scholar] [CrossRef]
- Nieminen, P. Application of Standardized Regression Coefficient in Meta-Analysis. BioMedInformatics 2022, 2, 434–458. [Google Scholar] [CrossRef]
- Migliavaca, C.B.; Stein, C.; Colpani, V.; Barker, T.H.; Ziegelmann, P.K.; Munn, Z.; Falavigna, M. Meta-analysis of prevalence: I 2 statistic and how to deal with heterogeneity. Res. Synth. Methods 2022, 13, 363–367. [Google Scholar] [CrossRef]
- Bertino, E.; Giuliani, F.; Prandi, G.; Coscia, A.; Martano, C.; Fabris, C. Necrotizing enterocolitis: Risk factor analysis and role of gastric residuals in very low birth weight infants. J. Pediatr. Gastroenterol. Nutr. 2009, 48, 437–442. [Google Scholar] [CrossRef] [PubMed]
- dos Santos Mezzacappa, M.A.M.; Collares, F.F. Gastric emptying in premature newborns with acute respiratory distress. J. Pediatr. Gastroenterol. Nutr. 2005, 40, 339–344. [Google Scholar] [CrossRef]
- Ruccio, L.R. Discarding Residuals: Implementing a Feeding Algorithm in a Neonatal Intensive Care Unit. 2021. Available online: https://archive.hshsl.umaryland.edu/handle/10713/15689 (accessed on 1 March 2025).
- Fucile, S.; Samdup, D.; MacFarlane, V.; Sinclair, M.A. Risk Factors Associated with Long-term Feeding Problems in Preterm Infants: A Scoping Review. Adv. Neonatal Care 2022, 22, 161–169. [Google Scholar] [CrossRef]
- Singh, B.; Rochow, N.; Chessell, L.; Wilson, J.; Cunningham, K.; Fusch, C.; Dutta, S.; Thomas, S. Gastric residual volume in feeding advancement in preterm infants (grip study): A randomized trial. J. Pediatr. 2018, 200, 79–83. [Google Scholar] [CrossRef]
- Sharma, P.; Nangia, S.; Tiwari, S.; Goel, A.; Singla, B.; Saili, A. Gastric lavage for prevention of feeding problems in neonates with meconium-stained amniotic fluid: A randomised controlled trial. Ann. Trop. Paediatr. 2014, 34, 115–119. [Google Scholar] [CrossRef] [PubMed]
- Krishnamurthy, S.; Gupta, P.; Debnath, S.; Gomber, S. Slow versus rapid enteral feeding advancement in preterm newborn infants 1000–1499 g: A randomized controlled trial. Acta Paediatr. 2010, 99, 42–46. [Google Scholar] [CrossRef] [PubMed]
- Bala, P.; Kaur, R.; Mukhopadhyay, K.; Kaur, S. Oromotor stimulation for transition from gavage to full oral feeding in preterm neonates: A randomized controlled trial. Indian Pediatr. 2016, 53, 36–38. [Google Scholar] [CrossRef] [PubMed]
- Ardiansyah, D.; Nurhidayah, I.; Trisyany, Y.; Apriany, D.; Setiasih, Y. Effect of abdominal massage on feeding intolerance among premature baby with mechanical ventilation in neonatal intensive care unit in Indonesia. J. Neonatal Nurs. 2021, 27, 280–284. [Google Scholar] [CrossRef]
- Terrin, G.; Conti, M.G.; Antonella, S. Enteral feeding and infections in preterm neonates. In Diet and Nutrition in Critical Care; Springer: Berlin, Germany, 2015; pp. 1481–1498. [Google Scholar]
- Munkstrup, C.; Krogfelt, K.A.; Greisen, G.; Juhl, S.M. Feeding tube practices and the colonisation of the preterm stomach in the first week of life. Dan. Med. J. 2022, 69, 8. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Database | PICO | MeSH Term | Keyword Term |
|---|---|---|---|
| PubMed, CINAHL, Web of science, ProQuest Dissertations Cochrane, Clinical Trial Registry of India, ClinicalTrials.gov, Australian New Zealand Clinical Trial Registry, and EU Clinical Trials Register (the Cochrane Neonatal search strategy for specialized register). | Population | Preterm neonate, premature born | Preterm AND Neonate Low birth weight AND premature Preterm neonate NOT Term neonate |
| Intervention | Routine prefeed gastric residue monitoring | Gastric residual OR Gastric aspirate | |
| Comparison | No prefeed gastric residue aspiration (or another intervention) | Avoid AND gastric residual OR abdominal Girth monitoring | |
| Outcome | NEC, time to reach full enteral feeds, number of days of parenteral nutrition, sepsis, and mortality | NEC AND gastric residual monitoring time to reach full enteral feeds AND gastric residual monitoring, sepsis AND gastric residual monitoring, mortality AND gastric residual monitoring | |
| Time | 2017–2023 | ||
| Study | Randomized OR quasi-randomized trials OR cluster-randomized trials | ||
| Criteria | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Type of studies | Randomized or quasi-randomized trials and cluster-randomized trials from 2017 to 2023, comparing routine prefeed gastric residual aspiration with either no aspiration or any other intervention. | Reviews, letters to editors, editorials, survey reports, only abstract available, animal studies |
| Type of participants | Preterm (<37 weeks’ gestation) infants on gavage feeds (nasogastric (NG) tube). | Term neonates, older children |
| Type of intervention and control | Intervention: Routine monitoring of gastric of enteral feeds in infants. | Studies with descriptive results and outcomes not numerically reported |
| Control: No monitoring of gastric residual or other alternative monitoring approach. | Studies reporting laboratory data only | |
| Article | Full text availability, all language articles. |
| GRADE Quality of Evidence | Interpretation |
|---|---|
| High quality | “Further research is very unlikely to change the confidence in the estimate of effect” |
| Moderate quality | “Further research is likely to have an impact confidence in the estimate of effect and may change the estimate” |
| Low quality | “Further research is very likely to have an impact confidence in the estimate of effect and is likely to change the estimate” |
| Very low quality | “Any estimate of effect is very uncertain” |
| Study Authors | Participant Characteristics | Number of Patients | Outcome/s Assessed in the Study | Remarks | GRADE Evidence | ||||
|---|---|---|---|---|---|---|---|---|---|
| Routine Gastric Residual Volume Evaluations | No Gastric Residual Volume Evaluations or Other Interventions Adopted | ||||||||
| Gestational Age (Week) (SD) | Birth Weight (g) (SD) | Gestational Age (Week) (SD) | Birth Weight (g) (SD) | ||||||
| Akar 2019 [20] | 30.37 ± 2.58 | 1538.48 ± 509.05 | 29.31 ± 3.37 | 1443.65 ± 550.38 | 169 | 122 | -Days to full enteral intake; -Days of parenteral nutrition; -Sepsis (late sepsis); -NEC ≥ grade 2, patent ductus arteriosus; -IVH (all grades); -Duration of invasive mechanical ventilation (days); -Weight at discharge (g); -Duration of nCPAP (days); -Duration of hospitalization (days). | Total duration of parenteral nutrition, ≥grade 2 NEC, weight at discharge and duration of hospitalization were reported to be similar between the groups. Supports the avoidance of routine gastric residual control before each feeding as it shortens the time to full enteral intake without increasing the incidence of NEC and duration of parenteral feeding. | Moderate |
| Elia 2022 [21] | 28.1 ± 2.5 | 1084 ± 347 | 27.8 ± 2.2 | 1100 ± 427 | 59 | 49 | -Age at full (150 mL/kg/d) enteral feeding (d); -Age at full oral enteral feeding (d); -Age at birth weight recovery (d); -Duration of parenteral nutrition (d); -Duration of NICU stay (d); -Duration of hospital stay (d). | Supports the selective monitoring of GR in extremely preterm infants and was associated with a decrease in age at full enteral feeding and at birth weight recovery, and was associated with better Z-scores of weight at discharge in comparison with routine GR monitoring. | Moderate |
| Parker 2019 [22] | 27.1 (2.4) (SD), wk | 888.8 (206.6) (SD), g | 27.0 (1.2) (SD), wk | 915.2 (180.0) (SD), g | 74 | 69 | -Days to full feeds, 120 mL/kg/d; -Hours of parenteral nutrition; -Hours with central access; -Days requiring invasive ventilation; -Days to discharge. | Incidence of NEC, late-onset sepsis, and ventilator-associated pneumonia were reported to be similar between groups. The study concluded that among extremely preterm infants, the omission of gastric residual evaluation increased the delivery of enteral nutrition as well as improved weight gain and led to earlier hospital discharge. | Moderate |
| Ramadan 2020 [23] | 32.13 ± 3.34 | 75.19 ± 12.89 | 32.68 ± 2.99 | 74.88 ± 11.56 | 30 | 30 | -Days to full enteral intake of 120 mL kg per day; -Days of PN; -Days of life to parenteral nutrition discontinuation; -Days to discharge; -Sepsis; -NEC (definite); -Weight at discharge mean. | It is concluded here that eliminating routine prefeed gastric aspirate monitoring decreases late-onset sepsis, permits preterm infants to receive complete enteral feeds sooner, and allows them to leave the hospital sooner. It also did not affect the likelihood of mortality or NEC. | Low |
| Riskin 2017 [24] | 32.0 (29.7–33.0) | 1625 (1207–1934) | 32.4 (30.4–33.4) | 1645 (1297–1954) | 239 | 233 | -NPO (d); -Number of NPO episodes; -PN (d); -Age at full enteral feeds (d); -Time to full enteral feeds (d); -Age at full PO feeds (d); -LOS (d); -Weight at discharge (g); -Weight gain from birth to discharge (g); -Percent weight gain (%); -Postmenstrual age at discharge (wk); -NEC (%) infants with NEC Bell stage ≥ 2 (%); -Days of antibiotic treatment (d); -Number of infections. | Reports that the time to full oral feedings and lengths of stay were similar in both groups. The rate of NEC was reported as being higher in the selective gastric residual volume evaluation group. This study states that the strongest predictor of time to full enteral feedings is GA. This study highlights that the routine evaluation of gastric residual volume and increasing time on non-invasive ventilation both prolong the attainment of full enteral feedings. | Moderate |
| Thomas 2018 [25] | 30.8 ± 1.5 | 30.8 ± 1.5 | 30.8 ± 1.5 | 1312 ± 265.7 | 24 | 26 (AG monitoring) | -Time to reach full feeds, d; -Episodes of feed intolerance; -No. of feeds withheld; -Duration of hospital stay, d; -Duration of parenteral nutrition, d; -Sepsis, n; -NEC. | This study concludes that the infants in the AG group reached full feeds earlier than infants in the GRV group. No significant differences were found between the two groups with regard to secondary outcomes. The study recommends abdominal girth measurement as a marker for feed tolerance but suggests that it needs to be studied in infants less than 750 g and at less than 26 weeks of gestation. | Low |
| Outcome | No. of Studies (Participants) | RR/MD [95% CI] | Heterogeneity (I2), p Value |
|---|---|---|---|
| Time to reach full feeds (180 mL/kg/day) | 4 (996) | −3.00 [−3.26, −1.52] | 0%, 0.7 |
| Any sepsis | 5 (1118) | 0.617 [0.32, 0.81] | 0%, 0.5 |
| Days of central venous line usage | 2 (434) | −0.98 [−5.12, 1.18] | 64%, 0.3 |
| All-cause mortality | 2 (160) | 0.44 [0.23, 0.92] | 0%, 0.2 |
| Time to regain birth weight | 1 (100) | −0.69 [−1.38, 0.88] | 0%, 1.1 |
| Outcome Parameter | ≤32 Weeks/≤1250 g | >1250 g | ||
|---|---|---|---|---|
| No. of Studies (Participants) | RR/MD [95% CI] | No. of Studies (Participants) | RR/MD [95% CI] | |
| NEC (stage 2 or more) | 5 (1118) | 1.00 [0.13, 3.12] | - | 0.04 [0.02, 1.29] |
| Time to reach full enteral feeds | 5 (1118) | −1.22 [−3.41, 0.22] | - | −0.01 [−1.43, 1.82] |
| Culture-positive sepsis | 4 (1020) | 0.73 [0.59, 1.31] | 1 (46) | 0.116 [0.02, 2.98] |
| Any sepsis | 4 (966) | 0.90 [0.52, 1.12] | 1 (122) | 0.16 [0.01, 1.91] |
| Days of total parenteral nutrition | 5 (1118) | −0.23 [−1631, 0.31] | - | - |
| Days of central venous line usage | 4 (434) | −1.37 [−5.51, 2.0] | - | - |
| All-cause mortality | 2 (160) | 0.13 [0.05, 0.34] | 1 (17) | 0.271 [0.01, 8.11] |
| Time to regain birth weight | - | - | 1 (100) | −1.21 [−6.05, 1.35] |
| Duration of hospital stay | 5 (11066) | −5.30 [−12.00, 0.33] | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-shehri, H. Practice of Routine Monitoring of Gastric Residual in Preterm Infants: A Meta-Analysis Article. Children 2025, 12, 526. https://doi.org/10.3390/children12040526
Al-shehri H. Practice of Routine Monitoring of Gastric Residual in Preterm Infants: A Meta-Analysis Article. Children. 2025; 12(4):526. https://doi.org/10.3390/children12040526
Chicago/Turabian StyleAl-shehri, Hassan. 2025. "Practice of Routine Monitoring of Gastric Residual in Preterm Infants: A Meta-Analysis Article" Children 12, no. 4: 526. https://doi.org/10.3390/children12040526
APA StyleAl-shehri, H. (2025). Practice of Routine Monitoring of Gastric Residual in Preterm Infants: A Meta-Analysis Article. Children, 12(4), 526. https://doi.org/10.3390/children12040526