

Overshoot of the Respiratory Exchange Ratio during Recovery from Maximal Exercise Testing in Young Patients with Congenital Heart Disease
 , , ,
, , ,  , ,
, ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Population Characteristics
2.2. Cardiopulmonary Exercise Testing
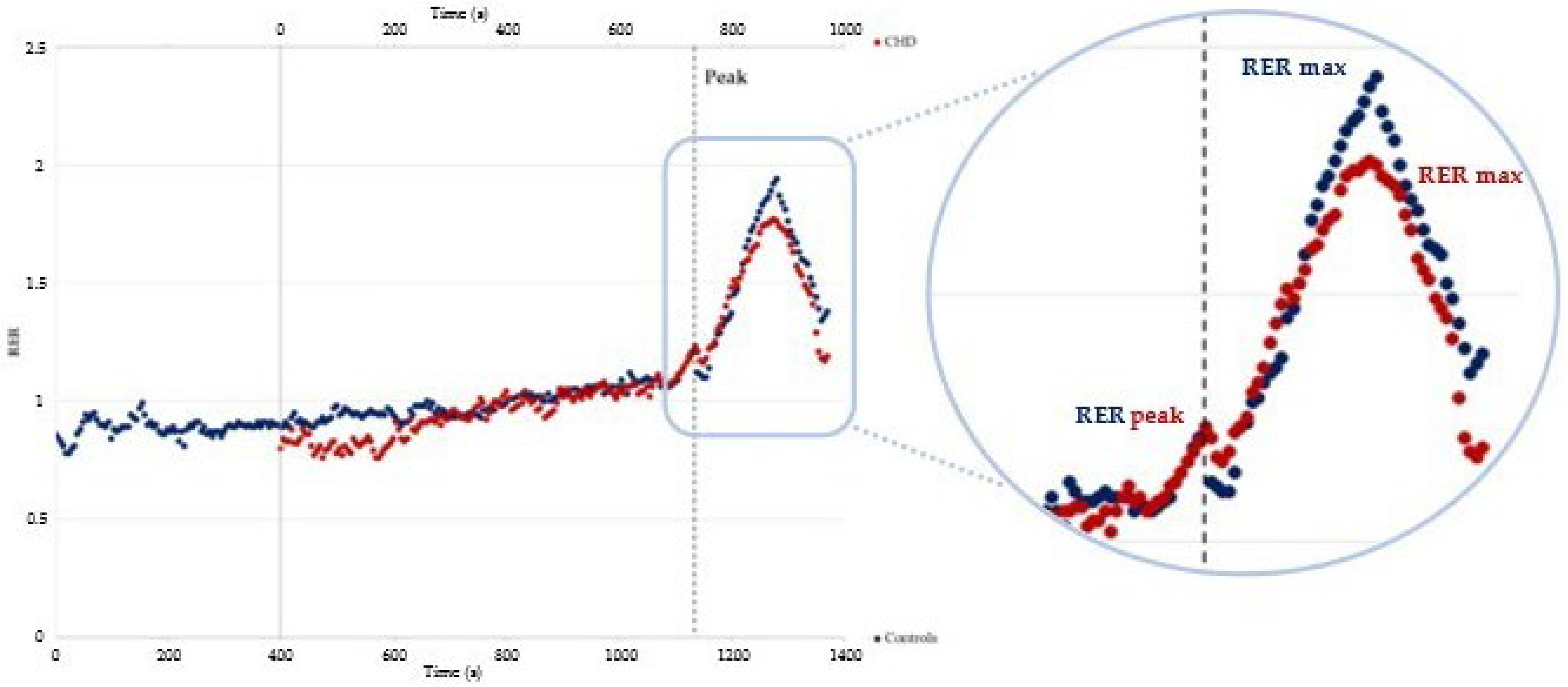
2.3. Overshoot Analyses
- the RER at peak exercise (RER peak) was defined as the highest value of the RER reached during exercise;
- the highest RER value reached during the recovery phase (RER max);
- the difference between RER max and RER peak, calculated as the percentual increase during the recovery phase; i.e., RER magnitude (RER mag);
- the slope of the RER calculated by linearly regressing the RER data between RER peak and RER max during the recovery phase (RER slope);
- the time between RER peak and RER max (Time to RER max) [12].
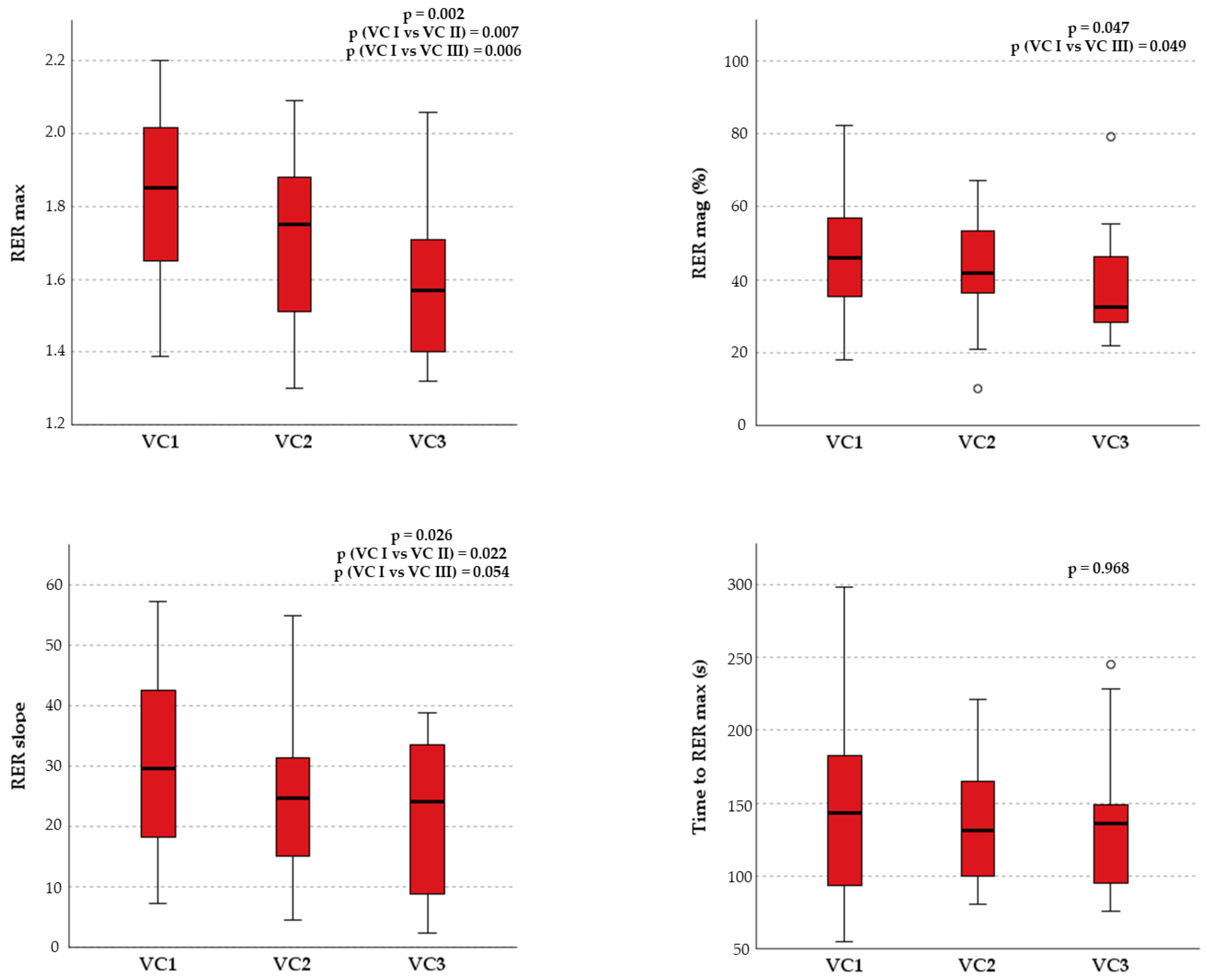
2.4. Ventricular Function Assessment
2.5. Statistical Analyses
3. Results
3.1. Patients Selection
3.2. Baseline Characteristics
3.3. Cardiopulmonary Exercise Testing and Echocardiographic Assessments
3.4. Overshoot Analysis
4. Discussion
- All patients with CHD presented an overshoot of the RER during recovery after maximal CPET.
- Patients with CHD showed reduced RER recovery overshoot compared to healthy subjects.
- Although there are significant differences regarding the cardiopulmonary response during exercise between the subgroups of CHD, no differences in the RER recovery parameters were evident.
- RER recovery parameters significantly correlated with the most important cardiorespiratory fitness and efficiency indices, independently from the RER peak reached during exercise.
4.1. Why Is the CPET Recovery Phase Relevant in Patients with CHD?
4.2. Exercise Phase
4.3. Recovery Phase
4.4. RER Overshoot and Cardiorespiratory Fitness/Efficiency
4.5. Limitations and Perspectives
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- van der Linde, D.; Konings, E.E.M.; Slager, M.A.; Witsenburg, M.; Helbing, W.A.; Takkenberg, J.J.M.; Roos-Hesselink, J.W. Birth Prevalence of Congenital Heart Disease Worldwide: A Systematic Review and Meta-Analysis. J. Am. Coll Cardiol. 2011, 58, 2241–2247. [Google Scholar] [CrossRef] [PubMed]
- Dolk, H.; Loane, M.; Garne, E. Congenital Heart Defects in Europe: Prevalence and Perinatal Mortality, 2000 to 2005. Circulation 2011, 123, 841–849. [Google Scholar] [CrossRef]
- Best, K.E.; Rankin, J. Long-Term Survival of Individuals Born With Congenital Heart Disease: A Systematic Review and Meta-Analysis. J. Am. Heart Assoc. 2016, 5, e002846. [Google Scholar] [CrossRef] [PubMed]
- Oliver, J.M.; Gallego, P.; Gonzalez, A.E.; Garcia-Hamilton, D.; Avila, P.; Yotti, R.; Ferreira, I.; Fernandez-Aviles, F. Risk Factors for Excess Mortality in Adults with Congenital Heart Diseases. Eur. Heart J. 2017, 38, 1233–1241. [Google Scholar] [CrossRef]
- Amedro, P.; Gavotto, A.; Guillaumont, S.; Bertet, H.; Vincenti, M.; de La Villeon, G.; Bredy, C.; Acar, P.; Ovaert, C.; Picot, M.C.; et al. Cardiopulmonary Fitness in Children with Congenital Heart Diseases versus Healthy Children. Heart 2018, 104, 1026–1036. [Google Scholar] [CrossRef]
- Warnes, C.A.; Williams, R.G.; Bashore, T.M.; Child, J.S.; Connolly, H.M.; Dearani, J.A.; del Nido, P.; Fasules, J.W.; Graham, T.P.; Hijazi, Z.M.; et al. ACC/AHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Develop Guidelines on the Management of Adults with Congenital Heart Disease). Circulation 2008, 118, e714–e833. [Google Scholar] [CrossRef] [PubMed]
- Wadey, C.A.; Weston, M.E.; Dorobantu, D.M.; Pieles, G.E.; Stuart, G.; Barker, A.R.; Taylor, R.S.; Williams, C.A. The Role of Cardiopulmonary Exercise Testing in Predicting Mortality and Morbidity in People with Congenital Heart Disease: A Systematic Review and Meta-Analysis. Eur. J. Prev. Cardiol. 2022, 29, 513–533. [Google Scholar] [CrossRef]
- Guazzi, M. “Recovering” the Recognition for VO2 Kinetics During Exercise Recovery in Heart Failure: A Good Practice in Need of More Exercise. J. ACC Heart Fail. 2018, 6, 340–342. [Google Scholar] [CrossRef]
- Guazzi, M.; Bandera, F.; Ozemek, C.; Systrom, D.; Arena, R. Cardiopulmonary Exercise Testing: What Is Its Value? J. Am. Coll Cardiol. 2017, 70, 1618–1636. [Google Scholar] [CrossRef]
- Arena, R.; Myers, J.; Guazzi, M. Cardiopulmonary Exercise Testing Is a Core Assessment for Patients With Heart Failure. Congest. Heart Fail. 2011, 17, 115–119. [Google Scholar] [CrossRef]
- Tanabe, Y.; Takahashi, M.; Hosaka, Y.; Ito, M.; Ito, E.; Suzuki, K. Prolonged Recovery of Cardiac Output after Maximal Exercise in Patients with Chronic Heart Failure. J. Am. Coll Cardiol. 2000, 35, 1228–1236. [Google Scholar] [CrossRef] [PubMed]
- Takayanagi, Y.; Koike, A.; Nagayama, O.; Nagamine, A.; Qin, R.; Kato, J.; Nishi, I.; Himi, T.; Kato, Y.; Sato, A.; et al. Clinical Significance of the Overshoot Phenomena of Respiratory Gas Indices during Recovery from Maximal Exercise Testing. J. Cardiol. 2017, 70, 598–606. [Google Scholar] [CrossRef]
- Bailey, C.S.; Wooster, L.T.; Buswell, M.; Patel, S.; Pappagianopoulos, P.P.; Bakken, K.; White, C.; Tanguay, M.; Blodgett, J.B.; Baggish, A.L.; et al. Post-Exercise Oxygen Uptake Recovery Delay: A Novel Index of Impaired Cardiac Reserve Capacity in Heart Failure. JACC Heart Fail. 2018, 6, 329–339. [Google Scholar] [CrossRef] [PubMed]
- Falk, B.; Dotan, R. Child-Adult Differences in the Recovery from High-Intensity Exercise. Exerc. Sport Sci. Rev. 2006, 34, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Zanconato, S.; Cooper, D.M.; Armon, Y. Oxygen Cost and Oxygen Uptake Dynamics and Recovery with 1 Min of Exercise in Children and Adults. J. Appl. Physiol. 1991, 71, 993–998. [Google Scholar] [CrossRef]
- Singh, T.P.; Alexander, M.E.; Gauvreau, K.; Curran, T.; Rhodes, Y.; Rhodes, J. Recovery of Oxygen Consumption after Maximal Exercise in Children. Med. Sci. Sports Exerc. 2011, 43, 555–559. [Google Scholar] [CrossRef]
- Greutmann, M.; Rozenberg, D.; Le, T.L.; Silversides, C.K.; Granton, J.T. Recovery of Respiratory Gas Exchange after Exercise in Adults with Congenital Heart Disease. Int. J. Cardiol. 2014, 176, 333–339. [Google Scholar] [CrossRef] [PubMed]
- Lurz, P.; Riede, F.T.; Taylor, A.M.; Wagner, R.; Nordmeyer, J.; Khambadkone, S.; Kinzel, P.; Derrick, G.; Schuler, G.; Bonhoeffer, P.; et al. Impact of Percutaneous Pulmonary Valve Implantation for Right Ventricular Outflow Tract Dysfunction on Exercise Recovery Kinetics. Int. J. Cardiol. 2014, 177, 276–280. [Google Scholar] [CrossRef]
- Giardini, A.; Specchia, S.; Coutsoumbas, G.; Donti, A.; Formigari, R.; Fattori, R.; Oppido, G.; Gargiulo, G.; Picchio, F.M. Impact of Pulmonary Regurgitation and Right Ventricular Dysfunction on Oxygen Uptake Recovery Kinetics in Repaired Tetralogy of Fallot. Eur. J. Heart Fail. 2006, 8, 736–743. [Google Scholar] [CrossRef] [PubMed]
- Neunhaeuserer, D.; Battista, F.; Mazzucato, B.; Vecchiato, M.; Meneguzzo, G.; Quinto, G.; Niebauer, J.; Gasperetti, A.; Vida, V.; di Salvo, G.; et al. Exercise Capacity and Cardiorespiratory Fitness in Children with Congenital Heart Diseases: A Proposal for an Adapted NYHA Classification. Int. J. Environ. Res. Public Health 2022, 19, 5907. [Google Scholar] [CrossRef] [PubMed]
- Hollenberg, M.; Tager, I.B. Oxygen Uptake Efficiency Slope: An Index of Exercise Performance and Cardiopulmonary Reserve Requiring Only Submaximal Exercise. J. Am. Coll Cardiol. 2000, 36, 194–201. [Google Scholar] [CrossRef]
- Vecchiato, M.; Neunhaeuserer, D.; Quinto, G.; Bettini, S.; Gasperetti, A.; Battista, F.; Vianello, A.; Vettor, R.; Busetto, L.; Ermolao, A. Cardiopulmonary Exercise Testing in Patients with Moderate-Severe Obesity: A Clinical Evaluation Tool for OSA? Sleep Breath. 2021, 26, 1115–1123. [Google Scholar] [CrossRef]
- Nanas, S.; Nanas, J.; Kassiotis, C.; Nikolaou, C.; Tsagalou, E.; Sakellariou, D.; Terovitis, I.; Papazachou, O.; Drakos, S.; Papamichalopoulos, A.; et al. Early Recovery of Oxygen Kinetics after Submaximal Exercise Test Predicts Functional Capacity in Patients with Chronic Heart Failure. Eur. J. Heart Fail. 2001, 3, 685–692. [Google Scholar] [CrossRef] [PubMed]
- Cohen-Solal, A.; Laperche, T.; Morvan, D.; Geneves, M.; Caviezel, B.; Gourgon, R. Prolonged Kinetics of Recovery of Oxygen Consumption After Maximal Graded Exercise in Patients With Chronic Heart Failure. Circulation 1995, 91, 2924–2932. [Google Scholar] [CrossRef] [PubMed]
- Scrutinio, D.; Passantino, A.; Lagioia, R.; Napoli, F.; Ricci, A.; Rizzon, P. Percent Achieved of Predicted Peak Exercise Oxygen Uptake and Kinetics of Recovery of Oxygen Uptake after Exercise for Risk Stratification in Chronic Heart Failure. Int. J. Cardiol. 1998, 64, 117–124. [Google Scholar] [CrossRef] [PubMed]
- Belardinelli, R.; Barstow, T.J.; Nguyen, P.; Wasserman, K. Skeletal Muscle Oxygenation and Oxygen Uptake Kinetics Following Constant Work Rate Exercise in Chronic Congestive Heart Failure. Am. J. Cardiol. 1997, 80, 1319–1324. [Google Scholar] [CrossRef]
- Zavin, A.; Arena, R.; Joseph, J.; Allsup, K.; Daniels, K.; Christian Schulze, P.; Lecker, S.; Forman, D.E. Dynamic Assessment of Ventilatory Efficiency during Recovery from Peak Exercise to Enhance Cardiopulmonary Exercise Testing. Eur. J. Prev. Cardiol. 2013, 20, 779–785. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, T.; Koike, A.; Nagayama, O.; Sakurada, K.; Tsuneoka, H.; Kato, J.; Yamashita, T.; Yamazaki, J. Overshoot Phenomena of Respiratory Gas Variables During Exercise Recovery in Cardiac Patients. Circ. J. 2012, 76, 876–883. [Google Scholar] [CrossRef] [PubMed]
- Fortin, M.; Turgeon, P.Y.; Nadreau, É.; Grégoire, P.; Maltais, L.G.; Sénéchal, M.; Provencher, S.; Maltais, F. Prognostic Value of Oxygen Kinetics During Recovery From Cardiopulmonary Exercise Testing in Patients With Chronic Heart Failure. Can. J. Cardiol. 2015, 31, 1259–1265. [Google Scholar] [CrossRef]
- Toste, A.; Soares, R.; Feliciano, J.; Andreozzi, V.; Silva, S.; Abreu, A.; Ramos, R.; Santos, N.; Ferreira, L.; Ferreira, R.C. Prognostic Value of a New Cardiopulmonary Exercise Testing Parameter in Chronic Heart Failure: Oxygen Uptake Efficiency at Peak Exercise—Comparison with Oxygen Uptake Efficiency Slope. Rev. Port. De Cardiol. 2011, 30, 781–787. [Google Scholar] [CrossRef] [PubMed]
- Coomans, I.; de Kinder, S.; van Belleghem, H.; de Groote, K.; Panzer, J.; de Wilde, H.; Mosquera, L.M.; François, K.; Bové, T.; Martens, T.; et al. Analysis of the Recovery Phase after Maximal Exercise in Children with Repaired Tetralogy of Fallot and the Relationship with Ventricular Function. PLoS ONE 2020, 15, e0244312. [Google Scholar] [CrossRef]
- Rychik, J.; Goldberg, D.J. Late Consequences of the Fontan Operation. Circulation 2014, 130, 1525–1528. [Google Scholar] [CrossRef] [PubMed]
- Feinstein, J.A.; Benson, D.W.; Dubin, A.M.; Cohen, M.S.; Maxey, D.M.; Mahle, W.T.; Pahl, E.; Villafae, J.; Bhatt, A.B.; Peng, L.F.; et al. Hypoplastic Left Heart Syndrome: Current Considerations and Expectations. J. Am. Coll Cardiol. 2012, 59, S1–S42. [Google Scholar] [CrossRef] [PubMed]
- Stout, K.K.; Daniels, C.J.; Aboulhosn, J.A.; Bozkurt, B.; Broberg, C.S.; Colman, J.M.; Crumb, S.R.; Dearani, J.A.; Fuller, S.; Gurvitz, M.; et al. 2018 AHA/ACC Guideline for the Management of Adults With Congenital Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019, 139, e698–e800. [Google Scholar] [CrossRef] [PubMed]
- Kempny, A.; Dimopoulos, K.; Uebing, A.; Moceri, P.; Swan, L.; Gatzoulis, M.A.; Diller, G.P. Reference Values for Exercise Limitations among Adults with Congenital Heart Disease. Relation to Activities of Daily Life--Single Centre Experience and Review of Published Data. Eur. Heart J. 2012, 33, 1386–1396. [Google Scholar] [CrossRef]
- Inuzuka, R.; Diller, G.P.; Borgia, F.; Benson, L.; Tay, E.L.W.; Alonso-Gonzalez, R.; Silva, M.; Charalambides, M.; Swan, L.; Dimopoulos, K.; et al. Comprehensive Use of Cardiopulmonary Exercise Testing Identifies Adults with Congenital Heart Disease at Increased Mortality Risk in the Medium Term. Circulation 2012, 125, 250–259. [Google Scholar] [CrossRef] [PubMed]
- Kipps, A.K.; Graham, D.A.; Harrild, D.M.; Lewis, E.; Powell, A.J.; Rhodes, J. Longitudinal Exercise Capacity of Patients with Repaired Tetralogy of Fallot. Am. J. Cardiol. 2011, 108, 99–105. [Google Scholar] [CrossRef]
- Villaseca-Rojas, Y.; Varela-Melo, J.; Torres-Castro, R.; Vasconcello-Castillo, L.; Mazzucco, G.; Vilaró, J.; Blanco, I. Exercise Capacity in Children and Adolescents With Congenital Heart Disease: A Systematic Review and Meta-Analysis. Front. Cardiovasc. Med. 2022, 9, 990. [Google Scholar] [CrossRef]
- Fredriksen, P.M.; Veldtman, G.; Hechter, S.; Therrien, J.; Chen, A.; Warsi, M.A.; Freeman, M.; Liu, P.; Siu, S.; Thaulow, E.; et al. Aerobic Capacity in Adults with Various Congenital Heart Diseases. Am. J. Cardiol. 2001, 87, 310–314. [Google Scholar] [CrossRef] [PubMed]
- Diller, G.P.; Dimopoulos, K.; Okonko, D.; Li, W.; Babu-Narayan, S.V.; Broberg, C.S.; Johansson, B.; Bouzas, B.; Mullen, M.J.; Poole-Wilson, P.A.; et al. Exercise Intolerance in Adult Congenital Heart Disease: Comparative Severity, Correlates, and Prognostic Implication. Circulation 2005, 112, 828–835. [Google Scholar] [CrossRef]
- Patti, A.; Neunhaeuserer, D.; Gasperetti, A.; Baioccato, V.; Vecchiato, M.; Battista, F.; Marchini, F.; Bergamin, M.; Furian, L.; Ermolao, A. Overshoot of the Respiratory Exchange Ratio during Recovery from Maximal Exercise Testing in Kidney Transplant Recipients. Int. J. Environ. Res. Public Health 2021, 18, 9236. [Google Scholar] [CrossRef] [PubMed]
- Neunhaeuserer, D.; Gasperetti, A.; Savalla, F.; Gobbo, S.; Bullo, V.; Bergamin, M.; Foletto, M.; Vettor, R.; Zaccaria, M.; Ermolao, A. Functional Evaluation in Obese Patients Before and After Sleeve Gastrectomy. Obes. Surg. 2017, 27, 3230–3239. [Google Scholar] [CrossRef] [PubMed]
- Malhotra, R.; Bakken, K.; D’Elia, E.; Lewis, G.D. Cardiopulmonary Exercise Testing in Heart Failure. JACC Heart Fail. 2016, 4, 607–616. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | Controls (n = 24) | CHD (n = 93) | TGA (n = 23) | Fon (n = 22) | CoA (n = 24) | ToF (n = 24) |
|---|---|---|---|---|---|---|
| Gender—females, n (%) | 11 (46%) | 34 (37%) | 4 (17%) | 9 (41%) | 9 (38%) | 12 (50%) |
| Age (years) | 14.84 ± 2.69 | 14.41 ± 3.18 | 14.39 ± 2.79 | 14.86 ± 2.92 | 13.88 ± 3.35 | 14.54 ± 3.66 |
| Height (cm) | 156.00 ± 14.60 | 161.50 ± 13.51 | 164.80 ± 10.53 | 161.82 ± 14.90 | 159.30 ± 13.80 | 160.25 ± 14.65 |
| BMI (kg/m2) | 19.55 ± 2.64 | 20.70 ± 4.38 | 22.52 ± 5.23 | 19.06 ± 2.42 | 20.45 ± 4.41 | 20.69 ± 4.46 |
| SBP rest (mmHg) | 106.20 ± 15.10 | 114.25 ± 14.38 | 118.22 ± 11.92 | 104.64 ± 15.05 | 119.92 ± 14.65 | 113.60 ± 11.50 |
| DBP rest (mmHg) | 53.80 ± 9.50 | 64.92 ± 9.80 | 63.35 ± 10.30 | 63.60 ± 8.61 | 66.12 ± 9.64 | 66.50 ± 10.65 |
| Desaturation at rest, n (%) | 0 (0%) | 5 (5%) | 0 (0%) | 5 (23%) | 0 (0%) | 0 (0%) |
| Competitive sports, n (%) | 23 (96%) | 2 (2%) | 0 (0%) | 0 (0%) | 2 (8%) | 0 (0%) |
| Physical activity (h/week) | 5.42 ± 2.67 | 2.26 ± 1.33 | 2.14 ± 1.58 | 2.02 ± 1.32 | 2.68 ± 1.38 | 2.12 ± 1.11 |
| Cardio-Aspirine, n (%) | 0 (0%) | 72 (77%) | 1 (4%) | 18 (82%) | 0 (0%) | 2 (8%) |
| Anti-hypertensive drugs, n (%) | 0 (0%) | 9 (10%) | 1 (4%) | 7 (32%) | 1 (4%) | 0 (0%) |
| Variables | Controls (n = 24) | CHD (n = 93) | p | TGA (n = 23) | Fon (n = 22) | CoA (n = 24) | ToF (n = 24) | p |
|---|---|---|---|---|---|---|---|---|
| HR peak (bpm) | 190.00 (185.35–192.89) | 184.00 (178.21–185.41) | 0.013 | 187.00 (173.36–193.25) | 176.00 (166.44–180.10) | 190.00 (184.74–194.51) | 182.50 (174.01–186.74) | <0.001 |
| HR peak (%) | 91.00 (89.82–93.70) | 90.00 (86.41–89.97) | 0.042 | 92.00 (84.13–94.05) | 85.50 (80.80–87.65) | 92.00 (89.37–94.22) | 89.00 (84.22–90.53) | <0.001 |
| HRRec 1 (-bpm) | −33.00 (−44.12/−30.84) | −26.00 (−31.03/−25.71) | 0.007 | −28.00 (−35.61–(−24.13)) | −18.50 (−25.79–(−16.39)) | −30.00 (−37.50–(−27.34)) | −26.00 (−35.20–(−23.88)) | 0.001 |
| HR/VO2 slope (bpm/mL) | 7.03 ± 3.12 | 8.34 ± 3.34 | 0.140 | 7.30 ± 2.65 | 9.27 ± 3.72 | 7.28 ± 2.42 | 9.55 ± 3.87 | 0.048 |
| O2 pulse (mL/bpm) | 11.10 (10.45- 13.55) | 10.20 (10.25–11.69) | 0.174 | 11.10 (11.27–13.77) | 8.85 (8.44–10.76) | 10.85 (9.61–13.07) | 9.05 (8.83–11.92) | 0.004 |
| O2 pulse (%) | 104.00 (100.93–118.19) | 93.00 (91.02–99.63) | 0.005 | 100.00 (90.19–109.38) | 86.00 (76.20–96.98) | 97.50 (92.38–108.70) | 92.00 (86.76–100.91) | 0.004 |
| Oxygen Pulse Behaviour | Normal: 24 (100%) | Normal: 65 (70%) Early Plateau: 25 (27%) Deflection: 3 (3%) | 0.007 | Normal: 15 (65%) Early Plateau: 6 (26%) Deflection: 2 (9%) | Normal: 16 (73%) Early Plateau: 6 (27%) Deflection: 0 | Normal: 21 (87%) Early Plateau: 3 (12%) Deflection: 0 | Normal: 13 (54%) Early Plateau: 10 (42%) Deflection: 1 (4%) | 0.147 |
| SBP peak (mmHg) | 150.00 (140.60–157.00) | 150.00 (143.9–153.40) | 0.947 | 150.00 (142.77–157.66) | 137.50 (130.25–147.02) | 150.00 (146.54–168.88) | 147.50 (136.69–157.89) | 0.152 |
| DBP peak (mmHg) | 50.00 (45.48–56.12) | 60.00 (58.29–64.40) | <0.001 | 60.00 (55.90–69.75) | 60.00 (54.24–65.77) | 50.00 (52.37–65.55) | 60.00 (57.27–69.81) | 0.012 |
| SpO2 peak (%) | 99.00 (98.86–99.53) | 96.00 (95.11–96.84) | <0.001 | 98.00 (97.37–98.36) | 92.00 (89.46–94.14) | 98.00 (97.03–98.88) | 97.50 (93.85–97.42) | <0.001 |
| Desaturation at peak, n (%) | 0 (0%) | 19 (21%) | 0.012 | 0 (0%) | 12 (60%) | 1 (4%) | 6 (27%) | <0.001 |
| VE/VCO2 slope | 27.93 (26.36–29.35) | 29.14 (28.73–30.61) | 0.102 | 28.25 (27.14–30.72) | 31.06 (29.10–33.20) | 28.17 (26.47–30.47) | 28.68 (28.28–32.17) | 0.120 |
| OUES (mL/logL) | 1849.19 (1739.05–2281.50) | 1784.00 (1739.96–1994.13) | 0.365 | 1990.00 (1804.69–2220.96) | 1613.50 (1460.38–1949.52) | 1887.50 (1695.67–2342.09) | 1565.50 (1475.68–1972.49) | 0.087 |
| VO2 peak (mL/min/kg) | 43.72 ± 6.13 | 36.27 ± 8.33 | <0.001 | 36.83 ± 8.70 | 32.05 ± 5.90 | 40.98 ± 8.40 | 34.90 ± 7.85 | <0.001 |
| VO2 peak (%) | 108.84 ± 15.82 | 86.70 ± 17.90 | <0.001 | 83.30 ± 15.80 | 76.64 ± 14.40 | 99.00 ± 17.10 | 86.92 ± 17.10 | <0.001 |
| VO2 at VT (mL/Kg/min) | 23.90 (22.34–26.22) | 22.80 (21.81–24.50) | 0.229 | 22.80 (21.11–24.22) | 21.40 (19.47–22.89) | 25.60 (22.82–26.26) | 21.60 (19.19–29.06) | 0.085 |
| VO2 at RCP (mL/Kg/min) | 34.50 (32.28–38.89) | 28.200 (27.69–30.57) | <0.001 | 28.80 (25.93–31.63) | 25.10 (23.52–28.75) | 31.45 (29.83–36.15) | 28.00 (25.50–30.76) | <0.001 |
| METs | 16.76 ± 2.09 | 15.03 ± 2.48 | 0.001 | 15.00 ± 2.61 | 14.72 ± 1.95 | 15.65 ± 2.80 | 14.75 ± 2.52 | 0.040 |
| LVEF * (%) | - | 64.00 (60.00–70.00) | - | 63.00 (61.25–69.00) | 58.00 (50.47–63.24) | 68.00 (64.51–70.93) | 66.00 (61.08–68.52) | 0.002 |
| TAPSE ** (mm) | - | 19.00 (16.40–22.10) | - | 17.00 (15.21–18.10) | 12.60 (9.15–18.59) | 25.10 (22.24–27.10) | 19.00 (16.67–20.59) | <0.001 |
| FAC *** (%) | - | 44.50 (40.00–48.00) | - | 40.50 (34.15–46.85) | 48.00 (33.63–55.17) | 42.50 (37.60–47.40) | 44.00 (38.89–46.66) | 0.392 |
| Variables | Controls (n = 24) | CHD (n = 93) | p | TGA (n = 23) | Fon (n = 22) | CoA (n = 24) | ToF (n = 24) | p |
|---|---|---|---|---|---|---|---|---|
| RER peak | 1.22 ± 0.11 | 1.23 ± 0.12 | 0.819 | 1.24 ± 0.14 | 1.22 ± 0.11 | 1.20 ± 0.12 | 1.24 ± 0.10 | 0.902 |
| RER max | 1.94 ± 0.28 | 1.77 ± 0.23 | 0.010 | 1.80 ± 0.25 | 1.74 ± 0.24 | 1.80 ± 0.21 | 1.75 ± 0.24 | 0.076 |
| RER mag (%) | 58.54 ± 14.72 | 44.41 ± 14.75 | 0.010 | 43.74 ± 13.81 | 42.31 ± 13.10 | 49.95 ± 15.23 | 41.42 ± 15.94 | 0.001 |
| RER slope | 34.40 ± 16.50 | 27.63 ± 13.52 | 0.037 | 29.81 ± 15.40 | 23.12 ± 10.84 | 28.80 ± 13.70 | 28.50 ± 13.60 | 0.207 |
| Time to RER max (s) | 146.00 (126.31–164.17) | 139.00 (129.47–151.50) | 0.403 | 130.00 (107.60–151.87) | 151.50 (137.58–186.60) | 145.00 (119.90–170.51) | 119.00 (108.58–143.92) | 0.136 |
| Variables | RER Peak | RER Max | RER Mag | RER Slope | Time to RER Max |
|---|---|---|---|---|---|
| Age (years) | 0.428 (p = 0.001) | 0.277 (p = 0.007) | −0.034 (p = 0.744) | −0.085 (p = 0.418) | 0.174 (p = 0.095) |
| HR peak (bpm) | 0.227 (p = 0.021) | 0.323 (p = 0.001) | 0.366 (p = 0.001) | 0.297 (p = 0.004) | −0.042 (p = 0.692) |
| HR/VO2 slope (bpm/mL) | 0.059 (p = 0.581) | −0.135 (p = 0.103) | −0.232 (p = 0.004) | −0.154 (p = 0.418) | −0.095 (p = 0.089) |
| HRRec 1 (-bpm) | 0.412 (p < 0.001) | 0.253 (p = 0.014) | −0.042 (p = 0.687) | 0.122 (p = 0.242) | 0.006 (p = 0.950) |
| VE/VCO2 slope | −0.429 (p = 0.001) | −0.343 (p = 0.001) | −0.100 (p = 0.334) | −0.201 (p = 0.054) | −0.021 (p = 0.840) |
| VO2 at VT (ml/kg/min) | −0.265 (p = 0.008) | −0.115 (p = 0.274) | 0.100 (p = 0.343) | 0.123 (p = 0.245) | −0.060 (p = 0.573) |
| VO2 peak (ml/kg/min) | −0.100 (p = 0.314) | 0.212 (p = 0.040) | 0.393 (p = 0.001) | 0.297 (p = 0.004) | −0.048 (p = 0.650) |
| OUES (ml/logL) | 0.213 (p = 0.031) | 0.370 (p = 0.001) | 0.311 (p = 0.002) | 0.137 (p = 0.191) | 0.143 (p = 0.170) |
| LVEF (%) | 0.056 (p = 0.608) | −0.003 (p = 0.975) | 0.002 (p = 0.989) | 0.083 (p = 0.449) | −0.072 (p = 0.510) |
| TAPSE (mm) | 0.241 (p = 0.057) | 0.312 (p = 0.012) | 0.151 (p = 0.234) | −0.083 (p = 0.516) | 0.192 (p = 0.132) |
| FAC (%) | 0.199 (p = 0.365) | −0.068 (p = 0.764) | −0.065 (p = 0.772) | 0.035 (p = 0.877) | −0.090 (p = 0.692) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vecchiato, M.; Ermolao, A.; Zanardo, E.; Battista, F.; Ruvoletto, G.; Palermi, S.; Quinto, G.; Degano, G.; Gasperetti, A.; Padalino, M.A.; et al. Overshoot of the Respiratory Exchange Ratio during Recovery from Maximal Exercise Testing in Young Patients with Congenital Heart Disease. Children 2023, 10, 521. https://doi.org/10.3390/children10030521
Vecchiato M, Ermolao A, Zanardo E, Battista F, Ruvoletto G, Palermi S, Quinto G, Degano G, Gasperetti A, Padalino MA, et al. Overshoot of the Respiratory Exchange Ratio during Recovery from Maximal Exercise Testing in Young Patients with Congenital Heart Disease. Children. 2023; 10(3):521. https://doi.org/10.3390/children10030521
Chicago/Turabian StyleVecchiato, Marco, Andrea Ermolao, Emanuele Zanardo, Francesca Battista, Giacomo Ruvoletto, Stefano Palermi, Giulia Quinto, Gino Degano, Andrea Gasperetti, Massimo A. Padalino, and et al. 2023. "Overshoot of the Respiratory Exchange Ratio during Recovery from Maximal Exercise Testing in Young Patients with Congenital Heart Disease" Children 10, no. 3: 521. https://doi.org/10.3390/children10030521
APA StyleVecchiato, M., Ermolao, A., Zanardo, E., Battista, F., Ruvoletto, G., Palermi, S., Quinto, G., Degano, G., Gasperetti, A., Padalino, M. A., Di Salvo, G., & Neunhaeuserer, D. (2023). Overshoot of the Respiratory Exchange Ratio during Recovery from Maximal Exercise Testing in Young Patients with Congenital Heart Disease. Children, 10(3), 521. https://doi.org/10.3390/children10030521