
Direct Parent Engagement to Improve Fundamental Movement Skills in Children: A Systematic Review



Abstract
1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Study Selection Criteria
2.3. Search Strategy
2.4. Study Quality Assessment
2.5. Analysis
3. Results
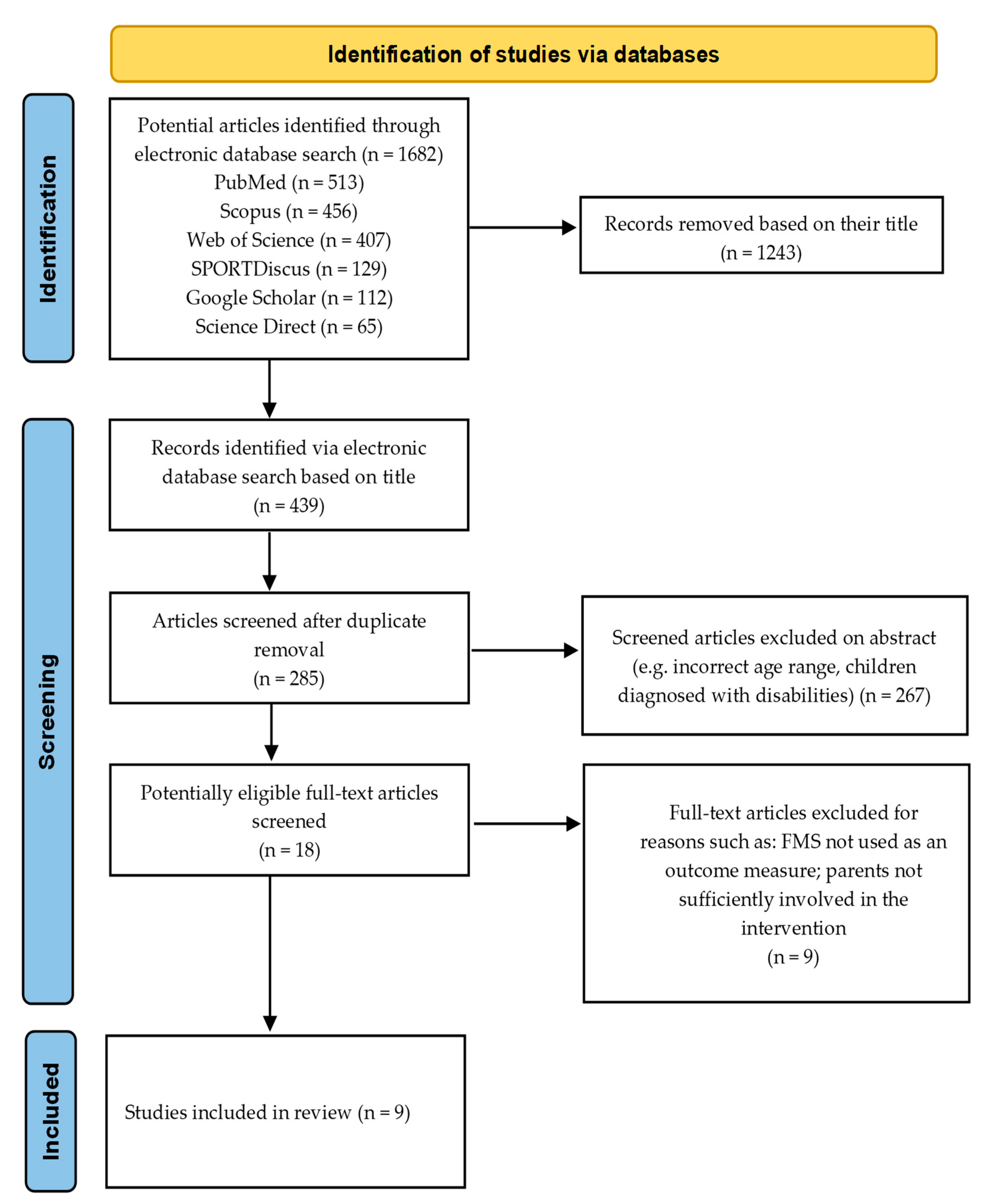
3.1. Study Selection
3.2. Origin and Participants
3.3. Study Design
3.4. Study Quality Assessment
3.5. Settings and Parental Involvement
3.6. Outcome Measures
3.7. Overall Findings
4. Discussion
4.1. Strengths and Limitations
4.2. Practical Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Seefeldt, V. Developmental motor patterns: Implications for elementary school physical education. Psychol. Mot. Behav. Sport 1980, 36, 314–323. [Google Scholar]
- Wick, K.; Leeger-Aschmann, C.S.; Monn, N.D.; Radtke, T.; Ott, L.V.; Rebholz, C.E.; Cruz, S.; Gerber, N.; Schmutz, E.A.; Puder, J.J.; et al. Interventions to promote fundamental movement skills in childcare and kindergarten: A systematic review and meta-analysis. Sports Med. 2017, 47, 2045–2068. [Google Scholar] [CrossRef]
- Rudd, J.R.; Barnett, L.M.; Butson, M.L.; Farrow, D.; Berry, J.; Polman, R.C. Fundamental movement skills are more than run, throw and catch: The role of stability skills. PLoS ONE 2015, 10, e0140224. [Google Scholar] [CrossRef] [PubMed]
- Foulkes, J.D.; Knowles, Z.; Fairclough, S.J.; Stratton, G.; O’Dwyer, M.; Ridgers, N.D.; Foweather, L. Fundamental movement skills of preschool children in Northwest England. Percept. Mot. Ski. 2015, 121, 260–283. [Google Scholar] [CrossRef] [PubMed]
- Morley, D.; Till, K.; Ogilvie, P.; Turner, G. Influences of gender and socioeconomic status on the motor proficiency of children in the UK. Hum. Mov. Sci. 2015, 44, 150–156. [Google Scholar] [CrossRef]
- Stodden, D.F.; Goodway, J.D.; Langendorfer, S.J.; Roberton, M.A.; Rudisill, M.E.; Garcia, C.; Garcia, L.E. A Developmental Perspective on the Role of Motor Skill Competence in Physical Activity: An Emergent Relationship. Quest 2008, 60, 290–306. [Google Scholar] [CrossRef]
- Lawson, C.; Eyre, E.L.; Tallis, J.; Duncan, M.J. Fundamental movement skill proficiency among British primary school children: Analysis at a behavioral component level. Percept. Mot. Ski. 2021, 128, 625–648. [Google Scholar] [CrossRef]
- Ali, A.; McLachlan, C.; Mugridge, O.; McLaughlin, T.; Conlon, C.; Clarke, L. The effect of a 10-week physical activity programme on fundamental movement skills in 3–4-year-old children within early childhood education centres. Children 2021, 8, 440. [Google Scholar] [CrossRef]
- Cohen, K.E.; Morgan, P.J.; Plotnikoff, R.C.; Callister, R.; Lubans, D.R. Fundamental movement skills and physical activity among children living in low-income communities: A cross-sectional study. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 49. [Google Scholar] [CrossRef]
- Holfelder, B.; Schott, N. Relationship of fundamental movement skills and physical activity in children and adolescents: A systematic review. Psychol. Sport Exerc. 2014, 15, 382–391. [Google Scholar] [CrossRef]
- Vandorpe, B.; Vandendriessche, J.; Vaeyens, R.; Pion, J.; Matthys, S.; Lefevre, J.; Philippaerts, R.; Lenoir, M. Relationship between sports participation and the level of motor coordination in childhood: A longitudinal approach. J. Sci. Med. Sport 2012, 15, 220–225. [Google Scholar] [CrossRef] [PubMed]
- Robinson, L.E.; Stodden, D.F.; Barnett, L.M.; Lopes, V.P.; Logan, S.W.; Rodrigues, L.P.; D’Hondt, E. Motor competence and its effect on positive developmental trajectories of health. Sports Med. 2015, 45, 1273–1284. [Google Scholar] [CrossRef] [PubMed]
- Bolger, L.E.; Bolger, L.A.; O’Neill, C.; Coughlan, E.; O’Brien, W.; Lacey, S.; Burns, C.; Bardid, F. Global levels of fundamental motor skills in children: A systematic review. J. Sports Sci. 2021, 39, 717–753. [Google Scholar] [CrossRef] [PubMed]
- Duncan, M.J.; Roscoe, C.M.; Noon, M.; Clark, C.C.; O’Brien, W.; Eyre, E.L. Run, jump, throw and catch: How proficient are children attending English schools at the fundamental motor skills identified as key within the school curriculum? Eur. Phys. Educ. Rev. 2020, 26, 814–826. [Google Scholar] [CrossRef]
- O’Brien, W.; Belton, S.; Issartel, J. Fundamental movement skill proficiency amongst adolescent youth. Phys. Educ. Sport Pedagog. 2016, 21, 557–571. [Google Scholar] [CrossRef]
- Dobell, A.; Pringle, A.; Faghy, M.A.; Roscoe, C.M. Fundamental Movement Skills and Accelerometer-Measured Physical Activity Levels during Early Childhood: A Systematic Review. Children 2020, 7, 224. [Google Scholar] [CrossRef]
- GOV.UK. Physical Activity Guidelines: Early Years (Under 5s). 2019. Available online: www.gov.uk (accessed on 14 May 2023).
- World Health Organisation. WHO Guidelines on Physical Activity and Sedentary Behaviour. 2020. Available online: https://www.who.int/publications/i/item/9789240015128 (accessed on 21 October 2022).
- Hallal, P.C.; Andersen, L.B.; Bull, F.C.; Guthold, R.; Haskell, W.; Ekelund, U. Lancet Physical Activity Series Working Group. Global physical activity levels: Surveillance progress, pitfalls, and prospects. Lancet 2012, 380, 247–257. [Google Scholar]
- Hardy, L.L.; Barnett, L.; Espinel, P.; Okely, A.D. Thirteen-year trends in child and adolescent fundamental movement skills: 1997–2010. Med. Sci. Sports Exerc. 2013, 45, 1965–1970. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Physical Activity Facts | Healthy Schools | CDC. 2022. Available online: https://www.cdc.gov/healthyschools/physicalactivity/facts.htm (accessed on 21 October 2022).
- Public Health England. Physical Activity Helps Children to Deal with Life’s Challenges. 2019. Available online: www.gov.uk (accessed on 14 September 2022).
- Tinner, L.; Kipping, R.; White, J.; Jago, R.; Metcalfe, C.; Hollingworth, W. Cross-sectional analysis of physical activity in 2–4-year-olds in England with paediatric quality of life and family expenditure on physical activity. BMC Public Health 2019, 19, 846. [Google Scholar]
- De Meester, A.; Stodden, D.; Goodway, J.; True, L.; Brian, A.; Ferkel, R.; Haerens, L. Identifying a motor proficiency barrier for meeting physical activity guidelines in children. J. Sci. Med. Sport 2018, 21, 58–62. [Google Scholar] [CrossRef]
- Cliff, D.P.; Okely, A.D.; Morgan, P.J.; Jones, R.A.; Steele, J.R.; Baur, L.A. Proficiency deficiency: Mastery of fundamental movement skills and skill components in overweight and obese children. Obesity 2012, 20, 1024–1033. [Google Scholar] [PubMed]
- Han, A.; Fu, A.; Cobley, S.; Sanders, R.H. Effectiveness of exercise intervention on improving fundamental movement skills and motor coordination in overweight/obese children and adolescents: A systematic review. J. Sci. Med. Sport 2018, 21, 89–102. [Google Scholar] [PubMed]
- Siahkouhian, M.; Mahmoodi, H.; Salehi, M. Relationship between fundamental movement skills and body mass index in 7-to-8 year-old children. World Appl. Sci. J. 2011, 15, 1354–1360. [Google Scholar]
- Morgan, P.J.; Grounds, J.A.; Ashton, L.M.; Collins, C.E.; Barnes, A.T.; Pollock, E.R.; Kennedy, S.L.; Rayward, A.T.; Saunders, K.L.; Drew, R.J.; et al. Impact of the ‘Healthy Youngsters, Healthy Dads’ program on physical activity and other health behaviours: A randomised controlled trial involving fathers and their preschool-aged children. BMC Public Health 2022, 22, 1166. [Google Scholar]
- Brian, A.; Taunton Miedema, S.; Starrett, A.; Griffin, S.; Stribing, A.; Miedema, B.; Walker, M.; Casner, C.; Wainwright, N.; Wadsworth, D.; et al. SKIPping with PALS: Exploring Parental Engagement in a Motor Intervention for Their Preschool Children. Res. Q. Exerc. Sport 2022, 1–10. [Google Scholar] [CrossRef]
- Bryant, E.S.; Duncan, M.J.; Birch, S.L. Fundamental movement skills and weight status in British primary school children. Eur. J. Sport Sci. 2014, 14, 730–736. [Google Scholar] [CrossRef]
- Kokštejn, J.; Musálek, M.; Tufano, J.J. Are sex differences in fundamental motor skills uniform throughout the entire preschool period? PLoS ONE 2017, 12, e0176556. [Google Scholar]
- Hesketh, K.R.; Griffin, S.J.; van Sluijs, E.M. UK Preschool-aged children’s physical activity levels in childcare and at home: A cross-sectional exploration. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 123. [Google Scholar]
- Lai, S.K.; Costigan, S.A.; Morgan, P.J.; Lubans, D.R.; Stodden, D.F.; Salmon, J.; Barnett, L.M. Do school-based interventions focusing on physical activity, fitness, or fundamental movement skill competency produce a sustained impact in these outcomes in children and adolescents? A systematic review of follow-up studies. Sports Med. 2014, 44, 67–79. [Google Scholar]
- Olesen, L.G.; Kristensen, P.L.; Ried-Larsen, M.; Grøntved, A.; Froberg, K. Physical activity and motor skills in children attending 43 preschools: A cross-sectional study. BMC Pediatr. 2014, 14, 229. [Google Scholar]
- Hardy, L.L.; King, L.; Farrell, L.; Macniven, R.; Howlett, S. Fundamental movement skills among Australian preschool children. J. Sci. Med. Sport 2010, 13, 503–508. [Google Scholar] [PubMed]
- Zheng, Y.; Ye, W.; Korivi, M.; Liu, Y.; Hong, F. Gender Differences in Fundamental Motor Skills Proficiency in Children Aged 3–6 Years: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 8318. [Google Scholar] [CrossRef] [PubMed]
- Hardy, L.L.; Reinten-Reynolds, T.; Espinel, P.; Zask, A.; Okely, A.D. Prevalence and correlates of low fundamental movement skill competency in children. Pediatrics 2012, 130, e390–e398. [Google Scholar] [CrossRef] [PubMed]
- Eyre, E.L.; Adeyemi, L.J.; Cook, K.; Noon, M.; Tallis, J.; Duncan, M. Barriers and Facilitators to Physical Activity and FMS in Children Living in Deprived Areas in the UK: Qualitative Study. Int. J. Environ. Res. Public Health 2022, 19, 1717. [Google Scholar] [CrossRef] [PubMed]
- Eyre, E.L.; Walker, L.J.; Duncan, M.J. Fundamental movement skills of children living in England: The role of ethnicity and native English language. Percept. Mot. Ski. 2018, 125, 5–20. [Google Scholar] [CrossRef]
- Webster, E.K.; Martin, C.K.; Staiano, A.E. Fundamental motor skills, screen-time, and physical activity in preschoolers. J. Sport Health Sci. 2019, 8, 114–121. [Google Scholar] [CrossRef]
- Spessato, B.C.; Gabbard, C.; Valentini, N.; Rudisill, M. Gender differences in Brazilian children’s fundamental movement skill performance. Early Child Dev. Care 2013, 183, 916–923. [Google Scholar] [CrossRef]
- Capio, C.M.; Poolton, J.M.; Sit, C.H.P.; Holmstrom, M.; Masters, R.S.W. Reducing errors benefits the field-based learning of a fundamental movement skill in children. Scand. J. Med. Sci. Sports 2013, 23, 181–188. [Google Scholar] [CrossRef]
- Eddy, L.; Hill, L.J.; Mon-Williams, M.; Preston, N.; Daly-Smith, A.; Medd, G.; Bingham, D.D. Fundamental movement skills and their assessment in primary schools from the perspective of teachers. Meas. Phys. Educ. Exerc. Sci. 2021, 25, 236–249. [Google Scholar] [CrossRef]
- Dobell, A.; Pringle, A.; Faghy, M.A.; Roscoe, C.M. Educators Perspectives on the Value of Physical Education, Physical Activity and Fundamental Movement Skills for Early Years Foundation Stage Children in England. Children 2021, 8, 338. [Google Scholar] [CrossRef]
- Chan, C.H.; Ha, A.S.; Ng, J.Y.; Lubans, D.R. The A+ FMS cluster randomized controlled trial: An assessment-based intervention on fundamental movement skills and psychosocial outcomes in primary schoolchildren. J. Sci. Med. Sport 2019, 22, 935–940. [Google Scholar] [PubMed]
- Grainger, F.; Innerd, A.; Graham, M.; Wright, M. Integrated strength and fundamental movement skill training in children: A pilot study. Children 2020, 7, 161. [Google Scholar] [CrossRef] [PubMed]
- Faigenbaum, A.D.; Myer, G.D. Exercise deficit disorder in youth: Play now or pay later. Curr. Sports Med. Rep. 2012, 11, 196–200. [Google Scholar] [CrossRef] [PubMed]
- O’Sullivan, C.Ó.; Parker, M.; Comyns, T.; Ralph, A. Enhancing Fundamental Movement Skills: Understanding Student Voices. J. Teach. Phys. Educ. 2020, 40, 126–135. [Google Scholar]
- Pot, N.; van Hilvoorde, I.; Afonso, J.; Koekoek, J.; Almond, L. Meaningful movement behaviour involves more than the learning of fundamental movement skills. Int. Sports Stud. 2017, 39, 5–20. [Google Scholar] [CrossRef]
- Cohen, K.E.; Morgan, P.J.; Plotnikoff, R.C.; Barnett, L.M.; Lubans, D.R. Improvements in fundamental movement skill competency mediate the effect of the SCORES intervention on physical activity and cardiorespiratory fitness in children. J. Sports Sci. 2015, 33, 1908–1918. [Google Scholar] [CrossRef]
- Roscoe, C.M.; James, R.S.; Duncan, M.J. Preschool staff and parents’ perceptions of preschool children’s physical activity and fundamental movement skills from an area of high deprivation: A qualitative study. Qual. Res. Sport Exerc. Health 2017, 9, 619–635. [Google Scholar] [CrossRef]
- Coleman, B.; Dyment, J.E. Factors that limit and enable preschool-aged children’s physical activity on child care centre playgrounds. J. Early Child. Res. 2013, 11, 203–221. [Google Scholar] [CrossRef]
- Adamo, K.B.; Wilson, S.; Harvey, A.L.; Grattan, K.P.; Naylor, P.J.; Temple, V.A.; Goldfield, G.S. Does intervening in childcare settings impact fundamental movement skill development. Med. Sci. Sports Exerc. 2016, 48, 926–932. [Google Scholar] [CrossRef]
- Leis, A.; Ward, S.; Vatanparast, H.; Humbert, M.L.; Chow, A.F.; Muhajarine, N.; Engler-Stringer, R.; Bélanger, M. Effectiveness of the Healthy Start-Départ Santé approach on physical activity, healthy eating and fundamental movement skills of preschoolers attending childcare centres: A randomized controlled trial. BMC Public Health 2020, 20, 523. [Google Scholar] [CrossRef]
- Tugault-Lafleur, C.N.; Naylor, P.J.; Carson, V.; Faulkner, G.; Lau, E.Y.; Wolfenden, L.; Mâsse, L.C. Does an active play standard change childcare physical activity and healthy eating policies? A natural policy experiment. BMC Public Health 2022, 22, 687. [Google Scholar] [CrossRef] [PubMed]
- Ha, A.S.; Lonsdale, C.; Lubans, D.R.; Ng, F.F.; Ng, J.Y. Improving children’s fundamental movement skills through a family-based physical activity program: Results from the “Active 1+ FUN” randomized controlled trial. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 99. [Google Scholar] [CrossRef] [PubMed]
- Johnstone, A.; Hughes, A.R.; Martin, A.; Reilly, J.J. Utilising active play interventions to promote physical activity and improve fundamental movement skills in children: A systematic review and meta-analysis. BMC Public Health 2018, 18, 789. [Google Scholar]
- Lane, C.; Naylor, P.J.; Predy, M.; Kurtzhals, M.; Rhodes, R.E.; Morton, K.; Hunter, S.; Carson, V. Exploring a parent-focused physical literacy intervention for early childhood: A pragmatic controlled trial of the PLAYshop. BMC Public Health 2022, 22, 659. [Google Scholar] [CrossRef]
- Roscoe, C.M.; James, R.S.; Duncan, M.J. Accelerometer-based physical activity levels differ between week and weekend days in British preschool children. J. Funct. Morphol. Kinesiol. 2019, 4, 65. [Google Scholar] [CrossRef]
- Bedard, C.; Bremer, E.; Campbell, W.; Cairney, J. A quasi-experimental study of a movement and preliteracy program for 3-and 4-year-old children. Front. Pediatr. 2017, 5, 94. [Google Scholar] [CrossRef]
- Barnett, L.M.; Hnatiuk, J.A.; Salmon, J.; Hesketh, K.D. Modifiable factors which predict children’s gross motor competence: A prospective cohort study. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 129. [Google Scholar] [CrossRef]
- Horodyska, K.; Boberska, M.; Kruk, M.; Szczuka, Z.; Wiggers, J.; Wolfenden, L.; Scholz, U.; Radtke, T.; Luszczynska, A. Perceptions of physical activity promotion, transportation support, physical activity, and body mass: An insight into parent-child dyadic processes. Int. J. Behav. Med. 2019, 26, 255–265. [Google Scholar]
- Cools, W.; De Martelaer, K.; Samaey, C.; Andries, C. Fundamental movement skill performance of preschool children in relation to family context. J. Sports Sci. 2011, 29, 649–660. [Google Scholar] [CrossRef]
- Brandelli, Y.N.; Stone, M.; Westheuser, V.; Huber, A.M.; Joshi, N.; Reid, A.; Stringer, E.; Stevens, D. Parent Risk Perceptions, Physical Literacy, and Fundamental Movement Skills in Children with Juvenile Idiopathic Arthritis. Pediatr. Phys. Ther. 2022, 34, 536–544. [Google Scholar] [CrossRef]
- Corder, K.; Crespo, N.C.; van Sluijs, E.M.; Lopez, N.V.; Elder, J.P. Parent awareness of young children’s physical activity. Prev. Med. 2012, 55, 201–205. [Google Scholar] [CrossRef] [PubMed]
- Liong, G.H.; Ridgers, N.D.; Barnett, L.M. Associations between skill perceptions and young children’s actual fundamental movement skills. Percept. Mot. Ski. 2015, 120, 591–603. [Google Scholar] [CrossRef] [PubMed]
- Bentley, G.F.; Goodred, J.K.; Jago, R.; Sebire, S.J.; Lucas, P.J.; Fox, K.R.; Stewart-Brown, S.; Turner, K.M. Parents’ views on child physical activity and their implications for physical activity parenting interventions: A qualitative study. BMC Pediatr. 2012, 12, 180. [Google Scholar] [CrossRef] [PubMed]
- Kesten, J.M.; Jago, R.; Sebire, S.J.; Edwards, M.J.; Pool, L.; Zahra, J.; Thompson, J.L. Understanding the accuracy of parental perceptions of child physical activity: A mixed methods analysis. J. Phys. Act. Health 2015, 12, 1529–1535. [Google Scholar] [CrossRef]
- Agard, B.; Zeng, N.; McCloskey, M.L.; Johnson, S.L.; Bellows, L.L. Moving together: Understanding parent perceptions related to physical activity and motor skill development in preschool children. Int. J. Environ. Res. Public Health 2021, 18, 9196. [Google Scholar] [CrossRef]
- Lijuan, W.; Jiancui, S.; Suzhe, Z. Parental influence on the physical activity of Chinese children: Do gender differences occur? Eur. Phys. Educ. Rev. 2017, 23, 110–126. [Google Scholar] [CrossRef]
- Tompsett, C.; Sanders, R.; Taylor, C.; Cobley, S. Pedagogical approaches to and effects of fundamental movement skill interventions on health outcomes: A systematic review. Sports Med. 2017, 47, 1795–1819. [Google Scholar] [CrossRef]
- Lane, C.; Carson, V.; Morton, K.; Reno, K.; Wright, C.; Predy, M.; Naylor, P.J. A real-world feasibility study of the PLAYshop: A brief intervention to facilitate parent engagement in developing their child’s physical literacy. Pilot Feasibility Stud. 2021, 7, 113. [Google Scholar] [CrossRef]
- Stevenson, A.; Wainwright, N.; Williams, A. Interventions targeting motor skills in pre-school-aged children with direct or indirect parent engagement: A systematic review and narrative synthesis. Education 2022, 51, 1003–1016. [Google Scholar] [CrossRef]
- Morgan, P.J.; Young, M.D.; Barnes, A.T.; Eather, N.; Pollock, E.R.; Lubans, D.R. Engaging fathers to increase physical activity in girls: The “dads and daughters exercising and empowered” (DADEE) randomized controlled trial. Ann. Behav. Med. 2019, 53, 39–52. [Google Scholar] [CrossRef]
- Webster, E.K.; Kracht, C.L.; Newton, R.L., Jr.; Beyl, R.A.; Staiano, A.E. Intervention to Improve Preschool Children’s Fundamental Motor Skills: Protocol for a Parent-Focused, Mobile App–Based Comparative Effectiveness Trial. JMIR Res. Protoc. 2020, 9, e19943. [Google Scholar] [CrossRef] [PubMed]
- Staiano, A.E.; Newton, R.L.; Beyl, R.A.; Kracht, C.L.; Hendrick, C.A.; Viverito, M.; Webster, E.K. mHealth Intervention for Motor Skills: A Randomized Controlled Trial. Pediatrics 2022, 149, e2021053362. [Google Scholar] [CrossRef] [PubMed]
- Trost, S.G.; Brookes, D.S. Effectiveness of a novel digital application to promote fundamental movement skills in 3-to 6-year-old children: A randomized controlled trial. J. Sports Sci. 2021, 39, 453–459. [Google Scholar] [CrossRef] [PubMed]
- James, M.E.; Bedard, C.; Bremer, E.; Cairney, J. The acceptability and feasibility of a preschool intervention targeting motor, social, and emotional development. Front. Pediatr. 2020, 8, 319. [Google Scholar] [CrossRef] [PubMed]
- Veldman, S.L.; Jones, R.A.; Okely, A.D. Efficacy of gross motor skill interventions in young children: An updated systematic review. BMJ Open Sport Exerc. Med. 2016, 2, e000067. [Google Scholar] [CrossRef] [PubMed]
- Hong, Q.N.; Fàbregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.P.; Griffiths, F.; Nicolau, B.; O’Cathain, A.; et al. The Mixed Methods Appraisal Tool (MMAT) version 2018 for information professionals and researchers. Educ. Inf. 2018, 34, 285–291. [Google Scholar] [CrossRef]
- Wasenius, N.S.; Grattan, K.P.; Harvey, A.L.; Naylor, P.J.; Goldfield, G.S.; Adamo, K.B. The effect of a physical activity intervention on preschoolers’ fundamental motor skills—A cluster RCT. J. Sci. Med. Sport 2018, 21, 714–719. [Google Scholar] [CrossRef]
- Altunsöz, I.H.; Goodway, J.D. Skiping to motor competence: The influence of project successful kinesthetic instruction for preschoolers on motor competence of disadvantaged preschoolers. Phys. Educ. Sport Pedagog. 2016, 21, 366–385. [Google Scholar] [CrossRef]
- Laukkanen, A.; Pesola, A.J.; Heikkinen, R.; Sääkslahti, A.K.; Finni, T. Family-based cluster randomized controlled trial enhancing physical activity and motor competence in 4–7-year-old children. PLoS ONE 2015, 10, e0141124. [Google Scholar]
- Iivonen, S.; Sääkslahti, A.; Laukkanen, A. A review of studies using the Körperkoordinationstest für Kinder (KTK). Eur. J. Adapt. Phys. Act. 2016, 8. [Google Scholar] [CrossRef]
- Numminen, P. APM inventory: Manual and test booklet for assessing pre-school children’s perceptual and basic motor skills. Liikunnan Kansanterveyden Julk. 1995, 98, 44. [Google Scholar]
- Rey, E.; Carballo-Fazanes, A.; Varela-Casal, C.; Abelairas-Gómez, C.; ALFA-MOV Project Collaborators. Reliability of the test of gross motor development: A systematic review. PLoS ONE 2020, 15, e0236070. [Google Scholar] [CrossRef] [PubMed]
- Zanella, L.W.; Valentini, N.C.; Copetti, F.; Nobre, G.C. Peabody Developmental Motor Scales-(PDMS-2): Reliability, content and construct validity evidence for Brazilian children. Res. Dev. Disabil. 2021, 111, 103871. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, M.; Goodway, J.; Haubenstricker, J. Parent-assisted instruction in a motor skill program for at-risk preschool children. Adapt. Phys. Act. Q. 1999, 16, 415–426. [Google Scholar] [CrossRef]
- Riethmuller, A.M.; Jones, R.A.; Okely, A.D. Efficacy of interventions to improve motor development in young children: A systematic review. Pediatrics 2009, 124, e782–e792. [Google Scholar] [CrossRef]
- Van Capelle, A.; Broderick, C.R.; van Doorn, N.; Ward, R.E.; Parmenter, B.J. Interventions to improve fundamental motor skills in pre-school aged children: A systematic review and meta-analysis. J. Sci. Med. Sport 2017, 20, 658–666. [Google Scholar] [CrossRef]
- Livonen, S.; Sääkslahti, A.K. Preschool children’s fundamental motor skills: A review of significant determinants. Early Child Dev. Care 2014, 184, 1107–1126. [Google Scholar] [CrossRef]
- Donath, L.; Faude, O.; Hagmann, S.; Roth, R.; Zahner, L. Fundamental movement skills in preschoolers: A randomized controlled trial targeting object control proficiency. Child Care Health Dev. 2015, 41, 1179–1187. [Google Scholar] [CrossRef]
- Scott-Andrews, K.Q.; Hasson, R.E.; Miller, A.L.; Templin, T.J.; Robinson, L.E. Associations Between Physical Activity and Gross Motor Skills in Parent–Child Dyads. J. Mot. Learn. Dev. 2022, 10, 485–503. [Google Scholar] [CrossRef]
- Laukkanen, A.; Niemistö, D.; Finni, T.; Cantell, M.; Korhonen, E.; Sääkslahti, A. Correlates of physical activity parenting: The Skilled Kids study. Scand. J. Med. Sci. Sports 2018, 28, 2691–2701. [Google Scholar] [CrossRef]
- Logan, S.W.; Robinson, L.E.; Wilson, A.E.; Lucas, W.A. Getting the fundamentals of movement: A meta-analysis of the effectiveness of motor skill interventions in children. Child Care Health Dev. 2012, 38, 305–315. [Google Scholar] [CrossRef]
- McCloskey, M.L.; Thompson, D.A.; Chamberlin, B.; Clark, L.; Johnson, S.L.; Bellows, L.L. Mobile device use among rural, low-income families and the feasibility of an app to encourage preschoolers’ physical activity: Qualitative study. JMIR Pediatr. Parent. 2018, 1, e10858. [Google Scholar] [CrossRef] [PubMed]
- Swindle, T.; Poosala, A.B.; Zeng, N.; Børsheim, E.; Andres, A.; Bellows, L.L. Digital intervention strategies for increasing physical activity among preschoolers: Systematic review. J. Med. Internet Res. 2022, 24, e28230. [Google Scholar] [CrossRef] [PubMed]
- Bai, P.; Thornton, A.; Lester, L.; Schipperijn, J.; Trapp, G.; Boruff, B.; Ng, M.; Wenden, E.; Christian, H. Nature play and fundamental movement skills training programs improve childcare educator supportive physical activity behavior. Int. J. Environ. Res. Public Health 2020, 17, 223. [Google Scholar] [CrossRef] [PubMed]
- Dowdell, K.; Gray, T.; Malone, K. Nature and its influence on children’s outdoor play. J. Outdoor Environ. Educ. 2011, 15, 24–35. [Google Scholar] [CrossRef]
- Ayubia, N.; Komainib, A. The Impact of the COVID-19 Pandemic on Children’s Motor Skills (Literature Review). Children 2021, 90, 66–70. [Google Scholar] [CrossRef]
- Coppens, E.; Rommers, N.; Bardid, F.; Deconinck, F.J.; De Martelaer, K.; D’Hondt, E.; Lenoir, M. Long-term effectiveness of a fundamental motor skill intervention in Belgian children: A 6-year follow-up. Scand. J. Med. Sci. Sports 2021, 31, 23–34. [Google Scholar] [CrossRef]
- Making Our Move. Our Shared Vision for Uniting the Movement in Notts and Derbyshire. Available online: https://makingourmove.org.uk/about/making-our-move/ (accessed on 13 June 2023).
- The First 1000 Days Yorkshire Giving Every Child the Best Possible Start; University of Leeds: Leeds, UK, 2023.
- Lopes, L.; Santos, R.; Coelho-e-Silva, M.; Draper, C.; Mota, J.; Jidovt seff, B.; Clark, C.; Schmidt, M.; Morgan, P.; Duncan, M.; et al. A Narrative Review of Motor Competence in Children and Adolescents: What We Know and What We Need to Find Out. Int. J. Environ. Res. Public Health 2021, 18, 18. [Google Scholar] [CrossRef]
- International Motor Development Research Consortium. Advancing Motor Development Research in the 21st Century. 2023. Available online: https://www.i-mdrc.com/ (accessed on 19 June 2023).


{kind=link}
| Author and Year of Publication | MMAT Score |
|---|---|
| Trost and Brookes, 2021 [77] | 7 |
| Staiano et al., 2022 [76] | 7 |
| Wasenius et al., 2018 [81] | 7 |
| Morgan et al., 2022 [28] | 7 |
| James et al., 2020 [78] | 6 |
| Altunsoz and Goodway, 2016 [82] | 7 |
| Brian et al., 2022 [29] | 5 |
| Laukkanen et al., 2015 [83] | 6 |
| Bedard et al., 2017 [60] | 7 |
| Author & Country | Study Design | Setting | Parent Component Method and Intervention Description | Duration (Weeks) | Sample | Mean Child Age (Years) | FMS Assessment Tool(s) | Overall Findings |
|---|---|---|---|---|---|---|---|---|
| Trost and Brookes (2021) [77]. Australia | RCT | Home | Smartphone app for joint parent–child participation: A digital games library of physical literacy skills to promote parent–child participation in 60 min of daily MVPA and to enhance FMS. | 8 | 34 parent–child dyads: 17 boys 17 girls | 5.3 ± 1.2 | TGMD-2: 6 LOCO skills (run, gallop, hop, leap, jump, slide); 6 OC skills (strike, dribble, catch, kick, throw, roll). |
|
| Staiano et al. (2022) [76]. USA | RCT | Home | Smartphone app for parent home delivery: 12 h (12 min per day, 5 × per week) of structured motor skills delivered by parents at home. | 12 | 72 children: 31 boys 41 girls | 4.0 ± 0.8 | TGMD-3: 6 LOCO skills (run, gallop, skip, hop, jump, slide); 7 OC skills (two-hand strike, one-hand strike, dribble, catch, kick, throw, roll). |
|
| Laukkanen et al. (2015) [83]. Finland | Cluster RCT | Home | Parent education and counselling: Parents received one lecture followed by face-to-face counselling and goal-setting to promote PA. Telephone discussions for reinforcement held at 2 months and 5 months. | 52 | 91 children: 42 boys 49 girls 122 parents 52 males 70 females | 6.2 ± 1.1 | KTK: Walking backwards, hopping for height, jumping sideways, moving sideways. TCB test from APM Inventory. |
|
| Wasenius et al. (2018) [81]. Canada | Cluster RCT | Hybrid: Children’s Centre and Home | Online parent education and paper materials for parent home delivery: Childcare providers received 2 × 3 h workshops and bi-monthly booster sessions to deliver a structured activity programme to the children within the centre. Parents received two online webinars of similar content to the childcare providers, an ABC manual to follow with the children at home, and bi-weekly postcards to encourage PA at home and in the community. | 26 | 215 children: 117 boys 98 girls | 3.6 ± 0.5 | TGMD-2: 6 LOCO skills (run, gallop, hop, leap, jump, slide); 6 OC skills (strike, dribble, catch, kick, throw, roll). |
|
| Brian et al. (2022) [29]. USA | Quasi-experimental Study | Hybrid: Childcare Centre and Home | Parent education & joint parent–child participation: 1 × 60-min centre-based session per month (30 min parent education, 30 min parent–child participation. Parents provided with online materials to encourage FMS and PA engagement at home. | 26 | 104 children: 53 boys 51 girls 134 parents: 20 males 106 females 8 guardians | 5.1 ± 0.5 | TGMD-3: 6 LOCO skills (run, jump, hop, gallop, skip, slide); 7 OC skills (dribble, strike with bat, strike with paddle, underarm throw, overarm throw, kick, catch). |
|
| Morgan et al. (2022) [28]. Australia | RCT | Hybrid: Childcare Centre and Home | Parent education & joint parent–child participation: 2 × 2-h fathers-only face-to-face workshops. 8 × 75-min father-child practical sessions delivered in centre. Activity handbook for fathers and children to complete at home. | 8 | 125 father-child dyads: 76 boys 49 girls | 3.9 ± 0.5 | TGMD-3: 5 OC skills (two-hand strike, one-hand strike, dribble, overarm throw, underarm throw). |
|
| Altunsoz and Goodway (2016) [82]. USA | Quasi-experimental Study | Hybrid: Childcare Centre and Home | Parent education for home delivery: 16 × 30-min OC skill development sessions delivered in centre by a trained motor skill instructor. Parents received a 1.5-h workshop to prepare to deliver 24 × 10–15-min sessions to their children at home. A parent–child motor activity calendar was provided to be followed at home. | 8 | 72 children: 36 boys 36 girls | 4.0 ± 0.6 | TGMD-2: 6 OC skills (strike, dribble, catch, kick, throw, roll). |
|
| James et al. (2020) [78]. Canada | Exploratory Pilot Study | Hybrid: Community Centre and Home | Joint parent–child participation: 1 × 60-min session per week for 10 weeks delivered by master’s students and undergraduate volunteers, involving direct FMS instruction, free play, and social emotional learning. Parents and caregivers actively participated and were provided with a take home guide to practice activities at home. | 10 | 11 parent–child dyads: 7 boys 4 girls | 4.2 ± 0.7 | PDMS-2: Stationary performance (30 items), locomotion (89 items), object manipulation (24 items). |
|
| Bedard et al. (2017) [60]. Canada | Quasi-experimental Study | Hybrid: Community Centre and Home | Joint parent–child participation: 1 × 60-min session per week for 10 weeks delivered by graduate students, involving direct FMS instruction, free play, and storybook reading. Parents and caregivers actively participated in the sessions. Weekly handouts were provided with activities to be practiced at home. | 10 | 19 children: 10 boys 9 girls | 3.7 | PDMS-2: Stationary performance (30 items), locomotion (89 items), object manipulation (24 items). |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Flynn, R.J.; Pringle, A.; Roscoe, C.M.P. Direct Parent Engagement to Improve Fundamental Movement Skills in Children: A Systematic Review. Children 2023, 10, 1247. https://doi.org/10.3390/children10071247
Flynn RJ, Pringle A, Roscoe CMP. Direct Parent Engagement to Improve Fundamental Movement Skills in Children: A Systematic Review. Children. 2023; 10(7):1247. https://doi.org/10.3390/children10071247
Chicago/Turabian StyleFlynn, Robert J., Andy Pringle, and Clare M. P. Roscoe. 2023. "Direct Parent Engagement to Improve Fundamental Movement Skills in Children: A Systematic Review" Children 10, no. 7: 1247. https://doi.org/10.3390/children10071247
APA StyleFlynn, R. J., Pringle, A., & Roscoe, C. M. P. (2023). Direct Parent Engagement to Improve Fundamental Movement Skills in Children: A Systematic Review. Children, 10(7), 1247. https://doi.org/10.3390/children10071247