
Amenable Mortality in Children under 5: An Indicator for Identifying Inequalities in Healthcare Delivery: A Review
 , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
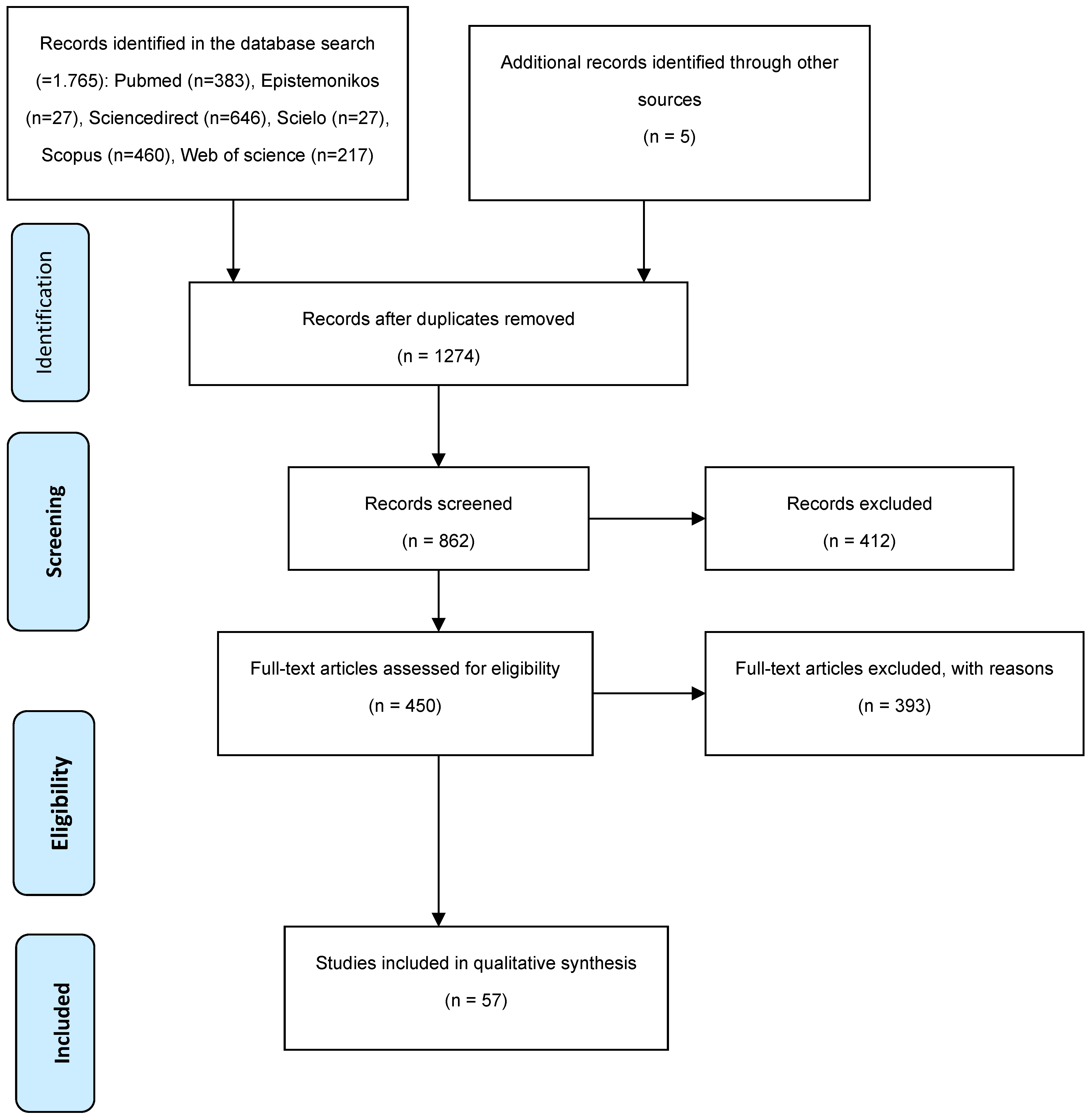
2.1. Search Strategy
- “amenable mortality”
- “treatable mortality”
- “child”
2.2. Inclusion and Exclusion Criteria
- Inclusion Criteria:
- Studies investigating amenable mortality in children under five years old.
- Articles published in English, Spanish, or Portuguese.
- Full-text articles available.
- Exclusion Criteria:
- Studies not focusing on amenable mortality (e.g., studies focusing solely on preventable mortality or all-cause mortality).
- Reviews, editorials, letters, or opinion pieces.
- Articles without full-text availability.
2.3. Data Extraction
- Study characteristics: Authors, publication year, and study design.
- Population characteristics: Age range and sample size.
- Methods: Data sources, inclusion/exclusion criteria.
- Outcomes: Amenable mortality rates and causes of death.
2.4. Data Synthesis
2.5. Study Selection
- PubMed (n = 383)
- Epistemonikos (n = 27)
- ScienceDirect (n = 646)
- SciELO (n = 27)
- Scopus (n = 460)
- Web of Science (n = 217)
2.6. Results Overview
3. Results
3.1. Low and Middle-Income Countries (LMICs)
3.2. Countries with High Economic Resources
3.3. Avoidable (and Amenable) Mortality and COVID-19
4. Discussion
4.1. Strengths and Limitations of This Study
4.2. Practical Applications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- The World Bank. Universal Health Coverage as a Sustainable Development Goal. 2023. Available online: https://datatopics.worldbank.org/world-development-indicators/stories/universal-health-coverage-as-a-sustainable-development-goal.html (accessed on 15 April 2023).
- Barredo, L.; Agyepong, I.; Liu, G.; Reddy, S. Objetivo 3—Los Objetivos de Desarrollo Sostenible y un 2030 Más Saludable. Available online: https://www.un.org/es/chronicle/article/objetivo-3-los-objetivos-de-desarrollo-sostenible-y-un-2030-mas-saludable (accessed on 15 April 2023).
- The Global Heatlh Observatory. Child Mortality and Causes of Death. 2023. Available online: https://www.who.int/data/gho/data/themes/topics/topic-details/GHO/child-mortality-and-causes-of-death#:~:text=Since1990%2Ctheglobalunder,to2.3millionin2021 (accessed on 15 April 2023).
- Wang, H.; Abajobir, A.A.; Abate, K.H.; Abbafati, C.; Abbas, K.M.; Abd-Allah, F.; Abera, S.F.; Abraha, H.N.; Abu-Raddad, L.J.; Abu-Rmeileh, N.M.E.; et al. Global, regional, and national under-5 mortality, adult mortality, age-specific mortality, and life expectancy, 1970–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1084–1150. [Google Scholar] [CrossRef] [PubMed]
- Petrou, S.; Fraser, J.; Sidebotham, P. Child death in high-income countries. Lancet 2014, 384, 831–833. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Children: Improving Survival and Well-Being. 2020. Available online: https://www.who.int/es/news-room/fact-sheets/detail/children-reducing-mortality (accessed on 26 January 2021).
- Rojas-Botero, M.; Fernández, J.A.; Borrero-Martinez, Y. Trends of inequalities of avoidable mortality among children in Colombia: A group-based trajectory analysis. Res. Sq. 2022. [Google Scholar] [CrossRef]
- Houweling, T.A.J.; Kunst, A.E. Socio-economic inequalities in childhood mortality in low- and middle-income countries: A review of the international evidence. Br. Med. Bull. 2010, 93, 7–26. [Google Scholar] [CrossRef]
- Rutstein, D.D.; Berenberg, W.; Chalmers, T.C.; Child, C.G.; Fishman, A.P.; Perrin, E.B.; Feldman, J.J.; Leaverton, P.E.; Lane, J.M.; Sencer, D.J.; et al. Measuring the Quality of Medical Care. N. Engl. J. Med. 1976, 294, 582–588. [Google Scholar] [CrossRef] [PubMed]
- Cardona, M.; Millward, J.; Gemmill, A.; Jison Yoo, K.; Bishai, D.M. Estimated impact of the 2020 economic downturn on under-5 mortality for 129 countries. PLoS ONE 2022, 17, e0263245. [Google Scholar] [CrossRef]
- Lozano, R.; Fullman, N.; Mumford, J.E.; Knight, M.; Barthelemy, C.M.; Abbafati; Abbastabar, H.; Abd-Allah, F.; Abdollahi, M.; Abedi, A.; et al. Measuring universal health coverage based on an index of effective coverage of health services in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1250–1284. [Google Scholar] [CrossRef]
- Tobias, M.; Yeh, L.-C. How much does health care contribute to health gain and to health inequality? Trends in amenable mortality in New Zealand 1981–2004. Aust. N. Z. J. Public Health 2009, 33, 70–78. [Google Scholar] [CrossRef] [PubMed]
- OECD. Avoidable Mortality: OECD/Eurostat Lists of Preventable and Treatable Causes of Death (October 2021 Version). 2021. Available online: https://www.oecd.org/health/health-systems/Avoidable-mortality-2019-Joint-OECD-Eurostat-List-preventable-treatable-causes-of-death.pdf (accessed on 30 March 2024).
- Paho. Potentially Avoidable Premature Mortality: What Is It and Why Is It Relevant? 2021. Available online: https://hia.paho.org/en/potentially-avoidable-premature-mortality-what-it-and-why-it-relevant (accessed on 15 April 2023).
- Kossarova, L.; Holland, W.; Nolte, E.; McKee, M. Measuring ‘Avoidable’ Mortality: Methodological Note. 2009. Available online: http://eprints.lse.ac.uk/46390/ (accessed on 30 March 2024).
- Rojas-Botero, M.L.; Borrero-Ramírez, Y.E.; Cáceres-Manrique, F.d.M. Lista de causas de muerte potencialmente evitables en la niñez: Una propuesta para Colombia. Cad. Saude Publica 2020, 36, e00086519. [Google Scholar] [CrossRef]
- Organización Mundial de la Salud. Mortalidad Prematura Potencialmente Evitable: ¿Qué es y por qué es relevante? 2021. Available online: https://hia.paho.org/es/mppe-por-que-relevante (accessed on 30 March 2024).
- Kruk, M.E.; Gage, A.D.; Joseph, N.T.; Danaei, G.; García-Saisó, S.; Salomon, J.A. Mortality due to low-quality health systems in the universal health coverage era: A systematic analysis of amenable deaths in 137 countries. Lancet 2018, 392, 2203–2212. [Google Scholar] [CrossRef]
- Yirgu, R.; Molla, M.; Sibley, L. Determinants of neonatal mortality in rural Northern Ethiopia: A population based nested case control study. PLoS ONE 2017, 12, e0172875. [Google Scholar] [CrossRef]
- El-Sayed, A.M.; Finkton, D.W.; Paczkowski, M.; Keyes, K.M.; Galea, S. Socioeconomic position, health behaviors, and racial disparities in cause-specific infant mortality in Michigan, USA. Prev. Med. 2015, 76, 8–13. [Google Scholar] [CrossRef]
- Bayley, O.; Chapota, H.; Kainja, E.; Phiri, T.; Gondwe, C.; King, C.; Nambiar, B.; Mwansambo, C.; Kazembe, P.; Costello, A.; et al. Community-linked maternal death review (CLMDR) to measure and prevent maternal mortality: A pilot study in rural Malawi. BMJ Open 2015, 5, e007753. [Google Scholar] [CrossRef] [PubMed]
- Bahk, J.; Jung-Choi, K. The Contribution of Avoidable Mortality to the Life Expectancy Gains in Korea between 1998 and 2017. Int. J. Environ. Res. Public Health 2020, 17, 6499. [Google Scholar] [CrossRef]
- Truche, P.; Botelho, F.; Bowder, A.N.; Levis, A.W.; Greenberg, S.L.M.; Smith, E.; Corlew, S.; Bickler, S.; Rice, H.E.; Ameh, E.A.; et al. Potentially Avertable Child Mortality Associated with Surgical Workforce Scale-up in Low- and Middle-Income Countries: A Global Study. World J. Surg. 2021, 45, 2643–2652. [Google Scholar] [CrossRef] [PubMed]
- Alvarez, J.-A.; Aburto, J.M.; Canudas-Romo, V. Latin American convergence and divergence towards the mortality profiles of developed countries. Popul. Stud. 2020, 74, 75–92. [Google Scholar] [CrossRef] [PubMed]
- Aburto, J.M.; Riffe, T.; Canudas-Romo, V. Trends in avoidable mortality over the life course in Mexico, 1990–2015: A cross-sectional demographic analysis. BMJ Open 2018, 8, e022350. [Google Scholar] [CrossRef]
- Hone, T.; Rasella, D.; Barreto, M.; Atun, R.; Majeed, A.; Millett, C. Large Reductions In Amenable Mortality Associated with Brazil’s Primary Care Expansion And Strong Health Governance. Health Aff. 2017, 36, 149–158. [Google Scholar] [CrossRef]
- Aquino, R.; de Oliveira, N.F.; Barreto, M.L. Impact of the Family Health Program on Infant Mortality in Brazilian Municipalities. Am. J. Public Health 2009, 99, 87–93. [Google Scholar] [CrossRef]
- Rasella, D.; Aquino, R.; Barreto, M.L. Impact of the Family Health Program on the quality of vital information and reduction of child unattended deaths in Brazil: An ecological longitudinal study. BMC Public Health 2010, 10, 380. [Google Scholar] [CrossRef]
- Hone, T.; Rasella, D.; Barreto, M.L.; Majeed, A.; Millett, C. Association between expansion of primary healthcare and racial inequalities in mortality amenable to primary care in Brazil: A national longitudinal analysis. PLoS Med. 2017, 14, e1002306. [Google Scholar] [CrossRef]
- Pitchon, R.R.; Alvim, C.G.; de Andrade, C.R.; Lasmar, L.M.d.L.B.F.; Cruz, Á.A.; dos Reis, A.P. Asthma mortality in children and adolescents of Brazil over a 20-year period. J. Pediatr. 2020, 96, 432–438. [Google Scholar] [CrossRef] [PubMed]
- Victora, C.G.; Barros, F.C. Infant mortality due to perinatal causes in Brazil: Trends, regional patterns and possible interventions. Sao Paulo Med. J. 2001, 119, 33–42. [Google Scholar] [CrossRef] [PubMed]
- de Assis, H.M.; Machado, C.J.; Rodrigues, R.N. Perfis de mortalidade neonatal precoce: Um estudo para uma Maternidade Pública de Belo Horizonte (MG), 2001–2006. Rev. Bras. Epidemiol. 2008, 11, 675–686. Available online: http://www.scielosp.org/scielo.php?script=sci_arttext&pid=S1415-790X2008000400014&lang=es (accessed on 30 March 2024). [CrossRef]
- Mason, L.; Dellicour, S.; Ter Kuile, F.; Ouma, P.; Phillips-Howard, P.; Were, F.; Laserson, K.; Desai, M. Barriers and facilitators to antenatal and delivery care in western Kenya: A qualitative study. BMC Pregnancy Childbirth 2015, 15, 26. [Google Scholar] [CrossRef]
- Carshon-Marsh, R.; Aimone, A.; Ansumana, R.; IB, S.; Assalif, A.; Musa, A.; Meh, C.; Smart, F.; Fu, S.H.; Newcombe, L.; et al. Child, maternal, and adult mortality in Sierra Leone: Nationally representative mortality survey 2018–2020. Lancet Glob. Health 2021, 10, e114–e123. [Google Scholar] [CrossRef] [PubMed]
- Njuma Libwea, J.; Bebey Kingue, S.R.; Taku Ashukem, N.; Kobela, M.; Boula, A.; Sinata, K.-S.; Koki Ndombo, P. Assessing the causes of under-five mortality and proportion associated with pneumococcal diseases in Cameroon. A case-finding retrospective observational study: 2006–2012. PLoS ONE 2019, 14, e0212939. [Google Scholar] [CrossRef]
- Deribew, A.; Tessema, F.; Girma, B. Determinants of under-five mortality in Gilgel Gibe Field Research Center, Southwest Ethiopia. Ethiop. J. Health Dev. 2007, 21. Available online: https://ejhd.org/index.php/ejhd/article/view/539/400 (accessed on 30 March 2024).
- Cavallin, F.; Bonasia, T.; Yimer, D.A.; Manenti, F.; Putoto, G.; Trevisanuto, D. Risk factors for mortality among neonates admitted to a special care unit in a low-resource setting. BMC Pregnancy Childbirth 2020, 20, 722. [Google Scholar] [CrossRef]
- Abd salam El Vilaly, M.; Jones, M.A.; Stankey, M.C.; Seyi-Olajide, J.; Onajin-Obembe, B.; Dasogot, A.; Klug, S.J.; Meara, J.G.; Ameh, E.A.; Osagie, O.O.; et al. Access to paediatric surgery: The geography of inequality in Nigeria. BMJ Glob. Health 2021, 6, e006025. [Google Scholar] [CrossRef]
- Ahn, B.; Mupere, E.; Irarrázaval, B.; RO, O.; Aanyu-Tukamuhebwa, H.; CB, B.; Gingo, D.; NW, G. Qualitative needs assessment for paediatric emergency care in Kampala, Uganda. Afr. J. Emerg. Med. Rev. Afr. Med. d’urgence 2021, 11, 277–282. [Google Scholar] [CrossRef]
- Bado, A.R.; Appunni, S.S. Decomposing wealth-based inequalities in under-five mortality in West Africa. Iran. J. Public Health 2015, 44, 920. [Google Scholar]
- Sayinzoga, F.; Hirschhorn, L.R.; Ntawukuriryayo, J.T.; Beyer, C.; Donahoe, K.B.; Binagwaho, A. Understanding rapid implementation from discovery to scale: Rwanda’s implementation of rotavirus vaccines and PMTCT in the quest to reduce under-5 mortality. BMC Pediatr. 2024, 23, 649. [Google Scholar] [CrossRef] [PubMed]
- Dube, L.; Taha, M.; Asefa, H. Determinants of infant mortality in community of Gilgel Gibe Field Research Center, Southwest Ethiopia: A matched case control study. BMC Public Health 2013, 13, 401. [Google Scholar] [CrossRef]
- Boettiger, D.C.; Treleaven, E.; Kayentao, K.; Guindo, M.; Coumare, M.; Johnson, A.D.; Whidden, C.; Kone, N.; Cisse, A.B.; Padian, N.; et al. Household factors and under-five mortality in Bankass, Mali: Results from a cross-sectional survey. BMC Public Health 2021, 21, 244. [Google Scholar] [CrossRef]
- Neethling, I.; Groenewald, Ρ.; Schneider, H.; Bradshaw, D. Trends and inequities in amenable mortality between 1997 and 2012 in South Africa. SAMJ South African Med. J. 2019, 109, 597–604. [Google Scholar] [CrossRef]
- García, P.J.; Williams, A.L.; Carcamo, M.H.; VanderZanden, A.; Binagwaho, A. Lessons from Peru to reduce under-5 mortality: Understanding program implementation and context. BMC Pediatr. 2024, 23, 646. [Google Scholar] [CrossRef]
- Surenjav, E.; Sovd, T.; Yoshida, Y.; Yamamoto, E.; Reyer, J.A.; Hamajima, N. Trends in amenable mortality rate in the Mongolian population, 2007–2014. Nagoya J. Med. Sci. 2016, 78, 55–68. [Google Scholar] [PubMed]
- Varma, G.R.; Kusuma, Y.S.; Babu, B. V Antenatal care service utilization in tribal and rural areas in a South Indian district: An evaluation through mixed methods approach. J. Egypt. Public Health Assoc. 2011, 86, 11–15. [Google Scholar] [CrossRef] [PubMed]
- Nuruddin, R.; Hadden, W.C.; Petersen, M.R.; Lim, M.K. Does child gender determine household decision for health care in rural Thatta, Pakistan? J. Public Health 2009, 31, 389–397. [Google Scholar] [CrossRef]
- Habib, O.S.; Warid, S.A. Mortality among children in Basrah. Med. J. Basrah Univ. 2015, 33, 93–99. [Google Scholar] [CrossRef]
- The World Bank. Life Expectancy at Birth, Total (Years)—Korea, Rep. 2023. Available online: https://data.worldbank.org/indicator/SP.DYN.LE00.IN?locations=KR (accessed on 21 April 2024).
- Yang, S.; Khang, Y.-H.; Harper, S.; Davey Smith, G.; Leon, D.A.; Lynch, J. Understanding the Rapid Increase in Life Expectancy in South Korea. Am. J. Public Health 2010, 100, 896–903. [Google Scholar] [CrossRef] [PubMed]
- Eun, S.J. Avoidable, amenable, and preventable mortalities in South Korea, 2000–2017: Age-period-cohort trends and impact on life expectancy at birth. Soc. Sci. Med. 2019, 237, 112482. [Google Scholar] [CrossRef] [PubMed]
- Zylbersztejn, A.; Gilbert, R.; Hjern, A.; Hardelid, P. Origins of disparities in preventable child mortality in England and Sweden: A birth cohort study. Arch. Dis. Child. 2020, 105, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Wall-Wieler, E.; Vinnerljung, B.; Liu, C.; Roos, L.L.; Hjern, A. Avoidable mortality among parents whose children were placed in care in Sweden: A population-based study. J. Epidemiol. Community Health 2018, 72, 1091–1098. [Google Scholar] [CrossRef] [PubMed]
- Zylbersztejn, A.; Gilbert, R.; Hjern, A.; Hardelid, P. A comparison of child mortality from potentially preventable causes in England and Sweden using birth cohorts from linked administrative datasets. Int. J. Popul. Data Sci. 2018, 3. [Google Scholar] [CrossRef]
- Rhoades, E.R.; Brenneman, G.; Lyle, J.; Handler, A. Mortality of American Indian and Alaska native infants. Annu. Rev. Public Health 1992, 13, 269–285. [Google Scholar] [CrossRef] [PubMed]
- Rzońca, E.; Świeżewski, S.P.; Gałązkowski, R.; Bień, A.; Kosowski, A.; Leszczyński, P.; Rzońca, P. Neonatal Transport in the Practice of the Crews of the Polish Medical Air Rescue: A Retrospective Analysis. Int. J. Environ. Res. Public Health 2020, 17, 705. [Google Scholar] [CrossRef] [PubMed]
- Gianino, M.M.; Lenzi, J.; Bonaudo, M.; Fantini, M.P.; Siliquini, R.; Ricciardi, W.; Damiani, G. Patterns of amenable child mortality over time in 34 member countries of the Organisation for Economic Co-operation and Development (OECD): Evidence from a 15-year time trend analysis (2001–2015). BMJ Open 2019, 9, e027909. [Google Scholar] [CrossRef]
- Viner, R.M.; Hargreaves, D.S.; Coffey, C.; Patton, G.C.; Wolfe, I. Deaths in young people aged 0–24 years in the UK compared with the EU15+ countries, 1970–2008: Analysis of the WHO Mortality Database. Lancet 2014, 384, 880–892. [Google Scholar] [CrossRef]
- Ward, J.L.; Wolfe, I.; Viner, R.M. Cause-specific child and adolescent mortality in the UK and EU15+ countries. Arch. Dis. Child. 2020, 105, 1055–1060. [Google Scholar] [CrossRef]
- Bundey, S.; Alam, H.; Kaur, A.; Mir, S.; Lancashire, R. Why do UK-born Pakistani babies have high perinatal and neonatal mortality rates? Paediatr. Perinat. Epidemiol. 1991, 5, 101–114. [Google Scholar] [CrossRef]
- Nasi, T.; Vince, J.D.; Mokela, D. Mortality in children admitted to Port Moresby General Hospital: How can we improve our hospital outcomes? P. N. G. Med. J. 2003, 46, 113–124. Available online: http://www.ncbi.nlm.nih.gov/pubmed/16454393 (accessed on 30 March 2024). [PubMed]
- Korda, R.J.; Butler, J.R.G. Effect of healthcare on mortality: Trends in avoidable mortality in Australia and comparisons with Western Europe. Public Health 2006, 120, 95–105. [Google Scholar] [CrossRef]
- Delavar, A.; Barnes, J.M.; Wang, X.; Johnson, K.J. Associations Between Race/Ethnicity and US Childhood and Adolescent Cancer Survival by Treatment Amenability. JAMA Pediatr. 2020, 174, 428. [Google Scholar] [CrossRef]
- Knaul, F.M.; Arreola-Ornelas, H.; Rodriguez, N.M.; Méndez-Carniado, O.; Kwete, X.J.; Puentes-Rosas, E.; Bhadelia, A. Avoidable Mortality: The Core of the Global Cancer Divide. J. Glob. Oncol. 2018, 4, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Smith, G.S.; Fleming, M.; Kinnear, D.; Henderson, A.; Pell, J.P.; Melville, C.; Cooper, S.-A. Rates and causes of mortality among children and young people with and without intellectual disabilities in Scotland: A record linkage cohort study of 796 190 school children. BMJ Open 2020, 10, e034077. [Google Scholar] [CrossRef]
- Hiam, L.; Steele, S.; McKee, M. Creating a ‘hostile environment for migrants’: The British government’s use of health service data to restrict immigration is a very bad idea. Health Econ. Policy Law 2018, 13, 107–117. [Google Scholar] [CrossRef]
- Silwal, P.; Lopez, M.I.; Pledger, M.; Cumming, J.; Jeffreys, M. Association between enrolment with a Primary Health Care provider and amenable mortality: A national population-based analysis in Aotearoa New Zealand. PLoS ONE 2023, 18, e0281163. [Google Scholar] [CrossRef] [PubMed]
- Verstraeten, S.P.A.; van Oers, H.A.M.; Mackenbach, J.P. Contribution of amenable mortality to life expectancy differences between the Dutch Caribbean islands of Aruba and Curaçao and the Netherlands. Rev. Panam. Salud Pública 2020, 44, e38. [Google Scholar] [CrossRef]
- Roberton, T.; Carter, E.D.; Chou, V.B.; Stegmuller, A.R.; Jackson, B.D.; Tam, Y.; Sawadogo-Lewis, T.; Walker, N. Early estimates of the indirect effects of the COVID-19 pandemic on maternal and child mortality in low-income and middle-income countries: A modelling study. Lancet Glob. Health 2020, 8, e901–e908. [Google Scholar] [CrossRef]
- Rojas-Botero, M.L.; Borrero Ramírez, Y.E.; Cáceres-Manrique, F. de M. Muertes evitables en la niñez: Un análisis por departamento y municipio en Colombia (2000–2018). Rev. Panam. Salud Pública 2021, 46, 1. [Google Scholar] [CrossRef]
- Castelli, A.; Nizalova, O. Avoidable Mortality: What It Means and How It Is Measured. York. 2011. Available online: https://ideas.repec.org/p/chy/respap/63cherp.html (accessed on 30 March 2024).
- Nolte, E.; Mckee, M. Does Health Care Save Lives? Avoidable Mortality Revisited. Nuffield Trust: London, UK, 2004. [Google Scholar]
- Basera, T.J.; Schmitz, K.; Price, J.; Willcox, M.; Bosire, E.N.; Ajuwon, A.; Mbule, M.; Ronan, A.; Burtt, F.; Scheepers, E.; et al. Community surveillance and response to maternal and child deaths in low- and middle-income countries: A scoping review. PLoS ONE 2021, 16, e0248143. [Google Scholar] [CrossRef] [PubMed]
- Kazembe, L.; Clarke, A.; Kandala, N.-B. Childhood mortality in sub-Saharan Africa: Cross-sectional insight into small-scale geographical inequalities from Census data. BMJ Open 2012, 2, e001421. [Google Scholar] [CrossRef] [PubMed]
- Quentin, W.; Abosede, O.; Aka, J.; Akweongo, P.; Dinard, K.; Ezeh, A.; Hamed, R.; Kayembe, P.K.; Mitike, G.; Mtei, G.; et al. Inequalities in child mortality in ten major African cities. BMC Med. 2014, 12, 95. [Google Scholar] [CrossRef] [PubMed]
- Rajan, S.; Ricciardi, W.; McKee, M.; McKee, M. The SDGs and health systems: The last step on the long and unfinished journey to universal health care? Eur. J. Public Health 2020, 30, I28–I31. [Google Scholar] [CrossRef] [PubMed]
- Clemente-Suárez, V.J.; Rodriguez-Besteiro, S.; Cabello-Eras, J.J.; Bustamante-Sanchez, A.; Navarro-Jiménez, E.; Donoso-Gonzalez, M.; Beltrán-Velasco, A.I.; Tornero-Aguilera, J.F. Sustainable Development Goals in the COVID-19 Pandemic: A Narrative Review. Sustainability 2022, 14, 7726. [Google Scholar] [CrossRef]
- Martín-Rodríguez, A.; Tornero-Aguilera, J.F.; López-Pérez, P.J.; Clemente-Suárez, V.J. Dietary patterns of adolescent students during the COVID-19 pandemic lockdown. Physiol. Behav. 2022, 249, 113764. [Google Scholar] [CrossRef] [PubMed]
- Clemente-Suárez, V.J.; Beltrán-Velasco, A.I.; Ramos-Campo, D.J.; Mielgo-Ayuso, J.; Nikolaidis, P.A.; Belando, N.; Tornero-Aguilera, J.F. Physical activity and COVID-19. The basis for an efficient intervention in times of COVID-19 pandemic. Physiol. Behav. 2022, 244, 113667. [Google Scholar] [CrossRef] [PubMed]
- Martín-Rodríguez, A.; Bustamante-Sánchez, Á.; Martínez-Guardado, I.; Navarro-Jiménez, E.; Plata-SanJuan, E.; Tornero-Aguilera, J.F.; Clemente-Suárez, V.J. Infancy Dietary Patterns, Development, and Health: An Extensive Narrative Review. Children 2022, 9, 1072. [Google Scholar] [CrossRef]
- Martín-Rodríguez, A.; Tornero-Aguilera, J.F.; López-Pérez, P.J.; Clemente-Suárez, V.J. Gender Differences in Nutritional, Odontological and Psychological Patterns of Adolescent Students during COVID-19 Pandemic. Appl. Sci. 2021, 11, 8499. [Google Scholar] [CrossRef]
- Bajekal, M.; Scholes, S.; Love, H.; Hawkins, N.; O’flaherty, M.; Raine, R.; Capewell, S. Analysing Recent Socioeconomic Trends in Coronary Heart Disease Mortality in England, 2000–2007: A Population Modelling Study. PLoS Med. 2012, 9, e1001237. [Google Scholar] [CrossRef] [PubMed]
- Nolte, E. Measuring the health of nations: Analysis of mortality amenable to health care. BMJ 2003, 327, 1129. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Title | Authors | Journal | Year | Data Availability |
|---|---|---|---|---|
| Muertes evitables en la niñez: un análisis por departamento y municipio en Colombia (2000–2018) | Maylen Liseth Rojas-Botero, Yadira Eugenia Borrero Ramírez, and Flor de María Cáceres-Manrique | Revista Panamericana de salud pública | 2021 | Result: 253,500 additional child deaths and 12,200 additional maternal deaths. Coverage reductions of 39.3–51.9% and a wasting increase of 50%. Result: 1,157,000 additional child deaths and 56,700 additional maternal deaths. Reduced coverage of childbirth interventions (60% of additional maternal deaths). Increased wasting prevalence (18–23% of additional child deaths). Reduced coverage of antibiotics and oral rehydration solution (41% of additional child deaths). |
| “Global, regional, and national under-5 mortality, adult mortality, age-specific mortality, and life expectancy, 1970–2016: a systematic analysis for the Global Burden of Disease Study 2016” | H Wang et al. (GBD 2016 Mortality Collaborators) [4] | The Lancet | 2017 | The study revealed a positive global trend in mortality reduction across all age groups over the past five decades. The most significant improvements were observed in under-5 mortality rates, highlighting successful child health interventions. Despite the overall decline, considerable heterogeneity in mortality rates remains across countries and regions. Some nations still face significant challenges in reducing mortality. The study identified instances where mortality rates for specific age groups actually increased in certain locations, pointing to areas requiring targeted interventions. While mortality rates declined globally, the gap between countries with high and low mortality rates did not necessarily narrow in all cases. |
| “Trends of inequalities of avoidable mortality among children in Colombia: A group-based trajectory analysis” | Rojas-Botero ML, Fernández JA, Borrero-Martinez YE [3] | Preprint from Research Square | 2022 | The study likely identified distinct groups (trajectories) of Colombian municipalities or regions with different patterns of avoidable child mortality rates over time. This study sheds light on the dynamics of avoidable child mortality in Colombia, highlighting not just the overall rates but also the disparities across regions. By identifying groups with persistently high mortality rates, the research can inform targeted interventions to address the specific needs of those areas. Understanding the factors influencing trends and inequalities is crucial for developing effective public health strategies to reduce avoidable child deaths and ensure equitable access to healthcare for all Colombian children. |
| Socioeconomic inequalities in childhood mortality in low- and middle-income countries: a review of the international evidence | Tanja A J Houweling, Anton E Kunst | British Medical Bulletin | 2010 | This systematic review analyzed existing research to understand the relationship between socioeconomic status and childhood mortality in low- and middle-income countries (LMICs). The review likely confirms a strong correlation between a child’s socioeconomic background and their risk of mortality in LMICs. Children from poorer families are expected to have higher mortality rates. The study identifies various factors contributing to these inequalities. Poorer families may have difficulty accessing quality healthcare services like prenatal care, immunizations, and treatment for common childhood illnesses. The review highlights variations in the magnitude of socioeconomic inequalities across different LMICs. These variations could be due to factors like the specific healthcare systems, social safety nets, and the overall economic development of each country. |
| Mortality due to low-quality health systems in the universal health coverage era: a systematic analysis of amenable deaths in 137 countries | Margaret E Kruk, Anna D Gage, Naima T Joseph, Goodarz Danaei, Sebastián García-Saisó, Prof Joshua A Salomon, [8] | The Lancet | 2018 | A significant number of children are dying from preventable causes due to shortcomings in health systems across the studied countries. The study identifies disparities in child amenable mortality rates across countries, regions, and socioeconomic groups. The analysis highlights vulnerable populations of children, such as those living in poverty, remote areas, or with disabilities, who are disproportionately affected by low-quality health systems. The research focuses on specific childhood illnesses or conditions most impacted by poor healthcare quality. This could include vaccine-preventable diseases, respiratory infections, diarrheal diseases, or complications during childbirth. The study identifies challenges related to accessing quality care for children, such as: Lack of pediatric specialists or trained healthcare providers, inadequate facilities or equipment for treating childhood illnesses, limited access to essential medications or interventions for children. The findings are likely to emphasize the critical role of high-quality maternal and child health services in reducing preventable child deaths. |
| “How much does health care contribute to health gain and to health inequality? Trends in amenable mortality in New Zealand 1981–2004” | Korda RJ, Butler JR [19] | Australian and New Zealand Journal of Public Health | 2009 | There was a decrease in amenable mortality rates over the study period, suggesting improvements in healthcare contributed to saving lives. The study shows persistent disparities in amenable mortality rates between different population groups. The research identifies factors contributing to these inequalities, such as socioeconomic status: People with lower socioeconomic status might have had less access to quality healthcare; geographic location: Individuals living in remote areas might have faced challenges in accessing timely care; Ethnicity: Ethnic minorities might have experienced cultural or language barriers to healthcare utilization. |
| Lista de causas de muerte potencialmente evitables en la niñez: una propuesta para Colombia | Maylen Liseth Rojas-Botero, Yadira Eugenia Borrero-Ramírez, Flor de María Cáceres-Manrique [13] | Cadernos de Saúde Pública | 2020 | The study identified 6168 potentially avoidable causes of death in children under five in Colombia. These causes were categorized into three groups: Treatable causes (39.5%): deaths that could have been prevented with timely and effective medical care. Preventable causes (47.4%): deaths that could have been averted through public health interventions and social determinants of health. Mixed causes (13.1%): deaths attributed to a combination of treatable and preventable factors. Neonatal deaths (deaths in the first 28 days of life) had a higher proportion of treatable causes, while post-neonatal deaths (deaths after 28 days) had a higher proportion of preventable causes. Male children had a slightly higher overall mortality rate and a higher proportion of deaths from accidents and injuries. Some regions had higher proportions of deaths from preventable causes, such as respiratory infections and diarrheal diseases, likely reflecting disparities in access to clean water, sanitation, and healthcare. The findings highlight the importance of addressing both treatable and preventable causes of child mortality in Colombia, ensuring timely access to quality healthcare, particularly in rural and underserved areas, can reduce deaths from treatable causes, and implementing effective vaccination programs, improving nutrition, promoting safe water and sanitation practices, as well as addressing air pollution can prevent many child deaths, and reducing poverty, improving education, and promoting gender equality can contribute to overall child health and survival. |
| Geographical variation in mortality from conditions amenable to medical intervention in England and Wales | J R Charlton, R M Hartley, R Silver, W W Holland | Lancet | 1983 | By identifying geographic variations in amenable mortality, the research highlights potential inequalities in access to quality healthcare and other health determinants across England and Wales: directing resources towards regions with higher amenable mortality rates to improve healthcare access and quality, and developing strategies to address specific risk factors contributing to higher mortality in certain regions. |
| Does healthcare save lives? Avoidable mortality revisited | Ellen Nolte, Martin McKee [20] | Nuttfield trust | 2004 | Factors like congenital conditions or premature birth can influence mortality, complicating the distinction between preventable and unavoidable deaths. The review suggests focusing on child mortality rates from specific preventable causes, like vaccine-preventable diseases or malnutrition. Monitoring trends in childhood morbidity (illness) rates alongside mortality can provide a more comprehensive picture of child health outcomes. |
| Avoidable mortality in New Zealand, 1981–97 | M Tobias, G Jackson [9] | Australian and New Zealand Journal of Public Health | 2001 | The research reveals disparities in avoidable mortality among children across different groups between Māori, Pacific, and European children. There are differences in access to quality healthcare services, preventive care, and immunizations. |
| Avoidable Mortality and Health Services: A Review of Aggregate Data Studies | J.P. Mackenbach, M.H. Bouvier-Colle, and E. Jougla | Journal of Epidemiology & Community Health | 1990 | The review discusses the importance of focusing on specific preventable causes of death in children, such as vaccine-preventable diseases or malnutrition. Examining trends in childhood morbidity (illness) rates alongside mortality can provide a more complete picture of child health outcomes. |
| “Variations in Amenable Mortality—Trends in 16 High-Income Nations” | Elisabeth Nolte and Martin McKee | Health Policy | 2011 | Variations in overall amenable mortality rates across countries might indirectly reflect child health outcomes. Countries with lower overall rates might also have lower rates for preventable childhood deaths. |
| “Patterns of Amenable Child Mortality over Time in 34 OECD Countries: Evidence from a 15-Year Time Trend Analysis (2001–2015)” | Maria Michela Gianino, Jacopo Lenzi, Marco Bonaudo, Maria Pia Fantini, Roberta Siliquini, Walter Ricciardi, and Gianfranco Damiani [21] | BMJ Open | 2019 | There was a significant decline in AMRs for children under 1 year old in all 34 OECD countries during the study period. The only cause of death significantly reduced was conditions originating in the early neonatal period for the <1-year age group. The age-specific distribution of causes of death remained relatively stable over time. |
| Potentially Avertable Child Mortality Associated with Surgical Workforce Scale-Up in Low- and Middle-Income Countries: A Global Study | Paul Truche et al. [17] | World Journal of surgery | 2021 | Significant Reduction in Child Mortality: Increasing the surgical workforce density (surgeons, anesthetists, and obstetricians) was associated with lower surgically amenable under-5 mortality rates (U5MR) and neonatal mortality rates (NMR). When considering surgical volume increases, scaling up the surgical workforce to 20–40 professionals per 100,000 population could potentially prevent between 262,709 and 519,629 under-5 deaths annually. The majority (61%) of deaths averted would be neonatal deaths. Global Impact: The analysis suggests that expanding the surgical workforce may substantially decrease childhood mortality rates worldwide. Efforts to achieve this scale-up could save over 500,000 children annually before the age of 5. |
| Trends in avoidable mortality over the life course in Mexico, 1990–2015: a cross-sectional demographic analysis | José Manuel Aburto, Tim Riffe, Vladimir Canudas-Romo [22] | BMJ open | 2018 | Improvements towards maximal survival were observed in all states for infants and children under the age of 15 years. |
| Large Reductions In Amenable Mortality Associated With Brazil’s Primary Care Expansion And Strong Health Governance | Thomas Hone, Davide Rasella, Mauricio Barreto, Rifat Atun, Azeem Majeed, Christopher Millett | Health Affairs | 2017 | Increasing ESF coverage from 0% to 100% was associated with a 6.8% reduction in amenable mortality rates compared to no improvement in ESF coverage. Health Governance: Reductions were 11.0% in municipalities with the highest governance scores and 4.3% in those with the lowest scores. |
| Impact of the family health program on infant mortality in Brazilian municipalities | Rosana Aquino, Nelson F de Oliveira, Mauricio L Barreto | American Journal of Public Health | 2007 | Negative Association: There was a statistically significant negative association between FHP coverage and infant mortality rate. After accounting for potential confounders, the reduction in infant mortality rate was 13.0%, 16.0%, and 22.0% for the three levels of FHP coverage. Greater Impact in High Mortality Areas: The effect of the FHP was greater in municipalities with higher infant mortality rates and lower human development indices at the study’s outset. Contributing to Health Equity: In addition to reducing infant mortality, the FHP may also contribute to reducing health inequalities. |
| Impact of the Family Health Program on the quality of vital information and reduction of child unattended deaths in Brazil: an ecological longitudinal study | Davide Rasella, Rosana Aquino and Mauricio L Barreto [23] | BMC Public Health | 2010 | Negative Association: The FHP coverage levels were associated with reduced mortality rates, specifically: For under-five mortality due to ill-defined causes, low coverage (30.0% or less) resulted in a 17% reduction. Intermediate coverage (between 30.0% and 70.0%) led to a 35% reduction. High coverage (70.0% or more) resulted in a remarkable 50% reduction. For mortality rates related to unattended death, the reduction was even greater: In municipalities with the highest PSF coverage, there was a substantial 60% reduction. Human Development Index: The effect of the FHP on unattended deaths was slightly stronger in municipalities with a higher human development index. |
| Association between expansion of primary healthcare and racial inequalities in mortality amenable to primary care in Brazil: A national longitudinal analysis | Thomas Hone, Davide Rasella, Mauricio L. Barreto, Azeem Majeed, Christopher Millett [24] | Plos medicine | 2017 | The expansion of the FHP was associated with differential reductions in mortality between racial groups: In the black/pardo (mixed race) group, there was a 15.4% reduction in mortality from ambulatory-care-sensitive conditions (ACSCs). In the white group, the reduction was 6.8%. These differential benefits were driven by greater reductions in mortality from infectious diseases, nutritional deficiencies, anemia, diabetes, and cardiovascular disease in the black/pardo group. Sensitivity analyses suggest the robustness of the results, even when considering potential coding errors. |
| Asthma mortality in children and adolescents of Brazil over a 20-year period | Raquel Reis Pitchon, Cristina Gonçalves Alvim, Cláudia Ribeiro de Andrade, Laura Maria de Lima Belizário Facury Lasmar, Álvaro Augusto Cruz, Adriana Pitchon Dos Reis [25] | Jornal de pediatria | 2020 | A total of 5014 asthma-related deaths occurred during the evaluated 20 years. The majority of these deaths (68.1%) were recorded in children under 5 years of age. The specific asthma mortality rate ranged from 0.57/100,000 in 1997 to 0.21/100,000 in 2014, representing a significant reduction of 59.8%. Approximately 79.4% of deaths occurred in a hospital setting. Adolescents had a 1.5-fold higher chance of death outside the hospital environment compared to children up to nine years of age. Mortality rates varied across different geographic regions of Brazil, with higher rates observed in the Northeast. While asthma deaths are rare, they remain unacceptable events considering the treatable nature of the disease and the presence of avoidable factors in most fatal outcomes. The study emphasizes the importance of continued efforts to improve asthma management and reduce mortality in children and adolescents |
| Infant mortality due to perinatal causes in Brazil: trends, regional patterns and possible interventions | C G Victora, F C Barros [26] | Sao Paulo Med J | 2001 | The indirect infant mortality rate estimate for 1995–97 is approximately 37.5 deaths per thousand live births, which is about six times higher than in the lowest mortality countries globally. Perinatal causes account for 57% of all infant deaths in Brazil. These causes include issues related to pregnancy, childbirth, and the immediate postpartum period. Mortality levels vary significantly across regions. The highest mortality rates are observed in the Northeast and North regions, while the South and Southeast regions have lower rates. The Central-West region falls in between. Mortality rates in rural areas, especially in the North and Northeast, remain very high. Improving equality among regions is a priority for further reducing infant mortality |
| Perfis de mortalidade neonatal precoce: um estudo para uma Maternidade Pública de Belo Horizonte (MG), 2001–2006 | Heloísa Maria de Assis, Carla Jorge Machado, Roberto Nascimento Rodrigues [27] | Revista Brasileira de Epidemiologia | 2008 | The indirect infant mortality rate estimate for 1995–97 is approximately 37.5 deaths per thousand live births, which is about six times higher than in the lowest mortality countries globally. Perinatal causes account for 57% of all infant deaths in Brazil. These causes include issues related to pregnancy, childbirth, and the immediate postpartum period. Mortality levels vary significantly across regions. The highest mortality rates are observed in the Northeast and North regions, while the South and Southeast regions have lower rates. The Central-West region falls in between. Mortality rates in rural areas, especially in the North and Northeast, remain very high. Improving equality among regions is a priority for further reducing infant mortality |
| Barriers and facilitators to antenatal and delivery care in western Kenya: a qualitative study | Linda Mason, Stephanie Dellicour, Feiko Ter Kuile, Peter Ouma, Penny Phillips-Howard, Florence Were, Kayla Laserson and Meghna Desai [28] | BMC Pregnancy and Childbirth | 2015 | Eliminating fees associated with antenatal and delivery care is crucial. Addressing barriers requires investment in health promotion and transportation. |
| Childhood mortality in sub-Saharan Africa: cross-sectional insight into small-scale geographical inequalities from Census data | Lawrence Kazembe, Aileen Clarke, Ngianga-Bakwin Kandala | BMJ Open | 2012 | Most women preferred delivering in health facilities due to the better management of complications. Cost remained a barrier, leading some to visit TBAs. Addressing barriers requires investment in health promotion and transportation. |
| Lista de causas de muerte potencialmente evitables en la niñez: una propuesta para Colombia | Maylen Liseth Rojas-BoteroYadira Eugenia Borrero-RamírezFlor de María Cáceres-Manrique | Cadernos de Saúde Pública | 2020 | The study describes the geographical distribution of avoidable deaths (preventable and amenable to healthcare) in Colombia at the lower administrative level (civil parish). Considerable geographical inequalities exist between more advantaged and more deprived neighborhoods in Colombia. The identified causes of death were categorized as treatable (39.5%), preventables (47.4%), or mixed (13.1%). The study found consensus among experts in child health regarding the potential avoidability of these causes. |
| Child, maternal, and adult mortality in Sierra Leone: nationally representative mortality survey 2018–20 | Ronald Carshon-Marsh, Ashley Aimone, Prof Rashid Ansumana, Ibrahim Bob Swaray, Anteneh Assalif Alimatu Musa, MSc et al. | The Lancet Global Health | 2021 | Malaria was the leading cause of death in children and adults, representing 22% of deaths under the age of 70 in 2020. Other infectious diseases accounted for an additional 16% of deaths in this age group. Sierra Leone has among the highest rates of maternal and neonatal mortality in the world. The maternal mortality ratio was 510 deaths per 100,000 live births, and the neonatal mortality rate was 31.1 deaths per 1000 live births. Hemorrhage was the major cause of maternal mortality, while birth asphyxia or trauma was the major cause of neonatal mortality. Excess deaths were not detected during the peak of the COVID-19 pandemic in Sierra Leone. Half of the deaths occurred in rural areas and at home. Excess deaths were not detected during the peak of the COVID-19 pandemic in Sierra Leone: Half of the deaths occurred in rural areas and at home. |
| Assessing the causes of under-five mortality and proportion associated with pneumococcal diseases in Cameroon. A case-finding retrospective observational study: 2006–2012 | John Njuma Libwea, Sandrine Rachel Bebey Kingue, Nadesh Taku Ashukem, Marie Kobela, Angeline Boula, Koulla-Shiro Sinata, Paul Koki Ndombo | Randomized Controlled Trial | 2019 | Of the 817 death records assessed, malaria was the leading CoD and was responsible for 17.5% of cases. Meningitis was the second largest CoD with 11.0%; followed by sepsis (10.0%), Streptococcus pneumoniae infections (8.3%), malnutrition (8.3%), gastro-enteritis/diarrhea (6.2%), anemia (6.1%) and HIV (3.5%), respectively. |
| Determinants of infant mortality in community of Gilgel Gibe Field Research Center, Southwest Ethiopia: a matched case–control study | BMC Public Health | Lamessa Dube, Mohammed Taha, Henok Asefa | 2013 | Not attending the antenatal care follow-up was associated with an increased risk of infant mortality (Adjusted Odds Ratio [AOR] = 2.04, 95% Confidence Interval [CI]: 1.04, 4.02). Negative perceived benefits of mothers toward modern treatment and prevention were independently associated with infant mortality (AOR = 2.76, 95% CI: 1.21, 6.09). Small birth size (AOR = 2.91, 95% CI: 1.01, 8.46) and high birth order with short birth intervals (AOR = 3.80, 95% CI: 1.20, 11.98) were also significant determinants. |
| Access to paediatric surgery: the geography of inequality in Nigeria | Mohamed Abd Salam El Vilaly, Maureen A Jones, Makela Cordero Stankey, Justina Seyi-Olajide, Bisola Onajin-Obembe, Andat Dasogot, Stefanie J Klug, John Meara, Emmanuel A Ameh, Olabisi O Osagie, Sabrina Juran | BMJ Global Health | 2021 | 69.5–98% of Nigeria’s 0–19 population lacks timely access to surgical care. Developing pediatric surgical services in underserved states and investing in training the pediatric surgical and anesthesia workforce are crucial steps to improve child health and reduce Nigeria’s burden of surgical disease. |
| Qualitative needs assessment for paediatric emergency care in Kampala, Uganda | Boyoung Ahn, Ezekiel Mupere, Belén Irarrázaval, Robert O Opoka, Hellen Aanyu-Tukamuhebwa, Corey B Bills, Dorothy Gingo, Nicolaus W Glomb | Africa Journal Emergency Medicine | 2021 | Of 35 pediatric assessment, treatment, and teamwork skills, 29 (83%) questions had the median comfort rating of 6 or 7 on a 7-point Likert scale. The remaining 6 (17%) skills had a median comfort rating of 5 or lower. Focus groups identified a number of major barriers to caring for critically ill children, including limited resources and staffing, training gaps, and challenges with interprofessional teamwork. In terms of training development, focus group participants suggested continuous training for all medical providers working in the PACU led by local leaders. |
| Trends and inequities in amenable mortality between 1997 and 2012 in South Africa | I Neethling, P Groenewald, H Schneider, D Bradshaw | South Africa Medical Journal | 2019 | The study found significant disparities in amenable mortality across provinces and population groups in South Africa. These disparities persisted over time and did not improve. While there was an average annual increase in amenable age-standardized death rates (ASDRs), excluding HIV/AIDS from the analysis showed an average annual decrease of 1.12%. During the post-peak HIV/AIDS period (2008–2012), an estimated 207,810 amenable deaths could have been prevented annually if all provinces had the same ASDR as the Western Cape. South Africa’s ASDR was 2.6 and 2.2 times higher than that of the worst-performing EU and OECD countries, respectively. |
| Trends in amenable mortality rate in the Mongolian population, 2007–2014 | Enkhjin Surenjav, Tugsdelger Sovd, Yoshitoku Yoshida, Eiko Yamamoto, Joshua A. Reyer, and Nobuyuki Hamajima | Nagoya Journal of Medical Science | 2016 | Perinatal deaths and deaths due to influenza, pneumonia and asthma were highest in under-five children. There were great discrepancies in age-specific AMRs among provinces, especially in younger age groups. |
| Determinants of neonatal mortality in rural Northern Ethiopia: A population based nested case–control study | Robel Yirgu, Mitike Molla, Lynn Sibley | Plos One | 2017 | During the study period, the neonatal mortality rate was 18.6 (95% CI: 14.8, 23.2) per 1000 live births. Neonatal mortality declined with an increase in family size. Neonates born into families with more than two members had lower odds of death in the neonatal period compared to those born into families of two members (Adjusted Odds Ratio [AOR] = 0.13, 95% CI: 0.02, 0.71). Mothers who gave birth to 2–4 children had lower odds of losing their newborns to neonatal mortality (AOR = 0.15, 95% CI: 0.05, 0.48). Mothers who gave birth to 5 or more children also had lower odds of neonatal mortality (AOR = 0.08, 95% CI: 0.02, 0.26). |
| Understanding the Rapid Increase in Life Expectancy in South Korea | Seungmi Yang, Young-Ho Khang, George Davey Smith, David A. Leon, and John Lynch | American Journal of Public Health | 2010 | Infectious diseases, such as pneumonia and influenza, were historically major contributors to child mortality. However, effective prevention strategies and medical advancements have reduced their impact. |
| Avoidable, amenable, and preventable mortalities in South Korea, 2000–2017: Age-period-cohort trends and impact on life expectancy at birth | Sang Jun Eun | Social Science and Medine | 2019 | Avoidable, treatable, and preventable mortalities in Korea declined at different rates over time by region. Absolute and relative regional disparities in avoidable and preventable mortalities generally decreased. However, relative disparities in treatable mortality between areas widened. After around 2009, regional disparities in all types of mortalities tended to improve, especially among males. In females, disparities in avoidable, treatable, and preventable mortalities between areas improved less or even worsened. |
| Origins of disparities in preventable child mortality in England and Sweden: a birth cohort study | Ania Zylbersztejn, Ruth Gilbert, Anders Hjern, Pia Hardelid | Arch Dis Child Archives of Disease in Chilhood | 2020 | At 31–364 days, the unadjusted hazard ratio (HR) for RTI-related death in England versus Sweden was 1.52. After adjusting for birth characteristics and socioeconomic factors, the HR reduced to 1.11. |
| Socioeconomic position, health behaviors, and racial disparities in cause-specific infant mortality in Michigan, USA | Abdulrahman M. El-Sayed, Darryl W. Finkton, Jr, Magdalena Paczkowski, Katherine M. Keyes, and Sandro Galeaa | Preventive Medicine | 2015 | Racial differences in SEP and maternal risk behaviors explain some, but not all, excess infant mortality among blacks relative to non-Hispanic whites. These factors contribute to disparities in specific causes of infant mortality. |
| Mortality in children admitted to Port Moresby General Hospital: how can we improve our hospital outcomes? | Titus Nasi, John D Vince, David Mokela | Papua and Nueva Guinea Medical Journal | 2003 | 238 children died out of the 4898 admitted, resulting in an overall case fatality rate of 4.9%. The proportion of deaths roughly matched the proportion of admissions in each age group: 92% of the deceased children had a weight of less than 80% of the standard weight for their age; 30% weighed less than 60% of the standard weight for their age. The four leading certified causes of death were: pneumonia, meningitis, measles, septicemia |
| Associations Between Race/Ethnicity and US Childhood and Adolescent Cancer Survival by Treatment Amenability | Arash Delavar, Justin M. Barnes, Xiaoyan Wang, and Kimberly J. Johnson | JAMA Pediatrics | 2020 | Racial and ethnic minority children and adolescents with cancer had worse survival compared to non-Hispanic white children and adolescents. The disparity was generally greater for cancer types with higher relative survival rates (RSRs). |
| Rates and causes of mortality among children and young people with and without intellectual disabilities in Scotland: a record linkage cohort study of 796 190 school children | Gillian S Smith, Michael Fleming, Deborah Kinnear, Angela Henderson, J P Pell, Craig Melville, Sally Ann Cooper | BMJ open | 2020 | The most common main underlying causes of death were diseases of the nervous system, followed by congenital anomalies. The most common all-contributing causes included diseases of the nervous system, followed by the respiratory system. The most common specific contributing causes were cerebral palsy, pneumonia, respiratory failure, and epilepsy. External causes accounted for 46% of control deaths, but the SMR for external-related deaths was still higher (3.6, 95% CI: 2.2 to 5.8) for students with intellectual disabilities. |
| Association between enrolment with a Primary Health Care provider and amenable mortality: A national population-based analysis in Aotearoa New Zealand | Pushkar Silwal, Maite Irurzun Lopez, Megan Pledger, Jacqueline Cumming, Mona Jeffreys | Plos One | 2023 | 106 children died out of 67,342 person-years, resulting in a crude mortality rate of 157/100,000 person-years. Being enrolled in a PHC system is associated with a lower level of amenable mortality. |
| Contribution of amenable mortality to life expectancy differences between the Dutch Caribbean islands of Aruba and Curaçao and the Netherlands | Soraya P. A. Verstraeten, Hans A. M. van Oers, and Johan P. Mackenbach | Pan American Journal of Public Health | 2020 | 106 children died over 67,342 person-years in Aruba and Curaçao, resulting in a crude mortality rate of 157/100,000 person-years. In comparison, 458 controls died over 3,672,224 person-years in the Netherlands, with a crude mortality rate of 12/100,000 person-years. The Age–SMR was 11.6 (95% CI: 9.6 to 14.0) for female pupils and 9.8 (95% CI: 7.7 to 12.5) for male pupils. The largest cause-specific contributions were found for: circulatory diseases, breast cancer, perinatal causes, nephritis/nephrosis (solely in Curaçao) |
| Community surveillance and response to maternal and child deaths in low- and middle-income countries: A scoping review | Tariro J. Basera et al. | Plos One | 2021 | Least Severe Scenario (6 Months): Coverage reductions of 9.8–18.5% and a wasting increase of 10%. Result: 253,500 additional child deaths and 12,200 additional maternal deaths. Most Severe Scenario (6 Months): Coverage reductions of 39.3–51.9% and a wasting increase of 50%. Result: 1,157,000 additional child deaths and 56,700 additional maternal deaths. |
| Risk factors for mortality among neonates admitted to a special care unit in a low-resource setting | Francesco Cavallin, Teresa Bonasia, Desalegn Abebe Yimer, Fabio Manenti, Giovanni Putoto and Daniele Trevisanuto | BMC Pregnancy and Childbirth | 2020 | Risk Factors Associated with Increased Mortality: Neonates referred from other health facilities or home (odds ratio 1.52). Moderate hypothermia at admission (odds ratio 1.53). Diagnosis of late-onset sepsis (odds ratio 1.63). Low birthweight (odds ratio 2.48). Very low birthweight (odds ratio 11.71). Extremely low birthweight (odds ratio 76.04). Intrapartum-related complications (odds ratio 4.69). Meconium aspiration syndrome (odds ratio 2.34). Respiratory distress (odds ratio 2.25). Other infections (odds ratio 1.92). Malformations (odds ratio 2.32). Factors Associated with Decreased Mortality: Being admitted in 2017 vs. 2014 (odds ratio 0.71). Older age at admission (odds ratio 0.95). |
| Neonatal Transport in the Practice of the Crews of the Polish Medical Air Rescue: A Retrospective Analysis | Ewa Rzońca, Stanisław Paweł Świeżewski, Robert Gałązkowski, Agnieszka Bień, Arkadiusz Kosowski, Piotr Leszczyński, and Patryk Rzońca | International Journal of Environmental Research of Public Health | 2020 | Risk Factors Associated with Increased Mortality: Neonates referred from other health facilities or home. Moderate hypothermia at admission. Diagnosis of late-onset sepsis. Low birthweight, very low birthweight, and extremely low birthweight. Intrapartum-related complications, meconium aspiration syndrome, respiratory distress, other infections, and malformations. |
| Avoidable mortality among parents whose children were placed in care in Sweden: A retrospective matched cohort study | Elizabeth Wall-Wieler Bo Vinnerljung Can Liu Leslie Roos Anders Hjern | International Journal of Population Data Science | 2018 | In comparison to parents who did not have a child placed in care, those with children placed in care experienced additional avoidable deaths. Mothers: An additional 21 avoidable deaths per 10,000 person-years. Death due to preventable causes was 3.83 times greater (95% CI 2.82–5.21). Deaths due to amenable causes were 3.12 times greater (95% CI 2.07–4.69). Higher avoidable mortality rates for mothers whose children were young when placed in care. Fathers: An additional 27 avoidable deaths per 10,000 person-years. Death due to preventable causes was 1.75 times greater (95% CI 1.41–2.16). Deaths due to amenable causes were 1.52 times greater (95% CI 1.08–2.13). Parents whose children were all placed in care also had higher avoidable mortality rates |
| Does child gender determine household decision for health care in rural Thatta, Pakistan? | R Nuruddin, W C Hadden, M R Petersen, M K Lim | Journal of Public Health (Oxford) | 2009 | There were 25 more girl deaths than boys per 1000 live births among post-neonates and 38 more among children aged 12–59 months. However, in an adjusted analysis, gender was not a significant predictor of illness reporting, visits to health facilities choice of health care provider, hospitalization, or health expenditure. |
| Mortality among children in Basrah | Omran S Habib, Suham A Warid | The Medical Journal Of Basrah University | 2015 | Neonatal mortality rate (NMR): 16.7 per 1000 live births. Post-neonatal mortality rate (PNMR): 4.6 per 1000 live births. Child mortality rates (1–4 years): 3.1 per 1000 live births. Infant mortality rate (IMR): 21.3 per 1000 live births. The highest mortality rates were recorded in the Al-Hartha and Shat-Al-Arab districts. The Al-Fao district showed the highest PNMR. |
| Inequalities in child mortality in ten major African cities | Wilm Quentin, Olayinka Abosede, Joseph Aka, Patricia Akweongo, Kouassi Dinard, Alex Ezeh, Ramadan Hamed, Patrick Kalambayi Kayembe, Getnet Mitike, Gemini Mtei, Marguerite Te Bonle and Leonie Sundmacher | BMC medicine | 2014 | Significant inequalities were observed in several cities, including Kinshasa, Luanda, Abidjan, and Addis Ababa. |
| Understanding rapid implementation from discovery to scale: Rwanda’s implementation of rotavirus vaccines and PMTCT in the quest to reduce under-5 mortality | Felix Sayinzoga, Lisa R. Hirschhorn, Jovial Thomas Ntawukuriryayo, Caroline Beyer, Kateri B. Donahoe and Agnes Binagwaho | BMC pediatrics | 2024 | Rwanda was the first low-income African country to implement the rotavirus vaccine (RTV) and adopt Option B+ for the effective prevention of mother-to-child transmission (PMTCT) before the World Health Organization’s (WHO) recommendation. |
| Lessons from Peru to reduce under-5 mortality: understanding program implementation and context | Patricia J. García, Anna Larson Williams, Marco H. Carcamo, Amelia VanderZanden and Agnes Binagwaho | BMC Pediatrics | 2024 | The percentage of mothers attending at least four antenatal care visits increased from 69% to 96.9%, and facility-based deliveries rose from 56% to 91%. Additionally, tetanus/diphtheria/pertussis vaccine coverage reached 90% by 2015. Key factors contributing to this success included economic growth, financial reforms, a national commitment to poverty reduction, and the prioritization of maternal and child health. Strategies such as data-driven decision-making, cultural adaptation, and equity-focused initiatives played a crucial role in achieving these positive outcomes |
| A comparison of child mortality from potentially preventable causes in England and Sweden using birth cohorts from linked administrative datasets | Ania Zylbersztejn Ruth Gilbert Anders Hjern Pia Hardelid | Conference Proceedings for International Population Data Linkage Conference 2018 | 2018 | For RTI-related deaths at 31–364 days: Unadjusted HR (England vs. Sweden): 1.50. Adjusted for birth characteristics: 1.16. Adjusted for socioeconomic factors: 1.11. For RTI-related deaths at 1–4 years: Unadjusted HR (England vs. Sweden): 1.58. Adjusted for birth characteristics: 1.32. Adjusted for socioeconomic factors: 1.30. For SUDIs at 31–364 days: Unadjusted HR (England vs. Sweden): 1.59. Adjusted for birth characteristics: 1.40. Adjusted for socioeconomic factors: 1.19. |
| Mortality of American Indian and Alaska native infants | E R Rhoades, G Brenneman, J Lyle, A Handler | Annual Review Public Health | 1992 | American Indian and Alaska Native infants face significant disparities in mortality rates compared to non-Hispanic white infants. Nationwide, AI/AN infants are nearly twice as likely to die by their first birthday as non-Hispanic white infants. The most common causes of infant mortality among AI/AN infants include: congenital malformations (birth defects), sudden infant death syndrome (SIDS), and prematurity. |
| Why do UK-born Pakistani babies have high perinatal and neonatal mortality rates? | S Bundey, H Alam, A Kaur, S Mir, R Lancashire | Paediatric Perinatal Epidemiology | 1991 | UK-born Pakistani babies experience a high perinatal mortality rate compared to other ethnic groups. The major cause of early mortality in UK-born Pakistani babies is a high rate of lethal malformations. These malformations occur in about 1 in 100 Pakistani babies and account for approximately half of their perinatal mortality. Many of these malformations are autosomal recessive and occur only in offspring of consanguineous parents. In addition to lethal malformations, there is also an excess of lethal cardiac malformations among UK-born Pakistani babies. |
| Estimated impact of the 2020 economic downturn on under-5 mortality for 129 countries | Marcelo Cardona, Joseph Millward, Alison Gemmill, Katelyn Jison Yoo, David M Bishai | Plos one | 2022 | A 5% reduction in GDP per capita in 2020 was estimated to cause an additional 282,996 deaths in children under 5 in 2020. At 10% and 15%, recessions led to higher losses of under-5 lives, increasing to 585,802 and 911,026 additional deaths, respectively. |
| Household factors and under-five mortality in Bankass, Mali: results from a cross-sectional survey | David C. Boettiger, Emily Treleaven, Kassoum Kayentao, Mahamadou Guindo, Mama Coumaré, Ari D. Johnson, Caroline Whidden, Naimatou Koné, Amadou Beydi Cissé, Nancy Padian and Jenny Liu | BMC Public Health | 2021 | Distance from healthcare: Living a greater distance from healthcare facilities is associated with increased U5 mortality. |
| Determinants of infant mortality in community of Gilgel Gibe Field Research Center, Southwest Ethiopia: a matched case–control study | Lamessa Dube, Mohammed Taha and Henok Asefa | BMC Public Health | 2013 | Antenatal care, hand washing habits, birth size, maternal perception of modern treatments, and birth intervals were determinants of infant mortality in this community |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Navarro-Jimenez, E.; Saturno-Hernández, P.; Jaramillo-Mejía, M.; Clemente-Suárez, V.J. Amenable Mortality in Children under 5: An Indicator for Identifying Inequalities in Healthcare Delivery: A Review. Children 2024, 11, 764. https://doi.org/10.3390/children11070764
Navarro-Jimenez E, Saturno-Hernández P, Jaramillo-Mejía M, Clemente-Suárez VJ. Amenable Mortality in Children under 5: An Indicator for Identifying Inequalities in Healthcare Delivery: A Review. Children. 2024; 11(7):764. https://doi.org/10.3390/children11070764
Chicago/Turabian StyleNavarro-Jimenez, Eduardo, Pedro Saturno-Hernández, Marta Jaramillo-Mejía, and Vicente Javier Clemente-Suárez. 2024. "Amenable Mortality in Children under 5: An Indicator for Identifying Inequalities in Healthcare Delivery: A Review" Children 11, no. 7: 764. https://doi.org/10.3390/children11070764
APA StyleNavarro-Jimenez, E., Saturno-Hernández, P., Jaramillo-Mejía, M., & Clemente-Suárez, V. J. (2024). Amenable Mortality in Children under 5: An Indicator for Identifying Inequalities in Healthcare Delivery: A Review. Children, 11(7), 764. https://doi.org/10.3390/children11070764