Impact of Socioeconomic Inequalities on Dental Caries Status in Sardinian Children

 ,
,  , , ,
, , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
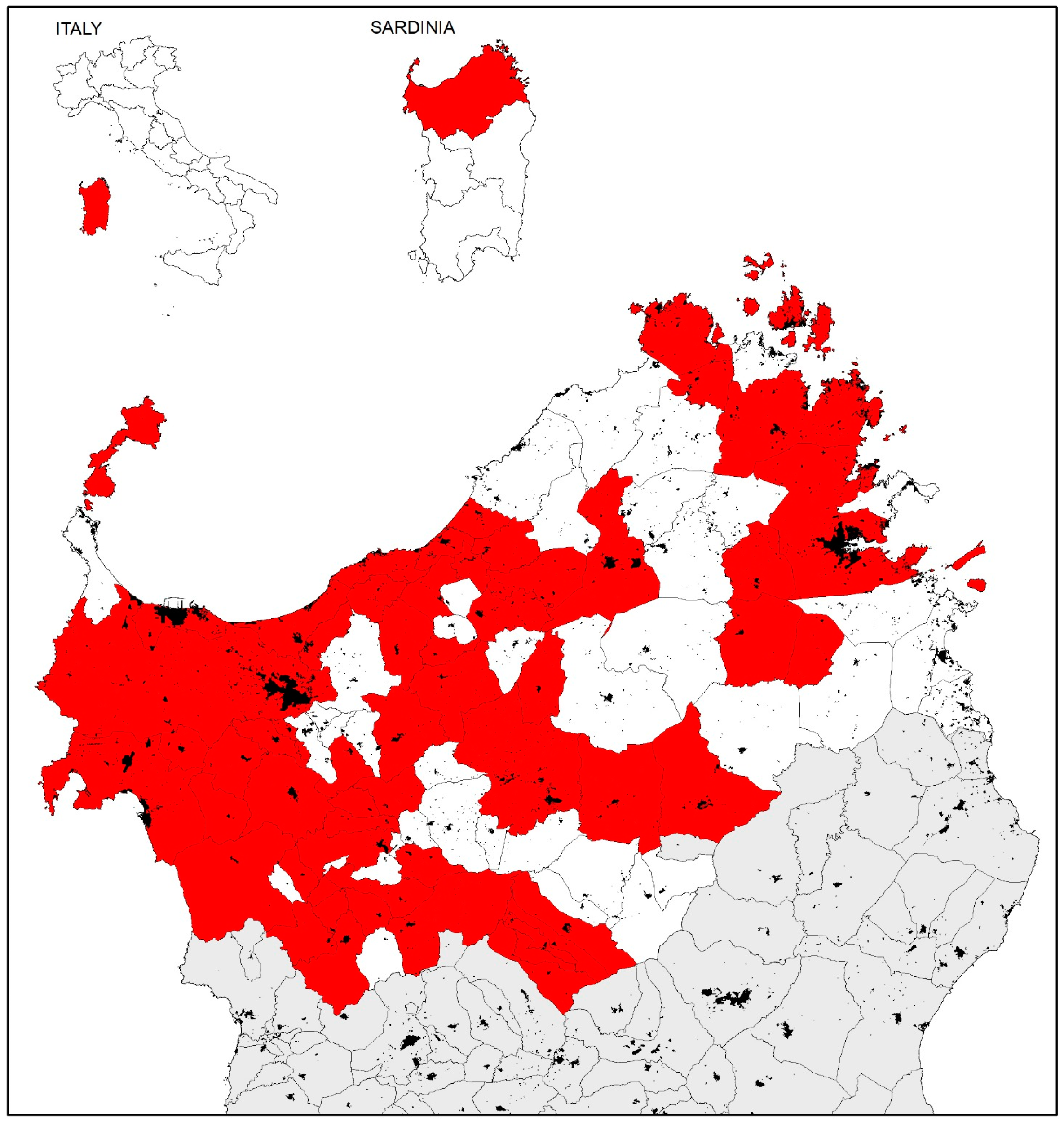
2.1. Study Setting
2.2. Study Design and Sample Size
2.3. Statistical Analysis
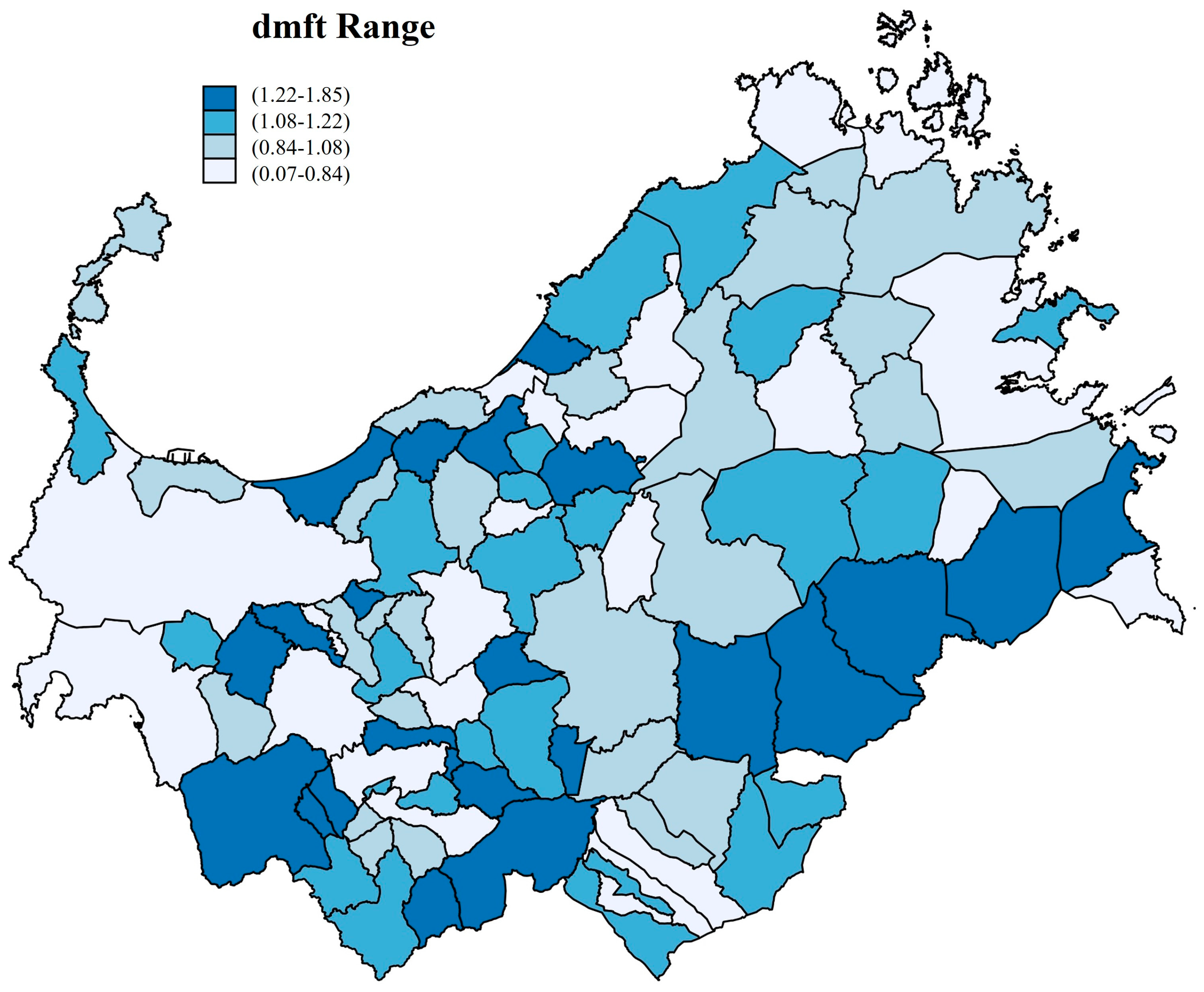
2.4. Autoregressive Analysis
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| (SED) | Socioeconomic Deprivation |
| (WHO) | World Health Organization |
| dmft/DMFT | (decayed (D), missing (M), and filled (F) teeth (T), where upper case denotes permanent dentition and lower case primary dentition) |
| (IDMS) | Sardinian Deprivation Index |
| (SAR) | Spatial Autoregressive Models |
References
- Lagerweij, M.; van Loveren, C. Chapter 7: Sugar and Dental Caries. Monogr. Oral Sci. 2020, 8, 68–76. [Google Scholar] [CrossRef]
- Kassebaum, N.J.; Smith, A.G.C.; Bernabé, E.; Fleming, T.D.; Reynolds, A.E.; Vos, T.; Murray, C.J.L.; Marcenes, W.; GBD 2015 Oral Health Collaborators. Global, Regional, and National Prevalence, Incidence, and Disability-Adjusted Life Years for Oral Conditions for 195 Countries, 1990–2015: A Systematic Analysis for the Global Burden of Diseases, Injuries, and Risk Factors. J. Dent. Res. 2017, 96, 380–387. [Google Scholar] [CrossRef] [PubMed]
- Hosseinpoor, A.R.; Parker, L.A.; Tursan d’Espaignet, E.; Chatterji, S. Socioeconomic inequality in smoking in low-income and middle-income countries: Results from the World Health Survey. PLoS ONE 2012, 7, e42843. [Google Scholar] [CrossRef]
- Folayan, M.O.; El Tantawi, M.; Vukovic, A.; Schroth, R.J.; Alade, M.; Mohebbi, S.Z.; Al-Batayneh, O.B.; Arheiam, A.; Amalia, R.; Gaffar, B.; et al. Governance, maternal well-being and early childhood caries in 3–5-year-old children. BMC Oral Health 2020, 5, 166. [Google Scholar] [CrossRef]
- Rai, N.K.; Tiwari, T. Parental Factors Influencing the Development of Early Childhood Caries in Developing Nations: A Systematic Review. Front. Public Health 2018, 16, 64. [Google Scholar] [CrossRef] [PubMed]
- Salmon-Ibarra, C.C.; Rezaee, A.; Morris, A.J.; Ravaghi, V. Deprivation and child dental attendance in England: Exploring the shape and moderators. Community Dent. Health 2020, 29, 161–166. [Google Scholar] [CrossRef]
- Rodriguez, J.L.; Thakkar-Samtani, M.; Heaton, L.J.; Tranby, E.P.; Tiwari, T. Caries risk and social determinants of health: A big data report. J. Am. Dent. Assoc. 2023, 154, 113–121. [Google Scholar] [CrossRef]
- Bradley, R.H.; Corwyn, R.F. Socioeconomic status and child development. Annu. Rev. Psychol. 2002, 53, 371–399. [Google Scholar] [CrossRef]
- Poulain, T.; Vogel, M.; Kiess, W. Review on the role of socioeconomic status in child health and development. Curr. Opin. Pediatr. 2020, 32, 308–314. [Google Scholar] [CrossRef]
- Campus, G.; Cocco, F.; Strohmenger, L.; Wolf, T.G.; Balian, A.; Arghittu, A.; Cagetti, M.G. Inequalities in caries among pre-school Italian children with different background. BMC Pediatr. 2022, 23, 443. [Google Scholar] [CrossRef]
- Campus, G.; Solinas, G.; Sanna, A.; Maida, C.; Castiglia, P. Determinants of ECC in Sardinian preschool children. Community Dent Health 2007, 24, 253–256. [Google Scholar] [PubMed]
- Matranga, D.; Campus, G.; Castiglia, P.; Strohmenger, L.; Solinas, G. Italian deprivation index and dental caries in 12-year-old children: A multilevel Bayesian analysis. Caries Res. 2014, 48, 584–593. [Google Scholar] [CrossRef] [PubMed]
- Karam, S.A.; Costa, F.D.S.; Peres, K.G.; Peres, M.A.; Barros, F.C.; Bertoldi, A.D.; Santos, I.S.; Tovo, L.; Matijasevich, A.B.; Menezes, A.M.; et al. Two decades of socioeconomic inequalities in the prevalence of untreated dental caries in early childhood: Results from three birth cohorts in southern Brazil. Community Dent. Oral Epidemiol. 2023, 51, 355–363. [Google Scholar] [CrossRef] [PubMed]
- Ludovichetti, F.S.; Zuccon, A.; Lucchi, P.; Cattaruzza, G.; Zerman, N.; Stellini, E.; Mazzoleni, S. Mothers’ Awareness of the Correlation between Their Own and Their Children’s Oral Health. Int. J. Environ. Res. Public Health 2022, 19, 14967. [Google Scholar] [CrossRef] [PubMed]
- Chalvatzoglou, E.; Anagnostou, F.; Arapostathis, K.; Boka, V.; Arhakis, A. Assessment of Young Mothers’ Oral Hygiene Practices during Pregnancy and Their Knowledge of Children’s Oral Health in Northern Greece. J. Contemp. Dent. Pract. 2023, 24, 202–206. [Google Scholar]
- Kassebaum, N.J.; Bernabé, E.; Dahiya, M.; Bhandari, B.; Murray, C.J.; Marcenes, W. Global burden of untreated caries: A systematic review and metaregression. J. Dent. Res. 2015, 94, 650–658. [Google Scholar] [CrossRef]
- Matsuyama, Y.; Isumi, A.; Doi, S.; Fujiwara, T. Persistent poverty and child dental caries: Time-varying exposure analysis. J. Epidemiol. Community Health 2023, 77, 670–675. [Google Scholar] [CrossRef]
- Lamloum, D.; Dettori, M.; La Corte, P.; Agnoli, M.R.; Cappai, A.; Viarchi, A.; Arghittu, A.; Wolf, T.G.; Castiglia, P.; Campus, G. Oral Health Survey in Burundi; Evaluation of the Caries Experience in Schoolchildren Using the DMFT Index. Medicina 2023, 59, 1538. [Google Scholar] [CrossRef]
- Kashem, T.; Al Sayah, F.; Tawiah, A.; Ohinmaa, A.; Johnson, J.A. The relationship between individual-level deprivation and health-related quality of life. Health Qual. Life Outcomes 2019, 17, 176. [Google Scholar] [CrossRef]
- Townsend, P.; Phillimore, P.; Beattie, A. Health and Deprivation: Inequality and the North, 1st ed.; Routledge: Abingdon, UK, 1988. [Google Scholar] [CrossRef]
- Townsend, P. Deprivation. J. Soc. Policy 1987, 16, 125–146. [Google Scholar] [CrossRef]
- Regione Autonoma della Sardegna, I.D.M.S. Available online: https://www.sardegnaprogrammazione.it/index.php?xsl=1227&s=35&v=9&c=14173&es=6603&na=1&n=10&ni=1 (accessed on 6 December 2023).
- Centre for North South Economic Research. Economy of Sardinia. 26th Report. 2019. Available online: https://crenos.unica.it/crenosterritorio/sites/default/files/allegati-pubblicazioni-tes/26%20%C2%B0%20Rapporto%20CRENoS%20sull%27Economia%20della%20Sardegna.pdf (accessed on 2 January 2024).
- Arghittu, A.; Dettori, M.; Masia, M.D.; Azara, A.; Dempsey, E.; Castiglia, P. Social deprivation indexes and anti-influenza vaccination coverage in the elderly in Sardinia, Italy, with a focus on the Sassari municipality. J. Prev. Med. Hyg. 2019, 28, E45–E50. [Google Scholar] [CrossRef]
- Regione Autonoma della Sardegna. Piano Regionale della Prevenzione 2020–2025. Available online: https://delibere.regione.sardegna.it/protected/58651/0/def/ref/DBR58366/ (accessed on 27 December 2023).
- Klein, H.; Palmer, C.E. Studies on Dental Caries: IX. The Prevalence and Incidence of Dental Caries Experience, Dental Care, and Carious Defects Requiring Treatment in High School Children. Public Health Rep. 1940, 55, 1258–1268. [Google Scholar] [CrossRef]
- World Health Organization. Oral Health Surveys: Basic Methods-5th Edition. Available online: https://www.who.int/publications/i/item/9789241548649 (accessed on 6 December 2023).
- Li, Y.; Wang, W. Predicting Caries in Permanent Teeth from Caries in Primary Teeth: An Eight-year Cohort Study. J. Dent. Res. 2002, 81, 561–566. [Google Scholar] [CrossRef]
- Frencken, J.E.; de Amorim, R.G.; Faber, J.; Leal, S.C. The Caries Assessment Spectrum and Treatment (CAST) index: Rational and development. Int. Dent. J. 2011, 61, 117–123. [Google Scholar] [CrossRef]
- Ismail, A.I.; Sohn, W.; Tellez, M.; Amaya, A.; Sen, A.; Hasson, H.; Pitts, N.B. The International Caries Detection and Assessment System (ICDAS): An integrated system for measuring dental caries. Community Dent. Oral Epidemiol. 2007, 35, 170–178. [Google Scholar] [CrossRef] [PubMed]
- Leal, S.C.; Ribeiro, A.P.D.; Frencken, J.E. Caries Assessment Spectrum and Treatment (CAST): A Novel Epidemiological Instrument. Caries Res. 2017, 51, 500–506. [Google Scholar] [CrossRef] [PubMed]
- Nyvad, B.; Baelum, V. Nyvad Criteria for Caries Lesion Activity and Severity Assessment: A Validated Approach for Clinical Management and Research. Caries Res. 2018, 52, 397–405. [Google Scholar] [CrossRef]
- Pitts, N.B.; Ekstrand, K.R.; ICDAS Foundation. International Caries Detection and Assessment System (ICDAS) and its International Caries Classification and Management System (ICCMS)—Methods for staging of the caries process and enabling dentists to manage caries. Community Dent. Oral. Epidemiol. 2013, 41, e41–e52. [Google Scholar] [CrossRef]
- Tuttitalia. Scuole Primarie in Sardegna. Available online: https://www.tuttitalia.it/sardegna/86-scuole/scuola-primaria/ (accessed on 6 December 2023).
- Gazzetta Ufficiale della Repubblica Italiana. Available online: https://www.gazzettaufficiale.it/eli/gu/2008/03/31/76/sg/pdf (accessed on 6 December 2023).
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef]
- Campus, G.; Solinas, G.; Cagetti, M.G.; Senna, A.; Minelli, L.; Majori, S.; Montagna, M.T.; Reali, D.; Castiglia, P.; Strohmenger, L. National Pathfinder survey of 12-year-old Children’s Oral Health in Italy. Caries Res. 2007, 41, 512–517. [Google Scholar] [CrossRef]
- Monse, B.; Heinrich-Weltzien, R.; Benzian, H.; Holmgren, C.; van Palenstein Helderman, W. PUFA—An index of clinical consequences of untreated dental caries. Community Dent. Oral. Epidemiol. 2010, 38, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Regione Autonoma della Sardegna. Sardegna Geoportale. Available online: https://www.sardegnageoportale.it/ (accessed on 6 December 2023).
- Shala, K.S.; Dula, L.J.; Pustina-Krasniqi, T.; Bicaj, T.; Ahmedi, E.F.; Lila-Krasniqi, Z.; Tmava-Dragusha, A. Evaluation of Sensibility Threshold for Interocclusal Thickness of Patients Wearing Complete Dentures. Int. J. Dent. 2017, 2017, 5138950. [Google Scholar] [CrossRef] [PubMed]
- Campus, G.; Cocco, F.; Strohmenger, L.; Cagetti, M.G. Caries severity and socioeconomic inequalities in a nationwide setting: Data from the Italian National pathfinder in 12-years children. Sci. Rep. 2020, 24, 15622. [Google Scholar] [CrossRef] [PubMed]
- Pizzo, G.; Matranga, D.; Maniscalco, L.; Buttacavoli, F.; Campus, G.; Giuliana, G. Caries Severity, Decayed First Permanent Molars and Associated Factors in 6–7 Years Old Schoolchildren Living in Palermo (Southern Italy). J. Clin. Med. 2023, 12, 4343. [Google Scholar] [CrossRef]
- Hargreaves, D.S.; Struijs, J.N.; Schuster, M.A. US Children and Adolescents Had Fewer Annual Doctor and Dentist Contacts Than Their Dutch Counterparts, 2010–12. Health Aff. 2015, 34, 2113–2120. [Google Scholar] [CrossRef]
- Dettori, M.; Arru, B.; Azara, A.; Piana, A.; Mariotti, G.; Camerada, M.V.; Stefanelli, P.; Rezza, G.; Castiglia, P. In the Digital Era, Is Community Outrage a Feasible Proxy Indicator of Emotional Epidemiology? The Case of Meningococcal Disease in Sardinia. Italy. Int. J. Environ. Res. Public Health 2018, 18, 1512. [Google Scholar] [CrossRef]
- Liao, Y.; Zhou, C.; Zhang, Q.; Wang, X.; Yan, F.; Xing, X. Prevalence of early childhood caries in three regions of China: A cross-sectional study. Int. J. Paediatr. Dent. 2022, 32, 627–638. [Google Scholar] [CrossRef]
- Schuurman, N.; Bell, N.; Dunn, J.R.; Oliver, L. Deprivation indices; population health and geography: An evaluation of the spatial effectiveness of indices at multiple scales. J. Urban Health 2007, 84, 591–603. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Pearson chi-square was used to evaluate the association between groups. | |||
| 3–5 years n (%) | 6–11 years n (%) | Total n (%) | |
| Sex | |||
| Males | 2677 (50.69) | 2897 (51.13) | 5574 (50.92) |
| Females | 2604 (49.31) | 2769 (48.87) | 5373 (49.08) |
| Pearson χ2(1) = 0.21 p = 0.65 | |||
| Caries Experience | |||
| Caries-free (dmf = 0) | 4553 (86.21) | 3728 (65.80) | 8281 (75.65) |
| Affected (dmf > 0) | 728 (13.79) | 1938 (34.20) | 2666 (24.35) |
| Pearson χ2(1) = 618.59 p < 0.01 | |||
| Caries Prevalence | |||
| d = 0 | 4613 (87.35) | 4043 (71.36) | 8656 (79.07) |
| d > 0 | 668 (12.65) | 1623 (28.64) | 2291 (20.93) |
| Pearson χ2(1) = 422.61 p < 0.01 | |||
| 3–5 Years Mean ± SD | 6–11 Years Mean ± SD | ANOVA One Way F-Value p-Value | |
|---|---|---|---|
| decayed (d) | 0.41 ± 1.48 | 0.81 ± 1.76 | F = 163.40 p < 0.01 |
| missing (m) | 0.01 ± 0.11 | 0.10 ± 0.35 | F = 89.49 p < 0.01 |
| filled (f) | 0.03 ± 0.31 | 0.20 ± 0.77 | F = 222.96 p < 0.01 |
| dmf | 0.45 ± 1.55 | 1.07 ± 2.02 | F = 317.42 p < 0.01 |
| -A Caries Experience | |||||
| dmf = 0 n (%) | dmf = 1–2 n (%) | dmf = 3–4 n (%) | dmf > 4 n (%) | Total | |
| Sex | |||||
| Males | 4105 (73.65) | 748 (13.42) | 407 (7.30) | 314 (5.63) | 5574 (50.92) |
| Females | 4176 (77.72) | 648 (12.06) | 297 (5.53) | 252 (4.69) | 5373 (49.08) |
| Pearson χ2(3) = 28.07 p < 0.01 Linear trend z = −4.90 p < 0.01 | |||||
| Age groups | |||||
| 3–5 years | 4553 (86.21) | 400 (7.57) | 162 (3.07) | 166 (3.14) | 5281 (48.24) |
| 6–11 years | 3728 (65.80) | 996 (17.58) | 542 (9.57) | 400 (7.06) | 5666 (51.76) |
| Pearson χ2(3) = 625.73 p < 0.01 Linear trend z = 22.01 p < 0.01 | |||||
| Deprivation Index * | |||||
| Very low | 2885 (80.90) | 385 (10.80) | 157 (4.40) | 139 (3.90) | 3566 (32.58) |
| Low | 3216 (79.88) | 454 (11.28) | 189 (4.69) | 167 (4.15) | 4026 (36.38) |
| Medium | 560 (61.07) | 168 (18.32) | 119 (12.98) | 70 (7.63) | 917 (8.37) |
| High | 1620 (66.45) | 389 (15.96) | 239 (9.80) | 190 (7.79) | 2438 (22.27) |
| Pearson χ2(3) = 343.49 p < 0.01 Linear trend z = −4.04 p < 0.01 | |||||
| -B Caries Prevalence | |||||
| d = 0 n (%) | d = 1–2 n (%) | d = 3–4 n (%) | d > 4 n (%) | Total | |
| Sex | |||||
| Males | 4317 (77.45) | 706 (12.67) | 323 (5.79) | 228 (4.09) | 5574 (50.92) |
| Females | 4339 (80.76) | 609 (11.33) | 231 (4.30) | 194 (3.61) | 5373 (49.08) |
| Pearson χ2(3) = 21.54 p < 0.01 Linear trend z = 13.73 p < 0.01 | |||||
| Age groups | |||||
| 3–5 years | 4613 (87.35) | 369 (6.99) | 148 (2.80) | 151 (2.86) | 5281 (48.24) |
| 6–11 years | 4043 (71.36) | 946 (16.70) | 406 (7.17) | 271 (4.78) | 5666 (51.76) |
| Pearson χ2(3) = 431.98 p < 0.01 Linear trend z = 16.97 p < 0.01 | |||||
| Deprivation Index * | |||||
| Very low | 2977 (83.48) | 365 (10.24) | 115 (3.22) | 109 (3.06) | 3566 (32.58) |
| Low | 3346 (83.11) | 411 (10.21) | 144 (3.58) | 125 (3.10) | 4026 (36.38) |
| Medium | 600 (65.43) | 176 (19.19) | 88 (9.60) | 53 (5.78) | 917 (8.37) |
| High | 1733 (71.08) | 363 (14.89) | 207 (8.49) | 135 (5.54) | 2438 (22.27) |
| Pearson χ2(3) = 308.47 p < 0.01 Linear trend z = 13.73 p < 0.01 | |||||
| RRR (SE) | p-Value | 95%CI | |
|---|---|---|---|
| -A Caries Experience N obs = 10,947 Log Likelihood = −8392.96 χ2(9) = 803.40 p < 0.01 | |||
| dmf = 0 | Base outcome | ||
| dmf = 1–2 | |||
| Sex (females) | 0.84 (0.05) | <0.01 | 0.74–0.95 |
| Age groups (6–11 yy) | 2.86 (0.18) | <0.01 | 2.52–3.24 |
| Deprivation index (high) | 1.16 (0.03) | <0.01 | 1.10–1.22 |
| Constant | 0.03 (0.01) | <0.01 | 0.02–0.04 |
| dmf = 3–4 | |||
| Sex (females) | 0.70 (0.05) | <0.01 | 0.60–0.82 |
| Age groups (6–11 yy) | 3.60 (0.34) | <0.01 | 3.00–4.33 |
| Deprivation index (high) | 1.36 (0.05) | <0.01 | 1.27–1.45 |
| Constant | 0.01 (0.01) | <0.01 | 0.01–0.01 |
| dmf > 4 | |||
| Sex (females) | 0.77 (0.07) | <0.01 | 0.65–0.92 |
| Age groups (6–11 yy) | 2.63 (0.25) | <0.01 | 2.18–3.18 |
| Deprivation index (high) | 1.30 (0.05) | <0.01 | 1.21–1.41 |
| Constant | 0.01 (0.01) | <0.01 | 0.01–0.02 |
| -B Caries Prevalence N obs = 10,947 Log Likelihood = −7549.30 χ2(9) = 593.84 p < 0.01 | |||
| RRR (SE) | p-value | 95%CI | |
| d = 0 | Base outcome | ||
| d = 1–2 | |||
| Sex (females) | 0.85 (0.05) | <0.01 | 0.76–0.96 |
| Age groups (6–11 yy) | 2.75 (0.18) | <0.01 | 2.42–3.13 |
| Deprivation index (high) | 1.15 (0.03) | <0.01 | 1.09–1.22 |
| Constant | 0.03 (0.01) | <0.01 | 0.02–0.04 |
| d = 3–4 | |||
| Sex (females) | 0.70 (0.06) | <0.01 | 0.85–0.83 |
| Age groups (6–11 yy) | 3.60 (0.34) | <0.01 | 2.20–2.26 |
| Deprivation index (high) | 1.44 (0.06) | <0.01 | 1.33–1.56 |
| Constant | 0.01 (0.01) | <0.01 | 0.01–0.01 |
| d > 4 | |||
| Sex (females) | 0.84 (0.08) | 0.07 | 0.68–1.02 |
| Age groups (6–11 yy) | 1.84 (0.19) | <0.01 | 1.50–2.26 |
| Deprivation index (high) | 1.28 (0.06) | <0.01 | 1.17–1.40 |
| Constant | 0.01 (0.01) | <0.01 | 0.01–0.02 |
| N obs = 92 municipalities Wald χ2(1) = 6.93 p < 0.01 | |||
| Caries prevalence | Coef (SE) | p-value | 95%CI |
| IDMS | 0.32 (0.12) | <0.01 | 0.08–0.55 |
| Constant | 0.96 | <0.01 | 0.88–1.05 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dettori, M.; Arghittu, A.; Cappai, A.; Castiglia, P.; Campus, G.; Children’s Smiles Sardinian Group. Impact of Socioeconomic Inequalities on Dental Caries Status in Sardinian Children. Children 2024, 11, 96. https://doi.org/10.3390/children11010096
Dettori M, Arghittu A, Cappai A, Castiglia P, Campus G, Children’s Smiles Sardinian Group. Impact of Socioeconomic Inequalities on Dental Caries Status in Sardinian Children. Children. 2024; 11(1):96. https://doi.org/10.3390/children11010096
Chicago/Turabian StyleDettori, Marco, Antonella Arghittu, Andrea Cappai, Paolo Castiglia, Guglielmo Campus, and Children’s Smiles Sardinian Group. 2024. "Impact of Socioeconomic Inequalities on Dental Caries Status in Sardinian Children" Children 11, no. 1: 96. https://doi.org/10.3390/children11010096
APA StyleDettori, M., Arghittu, A., Cappai, A., Castiglia, P., Campus, G., & Children’s Smiles Sardinian Group. (2024). Impact of Socioeconomic Inequalities on Dental Caries Status in Sardinian Children. Children, 11(1), 96. https://doi.org/10.3390/children11010096