
Attendance-Based Adherence and Outcomes of Obesity Management Program in Arab Adolescents

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
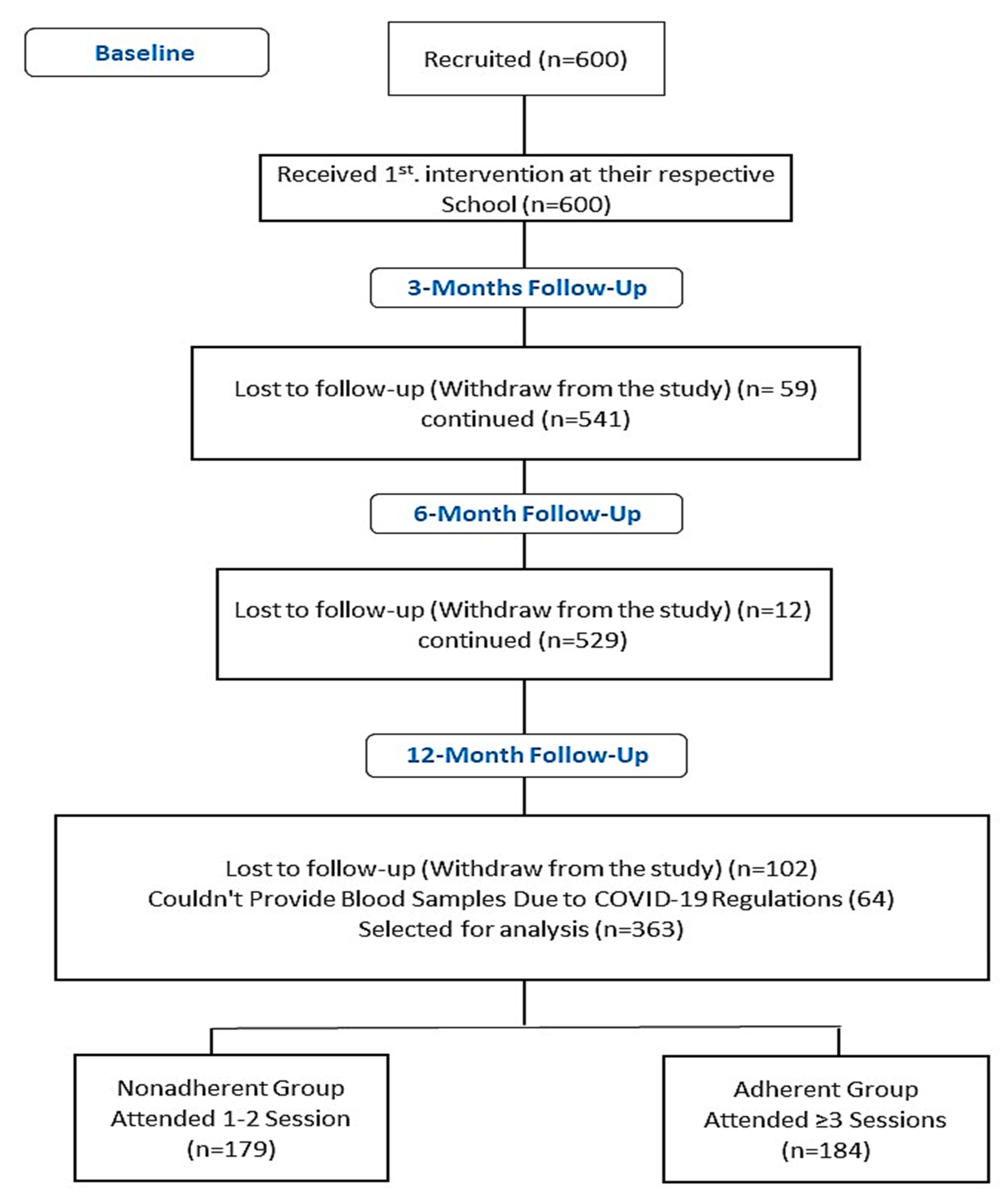
2.1. Participants
2.2. Intervention
2.3. Anthropometrics and Biochemical Parameters
2.4. Obesity and Hypertension Cut-Offs
2.5. Statistical Analysis
3. Results
3.1. Comparison of Clinical Characteristics in Adherent and Nonadherent Groups after 12-Month Follow-Up
3.2. Primary Outcomes
3.3. Pre- and Post-Intervention Comparison of Overweigh and Obese Participants in Both Groups
3.4. Pre- and Post-Intervention Comparison of Overweigh Participants in Both Groups
3.5. Pre- and Post-Intervention Comparison of Obese Participants in Both Groups
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Noncommunicable Diseases. Available online: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (accessed on 15 June 2023).
- Turer, C.B.; Brady, T.M.; de Ferranti, S.D. Obesity, Hypertension, and Dyslipidemia in Childhood Are Key Modifiable Antecedents of Adult Cardiovascular Disease: A Call to Action. Circulation 2018, 3, 1256–1259. [Google Scholar] [CrossRef] [PubMed]
- Charakida, M.; Deanfield, J.E. BMI Trajectories from Childhood: The Slippery Slope to Adult Obesity and Cardiovascular Disease. Eur. Heart J. 2018, 39, 2271–2273. [Google Scholar] [CrossRef] [PubMed]
- Bjerregaard, L.G.; Baker, J.L. Change in Overweight from Childhood to Early Adulthood and Risk of Type 2 Diabetes. New Engl. J. Med. 2018, 378, 2537–2538. [Google Scholar] [CrossRef] [PubMed]
- Reilly, J.J.; Kelly, J. Long-Term Impact of Overweight and Obesity in Childhood and Adolescence on Morbidity and Premature Mortality in Adulthood: Systematic Review. Int. J. Obes. 2011, 35, 891–898. [Google Scholar] [CrossRef]
- Smith, J.D.; Fu, E.; Kobayashi, M.A. Prevention and Management of Childhood Obesity and Its Psychological and Health Comorbidities. Annu. Rev. Clin. Psychol. 2020, 16, 351–378. [Google Scholar] [CrossRef]
- Al-Daghri, N.M.; Al-Attas, O.S.; Alokail, M.; Alkharfy, K.; Wani, K.; Amer, O.E.; Ul Haq, S.; Rahman, S.; Alnaami, A.M.; Livadas, S.; et al. Does visceral adiposity index signify early metabolic risk in children and adolescents? Association with insulin resistance, adipokines, and subclinical inflammation. Pediatr. Res. 2014, 75, 459–463. [Google Scholar] [CrossRef]
- Hamilton, D.; Dee, A.; Perry, I.J. The Lifetime Costs of Overweight and Obesity in Childhood and Adolescence: A Systematic Review. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2018, 19, 452–463. [Google Scholar] [CrossRef]
- Simmonds, M.; Llewellyn, A.; Owen, C.G.; Woolacott, N. Predicting Adult Obesity from Childhood Obesity: A Systematic Review and Meta-Analysis. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2016, 17, 95–107. [Google Scholar] [CrossRef]
- Mistry, S.K.; Puthussery, S. Risk factors of overweight and obesity in childhood and adolescence in South Asian countries: A systematic review of the evidence. Public Health 2015, 129, 200–209. [Google Scholar] [CrossRef]
- Luca, A.-C.; Curpan, A.-S.; Braha, E.E.; Ţarcă, E.; Iordache, A.-C.; Luca, F.-A.; Adumitrachioaiei, H. Increasing Trends in Obesity-Related Cardiovascular Risk Factors in Romanian Children and Adolescents—Retrospective Study. Healthcare 2022, 10, 2452. [Google Scholar] [CrossRef]
- Di Sessa, A.; Umano, G.R.; Miraglia Del Giudice, E.; Santoro, N. From the Liver to the Heart: Cardiac Dysfunction in Obese Children with Non-Alcoholic Fatty Liver Disease. World J. Hepatol. 2017, 9, 69–73. [Google Scholar] [CrossRef] [PubMed]
- Liang, Y.; Qi, Y. Developmental trajectories of adolescent overweight/obesity in China: Socio-economic status correlates and health consequences. Public Health 2020, 185, 246–253. [Google Scholar] [CrossRef]
- Shatat, I.F.; Brady, T.M. Editorial: Pediatric Hypertension: Update. Front. Pediatr. 2018, 6, 209. [Google Scholar] [CrossRef] [PubMed]
- Valerio, G.; Maffeis, C.; Saggese, G.; Ambruzzi, M.A.; Balsamo, A.; Bellone, S.; Bergamini, M.; Bernasconi, S.; Bona, G.; Calcaterra, V.; et al. Diagnosis, Treatment and Prevention of Pediatric Obesity: Consensus Position Statement of the Italian Society for Pediatric Endocrinology and Diabetology and the Italian Society of Pediatrics. Ital. J. Pediatr. 2018, 44, 88. [Google Scholar] [CrossRef]
- World Health Organization. Noncommunicable Diseases Country Profiles. 2014. Available online: https://apps.who.int/iris/handle/10665/128038 (accessed on 12 November 2022).
- Almughamisi, M. The Co-Development of a School-Based Nutrition Intervention to Prevent Childhood Obesity in Jeddah, Saudi Arabia. Ph.D. Thesis, King’s College, London, UK, 2021. [Google Scholar]
- Aboul-Enein, B.H.; Bernstein, J.; Neary, A.C. Dietary Transition and Obesity in Selected Arabicspeaking Countries: A Review of the Current Evidence. East. Mediterr. Health J. 2017, 22, 763–770. [Google Scholar] [CrossRef]
- NICE. Obesity: Identification, Assessment and Management. Clinical Guideline [CG189]. 2014. Available online: https://www.nice.org.uk/guidance/cg189 (accessed on 21 July 2023).
- Gungor, N.K. Overweight and obesity in children and adolescents. J. Clin. Res. Pediatr. Endocrinol. 2014, 6, 129–143. [Google Scholar] [CrossRef] [PubMed]
- Almughamisi, M.; O’Keeffe, M.; Harding, S. Adolescent Obesity Prevention in Saudi Arabia: Co-Identifying Actionable Priorities for Interventions. Front. Public Health 2022, 10, 863765. [Google Scholar] [CrossRef]
- Kalarchian, M.A.; Levine, M.D.; Arslanian, S.A.; Ewing, L.J.; Houck, P.R.; Cheng, Y.; Ringham, R.M.; Sheets, C.A.; Marcus, M.D. Family-Based Treatment of Severe Pediatric Obesity: Randomized, Controlled Trial. Pediatrics 2009, 124, 1060–1068. [Google Scholar] [CrossRef]
- Theim, K.R.; Sinton, M.M.; Goldschmidt, A.B.; Van Buren, D.J.; Doyle, A.C.; Saelens, B.E.; Stein, R.I.; Epstein, L.H.; Wilfley, D.E. Adherence to Behavioral Targets and Treatment Attendance during a Pediatric Weight Control Trial. Obesity 2013, 21, 394–397. [Google Scholar] [CrossRef]
- Brady, T.M. Obesity-Related Hypertension in Children. Front. Pediatr. 2017, 5, 197. [Google Scholar] [CrossRef]
- Friedemann, C.; Heneghan, C.; Mahtani, K.; Thompson, M.; Perera, R.; Ward, A.M. Cardiovascular disease risk in healthy children and its association with body mass index: Systematic review and meta-analysis. BMJ 2012, 345, e4759. [Google Scholar] [CrossRef] [PubMed]
- Reinehr, T.; Schaefer, A.; Winkel, K.; Finne, E.; Toschke, A.M.; Kolip, P. An effective lifestyle intervention in overweight children: Findings from a randomized controlled trial on “Obeldicks light”. Clin. Nutr. 2010, 29, 331–336. [Google Scholar] [CrossRef]
- Herouvi, D.; Paltoglou, G.; Soldatou, A.; Kalpia, C.; Karanasios, S.; Karavanaki, K. Lifestyle and Pharmacological Interventions and Treatment Indications for the Management of Obesity in Children and Adolescents. Children 2023, 10, 1230. [Google Scholar] [CrossRef] [PubMed]
- Scotto di Luzio, S.; Martinent, G.; Popa-Roch, M.; Ballereau, M.; Chahdi, S.; Escudero, L.; Guillet-Descas, E. Obesity in Childhood and Adolescence: The Role of Motivation for Physical Activity, Self-Esteem, Implicit and Explicit Attitudes toward Obesity and Physical Activity. Children 2023, 10, 1177. [Google Scholar] [CrossRef] [PubMed]
- Al-Hamdan, R.; Avery, A.; Al-Disi, D.; Sabico, S.; Al-Daghri, N.M.; McCullough, F. Efficacy of lifestyle intervention program for Arab women with prediabetes using social media as an alternative platform of delivery. J. Diabetes Investig. 2021, 12, 1872–1880. [Google Scholar] [CrossRef]
- Wani, K.; Alfawaz, H.; Alnaami, A.M.; Sabico, S.; Khattak, M.N.K.; Al-Attas, O.; Alokail, M.S.; Alharbi, M.; Chrousos, G.; Kumar, S.; et al. Effects of a 12-Month Intensive Lifestyle Monitoring Program in Predominantly Overweight/Obese Arab Adults with Prediabetes. Nutrients 2020, 12, 464. [Google Scholar] [CrossRef]
- Al Enazi, S.; Al Ajlan, R.; Al Khalaf, H.; Abolfotouh, M.; Alharbi, O.; Alfawaz, R.; Aldebasi, B.; Alghnam, S. Prevalence of Obesity among Children and Adolescents in Saudi Arabia: A Multicenter Population-Based Study. Saudi J. Med. Med. Sci. 2023, 11, 19–25. [Google Scholar] [PubMed]
- El-Setouhy, M.; Safhi, A.M.; Dallak, M.Y.; Ayoub, A.Y.; Suwaid, O.A.H.; Moafa, A.K.; Al-Ahmed, A.M.; Zaino, M.; Al Sayed, A. Prevalence and associated factors of pediatric hypertension in Jazan region, south of the Kingdom of Saudi Arabia. A pilot cross-sectional study. PLoS ONE 2023, 18, e0287698. [Google Scholar] [CrossRef]
- Al-Daghri, N.M.; Amer, O.E.; Hameidi, A.; Alfawaz, H.; Alharbi, M.; Khattak, M.N.K.; Alnaami, A.M.; Aljohani, N.J.; Alkhaldi, G.; Wani, K.; et al. Effects of a 12-Month Hybrid (In-Person + Virtual) Education Program in the Glycemic Status of Arab Youth. Nutrients 2022, 14, 1759. [Google Scholar] [CrossRef]
- Al-Daghri, N.M.; Wani, K.; Khattak, M.N.K.; Alnaami, A.M.; Amer, O.E.; Aljohani, N.J.; Hameidi, A.; Alfawaz, H.; Alharbi, M.; Sabico, S. Cardiometabolic Effects of a 12-Month, COVID-19 Lockdown-Interrupted Lifestyle Education Program for Arab Adolescents. Front Pediatr. 2022, 10, 887138. [Google Scholar] [CrossRef]
- Amer, O.E.; Sabico, S.; Khattak, M.N.K.; Alnaami, A.M.; Aljohani, N.J.; Alfawaz, H.; AlHameidi, A.; Al-Daghri, N.M. Increasing Prevalence of Pediatric Metabolic Syndrome and Its Components among Arab Youth: A Time-Series Study from 2010–2019. Children 2021, 8, 1129. [Google Scholar] [CrossRef] [PubMed]
- Al-Daghri, N.M.; Al-Othman, A.; Albanyan, A.; Al-Attas, O.S.; Alokail, M.S.; Sabico, S.; Chrousos, G.P. Perceived stress scores among Saudi students entering universities: A prospective study during the first year of university life. Int. J. Environ. Res. Public Health 2014, 11, 3972–3981. [Google Scholar] [CrossRef]
- US Preventive Services Task Force; Grossman, D.C.; Bibbins-Domingo, K.; Curry, S.J.; Barry, M.J.; Davidson, K.W.; Doubeni, C.A.; Epling, J.W., Jr.; Kemper, A.R.; Krist, A.H.; et al. Screening for Obesity in Children and Adolescents: US Preventive Services Task Force Recommendation Statement. JAMA 2017, 317, 2417–2426. [Google Scholar] [CrossRef] [PubMed]
- Flynn, J.T.; Kaelber, D.C.; Baker-Smith, C.M.; Blowey, D.; Carroll, A.E.; Daniels, S.R.; de Ferranti, S.D.; Dionne, J.M.; Falkner, B.; Flinn, S.K.; et al. Clinical Practice Guideline for Screening and Management of High Blood Pressure in Children and Adolescents. Pediatrics 2017, 140, e20171904. [Google Scholar] [CrossRef]
- Berkowitz, R.I.; Rukstalis, M.R.; Bishop-Gilyard, C.T.; Moore, R.H.; Gehrman, C.A.; Xanthopoulos, M.S.; Cochran, W.J.; Louden, D.; Wadden, T.A. Treatment of Adolescent Obesity Comparing Self-Guided and Group Lifestyle Modification Programs: A Potential Model for Primary Care. J. Pediatr. Psychol. 2013, 38, 978–986. [Google Scholar] [CrossRef] [PubMed]
- Reinehr, T.; de Sousa, G.; Toschke, A.M.; Andler, W. Long-term follow-up of cardiovascular disease risk factors in children after an obesity intervention. Am. J. Clin. Nutr. 2006, 84, 490–496. [Google Scholar] [CrossRef] [PubMed]
- Martinovic, M.; Belojevic, G.; Evans, G.W.; Kavaric, N.; Asanin, B.; Pantovic, S.; Jaksic, M.; Boljevic, J. Hypertension and correlates among Montenegrin schoolchildren—A cross-sectional study. Public Health 2017, 147, 15–19. [Google Scholar] [CrossRef] [PubMed]
- Novotny, R.; Nigg, C.R.; Li, F.; Wilkens, L.R. Pacific Kids DASH for Health (PacDASH) Randomized, Controlled Trial with DASH Eating Plan plus Physical Activity Improves Fruit and Vegetable Intake and Diastolic Blood Pressure in Children. Child. Obes. 2015, 11, 177–186. [Google Scholar] [CrossRef]
- Al Salloum, A.A.; El Mouzan, M.I.; Al Herbish, A.S.; Al Omar, A.A.; Qurashi, M.M. Blood Pressure Standards for Saudi Children and Adolescents. Ann. Saudi Med. 2009, 29, 173–178. [Google Scholar] [CrossRef]
- Kim, J.; Kim, Y.; Seo, Y.-G.; Park, K.-H.; Jang, H.B.; Lee, H.-J.; Park, S.I.; Lim, H. Evidence-Based Customized Nutritional Intervention Improves Body Composition and Nutritional Factors for Highly-Adherent Children and Adolescents with Moderate to Severe Obesity. Nutr. Res. Pract. 2020, 14, 262–275. [Google Scholar] [CrossRef]
- Parker, E.D.; Sinaiko, A.R.; Kharbanda, E.O.; Margolis, K.L.; Daley, M.F.; Trower, N.K.; Sherwood, N.E.; Greenspan, L.C.; Lo, J.C.; Magid, D.J.; et al. Change in weight status and development of hypertension. Pediatrics 2016, 137, e20151662. [Google Scholar] [CrossRef] [PubMed]
- Monzavi, R.; Dreimane, D.; Geffner, M.E.; Braun, S.; Conrad, B.; Klier, M.; Kaufman, F.R. Improvement in Risk Factors for Metabolic Syndrome and Insulin Resistance in Overweight Youth Who Are Treated with Lifestyle Intervention. Pediatrics 2006, 117, e1111–e1118. [Google Scholar] [CrossRef] [PubMed]
- Chung, S.J. Effect of Physical Activity on Adolescent Obesity Status over Time: A Latent Growth Modeling Approach. Healthcare 2021, 9, 1018. [Google Scholar] [CrossRef]
- Markert, J.; Herget, S.; Petroff, D.; Gausche, R.; Grimm, A.; Kiess, W.; Blüher, S. Telephone-based adiposity prevention for families with overweight children (T.A.F.F.-Study): One year outcome of a randomized, controlled trial. Int. J. Environ. Res. Public Health 2014, 11, 10327–10344. [Google Scholar] [CrossRef] [PubMed]
- Lobstein, T.; Baur, L.; Uauy, R. IASO International Obesity TaskForce. Obesity in children and young people: A crisis in public health. Obes. Rev. 2004, 5 (Suppl. S1), 4–104. [Google Scholar] [CrossRef] [PubMed]
- Cole, T.J.; Faith, M.S.; Pietrobelli, A.; Heo, M. What is the best measure of adiposity change in growing children: BMI, BMI %, BMI z-score or BMI centile? Eur. J. Clin. Nutr. 2005, 59, 419–425, Erratum in Eur. J. Clin. Nutr. 2005, 59, 807. [Google Scholar] [CrossRef]
- Yang, X.Y.; Gong, R.N.; Sassine, S.; Morsa, M.; Tchogna, A.S.; Drouin, O.; Chadi, N.; Jantchou, P. Risk Perception of COVID-19 Infection and Adherence to Preventive Measures among Adolescents and Young Adults. Children 2020, 7, 311. [Google Scholar] [CrossRef]
- Griffith, D.M.; Sharma, G.; Holliday, C.S.; Enyia, O.K.; Valliere, M.; Semlow, A.R.; Stewart, E.C.; Blumenthal, R.S. Men and COVID-19: A Biopsychosocial Approach to Understanding Sex Differences in Mortality and Recommendations for Practice and Policy Interventions. Prev. Chronic Dis. 2020, 17, E63. [Google Scholar] [CrossRef]
- Holt, E.; Joyce, C.; Dornelles, A.; Morisky, D.; Webber, L.S.; Muntner, P.; Krousel-Wood, M. Sex Differences in Barriers to Antihypertensive Medication Adherence: Findings from the Cohort Study of Medication Adherence among Older Adults. J. Am. Geriatr. Soc. 2013, 61, 558–564. [Google Scholar] [CrossRef]
- Qi, Y.; Lv, R.; Zhao, M.; Huang, Y.; Zhang, Y.; Zhang, H.; Song, P.; Li, Z.; Jia, P.; Zhang, H.; et al. Associations between parental adherence to healthy lifestyles and risk of obesity in offspring: A prospective cohort study in China. Lancet Glob. Health 2023, 11 (Suppl. S1), S6. [Google Scholar] [CrossRef]
- Ghofranipour, F.; Hamzavi Zarghani, N.; Mohammadi, E.; Mehrizi, A.A.H.; Tavousi, M.; De Craemer, M.; Cardon, G. An internet-based educational intervention for mothers targeting preschoolers’ weight management promotion (PWMP): A pilot study. BMC Public Health 2022, 22, 2220. [Google Scholar] [CrossRef] [PubMed]
- Chai, L.K.; Farletti, R.; Fathi, L.; Littlewood, R. A Rapid Review of the Impact of Family-Based Digital Interventions for Obesity Prevention and Treatment on Obesity-Related Outcomes in Primary School-Aged Children. Nutrients 2022, 14, 4837. [Google Scholar] [CrossRef] [PubMed]
- Varagiannis, P.; Magriplis, E.; Risvas, G.; Vamvouka, K.; Nisianaki, A.; Papageorgiou, A.; Pervanidou, P.; Chrousos, G.P.; Zampelas, A. Effects of Three Different Family-Based Interventions in Overweight and Obese Children: The “4 Your Family” Randomized Controlled Trial. Nutrients 2021, 13, 341. [Google Scholar] [CrossRef] [PubMed]
- Conn, V.S.; Ruppar, T.M.; Chase, J.-A.D.; Enriquez, M.; Cooper, P.S. Interventions to Improve Medication Adherence in Hypertensive Patients: Systematic Review and Meta-Analysis. Curr. Hypertens. Rep. 2015, 17, 94. [Google Scholar] [CrossRef]
- Conn, V.S.; Ruppar, T.M.; Enriquez, M.; Cooper, P. Medication Adherence Interventions that Target Subjects with Adherence Problems: Systematic Review and Meta-Analysis. Res. Social Adm. Pharm. 2016, 12, 218–246. [Google Scholar] [CrossRef]
- Hugtenburg, J.G.; Timmers, L.; Elders, P.J.; Vervloet, M.; van Dijk, L. Definitions, Variants, and Causes of Nonadherence with Medication: A Challenge for Tailored Interventions. Patient Prefer. Adherence 2013, 7, 675–682. [Google Scholar] [CrossRef]
- Sabico, S.; Al-Mashharawi, A.; Al-Daghri, N.M.; Wani, K.; Amer, O.E.; Hussain, D.S.; Ahmed Ansari, M.G.; Masoud, M.S.; Alokail, M.S.; McTernan, P.G. Effects of a 6-month multi-strain probiotics supplementation in endotoxemic, inflammatory and cardiometabolic status of T2DM patients: A randomized, double-blind, placebo-controlled trial. Clin. Nutr. 2019, 38, 1561–1569. [Google Scholar] [CrossRef]
- Amer, O.E.; Sabico, S.; Alfawaz, H.A.; Aljohani, N.; Hussain, S.D.; Alnaami, A.M.; Wani, K.; Al-Daghri, N.M. Reversal of Prediabetes in Saudi Adults: Results from an 18 Month Lifestyle Intervention. Nutrients 2020, 12, 804. [Google Scholar] [CrossRef]
- Schienkiewitz, A.; Truthmann, J.; Ernert, A.; Wiegand, S.; Schwab, K.O.; Scheidt-Nave, C. Age, maturation and serum lipid parameters: Findings from the German Health Survey for Children and Adolescents. BMC Public Health 2019, 19, 1627. [Google Scholar] [CrossRef]
- Maidowski, L.; Kiess, W.; Baber, R.; Dathan-Stumpf, A.; Ceglarek, U.; Vogel, M. Tracking of serum lipids in healthy children on a year-to-year basis. BMC Cardiovasc. Disord. 2023, 23, 386. [Google Scholar] [CrossRef]
- Mann, J.I. Evidence-Based Nutrition Recommendations for the Treatment and Prevention of Type 2 Diabetes and the Metabolic Syndrome. Food Nutr. Bull. 2006, 27, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Conn, V.S.; Hafdahl, A.R.; Mehr, D.R.; LeMaster, J.W.; Brown, S.A.; Nielsen, P.J. Metabolic Effects of Interventions to Increase Exercise in Adults with Type 2 Diabetes. Diabetologia 2007, 50, 913–921. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Muñoz, S.; Corella, C.; Abarca-Sos, A.; Zaragoza, J. Validation of three short physical activity questionnaires with accelerometers among university students in Spain. J. Sports Med. Phys. Fit. 2017, 57, 1660–1668. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Parameters | Overall | |||||
|---|---|---|---|---|---|---|
| Nonadherent | p-Value | Adherent | p-Value | |||
| Baseline | Follow-Up | Baseline | Follow-Up | |||
| N | 179 | 184 | ||||
| Age | 14.97 ± 1.6 | 14.89 ± 1.7 | ||||
| Weight (Kg) | 58.2 ± 18.3 | 60.6 ± 17.2 | <0.001 | 58.3 ± 17.5 | 60.2 ± 15.5 | <0.001 |
| BMI (kg/m2) | 22.9 ± 5.9 | 22.1 ± 5.9 | <0.001 | 23.82 ± 6.1 | 22.10 ± 5.6 | <0.001 |
| BMI Z-score | −0.015 ± 0.98 | 0.093 ± 1.05 | 0.007 | 0.117 ± 1.0 | 0.069 ± 0.96 | 0.09 |
| Waist (cm) | 75.0 ± 17.3 | 85.6 ± 10.4 | <0.001 | 74.2 ± 14.6 | 73.4 ± 15.6 | 0.29 |
| Hip (cm) | 81.6 ± 23.6 | 92.3 ± 11.6 | <0.001 | 88.8 ± 16.1 | 80.6 ± 15.0 | <0.001 |
| WHR | 0.86 ± 0.10 | 0.92 ± 0.10 | <0.001 | 0.84 ± 0.12 | 0.91 ± 0.07 | <0.001 |
| SBP (mmHg) | 120.6 ± 13.5 | 116.6 ± 8.7 | 0.003 | 121.2 ± 16.4 | 106.1 ± 13.6 | <0.001 |
| DBP (mmHg) | 68.7 ± 8.8 | 75.7 ± 7.1 | <0.001 | 72.9 ± 11.6 | 71.7 ± 6.5 | 0.12 |
| Glucose (mmol/L) | 5.3 ± 1.0 | 5.6 ± 2.2 | 0.03 | 5.2 ± 0.6 | 5.5 ± 2.3 | 0.06 |
| HbA1c (%) | 5.2 ± 0.6 | 5.3 ± 1.1 | 0.04 | 5.1 ± 0.6 | 5.3 ± 1.3 | 0.007 |
| TC (mmol/L) | 4.4 ± 0.8 | 6.0 ± 1.2 | <0.001 | 4.4 ± 0.7 | 5.8 ± 1.4 | <0.001 |
| HDL-c (mmol/L) | 1.0 ± 0.2 | 1.5 ± 0.5 | 0.001 | 0.95 ± 0.3 | 1.5 ± 0.6 | <0.001 |
| LDL-c (mmol/L) | 2.9 ± 0.7 | 3.7 ± 1.1 | <0.001 | 3.0 ± 0.6 | 3.7 ± 1.2 | <0.001 |
| TG (mmol/L) | 1.1 ± 0.5 | 1.8 ± 0.8 | <0.001 | 1.1 ± 0.6 | 1.7 ± 0.8 | <0.001 |
| Group (Total N) | Baseline | Follow-Up | p-Value |
|---|---|---|---|
| Overall (N = 363) | 69 (19) | 51 (14) | 0.16 |
| Nonadherent (N = 179) | 21 (12) | 31 (17) | 0.23 |
| Adherent (N = 184) | 48 (26) | 20 (11) | 0.003 |
| Normal body weight (N = 223) | |||
| Nonadherent (N = 122) | 9 (7) | 17 (14) | 0.15 |
| Adherent (N = 101) | 23 (23) | 14 (14) | 0.18 |
| Overweight (N = 72) | |||
| Nonadherent (N = 28) | 6 (21) | 7 (25) | 0.73 |
| Adherent (N = 44) | 10 (23) | 4 (9) | 0.18 |
| Obese (N = 68) | |||
| Nonadherent (N = 29) | 6 (25) | 4 (14) | 0.73 |
| Adherent (N = 39) | 15 (38) | 5 (13) | 0.03 |
| Parameters | Overall Overweight & Obese | Nonadherent | Adherent | p * | p ** | p *** | |||
|---|---|---|---|---|---|---|---|---|---|
| Baseline | Follow-Up | Baseline | Follow-Up | Baseline | Follow-Up | ||||
| N (M/F) | 140 (89/51) | 57 (51/6) | 83 (38/45) | ||||||
| Age (years) | 15.0 ± 1.7 | 15.2 ± 1.7 | 14.9 ± 1.6 | 0.35 | |||||
| Weight (kg) | 74.5 ± 15.1 | 74.9 ± 13.8 | 77.1 ± 15.9 | 78.4 ± 15.0 ** | 73.2 ± 14.5 | 73.1 ± 12.8 | 0.08 | 0.28 | 0.17 |
| BMI (kg/m2) | 29.5 ± 4.5 | 27.2 ± 4.8 ** | 29.8 ± 4.4 | 28.2 ± 4.9 ** | 29.3 ± 4.5 | 26.6 ± 4.7 ** | 0.35 | 0.15 | 0.18 |
| BMI Z-score | 1.1 ± 0.7 | 0.99 ± 0.8 * | 1.2 ± 0.7 | 1.2 ± 0.9 | 1.05 ± 0.75 | 0.87 ± 0.80 ** | 0.22 | 0.13 | 0.18 |
| Waist (cm) | 81.9 ± 18.6 | 80.3 ± 15.2 | 81.3 ± 21.8 | 88.7 ± 9.5 * | 82.2 ± 16.7 | 75.7 ± 15.9 ** | <0.001 | <0.001 | 0.02 |
| Hip (cm) | 95.1 ± 21.3 | 86.9 ± 14.5 ** | 90.6 ± 25.6 | 94.6 ± 10.4 | 97.4 ± 18.4 | 82.7 ± 14.9 ** | 0.002 | <0.001 | 0.03 |
| WHR | 0.85 ± 0.10 | 0.92 ± 0.05 ** | 0.88 ± 0.10 | 0.93 ± 0.04 ** | 0.84 ± 0.10 | 0.92 ± 0.06 ** | 0.46 | 0.15 | 0.95 |
| SBP (mmHg) | 125.7 ± 15.4 | 110.9 ± 12.6 ** | 125.5 ± 13.0 | 117.0 ± 8.3 ** | 125.9 ± 16.6 | 107.6 ± 13.4 ** | 0.02 | <0.001 | 0.26 |
| DBP (mmHg) | 72.5 ± 11.1 | 74.2 ± 7.2 | 69.6 ± 9.9 | 76.9 ± 7.4 ** | 74.1 ± 11.5 | 72.8 ± 6.8 | <0.001 | <0.001 | 0.095 |
| Glucose (mmol/L) | 5.4 ± 1.1 | 5.8 ± 2.7 | 5.6 ± 1.7 | 5.8 ± 2.1 | 5.3 ± 0.6 | 5.9 ± 3.0 | 0.89 | 0.71 | 0.95 |
| HbA1c (%) | 5.2 ± 0.7 | 5.5 ± 1.6 | 5.3 ± 0.7 | 5.2 ± 0.9 | 5.2 ± 0.7 | 5.6 ± 1.8 | 0.06 | 0.03 | 0.50 |
| TC (mmol/L) | 4.6 ± 0.7 | 6.0 ± 1.4 ** | 4.6 ± 0.8 | 6.1 ± 1.2 ** | 4.6 ± 0.7 | 5.9 ± 1.5 ** | <0.001 | 0.047 | 0.46 |
| HDL-c (mmol/L) | 0.9 ± 0.3 | 1.4 ± 0.6 ** | 1.0 ± 0.2 | 1.5 ± 0.4 ** | 0.9 ± 0.3 | 1.4 ± 0.6 ** | 0.002 | <0.001 | 0.04 |
| LDL-c (mmol/L) | 3.1 ± 0.7 | 3.8 ± 1.2 ** | 3.1 ± 0.8 | 3.8 ± 1.0 ** | 3.1 ± 0.6 | 3.8 ± 1.3 ** | <0.001 | <0.001 | 0.06 |
| TG (mmol/L) | 1.2 ± 0.6 | 1.7 ± 0.8 ** | 1.3 ± 0.8 | 1.9 ± 0.7 ** | 1.2 ± 0.6 | 1.7 ± 0.9 ** | 0.002 | 0.12 | 0.84 |
| Parameters | Overall Overweight | Nonadherent | Adherent | p * | p ** | p *** | |||
|---|---|---|---|---|---|---|---|---|---|
| Baseline | Follow-Up | Baseline | Follow-Up | Baseline | Follow-Up | ||||
| N (M/F) | 72 (38/34) | 28 (22/6) | 44 (16/28) | ||||||
| Age (years) | 15.2 ± 1.7 | 15.3 ± 1.8 | 15.1 ± 1.6 | 0.66 | |||||
| Weight (kg) | 64.4 ± 10.3 | 65.9 ± 9.5 ** | 66.3 ± 10.3 | 68.2 ± 9.5 ** | 63.5 ± 10.3 | 64.7 ± 9.3 * | 0.001 | 0.04 | 0.94 |
| BMI (kg/m2) | 26.0 ± 1.7 | 24.0 ± 3.2 ** | 26.4 ± 1.6 | 24.8 ± 3.3 ** | 25.8 ± 1.8 | 23.6 ± 3.1 ** | 0.35 | 0.51 | 0.49 |
| BMI Z-score | 0.54 ± 0.30 | 0.47 ± 0.58 | 0.63 ± 0.27 | 0.67 ± 0.605 | 0.50 ± 0.31 | 0.40 ± 0.55 | 0.50 | 0.43 | 0.41 |
| Waist (cm) | 74.6 ± 17.1 | 78.1 ± 15.4 | 69.8 ± 21.3 | 88.6 ± 9.4 | 77.2 ± 13.9 | 72.3 ± 15.0 | <0.001 | 0.02 | 0.28 |
| Hip (cm) | 89.8 ± 20.4 | 85.1 ± 14.9 | 82.3 ± 25.6 | 95.9 ± 11.2 ** | 93.7 ± 16.1 | 79.4 ± 13.6 ** | <0.001 | <0.001 | 0.007 |
| WHR | 0.8 ± 0.11 | 0.9 ± 0.06 ** | 0.8 ± 0.07 | 0.9 ± 0.04 * | 0.83 ± 0.12 | 0.91 ± 0.07 ** | 0.29 | 0.47 | 0.54 |
| SBP (mmHg) | 124.0 ± 15.4 | 109.1 ± 12.5 ** | 124.4 ± 11.8 | 116.9 ± 9.2 * | 123.8 ± 16.9 | 105.1 ± 12.1 ** | 0.18 | 0.003 | 0.15 |
| DBP (mmHg) | 70.9 ± 10.9 | 73.8 ± 7.8 | 69.3 ± 10.5 | 75.4 ± 8.1 * | 71.8 ± 11.2 | 72.9 ± 7.6 | 0.003 | 0.02 | 0.77 |
| Glucose (mmol/L) | 5.4 ± 1.5 | 5.7 ± 2.4 | 5.8 ± 2.3 | 5.7 ± 2.4 | 5.2 ± 0.7 | 5.63 ± 2.4 | 0.52 | 0.39 | 0.88 |
| HbA1c (%) | 5.2 ± 0.8 | 5.3 ± 1.3 | 5.3 ± 0.9 | 5.2 ± 0.8 | 5.2 ± 0.7 | 5.37 ± 1.5 | 0.001 | 0.001 | 0.83 |
| TC (mmol/L) | 4.5 ± 0.8 | 5.8 ± 1.2 ** | 4.4 ± 0.8 | 5.7 ± 1.1 ** | 4.6 ± 0.8 | 5.86 ± 1.3 ** | 0.001 | 0.13 | 0.32 |
| HDL-c (mmol/L) | 0.9 ± 0.3 | 1.6 ± 0.5 ** | 1.0 ± 0.2 | 1.6 ± 0.3 ** | 0.9 ± 0.3 | 1.56 ± 0.6 ** | 0.60 | 0.003 | 0.55 |
| LDL-c (mmol/L) | 3.1 ± 0.7 | 3.5 ± 1.1 ** | 2.9 ± 0.7 | 3.3 ± 1.04 | 3.2 ± 0.7 | 3.62 ± 1.1 * | <0.001 | 0.001 | 0.09 |
| TG (mmol/L) | 1.2 ± 0.7 | 1.6 ± 0.7 ** | 1.2 ± 0.5 | 1.7 ± 0.7 ** | 1.2 ± 0.7 | 1.6 ± 0.7 * | 0.22 | 0.82 | 0.79 |
| Parameters | Overall Overweight | Nonadherent | Adherent | p * | p ** | p *** | |||
|---|---|---|---|---|---|---|---|---|---|
| Baseline | Follow-Up | Baseline | Follow-Up | Baseline | Follow-Up | ||||
| N (M/F) | 68 (51/17) | 29 (29/0) | 39 (22/17) | ||||||
| Age (years) | 14.9 ± 1.7 | 15.1 ± 1.6 | 14.7 ± 1.7 | 0.34 | |||||
| Weight (kg) | 85.1 ± 11.6 | 84.5 ± 10.9 | 87.5 ± 13.4 | 88.2 ± 12.6 | 83.7 ± 10.4 | 82.3 ± 9.3 * | 0.53 | 0.45 | 0.16 |
| BMI (kg/m2) | 33.1 ± 3.4 | 30.5 ± 3.9 ** | 33.0 ± 3.7 | 31.5 ± 3.9 ** | 33.2 ± 3.3 | 30.0 ± 3.8 ** | 0.74 | 0.06 | 0.51 |
| BMI Z-score | 1.7 ± 0.58 | 1.6 ± 0.70 | 1.7 ± 0.63 | 1.8 ± 0.73 | 1.7 ± 0.6 | 1.5 ± 0.7 * | 0.13 | 0.08 | 0.55 |
| Waist (cm) | 89.2 ± 17.2 | 82.6 ± 14.9 * | 92.9 ± 15.6 | 88.8 ± 9.7 | 87.2 ± 17.9 | 79.1 ± 16.2 * | <0.001 | 0.001 | 0.62 |
| Hip (cm) | 100.6 ± 21.0 | 88.8 ± 14.1 ** | 99.0 ± 23.2 | 93.3 ± 9.7 | 101.4 ± 19.9 | 86.2 ± 15.6 | 0.06 | 0.008 | 0.87 |
| WHR | 0.9 ± 0.09 | 0.9 ± 0.04 ** | 0.9 ± 0.11 | 1.0 ± 0.02 | 0.8 ± 0.08 | 0.9 ± 0.05 | 0.73 | 0.47 | 0.30 |
| SBP (mmHg) | 127.6 ± 15.3 | 112.9 ± 12.6 ** | 126.6 ± 14.2 | 117.1 ± 7.5 ** | 128.2 ± 15.9 | 110.5 ± 14.3 ** | 0.002 | <0.001 | 0.43 |
| DBP (mmHg) | 74.1 ± 11.2 | 74.8 ± 6.6 | 69.9 ± 9.5 | 78.3 ± 6.4 ** | 76.6 ± 11.5 | 72.7 ± 5.9 * | <0.001 | 0.002 | 0.06 |
| Glucose (mmol/L) | 5.4 ± 0.5 | 6.0 ± 3.1 | 5.3 ± 0.5 | 5.8 ± 1.8 | 5.4 ± 0.5 | 6.1 ± 3.6 | 0.72 | 0.95 | 0.90 |
| HbA1c (%) | 5.2 ± 0.6 | 6.6 ± 1.8 | 5.3 ± 0.6 | 5.19 ± 0.9 | 5.22 ± 0.6 | 5.89 ± 2.1 | 0.79 | 0.96 | 0.23 |
| TC (mmol/L) | 4.7 ± 0.7 | 6.1 ± 1.6 ** | 4.9 ± 0.8 | 6.6 ± 1.1 ** | 4.6 ± 0.6 | 5.9 ± 1.7 ** | 0.006 | 0.37 | 0.94 |
| HDL-c (mmol/L) | 1.0 ± 0.2 | 1.3 ± 0.6 ** | 1.0 ± 0.11 | 1.4 ± 0.5 ** | 0.9 ± 0.3 | 1.2 ± 0.6 * | <0.001 | <0.001 | 0.002 |
| LDL-c (mmol/L) | 3.2 ± 0.7 | 4.1 ± 1.3 ** | 3.2 ± 0.8 | 4.3 ± 0.7 ** | 3.1 ± 0.6 | 4.0 ± 1.5 | <0.001 | 0.02 | 0.51 |
| TG (mmol/L) | 1.3 ± 0.6 | 1.9 ± 0.9 ** | 1.4 ± 0.7 | 2.0 ± 0.6 * | 1.2 ± 0.6 | 1.8 ± 1.10 ** | 0.002 | 0.04 | 0.37 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Daghri, N.M.; Amer, O.E.; Khattak, M.N.K.; Hussain, S.D.; Alkhaldi, G.; Alfawaz, H.A.; Elsaid, M.A.; Sabico, S. Attendance-Based Adherence and Outcomes of Obesity Management Program in Arab Adolescents. Children 2023, 10, 1449. https://doi.org/10.3390/children10091449
Al-Daghri NM, Amer OE, Khattak MNK, Hussain SD, Alkhaldi G, Alfawaz HA, Elsaid MA, Sabico S. Attendance-Based Adherence and Outcomes of Obesity Management Program in Arab Adolescents. Children. 2023; 10(9):1449. https://doi.org/10.3390/children10091449
Chicago/Turabian StyleAl-Daghri, Nasser M., Osama E. Amer, Malak N. K. Khattak, Syed D. Hussain, Ghadah Alkhaldi, Hanan A. Alfawaz, Mohamed A. Elsaid, and Shaun Sabico. 2023. "Attendance-Based Adherence and Outcomes of Obesity Management Program in Arab Adolescents" Children 10, no. 9: 1449. https://doi.org/10.3390/children10091449
APA StyleAl-Daghri, N. M., Amer, O. E., Khattak, M. N. K., Hussain, S. D., Alkhaldi, G., Alfawaz, H. A., Elsaid, M. A., & Sabico, S. (2023). Attendance-Based Adherence and Outcomes of Obesity Management Program in Arab Adolescents. Children, 10(9), 1449. https://doi.org/10.3390/children10091449