
COVID-19 Pediatric Follow-Up: Respiratory Long COVID-Associated Comorbidities and Lung Ultrasound Alterations in a Cohort of Italian Children


 , ,
, ,  ,
, 
Abstract

1. Introduction
COVID-19 and Atopic Diseases in Children
2. Materials and Methods
2.1. Assessment Tools
- a.
- Medical Questionnaire: Our initial step involved collecting data on the acute disease caused by SARS-CoV-2 by filling out a questionnaire provided to parents. This encompassed confirming SARS-CoV-2 diagnosis and recovery through nasopharyngeal swabs, documenting symptomatology (asymptomatic, cough, fever, anosmia, ageusia, muscular pains, etc.), duration of illness (less than or greater than 15 days), administered treatments (i.e., paracetamol, corticosteroids, non-steroidal anti-inflammatory drugs, oxygen supplementation, etc.), and the necessity of hospitalization. Additionally, we gathered information about the patient’s demographic and medical history concerning known allergic and respiratory conditions and previous allergic sensibilizations confirmed by validated tests (skin prick test, IgE specific count).
- b.
- Physical examination and BMI assessment: We visited the children, collected data from their respiratory physical examinations and recorded their weight and height to calculate their BMI. As per the Expert Committee Recommendations, being underweight is defined as having a BMI below the 5th percentile, while overweight is categorized between the 85th and less than the 95th percentile. Obesity is characterized by a BMI at or exceeding the 95th percentile for children and teenagers [46].
- c.
- Baseline spirometry and after bronchodilation test: Spirometry plays an important role in evaluating pulmonary health and detecting early signs of respiratory disorders in children. Spirometry provides a comprehensive analysis of lung function parameters, including forced vital capacity (FVC), forced expiratory volume in one second (FEV1), FEV1/FVC ratio, and forced expiratory flow between 25% and 75% (FEF 25–75%) of FVC. These measures aid in diagnosing various respiratory conditions including conditions like asthma and restrictive lung disorders in pediatric patients [47]. In our study, spirometry was used to measure FVC, FEV1, FEF 25–75%, and the FEV1/FVC ratio in patients aged 6 years old or younger if capable of performing it. Spirometry was performed according to ERS consensus guidelines [48]. An FEV1 < 80% and FVC < 80% of predicted values were considered abnormal, while FEF 25–75% values were considered abnormal when they were <70% of those predicted. A rise in FEV1 of ≥12% and/or ≥200 mL after inhaling 400 µg of a short-acting β2-agonist (salbutamol) was considered a significant bronchodilator response [49].
- d.
- Six-minute walking test: the six-minute walking test is a simple, practical test used to measure the functional exercise capacity. During the examination, participants are directed to walk for the maximum distance achievable within six minutes along a long, flat, straight, enclosed corridor [50,51,52]. In our study, for technical reasons, this test was performed on a treadmill. The goal for the patients was to walk at their own pace in six minutes. They could rest at any time during the test. During the test, heart rate (HR) and oxygen saturation (SpO2) were continuously monitored, using a finger pulse oximeter. The onset of symptoms such as dyspnea and cough has also been documented.
- e.
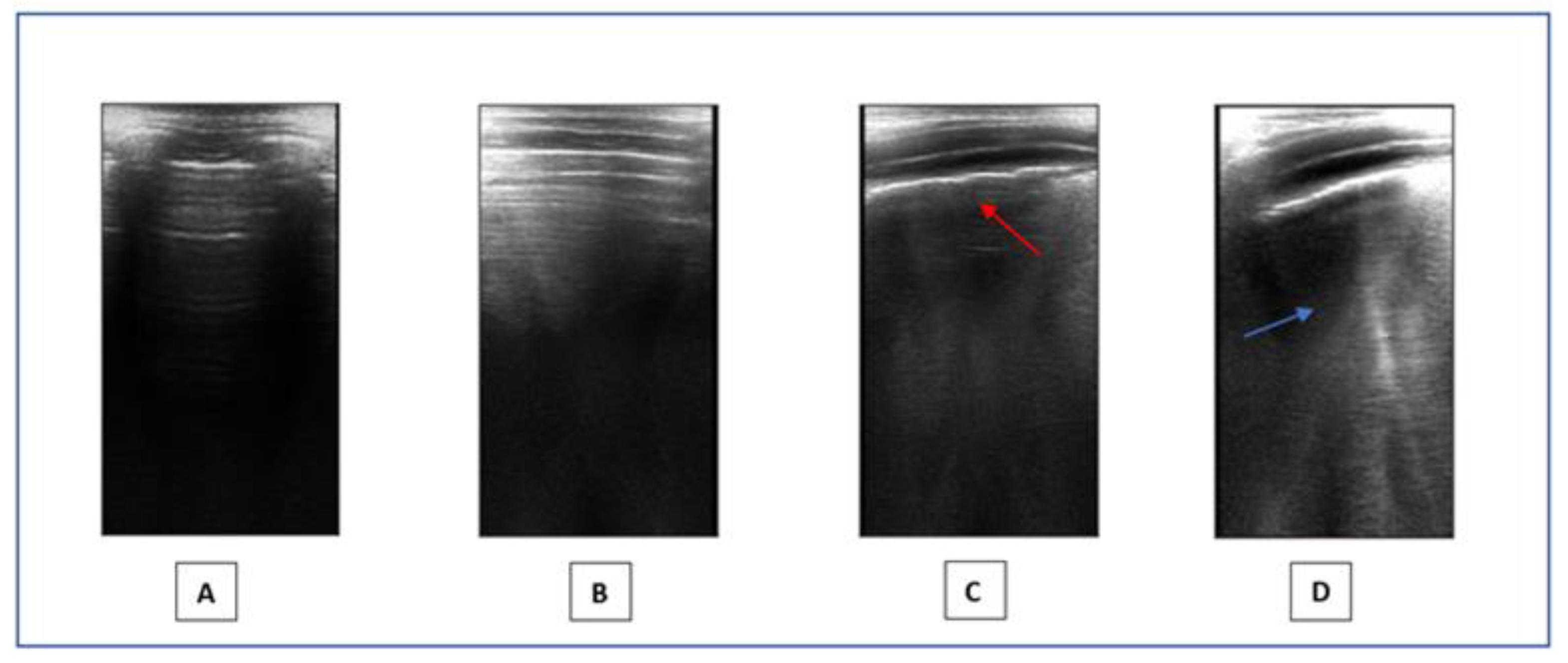
- Lung ultrasound: LUS is a non-invasive method that provides a real-time image of lung structures, enabling doctors to identify early alterations in lung function. The radiation-free approach and portability of ultrasound make it an attractive choice in children, helping to limit exposure to X-rays. LUS has gradually expanded its use to encompass various pediatric applications, including all types of pneumonia, pulmonary embolism, and typical chest and lung diseases in childhood [53]. Lung semiotics consists of artifacts originating from the air/tissue interface and authentic images, like effusions and consolidations [54]. Non-pathological ultrasound images exhibit A-lines and a consistently thin pleural line. Conversely, abnormal images are identified by the observation of three or more B-lines between two ribs in a single scan with the disappearance of A-lines, indicating subpleural interstitial edema, up to a ‘white lung’ picture, consolidations, an irregular or thickened pleural line, and pleural effusion (Figure 1). LUS is a very effective and sensible method for assessing the presence of small pleural effusion. Furthermore, in the diagnosis of childhood pneumonia, lung ultrasound (LUS) is considered as an imaging alternative to computed tomography (CT) scans, as LUS findings demonstrate a significant correlation with those observed in chest CT scans [55]. Nonspecific abnormalities, such as the presence of multiple bilateral B-lines, indicating a reduction in air content, thickening of the pleural line with associated abnormalities, and peripheral consolidation, may be observed on the LUS scans of children with COVID-19 pneumonia [56]. Since the early stages of the pandemic, LUS has demonstrated to be a helpful tool to assess lung conditions, monitor any changes over time, and guide therapeutic decisions in both adults and children [57,58,59,60,61]. The LUS in this study was conducted using a linear probe. We adhered to a standardized approach regarding acquisition protocol, as previously outlined by Volpicelli et al. [62]. We examined a total of 12 thoracic areas: 2 anterior, 2 lateral, and 2 posterior areas on each side. Based on the severity of the findings, a numerical score between 0 and 3 was assigned: 0 = normal; 1 = irregular pleural line with less than three B-lines between two ribs in a single scan; 2 = irregularities of the pleural line with more than three B-lines between two ribs in a single scan; 3 = areas of consolidations or ‘white lung’. Each LUS was performed by the same doctor, Dr. A.K., who is a pediatrician and a certified expert operator in pediatric lung ultrasound.
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Umano, G.R.; Rondinelli, G.; Rivetti, G.; Klain, A.; Aiello, F.; del Giudice, M.M.; Decimo, F.; Papparella, A.; del Giudice, E.M. Effect of COVID-19 Lockdown on Children’s Eating Behaviours: A Longitudinal Study. Children 2022, 9, 1078. [Google Scholar] [CrossRef]
- Cui, X.; Zhao, Z.; Zhang, T.; Guo, W.; Guo, W.; Zheng, J.; Zhang, J.; Dong, C.; Na, R.; Zheng, L.; et al. A systematic review and meta-analysis of children with coronavirus disease 2019 (COVID-19). J. Med. Virol. 2021, 93, 1057–1069. [Google Scholar] [CrossRef] [PubMed]
- Manti, S.; Licari, A.; Montagna, L.; Votto, M.; Leonardi, S.; Brambilla, I.; Castagnoli, R.; Foiadelli, T.; Marseglia, G.L.; Cardinale, F.; et al. SARS-CoV-2 infection in pediatric population. Acta Biomed. 2020, 91, e2020003. [Google Scholar] [CrossRef]
- Chiappini, E.; Licari, A.; Motisi, M.A.; Manti, S.; Marseglia, G.L.; Galli, L.; Lionetti, P. Gastrointestinal involvement in children with SARS-COV-2 infection: An overview for the pediatrician. Pediatr. Allergy Immunol. 2020, 31 (Suppl. S26), 92–95. [Google Scholar] [CrossRef]
- Parisi, G.F.; Brindisi, G.; Indolfi, C.; Diaferio, L.; Marchese, G.; Ghiglioni, D.G.; Zicari, A.M.; del Giudice, M.M. Upper airway involvement in pediatric COVID-19. Pediatr. Allergy Immunol. 2020, 31 (Suppl. S26), 85–88. [Google Scholar] [CrossRef]
- Parisi, G.F.; Brindisi, G.; Indolfi, C.; Diaferio, L.; Marchese, G.; Ghiglioni, D.G.; Zicari, A.M.; Del Giudice, M.M. COVID-19, anosmia, and ageusia in atopic children. Pediatr. Allergy Immunol. 2022, 33 (Suppl. S27), 99–101. [Google Scholar] [CrossRef]
- Brindisi, G.; Spalice, A.; Anania, C.; Bonci, F.; Gori, A.; Capponi, M.; Cinicola, B.; De Castro, G.; Martinelli, I.; Pulvirenti, F.; et al. COVID-19, Anosmia, and Allergies: Is There a Relationship? A Pediatric Perspective. J. Clin. Med. 2022, 11, 5019. [Google Scholar] [CrossRef] [PubMed]
- Sorg, A.-L.; Hufnagel, M.; Doenhardt, M.; Diffloth, N.; Schroten, H.; von Kries, R.; Berner, R.; Armann, J. Risk for severe outcomes of COVID-19 and PIMS-TS in children with SARS-CoV-2 infection in Germany. Eur. J. Pediatr. 2022, 181, 3635–3643. [Google Scholar] [CrossRef]
- Sorg, A.L.; Hufnagel, M.; Doenhardt, M.; Diffloth, N.; Schroten, H.; Kries, R.; Berner, R.; Armann, J. Risk of Hospitalization, severe disease, and mortality due to COVID-19 and PIMS-TS in children with SARS-CoV-2 infection in Germany. medRxiv 2021. [CrossRef]
- Borch, L.; Holm, M.; Knudsen, M.; Ellermann-Eriksen, S.; Hagstroem, S. Long COVID symptoms and duration in SARS-CoV-2 positive children—A nationwide cohort study. Eur. J. Pediatr. 2022, 181, 1597–1607. [Google Scholar] [CrossRef]
- Esposito, S.; Principi, N.; Azzari, C.; Cardinale, F.; Di Mauro, G.; Galli, L.; Gattinara, G.C.; Fainardi, V.; Guarino, A.; Lancella, L.; et al. Italian intersociety consensus on management of long covid in children. Ital. J. Pediatr. 2022, 48, 42. [Google Scholar] [CrossRef]
- Gupta, M.; Gupta, N.; Esang, M. Long COVID in Children and Adolescents. Prim Care Companion CNS Disord. 2022, 24, 21r03218. [Google Scholar] [CrossRef]
- del Giudice, M.M.; Klain, A.; Dinardo, G.; D’addio, E.; Bencivenga, C.L.; Fontanella, C.; Decimo, F.; Umano, G.R.; Siciliano, M.; Carotenuto, M.; et al. Behavioral and Sleep Disorders in Children and Adolescents following COVID-19 Disease: A Case-Control Study. Children 2023, 10, 1189. [Google Scholar] [CrossRef]
- Osmanov, I.M.; Spiridonova, E.; Bobkova, P.; Gamirova, A.; Shikhaleva, A.; Andreeva, M.; Blyuss, O.; El-Taravi, Y.; DunnGalvin, A.; Comberiati, P.; et al. Risk factors for post-COVID-19 condition in previously hospitalised children using the ISARIC Global follow-up protocol: A prospective cohort study. Eur. Respir. J. 2022, 59, 2101341. [Google Scholar] [CrossRef] [PubMed]
- Morello, R.; Mariani, F.; Mastrantoni, L.; De Rose, C.; Zampino, G.; Munblit, D.; Sigfrid, L.; Valentini, P.; Buonsenso, D. Risk factors for post-COVID-19 condition (Long Covid) in children: A prospective cohort study. EClinicalMedicine 2023, 59, 101961. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Leon, S.; Wegman-Ostrosky, T.; del Valle, N.C.A.; Perelman, C.; Sepulveda, R.; Rebolledo, P.A.; Cuapio, A.; Villapol, S. Long-COVID in children and adolescents: A systematic review and meta-analyses. Sci. Rep. 2022, 12, 9950. [Google Scholar] [CrossRef] [PubMed]
- Soriano, J.B.; Murthy, S.; Marshall, J.C.; Relan, P.; Diaz, J.V.; WHO Clinical Case Definition Working Group on Post-COVID-19 Condition. A clinical case definition of post-COVID-19 condition by a Delphi consensus. Lancet Infect. Dis. 2022, 22, e102–e107. [Google Scholar] [CrossRef] [PubMed]
- National Institute of Health. Long COVID Resources and Research about Long COVID. 2023. Available online: https://www.nhlbi.nih.gov/covid/long-covid#:~:text=Long%20COVID%2C%20long%2Dhaul%20COVID,than%20symptoms%20of%20COVID%2D19%20 (accessed on 12 December 2023).
- National Institute for Health and Care Excellence (NICE). COVID-19 Rapid Guideline: Managing the Long-Term Effects of COVID-19. 2023. Available online: https://www.nice.org.uk/guidance/ng188/resources/covid19-rapid-guideline-managing-the-longterm-effects-of-covid19-pdf-51035515742 (accessed on 12 December 2023).
- Esposito, S.; Deolmi, M.; Ramundo, G.; Puntoni, M.; Caminiti, C.; Principi, N. True prevalence of long COVID in children: A narrative review. Front. Microbiol. 2023, 14, 1225952. [Google Scholar] [CrossRef] [PubMed]
- De Filippo, M.; Votto, M.; Brambilla, I.; Castagnoli, R.; Montagna, L.; Caffarelli, C.; Cardinale, F.; Del Giudice, M.M.; Tosca, M.; Caimmi, S.; et al. Allergy and COVID-19. Acta Biomed. 2021, 92, e2021522. [Google Scholar] [CrossRef]
- Castro-Rodriguez, J.A.; Forno, E. Asthma and COVID-19 in children: A systematic review and call for data. Pediatr. Pulmonol. 2020, 55, 2412–2418. [Google Scholar] [CrossRef]
- Choi, J.H.; Choi, S.-H.; Yun, K.W. Risk Factors for Severe COVID-19 in Children: A Systematic Review and Meta-Analysis. J. Korean Med. Sci. 2022, 37, e35. [Google Scholar] [CrossRef] [PubMed]
- Tosca, M.A.; Licari, A.; Marseglia, G.L.; Ciprandi, G. COVID-19 in Italian children and adolescents: The role of allergy and asthma. Allergy Asthma Proc. 2021, 42, e101–e102. [Google Scholar] [CrossRef] [PubMed]
- Moeller, A.; Thanikkel, L.; Duijts, L.; Gaillard, E.A.; Garcia-Marcos, L.; Kantar, A.; Tabin, N.; Turner, S.; Zacharasiewicz, A.; Pijnenburg, M.W. COVID-19 in children with underlying chronic respiratory diseases: Survey results from 174 centres. ERJ Open Res. 2020, 6, 00409–02020. [Google Scholar] [CrossRef] [PubMed]
- Brindisi, G.; Zicari, A.M.; Parisi, G.F.; Diaferio, L.; Indolfi, C.; Marchese, G.; Ghiglioni, D.G.; Umano, G.R.; Klain, A.; Marseglia, G.L.; et al. Prevalence of COVID-19 in children affected by allergic rhinoconjunctivitis and asthma: Results from the second “SIAIP rhinosinusitis and conjunctivitis committee” survey. Ital. J. Pediatr. 2022, 48, 1–8. [Google Scholar] [CrossRef] [PubMed]
- A cura della Commissione Rinosinusite e Congiuntivite della SIAIP; Indolfi, C.; Diaferio, L.; Parisi, G.F.; Ghiglioni, D.; Brindisi, G.; Zicari, A.; Marchese, G.; del Giudice, M.M. Impatto del COVID-19 nei bambini in Italia: Risultati di una survey tra i pediatri italiani. Riv. Immunol. Allergol. Pediatr. 2021, 35, 17–20. [Google Scholar] [CrossRef]
- Arsenault, S.; Hoofman, J.; Poowuttikul, P.; Secord, E. Sustained decrease in pediatric asthma emergency visits during the first year of the COVID-19 pandemic. Allergy Asthma Proc. 2021, 42, 400–402. [Google Scholar] [CrossRef]
- Maheswari, S.; Pethannan, R.; Sabarimurugan, S. Air pollution enhances susceptibility to novel coronavirus (COVID-19) infection—An impact study. Environ. Anal. Health Toxicol. 2020, 35, e2020020. [Google Scholar] [CrossRef]
- Hamadneh, M.; Alquran, A.; Manna, R. Impact of the COVID-19 on asthma control among children: A systematic review. J. Public Health Res. 2023, 12, 22799036231197186. [Google Scholar] [CrossRef]
- Boechat, J.L.; Wandalsen, G.F.; Kuschnir, F.C.; Delgado, L. COVID-19 and pediatric asthma: Clinical and management challenges. Int. J. Environ. Res. Public Health 2021, 18, 1093. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.-J.; Dong, X.; Liu, G.-H.; Gao, Y.-D. Risk and Protective Factors for COVID-19 Morbidity, Severity, and Mortality. Clin. Rev. Allergy Immunol. 2023, 64, 90–107. [Google Scholar] [CrossRef] [PubMed]
- A Cura Della Commissione Asma Della, SIAIP; Licari, A.; Leone, M.; Di Cicco, M.E.; Bozzetto, S.; De Vittori, V.; Scavone, M.; Amato, D.; Capristo, C.; di Mauro, D.; et al. COVID-19: Asma e allergia proteggono dalle forme gravi? Raccomandazioni per la gestione dell’asma in tempo di COVID-19. Riv. Di Immunol. E Allergol. Pediatr. 2020, 34 (Suppl. S1), 17–19. [Google Scholar]
- Venturini, E.; Montagnani, C.; Garazzino, S.; DonÀ, D.; Pierantoni, L.; Vecchio, A.L.; Krzysztofiak, A.; Nicolini, G.; Bianchini, S.; Galli, L.; et al. Treatment of children with COVID-19: Update of the Italian Society of Pediatric Infectious Diseases position paper. Ital. J. Pediatr. 2021, 47, 199. [Google Scholar] [CrossRef] [PubMed]
- Yao, Y.; Wang, H.; Liu, Z. Expression of ACE2 in airways: Implication for COVID-19 risk and disease management in patients with chronic inflammatory respiratory diseases. Clin. Exp. Allergy 2020, 50, 1313–1324. [Google Scholar] [CrossRef] [PubMed]
- Perlini, S.; Ciprandi, G.; Castagnoli, R.; Licari, A.; Marseglia, G.L. Eosinopenia could be a relevant prognostic biomarker in patients with coronavirus disease 2019. Allergy Asthma Proc. 2020, 41, e80–e82. [Google Scholar] [CrossRef]
- Marseglia, G.L.; Chiappini, E.; Brambilla, I.; Licari, A.; Tosca, M.A.; Ciprandi, G. COVID-19 in Italy: The Point of View of the Italian Society of Pediatric Allergy and Immunology-COVID-19 Commission. Pediatr. Allergy Immunol. Pulmonol. 2020, 33, 121–123. [Google Scholar] [CrossRef]
- Zhang, J.J.; Dong, X.; Cao, Y.Y.; Yuan, Y.D.; Yang, Y.B.; Yan, Y.Q.; Akdis, C.A.; Gao, Y.D. Clinical characteristics of 140 patients infected with SARS-CoV-2 in Wuhan, China. Allergy 2020, 75, 1730–1741. [Google Scholar] [CrossRef] [PubMed]
- Lindsley, A.W.; Schwartz, J.T.; Rothenberg, M.E. Eosinophil responses during COVID-19 infections and coronavirus vaccination. J. Allergy Clin. Immunol. 2020, 146, 1–7. [Google Scholar] [CrossRef]
- Pazukhina, E.; Andreeva, M.; Spiridonova, E.; Bobkova, P.; Shikhaleva, A.; El-Taravi, Y.; Rumyantsev, M.; Gamirova, A.; Bairashevskaia, A.; Petrova, P.; et al. Prevalence and risk factors of post-COVID-19 condition in adults and children at 6 and 12 months after hospital discharge: A prospective, cohort study in Moscow (StopCOVID). BMC Med. 2022, 20, 244. [Google Scholar] [CrossRef]
- Körner, R.W.; Bansemir, O.Y.; Franke, R.; Sturm, J.; Dafsari, H.S. Atopy and Elevation of IgE, IgG3, and IgG4 May Be Risk Factors for Post COVID-19 Condition in Children and Adolescents. Children 2023, 10, 1598. [Google Scholar] [CrossRef]
- Zhang, H.; Sun, Y.; Wang, Y.; Yazici, D.; Azkur, D.; Ogulur, I.; Azkur, A.K.; Yang, Z.; Chen, X.; Zhang, A.; et al. Recent developments in the immunopathology of COVID-19. Allergy 2023, 78, 369–388. [Google Scholar] [CrossRef]
- Fernández-De-Las-Peñas, C.; Torres-Macho, J.; Velasco-Arribas, M.; Arias-Navalón, J.A.; Guijarro, C.; Hernández-Barrera, V.; Canto-Diez, M. Similar prevalence of long-term post-COVID symptoms in patients with asthma: A case-control study. J. Infect. 2021, 83, 237–279. [Google Scholar] [CrossRef]
- Zheng, Y.-B.; Zeng, N.; Yuan, K.; Tian, S.-S.; Yang, Y.-B.; Gao, N.; Chen, X.; Zhang, A.-Y.; Kondratiuk, A.L.; Shi, P.-P.; et al. Prevalence and risk factor for long COVID in children and adolescents: A meta-analysis and systematic review. J. Infect. Public Health 2023, 16, 660–672. [Google Scholar] [CrossRef]
- Available online: https://simri.it/simri/idPage/102/idNews/1290/Centri-SIMRI-per-follow-up-Covid-19-Conoscere-per-prevenire.html (accessed on 12 December 2023).
- Barlow, S.E.; Expert Committee. Expert committee recommendations regarding the prevention, assessment, and treatment of child and adolescent overweight and obesity: Summary report. Pediatrics 2007, 120 (Suppl. S4), S164–S192. [Google Scholar] [CrossRef]
- Jat, K.R. Spirometry in children. Prim. Care Respir. J. 2013, 22, 221–229. [Google Scholar] [CrossRef] [PubMed]
- Bhakta, N.R.; McGowan, A.; Ramsey, K.A.; Borg, B.; Kivastik, J.; Knight, S.L.; Sylvester, K.; Burgos, F.; Swenson, E.R.; McCarthy, K.; et al. European Respiratory Society/American Thoracic Society technical statement: Standardisation of the measurement of lung volumes, 2023 update. Eur. Respir. J. 2023, 62, 2201519. [Google Scholar] [CrossRef] [PubMed]
- Öztürk, G.K.; Beken, B.; Doğan, S.; Akar, H.H. Pulmonary function tests in the follow-up of children with COVID-19. Eur. J. Pediatr. 2022, 181, 2839–2847. [Google Scholar] [CrossRef]
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [CrossRef]
- Singh, S.J.; Puhan, M.A.; Andrianopoulos, V. An official systematic review of the European Respiratory Society/American Thoracic Society: Measurement properties of field walking tests in chronic respiratory disease. Eur. Respir. J. 2014, 44, 1447–1478. [Google Scholar] [CrossRef] [PubMed]
- Holland, A.E.; Spruit, M.A.; Troosters, T. An official European Respiratory Society/American Thoracic Society technical standard: Field walking tests in chronic respiratory disease. Eur. Respir. J. 2014, 44, 1428–1446. [Google Scholar] [CrossRef]
- Dietrich, C.F.; Buda, N.; Ciuca, I.M.; Dong, Y.; Fang, C.; Feldkamp, A.; Jüngert, J.; Kosiak, W.; Mentzel, H.J.; Pienar, C.; et al. Lung ultrasound in children, WFUMB review paper (part 2). Med. Ultrason. 2021, 23, 443–452. [Google Scholar] [CrossRef]
- Soldati, G.; Demi, M.; Smargiassi, A.; Inchingolo, R.; Demi, L. The role of ultrasound lung artifacts in the diagnosis of respiratory diseases. Expert Rev. Respir. Med. 2019, 13, 163–172. [Google Scholar] [CrossRef]
- Pereda, M.A.; Chavez, M.A.; Hooper-Miele, C.C.; Gilman, R.H.; Steinhoff, M.C.; Ellington, L.E.; Gross, M.M.; Price, C.; Tielsch, J.M.; Checkley, W. Lung ultrasound for the diagnosis of pneumonia in children: A meta-analysis. Pediatrics 2015, 135, 714–722. [Google Scholar] [CrossRef]
- Allinovi, M.; Parise, A.; Giacalone, M.; Amerio, A.; Delsante, M.; Odone, A.; Franci, A.; Gigliotti, F.; Amadasi, S.; Delmonte, D.; et al. Lung Ultrasound May Support Diagnosis and Monitoring of COVID-19 Pneumonia. Ultrasound Med. Biol. 2020, 46, 2908–2917. [Google Scholar] [CrossRef] [PubMed]
- Buonsenso, D.; Vetrugno, L. Lung Ultrasound in Adults and Children with COVID-19: From First Discoveries to Recent Advances. J. Clin. Med. 2022, 11, 4340. [Google Scholar] [CrossRef] [PubMed]
- Russo, G.; Flor, N.; Casella, F.; Ippolito, S.; Leidi, F.; Casazza, G.; Radovanovic, D.; Vezzulli, F.; Santus, P.; Cogliati, C. Lung ultrasound in the follow-up of severe COVID-19 pneumonia: Six months evaluation and comparison with CT. Intern. Emerg. Med. 2022, 17, 2261–2268. [Google Scholar] [CrossRef] [PubMed]
- Gaspardone, C.; Meloni, C.; Preda, A.; Romagnolo, D.; Brugliera, L.; Castellazzi, P.; Tettamanti, A.; Conte, C.; Secchi, A.; Maranta, F.; et al. Lung Ultrasound in COVID-19 A Role Beyond the Acute Phase? J. Ultrasound Med. 2021, 40, 503–511. [Google Scholar] [CrossRef]
- La Regina, D.P.; Pepino, D.; Nenna, R.; Iovine, E.; Mancino, E.; Andreoli, G.; Zicari, A.M.; Spalice, A.; Midulla, F.; On Behalf of The Long Covid Research Group. Pediatric COVID-19 Follow-Up with Lung Ultrasound: A Prospective Cohort Study. Diagnostics 2022, 12, 2202. [Google Scholar] [CrossRef]
- Buonsenso, D.; Morello, R.; Mariani, F.; De Rose, C.; Cortese, R.; Vetrugno, L.; Valentini, P. Role of Lung Ultrasound in the Follow-Up of Children with Previous SARS-CoV-2 Infection: A Case-Control Assessment of Children with Long COVID or Fully Recovered. J. Clin. Med. 2023, 12, 3342. [Google Scholar] [CrossRef]
- Volpicelli, G.; Elbarbary, M.; Blaivas, M.; Lichtenstein, D.A.; Mathis, G.; Kirkpatrick, A.W.; Melniker, L.; Gargani, L.; Noble, V.E.; Via, G.; et al. International evidence-based recommendations for point-of-care lung ultrasound. Intensive Care Med. 2012, 38, 577–591. [Google Scholar] [CrossRef]
- Brambilla, I.; Cave, F.D.; Guarracino, C.; De Filippo, M.; Votto, M.; Licari, A.; Pistone, C.; Tondina, E. Obesity and COVID-19 in children and adolescents: A double pandemic. Acta Biomed. 2022, 93, e2022195. [Google Scholar] [CrossRef]
- Kompaniyets, L.; Agathis, N.T.; Nelson, J.M.; Preston, L.E.; Ko, J.Y.; Belay, B.; Pennington, A.F.; Danielson, M.L.; DeSisto, C.L.; Chevinsky, J.R.; et al. Underlying Medical Conditions Associated With Severe COVID-19 Illness Among Children. JAMA Netw. Open 2021, 4, e2111182. [Google Scholar] [CrossRef]
- Arulanandam, B.; Beladi, H.; Chakrabarti, A. Obesity and COVID-19 mortality are correlated. Sci. Rep. 2023, 13, 5895. [Google Scholar] [CrossRef]
- Staatz, C.B.; Bann, D.; Ploubidis, G.B.; Goodman, A.; Silverwood, R.J. Age of First Overweight and Obesity, COVID-19 and Long COVID in Two British Birth Cohorts. J. Epidemiol. Glob. Health 2023, 13, 140–153. [Google Scholar] [CrossRef]
- Mancino, E.; Nenna, R.; Matera, L.; La Regina, D.P.; Petrarca, L.; Iovine, E.; Di Mattia, G.; Frassanito, A.; Conti, M.G.; Bonci, E.; et al. A Single Center Observational Study on Clinical Manifestations and Associated Factors of Pediatric Long COVID. Int. J. Environ. Res. Public Health 2023, 20, 6799. [Google Scholar] [CrossRef]
- Cantinotti, M.; Marchese, P.; Assanta, N.; Pizzuto, A.; Corana, G.; Santoro, G.; Franchi, E.; Viacava, C.; Eynde, J.V.D.; Kutty, S.; et al. Lung Ultrasound Findings in Healthy Children and in Those Who Had Recent, Not Severe COVID-19 Infection. J. Clin. Med. 2022, 11, 5999. [Google Scholar] [CrossRef]
- Gräger, S.; Pfirschke, R.; Lorenz, M.; Vilser, D.; Krämer, M.; Mentzel, H.-J.; Glutig, K. Lung ultrasound in children and adolescents with long-term effects of COVID-19: Initial results. Front. Pediatr. 2023, 11, 1112881. [Google Scholar] [CrossRef]
- Klain, A.; Indolfi, C.; Dinardo, G.; Contieri, M.; Decimo, F.; del Giudice, M.M. Pathological Lung Ultrasound May Take Time to Resolve Despite Respiratory Symptoms Improvement: A Pediatric Case Series Followed for Long COVID. Curr. Respir. Med. Rev. 2023, 19, 263–267. [Google Scholar] [CrossRef]
- Denina, M.; Pruccoli, G.; Scolfaro, C.; Mignone, F.; Zoppo, M.; Giraudo, I.; Silvestro, E.; Bertolotti, L.D.; Rosati, S.D.; Ramenghi, U.; et al. Sequelae of COVID-19 in Hospitalized Children: A 4-Months Follow-Up. Pediatr. Infect. Dis. J. 2020, 39, e458–e459. [Google Scholar] [CrossRef] [PubMed]
- Zubairi, A.B.S.; Shaikh, A.; Zubair, S.M.; Ali, A.S.; Awan, S.; Irfan, M. Persistence of post-COVID lung parenchymal abnormalities during the three-month follow-up. Adv. Respir. Med. 2021, 89, 477–483. [Google Scholar] [CrossRef] [PubMed]
- Dobrijević, D.; Antić, J.; Rakić, G.; Katanić, J.; Andrijević, L.; Pastor, K. Clinical Hematochemical Parameters in Differential Diagnosis between Pediatric SARS-CoV-2 and Influenza Virus Infection: An Automated Machine Learning Approach. Children 2023, 10, 761. [Google Scholar] [CrossRef] [PubMed]
- Dobrijević, D.; Vilotijević-Dautović, G.; Katanić, J.; Horvat, M.; Horvat, Z.; Pastor, K. Rapid Triage of Children with Suspected COVID-19 Using Laboratory-Based Machine-Learning Algorithms. Viruses 2023, 15, 1522. [Google Scholar] [CrossRef] [PubMed]
- Syeda, H.B.; Syed, M.; Sexton, K.W.; Syed, S.; Begum, S.; Syed, F.; Prior, F.; Yu, F., Jr. Role of Machine Learning Techniques to Tackle the COVID-19 Crisis: Systematic Review. JMIR Med. Inform. 2021, 9, e23811. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline Characteristics of the Population | |
|---|---|
| Male | 64.7% |
| Female | 35.3% |
| Mean age | 8.92 years |
| BMI: -<75° -75–85° ->85° | 41.6% 20.8% 37.6% |
| COVID-19 disease: -asymptomatic -fever -fever and respiratory symptoms -hospitalization with O2 supplementation | 17.6% 35.3% 46.1 1% |
| Duration of COVID-19: ->15 days -<15 days | 55.% 44.1% |
| Comorbidities: -allergic rhinitis, -46.1% asthma and -56.9% reported an allergic sensitization | 28.9% 46.1% 56.9% |
| Spirometry: -FEV1/FVC > 80% -FEV1/FVC < 80% | 98% 2% |
| Six-minute walking test: -Negative -Positive | 100% 0% |
| LUS score: -score 0 -score 1 -score 2 -score 3 | 73.3% 11.9% 14.9% 0% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Indolfi, C.; Klain, A.; Dinardo, G.; D’Addio, E.; Ferrara, S.; Decimo, F.; Ciprandi, G.; Tosca, M.A.; Miraglia del Giudice, M. COVID-19 Pediatric Follow-Up: Respiratory Long COVID-Associated Comorbidities and Lung Ultrasound Alterations in a Cohort of Italian Children. Children 2024, 11, 166. https://doi.org/10.3390/children11020166
Indolfi C, Klain A, Dinardo G, D’Addio E, Ferrara S, Decimo F, Ciprandi G, Tosca MA, Miraglia del Giudice M. COVID-19 Pediatric Follow-Up: Respiratory Long COVID-Associated Comorbidities and Lung Ultrasound Alterations in a Cohort of Italian Children. Children. 2024; 11(2):166. https://doi.org/10.3390/children11020166
Chicago/Turabian StyleIndolfi, Cristiana, Angela Klain, Giulio Dinardo, Elisabetta D’Addio, Serena Ferrara, Fabio Decimo, Giorgio Ciprandi, Maria Angela Tosca, and Michele Miraglia del Giudice. 2024. "COVID-19 Pediatric Follow-Up: Respiratory Long COVID-Associated Comorbidities and Lung Ultrasound Alterations in a Cohort of Italian Children" Children 11, no. 2: 166. https://doi.org/10.3390/children11020166
APA StyleIndolfi, C., Klain, A., Dinardo, G., D’Addio, E., Ferrara, S., Decimo, F., Ciprandi, G., Tosca, M. A., & Miraglia del Giudice, M. (2024). COVID-19 Pediatric Follow-Up: Respiratory Long COVID-Associated Comorbidities and Lung Ultrasound Alterations in a Cohort of Italian Children. Children, 11(2), 166. https://doi.org/10.3390/children11020166