
The Bidirectional Correlation between Fundamental Motor Skill and Moderate-to-Vigorous Physical Activities: A Systematic Review and Meta-Analysis

Abstract
:1. Introduction
2. Methods
2.1. Literature Search
2.2. Criteria for Study Inclusion and Exclusion
2.3. Study Selection and Data Extraction
2.4. Quality of the Evidence
2.5. Statistical Analysis
3. Results
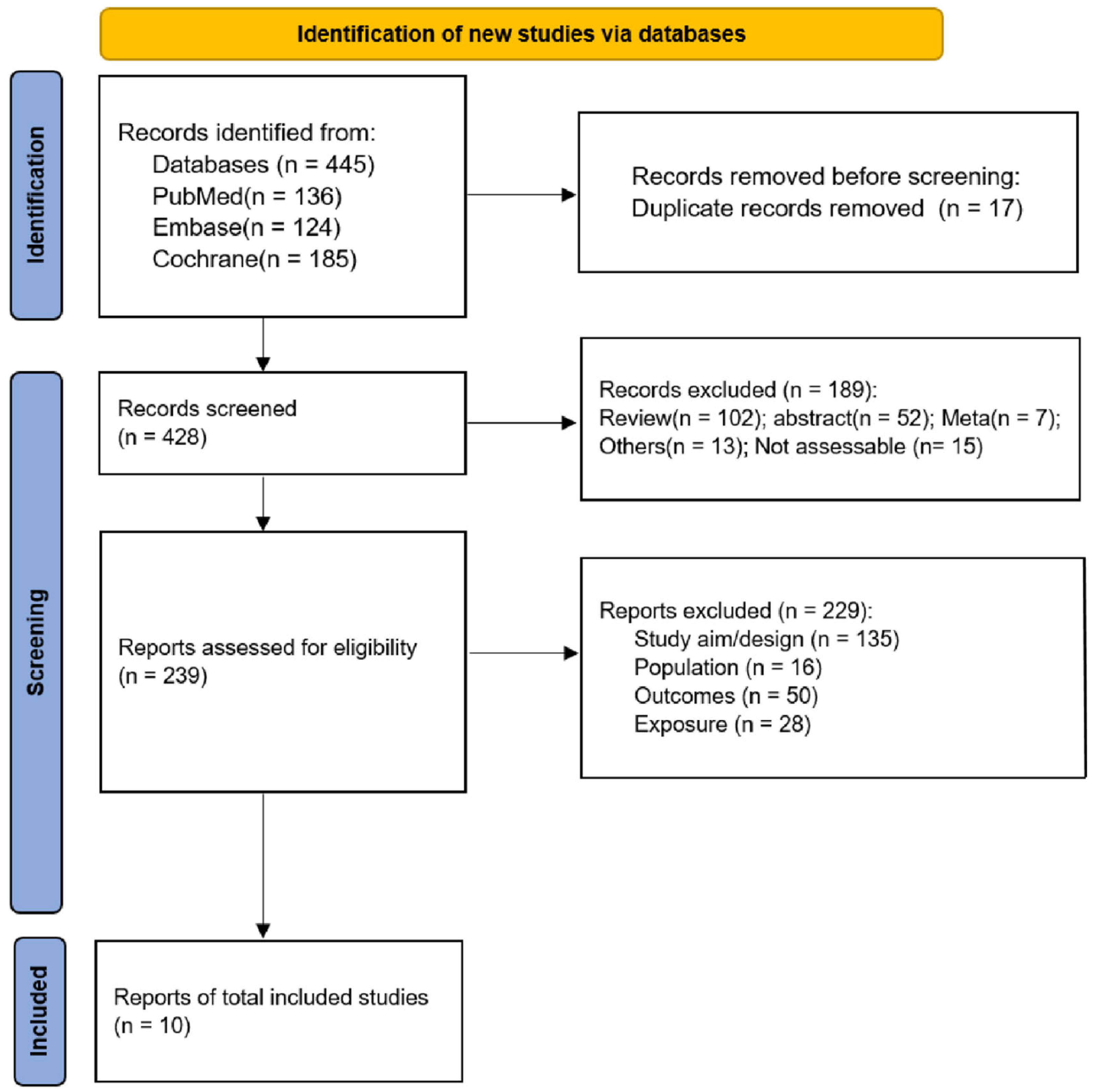
3.1. Study Selection
3.2. Study Characteristics
3.3. Quality Assessment
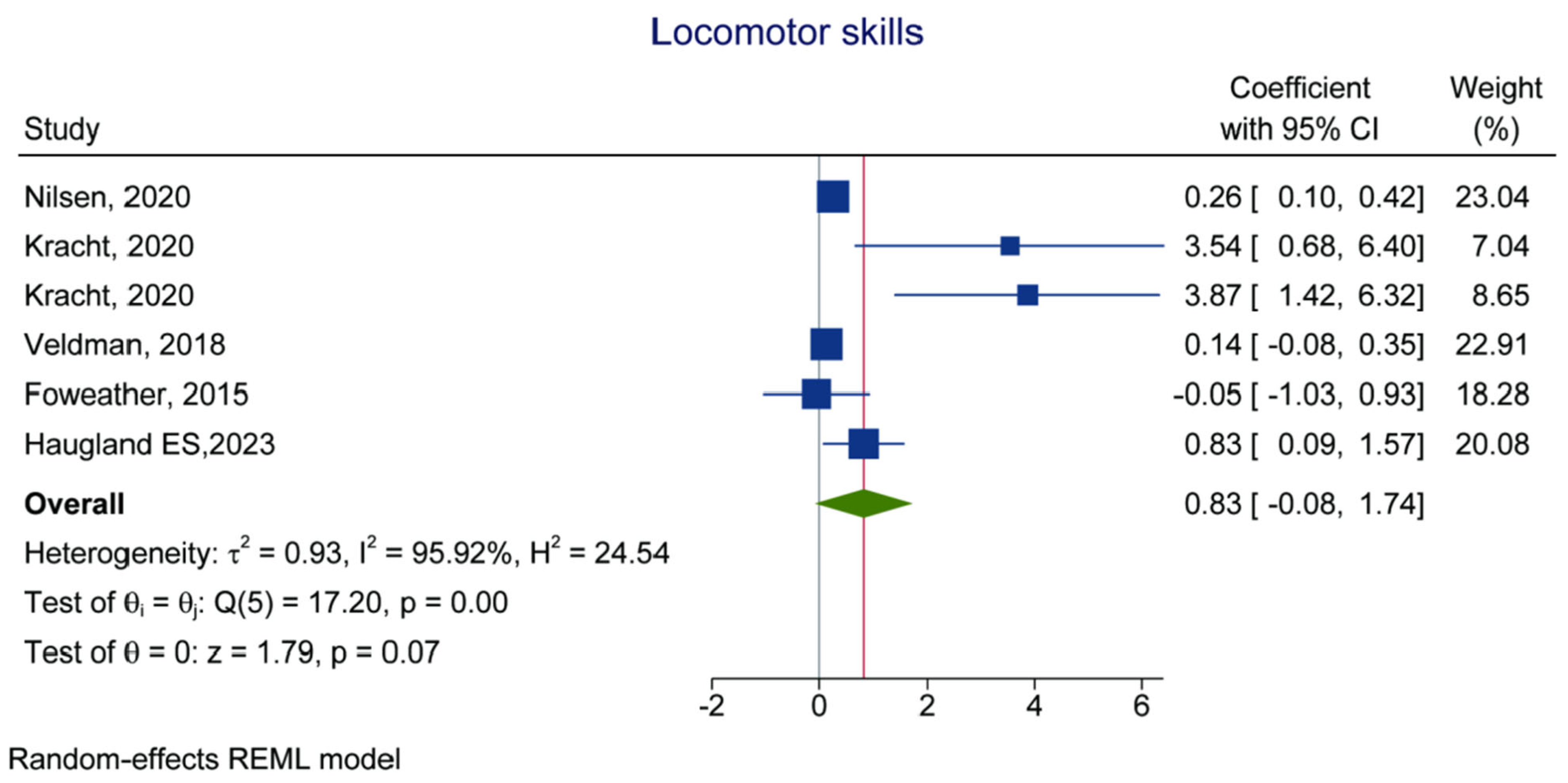
3.4. Locomotor Skills as the Outcome
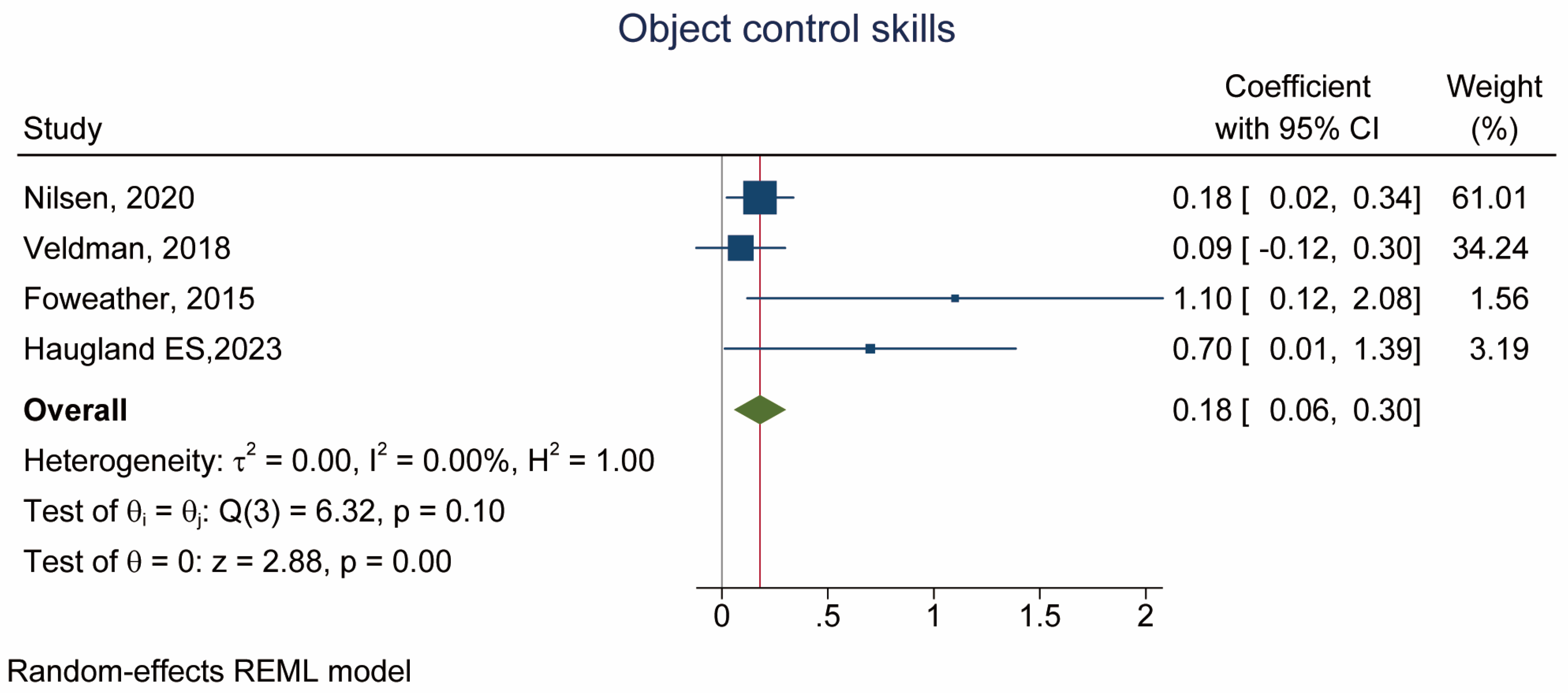
3.5. Control Skills as the Outcome
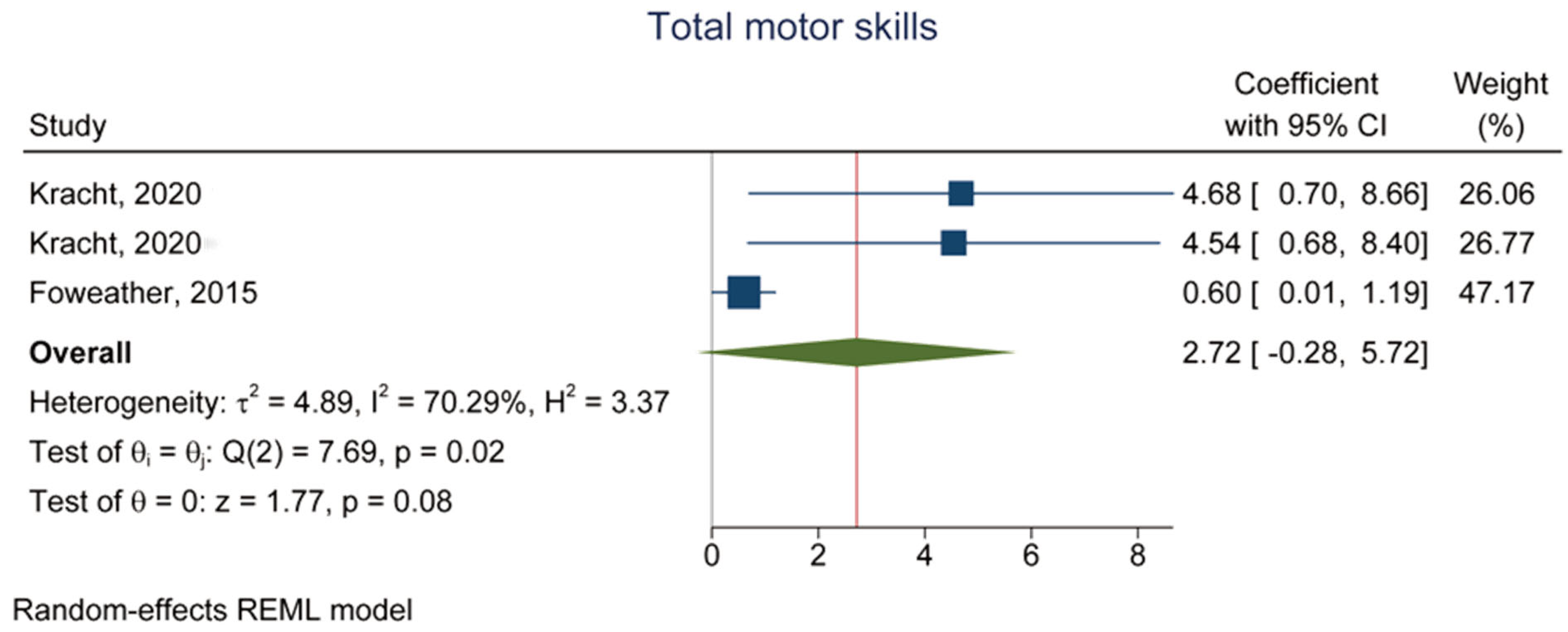
3.6. Total Motor Skills as the Outcome
3.7. MVPA as the Outcome
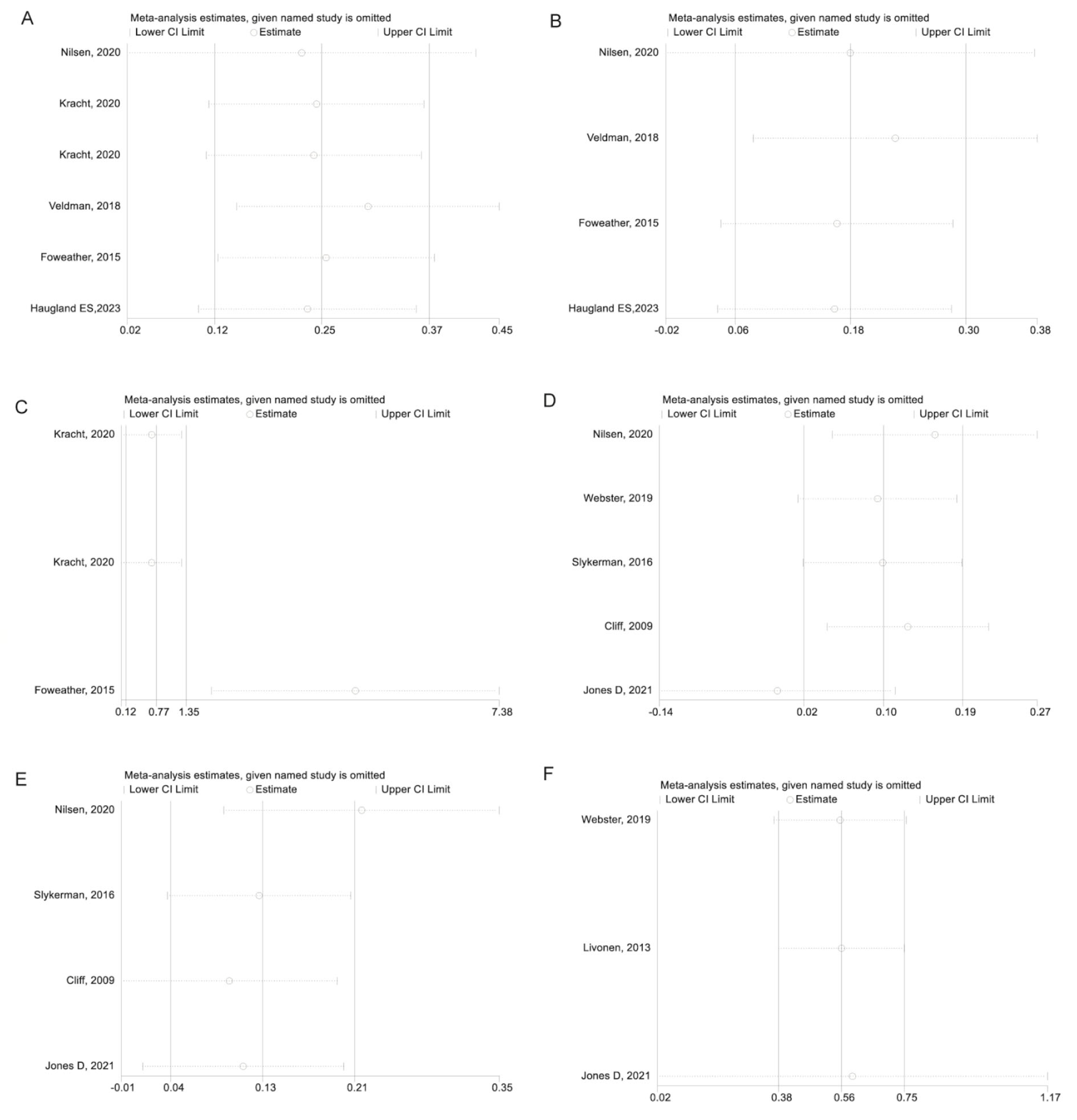
3.8. Sensitivity Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Veldman, S.L.C.; Chin, A.; Paw, M.J.M.; Altenburg, T.M. Physical activity and prospective associations with indicators of health and development in children aged <5 years: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 6. [Google Scholar] [CrossRef]
- Kemp, B.J.; Dumuid, D.; Chong, K.H.; Parrish, A.M.; Cliff, D. Cross-sectional and longitudinal associations of domain-specific physical activity composition with health-related quality of life in childhood and adolescence in Australia. Int. J. Behav. Nutr. Phys. Act. 2023, 20, 67. [Google Scholar] [CrossRef]
- Carson, V.; Lee, E.Y.; Hewitt, L.; Jennings, C.; Hunter, S.; Kuzik, N.; Stearns, J.A.; Unrau, S.P.; Poitras, V.J.; Gray, C.; et al. Systematic review of the relationships between physical activity and health indicators in the early years (0–4 years). BMC Public Health 2017, 17, 854. [Google Scholar] [CrossRef]
- O’Brien, W.; Khodaverdi, Z.; Bolger, L.; Murphy, O.; Philpott, C.; Kearney, P.E. Exploring Recommendations for Child and Adolescent Fundamental Movement Skills Development: A Narrative Review. Int. J. Environ. Res. Public Health 2023, 20, 3278. [Google Scholar] [CrossRef]
- Jago, R.; Salway, R.; House, D.; Walker, R.; Emm-Collison, L.; Sansum, K.; Breheny, K.; Reid, T.; Churchward, S.; Williams, J.G.; et al. Short and medium-term effects of the COVID-19 lockdowns on child and parent accelerometer-measured physical activity and sedentary time: A natural experiment. Int. J. Behav. Nutr. Phys. Act. 2023, 20, 42. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Kelly, A.S. Review of Childhood Obesity: From Epidemiology, Etiology, and Comorbidities to Clinical Assessment and Treatment. Mayo Clin. Proc. 2017, 92, 251–265. [Google Scholar] [CrossRef] [PubMed]
- Turer, C.B.; Barlow, S.E.; Sarwer, D.B.; Adamson, B.; Sanders, J.; Ahn, C.; Zhang, S.; Flores, G.; Skinner, C.S. Association of Clinician Behaviors and Weight Change in School-Aged Children. Am. J. Prev. Med. 2019, 57, 384–393. [Google Scholar] [CrossRef] [PubMed]
- Greydanus, D.E.; Agana, M.; Kamboj, M.K.; Shebrain, S.; Soares, N.; Eke, R.; Patel, D.R. Pediatric obesity: Current concepts. Dis. Mon. 2018, 64, 98–156. [Google Scholar] [CrossRef] [PubMed]
- Pratt, M.; Ramirez Varela, A.; Salvo, D.; Kohl Iii, H.W.; Ding, D. Attacking the pandemic of physical inactivity: What is holding us back? Br. J. Sports Med. 2020, 54, 760–762. [Google Scholar] [CrossRef]
- Tremblay, M.S.; Gray, C.E.; Akinroye, K.; Harrington, D.M.; Katzmarzyk, P.T.; Lambert, E.V.; Liukkonen, J.; Maddison, R.; Ocansey, R.T.; Onywera, V.O.; et al. Physical activity of children: A global matrix of grades comparing 15 countries. J. Phys. Act. Health. 2014, 11 (Suppl. S1), S113–S125. [Google Scholar] [CrossRef]
- Cliff, D.P.; McNeill, J.; Vella, S.A.; Howard, S.J.; Santos, R.; Batterham, M.; Melhuish, E.; Okely, A.D.; de Rosnay, M. Adherence to 24-Hour Movement Guidelines for the Early Years and associations with social-cognitive development among Australian preschool children. BMC Public Health 2017, 17 (Suppl. S5), 857. [Google Scholar] [CrossRef] [PubMed]
- Chaput, J.P.; Colley, R.C.; Aubert, S.; Carson, V.; Janssen, I.; Roberts, K.C.; Tremblay, M.S. Proportion of preschool-aged children meeting the Canadian 24-h Movement Guidelines and associations with adiposity: Results from the Canadian Health Measures Survey. BMC Public Health 2017, 17 (Suppl. S5), 829. [Google Scholar] [CrossRef]
- Aadland, E.; Okely, A.D.; Nilsen, A.K.O. Trajectories of physical activity and sedentary time in Norwegian children aged 3-9 years: A 5-year longitudinal study. Int. J. Behav. Nutr. Phys. Act. 2022, 19, 67. [Google Scholar] [CrossRef] [PubMed]
- Leis, A.; Ward, S.; Vatanparast, H.; Humbert, M.L.; Chow, A.F.; Muhajarine, N.; Engler-Stringer, R.; Bélanger, M. Effectiveness of the Healthy Start-Départ Santé approach on physical activity, healthy eating and fundamental movement skills of preschoolers attending childcare centres: A randomized controlled trial. BMC Public Health 2020, 20, 523. [Google Scholar] [CrossRef]
- Ryder, J.R.; Jacobs, D.R., Jr.; Sinaiko, A.R.; Kornblum, A.P.; Steinberger, J. Longitudinal Changes in Weight Status from Childhood and Adolescence to Adulthood. J. Pediatr. 2019, 214, 187–192.e2. [Google Scholar] [CrossRef]
- Donnelly, F.C.; Mueller, S.S.; Gallahue, D.L. Developmental Physical Education for All Children: Theory Into Practice, 5th ed.; Human Kinetics: Champaign, IL, USA, 2016. [Google Scholar]
- Ulrich, D.A. The test of gross motor development-3 (TGMD-3): Administration, scoring, and international norms. Spor Bilim. Derg. 2013, 24, 27–33. [Google Scholar]
- Sallis, J.F.; Owen, N.; Fotheringham, M.J. Behavioral epidemiology: A systematic framework to classify phases of research on health promotion and disease prevention. Ann. Behav. Med. 2000, 22, 294–298. [Google Scholar] [CrossRef]
- Robinson, L.E.; Stodden, D.F.; Barnett, L.M.; Lopes, V.P.; Logan, S.W.; Rodrigues, L.P.; D’Hondt, E. Motor Competence and its Effect on Positive Developmental Trajectories of Health. Sports Med. 2015, 45, 1273–1284. [Google Scholar] [CrossRef]
- Gallahue, D.L.; Ozmun, J.C.; Goodway, J.D. Understanding Motor Development: Infants, Children, Adolescents, Adults; McGraw-Hill: New York, NY, USA, 2012. [Google Scholar]
- Figueroa, R.; An, R. Motor Skill Competence and Physical Activity in Preschoolers: A Review. Matern. Child. Health J. 2017, 21, 136–146. [Google Scholar] [CrossRef]
- Nilsen, A.K.O.; Anderssen, S.A.; Johannessen, K.; Aadland, K.N.; Ylvisaaker, E.; Loftesnes, J.M.; Aadland, E. Bi-directional prospective associations between objectively measured physical activity and fundamental motor skills in children: A two-year follow-up. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 3. [Google Scholar] [CrossRef]
- Engel, A.; Broderick, C.; van Doorn, N.; Hardy, L.; Ward, R.; Kwai, N.; Parmenter, B. Effect of a fundamental motor skills intervention on fundamental motor skill and physical activity in a preschool setting: A cluster randomized controlled trial. Pediatr. Exerc. Sci. 2021, 34, 57–66. [Google Scholar] [CrossRef]
- Stodden, D.F.; Goodway, J.D.; Langendorfer, S.J.; Roberton, M.A.; Rudisill, M.E.; Garcia, C.; Garcia, L.E. A Developmental Perspective on the Role of Motor Skill Competence in Physical Activity: An Emergent Relationship. Quest 2008, 60, 290–306. [Google Scholar] [CrossRef]
- Gao, Z.; Wen, X.; Fu, Y.; Lee, J.E.; Zeng, N. Motor Skill Competence Matters in Promoting Physical Activity and Health. Biomed Res. Int. 2021, 2021, 9786368. [Google Scholar] [CrossRef] [PubMed]
- Lima, R.A.; Pfeiffer, K.; Larsen, L.R.; Bugge, A.; Moller, N.C.; Anderson, L.B.; Stodden, D.F. Physical Activity and Motor Competence Present a Positive Reciprocal Longitudinal Relationship Across Childhood and Early Adolescence. J. Phys. Act. Health 2017, 14, 440–447. [Google Scholar] [CrossRef]
- Goodman, D.; Park, H.L.; Stefanick, M.; LeBlanc, E.; Bea, J.; Qi, L.; Kapphahn, K.; Lamonte, M.; Manini, T.; Desai, M.; et al. Relation between self-recalled childhood physical activity and adult physical activity: The women’s health initiative. Open J. Epidemiol. 2013, 3, 224–231. [Google Scholar] [CrossRef]
- Itoh, H.; Kitamura, F.; Hagi, N.; Mashiko, T.; Matsukawa, T.; Yokoyama, K. Leisure-time physical activity in youth as a predictor of adult leisure physical activity among Japanese workers: A cross-sectional study. Environ. Health Prev. Med. 2017, 22, 37. [Google Scholar] [CrossRef]
- Kaseva, K.; Lounassalo, I.; Yang, X.; Kukko, T.; Hakonen, H.; Kulmala, J.; Pahkala, K.; Rovio, S.; Hirvensalo, M.; Raitakari, O.; et al. Associations of active commuting to school in childhood and physical activity in adulthood. Sci. Rep. 2023, 13, 7642. [Google Scholar] [CrossRef]
- García-Hermoso, A.; Izquierdo, M.; Ramírez-Vélez, R. Tracking of physical fitness levels from childhood and adolescence to adulthood: A systematic review and meta-analysis. Transl. Pediatr. 2022, 11, 474–486. [Google Scholar] [CrossRef]
- Selcuk, A.A. A Guide for Systematic Reviews: PRISMA. Turk. Arch. Otorhinolaryngol. 2019, 57, 57–58. [Google Scholar] [CrossRef]
- Aslam, S.; Emmanuel, P. Formulating a researchable question: A critical step for facilitating good clinical research. Indian J. Sex. Transm. Dis. AIDS 2010, 31, 47–50. [Google Scholar] [CrossRef]
- Lo, C.K.; Mertz, D.; Loeb, M. Newcastle-Ottawa Scale: Comparing reviewers’ to authors’ assessments. BMC Med. Res. Methodol. 2014, 14, 45. [Google Scholar] [CrossRef]
- Ma, L.L.; Wang, Y.Y.; Yang, Z.H.; Huang, D.; Weng, H.; Zeng, X.T. Methodological quality (risk of bias) assessment tools for primary and secondary medical studies: What are they and which is better? Mil. Med. Res. 2020, 7, 7. [Google Scholar] [CrossRef] [PubMed]
- Agency for Healthcare Research and Quality. Agency for Healthcare Research and Quality (AHRQ) Methodology Checklist for Cross-Sectional Studies; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2011. Available online: https://effectivehealthcare.ahrq.gov/sites/default/files/assessing-the-risk-of-bias_draft-report.pdf (accessed on 20 October 2022).
- Higgins, J.P.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions Version 6.1; Cochrane Collaboration: London, UK, 2020. [Google Scholar]
- Kracht, C.L.; Webster, E.K.; Staiano, A.E. Relationship between the 24-Hour Movement Guidelines and fundamental motor skills in preschoolers. J. Sci. Med. Sport 2020, 23, 1185–1190. [Google Scholar] [CrossRef]
- Webster, E.K.; Martin, C.K.; Staiano, A.E. Fundamental motor skills, screen-time, and physical activity in preschoolers. J. Sport. Health Sci. 2019, 8, 114–121. [Google Scholar] [CrossRef] [PubMed]
- Cliff, D.P.; Okely, A.D.; Smith, L.M.; McKeen, K. Relationships between fundamental movement skills and objectively measured physical activity in preschool children. Pediatr. Exerc. Sci. 2009, 21, 436–449. [Google Scholar] [CrossRef]
- Foweather, L.; Knowles, Z.; Ridgers, N.D.; O’Dwyer, M.V.; Foulkes, J.D.; Stratton, G. Fundamental movement skills in relation to weekday and weekend physical activity in preschool children. J. Sci. Med. Sport 2015, 18, 691–696. [Google Scholar] [CrossRef]
- Iivonen, K.S.; Saakslahti, A.K.; Mehtala, A.; Villberg, J.J.; Tammelin, T.H.; Kulmala, J.S.; Poskiparta, M. Relationship between fundamental motor skills and physical activity in 4-year-old preschool children. Percept. Mot. Skills 2013, 117, 627–646. [Google Scholar] [CrossRef]
- Slykerman, S.; Ridgers, N.D.; Stevenson, C.; Barnett, L.M. How important is young children’s actual and perceived movement skill competence to their physical activity? J. Sci. Med. Sport. 2016, 19, 488–492. [Google Scholar] [CrossRef]
- Veldman, S.L.C.; Jones, R.A.; Santos, R.; Sousa-Sa, E.; Pereira, J.R.; Zhang, Z.; Okely, A.D. Associations between gross motor skills and physical activity in Australian toddlers. J. Sci. Med. Sport. 2018, 21, 817–821. [Google Scholar] [CrossRef]
- Haugland, E.S.; Nilsen, A.K.O.; Okely, A.D.; Aadland, K.N.; Aadland, E. Multivariate physical activity association patterns for fundamental motor skills and physical fitness in preschool children aged 3–5 years. J. Sports Sci. 2023, 41, 654–667. [Google Scholar] [CrossRef]
- Jones, D.; Innerd, A.; Giles, E.L.; Azevedo, L.B. The association between physical activity, motor skills and school readiness in 4–5-year-old children in the northeast of England. Int. J. Environ. Res. Public Health 2021, 18, 11931. [Google Scholar] [CrossRef] [PubMed]
- Schmutz, E.A.; Haile, S.R.; Leeger-Aschmann, C.S.; Kakebeeke, T.H.; Zysset, A.E.; Messerli-Burgy, N.; Stulb, K.; Arhab, A.; Meyer, A.H.; Munsch, S.; et al. Physical activity and sedentary behavior in preschoolers: A longitudinal assessment of trajectories and determinants. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 35. [Google Scholar] [CrossRef] [PubMed]
- Venetsanou, F.; Kambas, A. Can Motor Proficiency in Preschool Age Affect Physical Activity in Adolescence? Pediatr. Exerc. Sci. 2017, 29, 254–259. [Google Scholar] [CrossRef]
- Lopes, L.; Silva Mota, J.A.P.; Moreira, C.; Abreu, S.; Agostinis Sobrinho, C.; Oliveira-Santos, J.; Oliveira, A.; Okely, A.; Santos, R. Longitudinal associations between motor competence and different physical activity intensities: LabMed physical activity study. J. Sports Sci. 2019, 37, 285–290. [Google Scholar] [CrossRef]
- Larsen, L.R.; Kristensen, P.L.; Junge, T.; Rexen, C.T.; Wedderkopp, N. Motor Performance as Predictor of Physical Activity in Children: The CHAMPS Study-DK. Med. Sci. Sports Exerc. 2015, 47, 1849–1856. [Google Scholar] [CrossRef]
- Barnett, L.M.; Salmon, J.; Hesketh, K.D. More active pre-school children have better motor competence at school starting age: An observational cohort study. BMC Public Health 2016, 16, 1068. [Google Scholar] [CrossRef]
- Tonge, K.L.; Jones, R.A.; Okely, A.D. Correlates of children’s objectively measured physical activity and sedentary behavior in early childhood education and care services: A systematic review. Prev. Med. 2016, 89, 129–139. [Google Scholar] [CrossRef]
- Zeng, N.; Ayyub, M.; Sun, H.; Wen, X.; Xiang, P.; Gao, Z. Effects of Physical Activity on Motor Skills and Cognitive Development in Early Childhood: A Systematic Review. Biomed Res. Int. 2017, 2017, 2760716. [Google Scholar] [CrossRef]
- Salem, Y.; Gropack, S.J.; Coffin, D.; Godwin, E.M. Effectiveness of a low-cost virtual reality system for children with developmental delay: A preliminary randomised single-blind controlled trial. Physiotherapy 2012, 98, 189–195. [Google Scholar] [CrossRef]
- Bonvin, A.; Barral, J.; Kakebeeke, T.H.; Kriemler, S.; Longchamp, A.; Schindler, C.; Marques-Vidal, P.; Puder, J.J. Effect of a governmentally-led physical activity program on motor skills in young children attending child care centers: A cluster randomized controlled trial. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 90. [Google Scholar] [CrossRef]
- Ward, D.S.; Vaughn, A.; McWilliams, C.; Hales, D. Interventions for increasing physical activity at child care. Med. Sci. Sports Exerc. 2010, 42, 526–534. [Google Scholar] [CrossRef] [PubMed]
- Hardy, L.L.; King, L.; Farrell, L.; Macniven, R.; Howlett, S. Fundamental movement skills among Australian preschool children. J. Sci. Med. Sport 2010, 13, 503–508. [Google Scholar] [CrossRef]
- Khan, N.A.; Hillman, C.H. The relation of childhood physical activity and aerobic fitness to brain function and cognition: A review. Pediatr. Exerc. Sci. 2014, 26, 138–146. [Google Scholar] [CrossRef]
- Loprinzi, P.D.; Lovorn, A.; Gilmore, J. Effects of exercise on explicit memory function: Incidental and intentional encoding may depend on exercise timing. Percept. Mot. Ski. 2021, 128, 865–884. [Google Scholar] [CrossRef]
- Sacko, R.; McIver, K.; Brazendale, K.; Pfeifer, C.; Brian, A.; Nesbitt, D.; Stodden, D.F. Comparison of Indirect Calorimetry- and Accelerometry-Based Energy Expenditure during Children’s Discrete Skill Performance. Res. Q. Exerc. Sport 2019, 90, 629–640. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Design | Country | Sample Size | Age (Year, Mean or Median) | MVPA (min/day) | Physical Activity | Fundamental Motor Skills | Cut-Off Value of MVPA | Covariates | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total | Boys | Girls | Total | Boys | Girls | Total | Boys | Girls | |||||||
| Jones et al., 2021 [46] | Cross-sectional study | UK | 325 | 170 | 155 | 5.5 (0.3) | / | / | 100.1 (23.4) | / | / | Accelerometer | TGMD-2 | ≥1680 cpm | Sex, age at exposure, BMI-z and SES |
| Haugland et al., 2023 [45] | Cross-sectional study | Australia | 952 | 488 | 464 | 4.3 (0.9) | 4.3 (0.9) | 4.4 (0.9) | 75 (17) | 79 (17) | 70 (15) | ActiGraph GT3X+ | TGMD-3 | ≥2296 cpm | Sex, age, BMI, SES, accelerometer wear time, and assessor for FMS outcomes |
| Kracht et al., 2020 [38] | Prospective cohort study | USA | 53 | 28 | 25 | 3.2 ± 0.5 | / | / | 102 (30) | / | / | ActiGraph GT4X+ accelerometer | TGMD-3 | ≥420 counts/15 s | Baseline raw score (locomotor, ball skills, or TGMD-3), race, the other behaviors, and accelerometer wear time |
| Nilsen et al., 2020 [22] | Prospective cohort study | Norway | 376 | 376 | 0 | 4.7 ± 0.9 | / | / | 70 (14) | / | / | ActiGraph GT3X+ accelerometer | TGMD-3 | ≥2296 cpm | Sex, baseline age, baseline BMI, parental education and income level, accelerometer wear time at both time points, and the person scoring FMS at both time points |
| Webster et al., 2019 [39] | Prospective cohort study | USA | 126 | 58 | 68 | 3.4 ± 0.5 | 3.4 ± 0.5 | 3.3 ± 0.5 | / | 120 (36) | 90 (30) | ActiGraph GT3X+ accelerometer | TGMD-3 | ≥1680 cpm | Age, sex, household, income, acceleromotor wear time |
| Cliff et al., 2009 [40] | Cross-sectional study | Australia | 46 | 25 | 21 | / | 4.24 ± 0.69 | 4.35 ± 0.64 | / | 23.25 (32.4) | 22.67 (15.37) | ActiGraph 7164 uniaxial accelerometers | TGMD-2 | MVPA, >2460, >3248 and, >3564 cpm, for 3-, 4-, and 5-year-olds | Age, SES, BMI |
| Foweather et al., 2015 [41] | Cross-sectional study | UK | 99 | 52 | 47 | 4.6 ± 0.5 | 4.7 ± 0.6 | 4.6 ± 0.5 | / | 92.8 (30.7) | 76.7 (26.7) | ActiGraph GT1M accelerometer | TGMD-2 | ≥1680 cpm | Clustering, age, sex, standardized BMI, accelerometer wear time |
| Kracht et al., 2020 [38] | Cross-sectional study | USA | 107 | 48 | 59 | 3.4 ± 0.6 | / | / | 102 (36) | / | / | ActiGraph GT3X+ accelerometer | TGMD-3 | ≥420 counts/15 s | Age, sex, race, and other behaviors |
| Iivonen et al., 2013 [42] | Cross-sectional study | Finland | 37 | 17 | 20 | 4.1 ± 0.34 | 4.2 ± 0.38 | 4.02 ± 0.29 | / | 61.50 (20.39) | 59.90 (18.42) | ActiGraph GT3X accelerometer | APM Inventory manual and test booklet by Numminen (1995) | ≥196 counts/5 s | Sex, age, BMI, total skill score |
| Slykerman et al., 2016 [43] | Cross-sectional study | Australia | 109 | 59 | 50 | 6.5 ± 1.0 | / | / | / | 76.1 (20) | 57.0 (17.7) | ActiGraph GT3X+ accelerometer | TGMD-2 | ≥2296 cpm | Age, sex, accelerometer wear time, English speaking background |
| Veldman et al., 2018 [44] | Cross-sectional study | Australia | 284 | 151 | 133 | 1.65 ± 0.35 | 1.65 ± 0.35 | 1.64 ± 0.34 | / | 528.35 ± 124.32 | 547.18 ± 100.28 | ActiGraph GT3X+ accelerometer | PDMS-2 | >1680 cpm | Sex, age, BMI. |
| N | Standardized β (95% CI) | p | I2 (%) | Pheterogeneity | |
|---|---|---|---|---|---|
| Fundamental motor skills (outcome) | |||||
| Total | 3 | 2.72 (−0.28, 5.72) | 0.08 | 70.29 | 0.02 |
| Locomotor skills | 6 | 0.83 (−0.08, 1.74) | 0.07 | 95.92 | 0.001 |
| Object control skills | 4 | 0.18 (0.06, 0.30) | 0.001 | 0.00 | 0.10 |
| Moderate-to-vigorous physical activity (outcome) | |||||
| Total | 3 | 0.56 (0.38, 0.75) | 0.001 | 0.00 | 0.99 |
| Locomotor skills | 5 | 0.06 (−0.35, 0.47) | 0.79 | 90.26 | 0.001 |
| Object control skills | 4 | 0.15 (0.02, 0.27) | 0.02 | 34.43 | 0.15 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, Y.; Li, Z.; Yuan, L.; Zhou, Z. The Bidirectional Correlation between Fundamental Motor Skill and Moderate-to-Vigorous Physical Activities: A Systematic Review and Meta-Analysis. Children 2023, 10, 1504. https://doi.org/10.3390/children10091504
Liu Y, Li Z, Yuan L, Zhou Z. The Bidirectional Correlation between Fundamental Motor Skill and Moderate-to-Vigorous Physical Activities: A Systematic Review and Meta-Analysis. Children. 2023; 10(9):1504. https://doi.org/10.3390/children10091504
Chicago/Turabian StyleLiu, Yu, Zhen Li, Li Yuan, and Zhixiong Zhou. 2023. "The Bidirectional Correlation between Fundamental Motor Skill and Moderate-to-Vigorous Physical Activities: A Systematic Review and Meta-Analysis" Children 10, no. 9: 1504. https://doi.org/10.3390/children10091504
APA StyleLiu, Y., Li, Z., Yuan, L., & Zhou, Z. (2023). The Bidirectional Correlation between Fundamental Motor Skill and Moderate-to-Vigorous Physical Activities: A Systematic Review and Meta-Analysis. Children, 10(9), 1504. https://doi.org/10.3390/children10091504