
Attendance in a Neonatal Follow-Up Program before and in the Time of COVID-19 Pandemic: A Mixed Prospective–Retrospective Observational Study

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Statistical Analysis
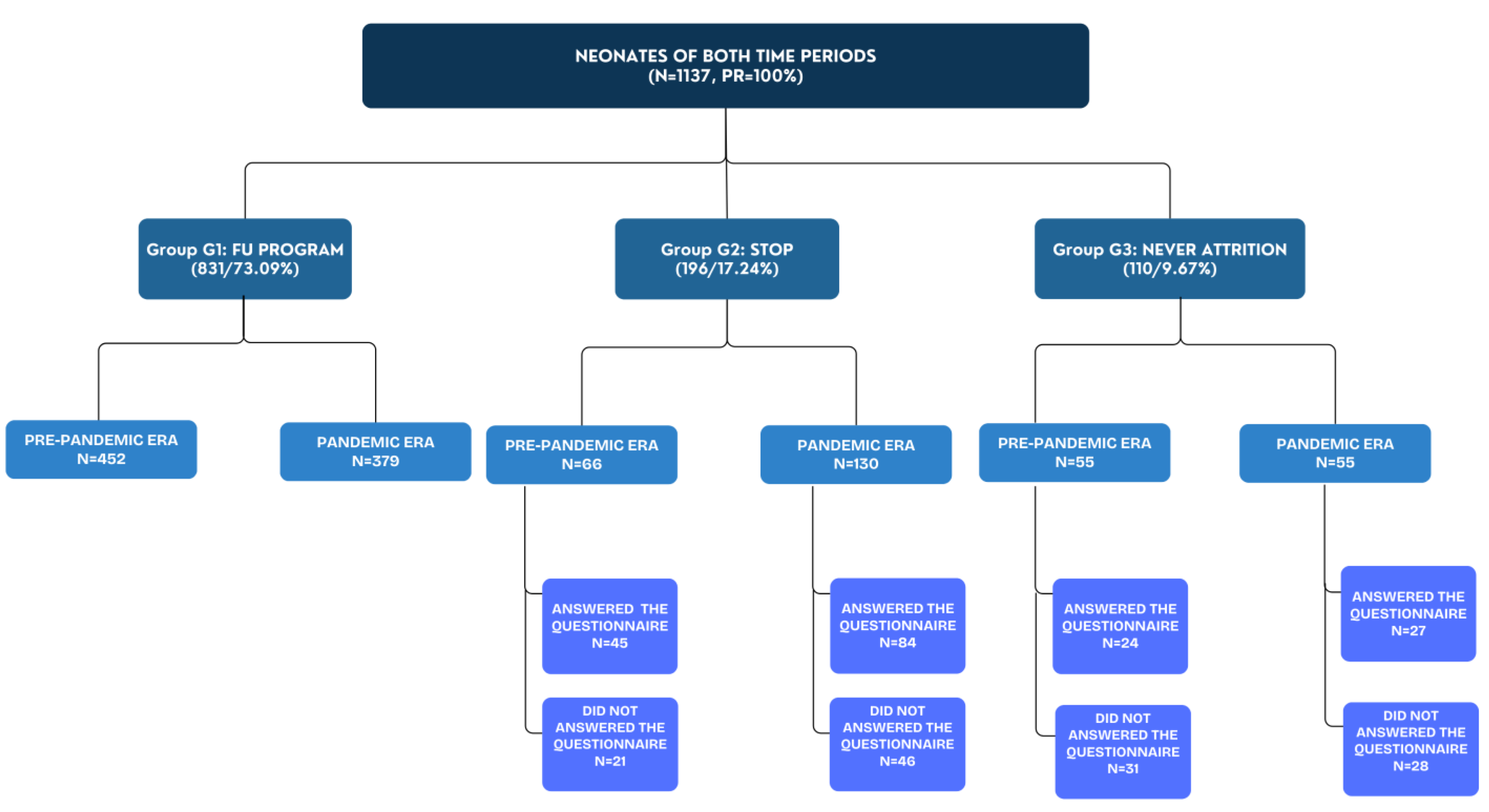
3. Results
3.1. Clinical and Demographic Characteristics before and after the Onset of COVID-19
3.2. Attendance Rates before and after the Onset of COVID-19
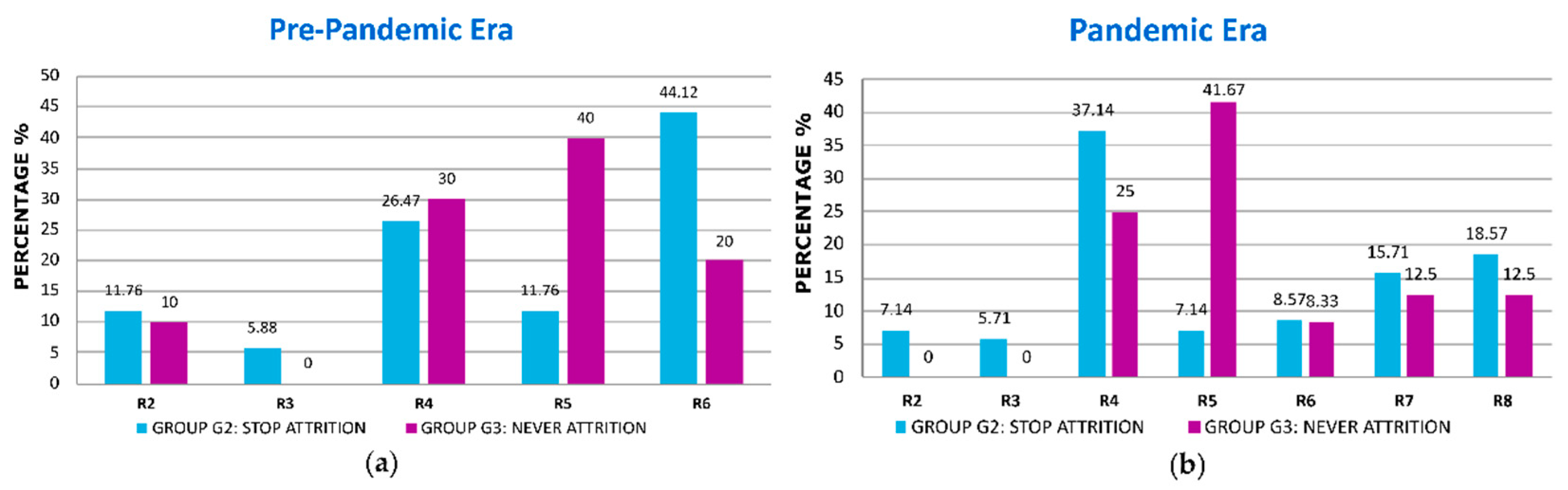
3.2.1. Reasons for Non-Attendance
3.2.2. Comparisons between Groups before the Onset of COVID-19
3.2.3. Comparisons between Groups after the Onset of COVID-19
3.2.4. Multiple Regression Analysis
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
References
- Blencowe, H.; Cousens, S.; Oestergaard, M.Z.; Chou, D.; Moller, A.-B.; Narwal, R.; Adler, A.; Garcia, C.V.; Rohde, S.; Say, L.; et al. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: A systematic analysis and implications. Lancet 2012, 379, 2162–2172. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Preterm Birth [Internet]. Available online: https://www.who.int/news-room/fact-sheets/detail/preterm-birth (accessed on 28 May 2023).
- McCormick, M.C.; Litt, J.S.; Smith, V.C.; Zupancic, J.A.F. Prematurity: An Overview and Public Health Implications. Annu. Rev. Public Health 2011, 32, 367–379. [Google Scholar] [CrossRef] [PubMed]
- Litt, J.S.; Campbell, D.E. High-Risk Infant Follow-Up after NICU Discharge. Clin. Perinatol. 2023, 50, 225–238. [Google Scholar] [CrossRef] [PubMed]
- Spittle, A.; Treyvaud, K. The role of early developmental intervention to influence neurobehavioral outcomes of children born preterm. Semin. Perinatol. 2016, 40, 542–548. [Google Scholar] [CrossRef]
- Patra, K.; Greene, M.M.; Perez, B.; Silvestri, J.M. Neonatal high-risk follow-up clinics: How to improve attendance in very low birth weight infants. E-J. Neonatal Res. 2014, 4, 3–12. [Google Scholar]
- McGowan, E.C.; Vohr, B.R. Neurodevelopmental Follow-up of Preterm Infants. Pediatr. Clin. N. Am. 2019, 66, 509–523. [Google Scholar] [CrossRef]
- Purdy, I.B.; Melwak, M.A. Who Is at Risk? High-Risk Infant Follow-up. Newborn Infant Nurs. Rev. 2012, 12, 221–226. [Google Scholar] [CrossRef]
- Orton, J.; Spittle, A.; Doyle, L.; Anderson, P.; Boyd, R. Do early intervention programmes improve cognitive and motor outcomes for preterm infants after discharge? A systematic review: Early Intervention for Preterm Infants. Dev. Med. Child. Neurol. 2009, 51, 851–859. [Google Scholar] [CrossRef]
- Doyle, L.W.; Anderson, P.J.; Battin, M.; Bowen, J.R.; Brown, N.; Callanan, C.; Campbell, C.; Chandler, S.; Cheong, J.; Darlow, B.; et al. Long term follow up of high risk children: Who, why and how? BMC Pediatr. 2014, 14, 279. [Google Scholar] [CrossRef]
- Ayala, L.; Winter, S.; Byrne, R.; Fehlings, D.; Gehred, A.; Letzkus, L.; Noritz, G.; Paton, M.C.; Pietruszewski, L.; Rosenberg, N.; et al. Assessments and Interventions for Spasticity in Infants with or at High Risk for Cerebral Palsy: A Systematic Review. Pediatr. Neurol. 2021, 118, 72–90. [Google Scholar] [CrossRef]
- Kuppala, V.S.; Tabangin, M.; Haberman, B.; Steichen, J.; Yolton, K. Current state of high-risk infant follow-up care in the United States: Results of a national survey of academic follow-up programs. J. Perinatol. 2012, 32, 293–298. [Google Scholar] [CrossRef] [PubMed]
- Tang, B. The State of Neonatal Follow-Up Programs. In Follow-Up for NICU Graduates: Promoting Positive Developmental and Behavioral Outcomes for At-Risk Infants; Needelman, H., Jackson, B.J., Eds.; Springer International Publishing: Cham, Switzerland, 2018; pp. 337–341. [Google Scholar] [CrossRef]
- Vohr, B.R.; O’Shea, M.; Wright, L.L. Longitudinal multicenter follow-up of high-risk infants: Why, who, when, and what to assess. Semin. Perinatol. 2003, 27, 333–342. [Google Scholar] [CrossRef] [PubMed]
- Bhutta, A.T.; Cleves, M.A.; Casey, P.H.; Cradock, M.M.; Anand, K.J.S. Cognitive and Behavioral Outcomes of School-Aged Children Who Were Born Preterm: A Meta-analysis. JAMA 2002, 288, 728. [Google Scholar] [CrossRef] [PubMed]
- Maitre, N.L.; Duncan, A.F. Neurologic and Developmental Outcomes of High-Risk Neonates. Clin. Perinatol. 2023, 50, xxi–xxii. [Google Scholar] [CrossRef] [PubMed]
- Perenyi, A.; Katz, J.; Flom, P.; Regensberg, S.; Sklar, T. Analysis of compliance, morbidities and outcome in neurodevelopmental follow-up visits in urban African-American infants at environmental risk. J. Dev. Orig. Health Dis. 2010, 1, 396–402. [Google Scholar] [CrossRef]
- Tang, B.; Lee, H.; Gray, E.; Gould, J.; Hintz, S. Programmatic and Administrative Barriers to High-Risk Infant Follow-Up Care. Am. J. Perinatol. 2018, 35, 940–945. [Google Scholar]
- Ballantyne, M.; Stevens, B.; Guttmann, A.; Willan, A.R.; Rosenbaum, P. Transition to Neonatal Follow-up Programs: Is Attendance a Problem? J. Perinat. Neonatal Nurs. 2012, 26, 90–98. [Google Scholar] [CrossRef]
- Harmon, S.L.; Conaway, M.; Sinkin, R.A.; Blackman, J.A. Factors associated with neonatal intensive care follow-up appointment compliance. Clin. Pediatr. 2013, 52, 389–396. [Google Scholar] [CrossRef]
- Brady, J.M.; Pouppirt, N.; Bernbaum, J.; D’Agostino, J.A.; Gerdes, M.; Hoffman, C.; Cook, N.; Hurt, H.; Kirpalani, H.; DeMauro, S.B. Why do children with severe bronchopulmonary dysplasia not attend neonatal follow-up care? Parental views of barriers. Acta Paediatr. 2018, 107, 996–1002. [Google Scholar] [CrossRef]
- Swearingen, C.; Simpson, P.; Cabacungan, E.; Cohen, S. Social disparities negatively impact neonatal follow-up clinic attendance of premature infants discharged from the neonatal intensive care unit. J. Perinatol. 2020, 40, 790–797. [Google Scholar] [CrossRef]
- DeMauro, S.B.; Bellamy, S.L.; Fernando, M.; Hoffmann, J.; Gratton, T.; Schmidt, B.; PROP Investigators. Patient, Family, and Center-Based Factors Associated with Attrition in Neonatal Clinical Research: A Prospective Study. Neonatology 2019, 115, 328–334. [Google Scholar] [CrossRef] [PubMed]
- Duarte, E.D.; Tavares, T.S.; Cardoso, I.V.L.; Vieira, C.S.; Guimarães, B.R.; Bueno, M. Factors associated with the discontinuance of outpatient follow-up in neonatal units. Rev. Bras. Enferm. 2020, 73, e20180793. [Google Scholar] [CrossRef] [PubMed]
- Ballantyne, M.; Benzies, K.; Rosenbaum, P.; Lodha, A. Mothers’ and health care providers’ perspectives of the barriers and facilitators to attendance at Canadian neonatal follow-up programs. Child. Care Health Dev. 2015, 41, 722–733. [Google Scholar] [CrossRef]
- Hintz, S.R.; Gould, J.B.; Bennett, M.V.; Lu, T.; Gray, E.E.; Jocson, M.A.L.; Fuller, M.G.; Lee, H.C. Factors Associated with Successful First High-Risk Infant Clinic Visit for Very Low Birth Weight Infants in California. J. Pediatr. 2019, 210, 91–98.e1. [Google Scholar] [CrossRef]
- Ballantyne, M.; Stevens, B.; Guttmann, A.; Willan, A.R.; Rosenbaum, P. Maternal and infant predictors of attendance at Neonatal Follow-Up programmes. Child. Care Health Dev. 2014, 40, 250–258. [Google Scholar] [CrossRef] [PubMed]
- Kim, N.H.; Youn, Y.A.; Cho, S.J.; Hwang, J.-H.; Kim, E.-K.; Kim, E.A.-R.; Lee, S.M.; Network, K.N. The predictors for the non-compliance to follow-up among very low birth weight infants in the Korean neonatal network. Gurgel RQ, editor. PLoS ONE 2018, 13, e0204421. [Google Scholar] [CrossRef]
- Nehra, V.; Pici, M.; Visintainer, P.; Kase, J.S. Indicators of compliance for developmental follow-up of infants discharged from a regional NICU. J. Perinat. Med. 2009, 37, 677–681. [Google Scholar] [CrossRef]
- Tuczyńska, M.; Matthews-Kozanecka, M.; Baum, E. Accessibility to Non-COVID Health Services in the World During the COVID-19 Pandemic: Review. Front. Public Health 2021, 9, 760795. [Google Scholar] [CrossRef]
- De Biase, S.; Cook, L.; Skelton, D.A.; Witham, M.; ten Hove, R. The COVID-19 rehabilitation pandemic. Age Ageing 2020, 49, 696–700. [Google Scholar] [CrossRef]
- Kondilis, E.; Tarantilis, F.; Benos, A. Essential public healthcare services utilization and excess non-COVID-19 mortality in Greece. Public Health 2021, 198, 85–88. [Google Scholar] [CrossRef]
- Roberton, T.; Carter, E.D.; Chou, V.B.; Stegmuller, A.R.; Jackson, B.D.; Tam, Y.; Sawadogo-Lewis, T.; Walker, N. Early estimates of the indirect effects of the COVID-19 pandemic on maternal and child mortality in low-income and middle-income countries: A modelling study. Lancet Glob. Health 2020, 8, e901–e908. [Google Scholar] [CrossRef] [PubMed]
- Erdei, C.; Liu, C.H. The downstream effects of COVID-19: A call for supporting family wellbeing in the NICU. J. Perinatol. 2020, 40, 1283–1285. [Google Scholar] [CrossRef] [PubMed]
- Fazzi, E.; Galli, J. New clinical needs and strategies for care in children with neurodisability during COVID-19. Dev. Med. Child Neurol. 2020, 62, 879–880. [Google Scholar] [CrossRef] [PubMed]
- Fraiman, Y.S.; Edwards, E.M.; Horbar, J.D.; Mercier, C.E.; Soll, R.F.; Litt, J.S. Racial Inequity in High-Risk Infant Follow-Up among Extremely Low Birth Weight Infants. Pediatrics 2023, 151, e2022057865. [Google Scholar] [CrossRef] [PubMed]
- Fuller, M.G.; Lu, T.; Gray, E.E.; Jocson, M.A.L.; Barger, M.K.; Bennett, M.; Lee, H.C.; Hintz, S.R. Rural Residence and Factors Associated with Attendance at the Second High-Risk Infant Follow-up Clinic Visit for Very Low Birth Weight Infants in California. Am. J. Perinatol. 2023, 40, 546–556. [Google Scholar] [CrossRef]
- Attar, M.A.; Gates, M.R.; Iatrow, A.M.; Lang, S.W.; Bratton, S.L. Barriers to Screening Infants for Retinopathy of Prematurity after Discharge or Transfer from a Neonatal Intensive Care Unit. J. Perinatol. 2005, 25, 36–40. [Google Scholar] [CrossRef]
- Panda, S.; Somu, R.; Maitre, N.; Levin, G.; Singh, A.P. Impact of the Coronavirus Pandemic on High-Risk Infant Follow-Up (HRIF) Programs: A Survey of Academic Programs. Children 2021, 8, 889. [Google Scholar] [CrossRef]
- Roberts, H.J.; Harris, R.M.; Krehbiel, C.; Banks, B.; Jackson, B.; Needelman, H. Examining disparities in the long term follow-up of Neonatal Intensive Care Unit graduates in Nebraska, U.S.A. J. Neonatal. Nurs. 2016, 22, 250–256. [Google Scholar] [CrossRef]
- Watson, L.; Woods, C.W.; Cutler, A.; DiPalazzo, J.; Craig, A.K. Telemedicine Improves Rate of Successful First Visit to NICU Follow-up Clinic. Hosp. Pediatr. 2023, 13, 3–8. [Google Scholar] [CrossRef]
- Caporali, C.; Pisoni, C.; Naboni, C.; Provenzi, L.; Orcesi, S. Challenges and opportunities for early intervention and neurodevelopmental follow-up in preterm infants during the COVID-19 pandemic. Child. Care Health Dev. 2021, 47, 140–141. [Google Scholar] [CrossRef]
- Christner, L.P.; Irani, S.; McGowan, C.; Dabaja, E.; Dejong, C.; Attar, M.A. Previous missed visits and independent risk of loss to follow-up in the high-risk neonatal follow-up clinic. Early Hum. Dev. 2023, 183, 105813. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Reasons for Νon-Attendance (R) | Categorization |
|---|---|
| R1 | Lack of health insurance. |
| R2 | Accessibility (distance of the clinic from the permanent residence/lack of means of transport/change in residence/moving (to another region/country)/bad weather. |
| R3 | Loaded parental/family work schedule. |
| R4 | Obstacles related to hospital services (limited availability during clinic hours/difficulty with parking/long waiting time/bad communication with the secretariat/disappointment from the experience at the hospital. Change (cancelation or postponement) either after consultation (with the Hospital/with Papageorgiou’s doctors) or at the initiative of the parents, closed outpatient clinics due to COVID-19. |
| R5 | Negligence–Absence of Specific Reason. |
| R6 | Assessment by the parents that monitoring/FU appointment was unnecessary. |
| R7 | Health issues/Death in the family. |
| R8 | Fear of diseases exposure (to COVID-19 or other diseases)/Difficulties due to COVID-19 (“Because only one parent was allowed to accompany” or difficulty with Rapid Tests). |
| Characteristics | Pre-Pandemic Era (n = 573) | Pandemic Era (n = 564) | p | OR and 95% CI |
|---|---|---|---|---|
| Gender (Male) a | 315 (54.97) | 283 (50.18) | 0.1091 | 0.82 (0.65–1.04) |
| Birth weight (gr) a | 2090 (1620–2830) | 1830 (1430–2490) | 0.0005 | NA |
| Gestational age (weeks) a | 34.6 (32–37.3) | 33.1 (31.4–35.7) | 0.0003 | NA |
| Age of mother a | 32 (29–38) | 33 (29–38) | 0.3454 | NA |
| Multiparity a | 1 (1–2) | 1 (1–2) | 0.4379 | NA |
| Multiple Gestation b | 104 (34.9) | 137 (34.25) | 0.8724 | 0.97 (0.71–1.33) |
| Small for Gestational Age (SGA) b | 72 (25.09) | 80 (20.89) | 0.2256 | 0.79 (0.55–1.13) |
| Gestational Hypertension b | 30 (11.03) | 55 (14.82) | 0.1947 | 1.4 (0.87–2.26) |
| Gestational Diabetes b | 34 (13.08) | 127 (36.6) | <0.0001 | 3.84 (2.52–5.85) |
| IntraUterine Growth Retardation (IUGR) b | 54 (19.85) | 94 (25.34) | 0.1078 | 1.37 (0.94–2) |
| Delivery mode: Cesarean Section (CS) b | 235 (80.48) | 317 (83.42) | 0.3607 | 0.82 (0.55–1.22) |
| Antenatal Steroid Administration (ASA) b | 62 (26.72) | 137 (37.53) | 0.0075 | 1.65 (1.15–2.36) |
| Respiratory Distress Syndrome b | 87 (29.49) | 173 (42.3) | 0.0005 | 1.75 (1.28–2.41) |
| Bronchopulmonary dysplasia b | 29 (9.83) | 44 (10.76) | 0.7092 | 1.11 (0.67–1.81) |
| Early onset sepsis (<=3 DOL) b | 35 (12.07) | 13 (3.32) | <0.0001 | 0.25 (0.13–0.48) |
| Late onset sepsis (>3 DOL) b | 38 (13.1) | 73 (18.39) | 0.0742 | 1.49 (0.98–2.29) |
| Jaundice b | 236 (64.13) | 277 (63.68) | 0.9412 | 0.98 (0.73–1.31) |
| Necrotizing Enterocolitis b | 6 (2.08) | 15 (3.87) | 0.2623 | 1.9 (0.73–4.95) |
| Retinopathy of Prematurity b | 7 (2.45) | 8 (2.04) | 0.7941 | 0.83 (0.3–2.31) |
| Number of visits a | 1 (1–4) | 2 (1–3) | 0.8534 | NA |
| Nationality (Foreign) b | 64 (11.17) | 67 (11.88) | 0.7114 | 0.93 (0.65–1.34) |
| Characteristics | G1 Group (n = 451) | G2 Group (n = 66) | G3 Group (n = 53) | G1 vs. G2 | G1 vs. G3 | ||
|---|---|---|---|---|---|---|---|
| p | OR (95% CI) | p | OR (95% CI) | ||||
| Number of visits a | 2 (1–5) | 2 (1–3) | 0 (0–0) | 0.329605 | NA | <0.0001 | NA |
| Birth weight (gr) a | 2115 (1620–2835) | 1750 (1355–2400) | 2282.5 (1917.5–3290) | 0.008906 | NA | 0.0264 | NA |
| Gestational age (weeks) a | 34.6 (32.1–37.1) | 32.9 (29.7–35.6) | 36.3 (33–38.3) | 0.002245 | NA | 0.0108 | NA |
| Antenatal Steroid Administration (ASA) b | 43 (29.25) | 14 (30.44) | 3 (8.11) | 0.86 | 1.06 (0.51–2.18) | 0.0097 | 4.76 (1.37–16.67) |
| Multiparity a | 1 (1–2) | 1 (1–2) | 2 (1–2.5) | 0.422272 | NA | <0.0001 | NA |
| Multiple Gestation b | 71 (38.17) | 22 (37.93) | 9 (17.31) | 1 | 0.99 (0.54–1.82) | 0.0047 | 2.94 (1.35–6.25) |
| Jaundice b | 169 (67.33) | 43 (69.36) | 23 (43.4) | 0.8796 | 1.1 (0.6–2) | 0.0016 | 2.70 (1.47–5) |
| Respiratory Distress Syndrome b | 54 (29.67) | 23 (38.98) | 8 (15.38) | 0.2005 | 1.51 (0.82–2.79) | 0.0493 | 2.33 (1.02–5.26) |
| Nationality (Foreign) b | 42 (9.31) | 9 (13.64) | 13 (24.53) | 0.2706 | 0.65 (0.3–1.41) | 0.0037 | 3.13 (1.56–6.25) |
| Characteristics | G1 Group (n = 451) | G2 Group (n = 66) | G3 Group (n = 53) | G1 vs. G2 | G1 vs. G3 | |
|---|---|---|---|---|---|---|
| p | OR (95% CI) | p | ||||
| Number of visits a | 2 (1–4) | 2 (1–3) | 0 (0–0) | 0.0006 | NA | 0.05 |
| Birth weight (gr) a | 1830 (1420–2430) | 1710 (1410–2250) | 2142.5 (1600–2660) | 0.3045 | NA | 0.0373 |
| Gestational age (weeks) a | 33.3 (31.1–36) | 32.4 (30.9–34.7) | 34.4 (33–37.4) | 0.1450 | NA | 0.0030 |
| Multiparity a | 1 (1–2) | 2 (1–2) | 2 (1–3) | 0.1980 | NA | 0.0091 |
| Jaundice b | 183 (68.03) | 76 (63.87) | 18 (38.3) | 0.4833 | NA | 0.0001 |
| Late onset sepsis (>3 DOL) b | 37 (16.02) | 34 (28.33) | 2 (4.35) | 0.0100 | 0.48 (0.28–0.82) | 0.0372 |
| Necrotizing Enterocolitis b | 6 (2.64) | 9 (7.76) | 0 (0) | 0.0467 | 0.32 (0.11–0.93) | 0.5936 |
| Respiratory Distress Syndrome b | 108 (44.81) | 53 (44.17) | 12 (25) | 1 | NA | 0.0155 |
| Hours of work b | 40 (20–40) | 40 (0–40) | 17.5 (0–40) | 0.2736 | NA | 0.0239 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nantsi, E.; Chatziioannidis, I.; Pouliakis, A.; Mitsiakos, G.; Kondilis, E. Attendance in a Neonatal Follow-Up Program before and in the Time of COVID-19 Pandemic: A Mixed Prospective–Retrospective Observational Study. Children 2024, 11, 1138. https://doi.org/10.3390/children11091138
Nantsi E, Chatziioannidis I, Pouliakis A, Mitsiakos G, Kondilis E. Attendance in a Neonatal Follow-Up Program before and in the Time of COVID-19 Pandemic: A Mixed Prospective–Retrospective Observational Study. Children. 2024; 11(9):1138. https://doi.org/10.3390/children11091138
Chicago/Turabian StyleNantsi, Evdoxia, Ilias Chatziioannidis, Abraham Pouliakis, Georgios Mitsiakos, and Elias Kondilis. 2024. "Attendance in a Neonatal Follow-Up Program before and in the Time of COVID-19 Pandemic: A Mixed Prospective–Retrospective Observational Study" Children 11, no. 9: 1138. https://doi.org/10.3390/children11091138
APA StyleNantsi, E., Chatziioannidis, I., Pouliakis, A., Mitsiakos, G., & Kondilis, E. (2024). Attendance in a Neonatal Follow-Up Program before and in the Time of COVID-19 Pandemic: A Mixed Prospective–Retrospective Observational Study. Children, 11(9), 1138. https://doi.org/10.3390/children11091138