
Neuropsychological Outcomes of Children Treated for Brain Tumors

 ,
, 
Abstract
1. Introduction
2. Epidemiology of Brain Tumors in Children
3. Neurologic and Sensory Late Effects
4. Cognitive and Neuropsychological Outcomes
4.1. Attention, Working Memory, and Processing Speed
4.2. Executive Functions
5. Factors Influencing Neurologic and Cognitive Outcomes
5.1. Individual Patient Characteristics
5.2. Tumor-Related Factors
5.2.1. Tumor Location
5.2.2. Obstructive Hydrocephalus
5.3. Treatment-Related Factors
5.3.1. Neurosurgery
5.3.2. Radiotherapy
5.3.3. Chemotherapy
5.4. Environmental Factors
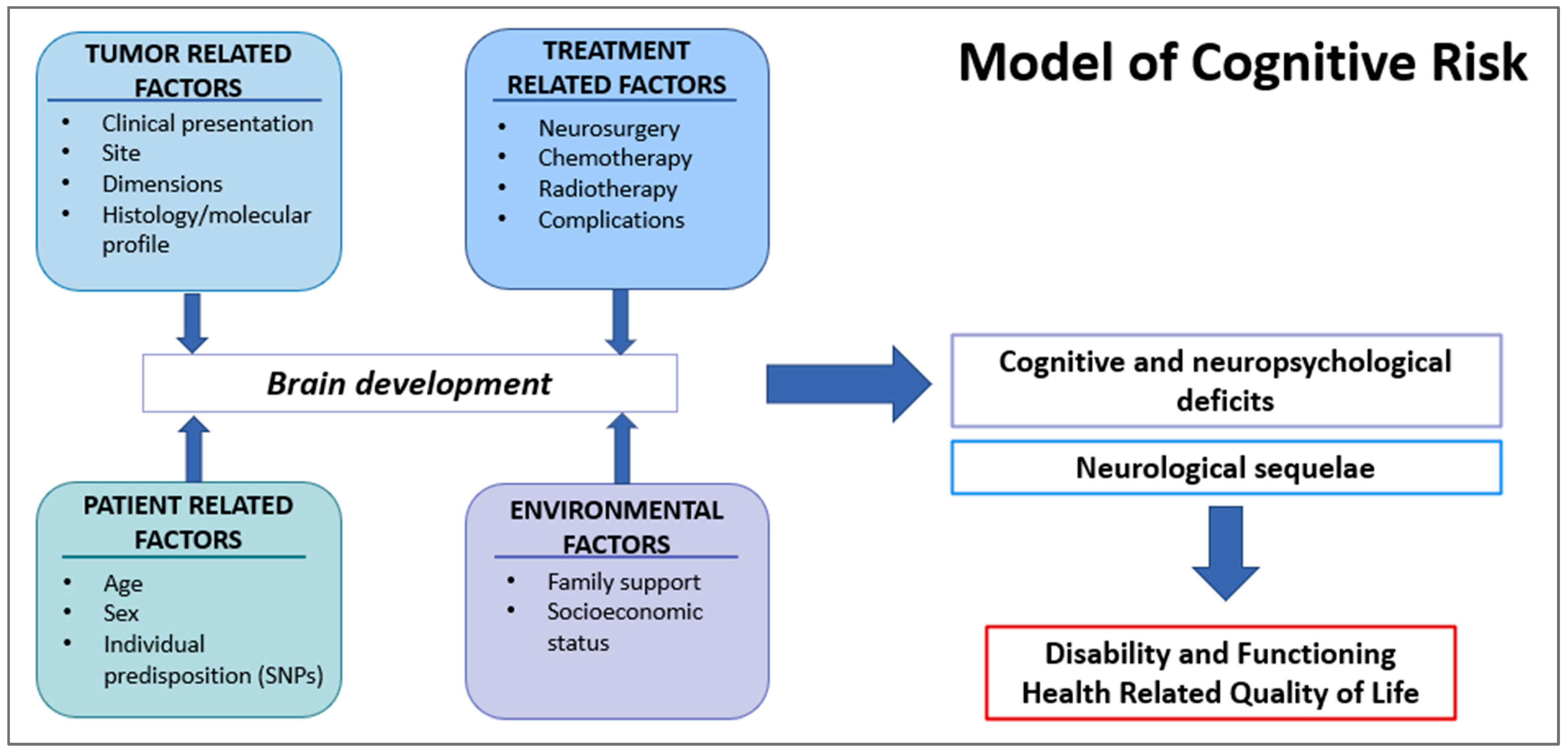
6. Neurodevelopmental Framework
7. Strategy of Monitoring and Potential Intervention
7.1. Who Is at Major Risk?
7.2. How to Screen and Follow-Up with These Patients?
7.3. When to Start Follow-Up and for How Long It Is Recommended to Continue It?
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kline, C.N.; Mueller, S. Neurocognitive Outcomes in Children with Brain Tumors. Semin. Neurol. 2020, 40, 315–321. [Google Scholar] [CrossRef]
- Blaney, S.M.; Adamson, P.C.; Helman, L.J. Pizzo and Poplack’s Pediatric Oncology; Wolters Kluwer Health: Philadelphia, PA, USA, 2020. [Google Scholar]
- Roddy, E.; Mueller, S. Late Effects of Treatment of Pediatric Central Nervous System Tumors. J. Child Neurol. 2016, 31, 237–254. [Google Scholar] [CrossRef] [PubMed]
- Ostrom, Q.T.; Price, M.; Ryan, K.; Edelson, J.; Neff, C.; Cioffi, G.; Waite, K.A.; Kruchko, C.; Barnholtz-Sloan, J.S. CBTRUS Statistical Report: Pediatric Brain Tumor Foundation Childhood and Adolescent Primary Brain and Other Central Nervous System Tumors Diagnosed in the United States in 2014–2018. Neuro-Oncology 2022, 24, iii1–iii38. [Google Scholar] [CrossRef] [PubMed]
- Miller, K.D.; Ostrom, Q.T.; Kruchko, C.; Patil, N.; Tihan, T.; Cioffi, G.; Fuchs, H.E.; Waite, K.A.; Jemal, A.; Siegel, R.L.; et al. Brain and other central nervous system tumor statistics, 2021. CA Cancer J. Clin. 2021, 71, 381–406. [Google Scholar] [CrossRef] [PubMed]
- Landier, W.; Skinner, R.; Wallace, W.H.; Hjorth, L.; Mulder, R.L.; Wong, F.L.; Yasui, Y.; Bhakta, N.; Constine, L.S.; Bhatia, S.; et al. Surveillance for Late Effects in Childhood Cancer Survivors. J. Clin. Oncol. 2018, 36, 2216–2222. [Google Scholar] [CrossRef]
- Hudson, M.M.; Mertens, A.C.; Yasui, Y.; Hobbie, W.; Chen, H.; Gurney, J.G.; Yeazel, M.; Recklitis, C.J.; Marina, N.; Robison, L.R.; et al. Health status of adult long-term survivors of childhood cancer: A report from the Childhood Cancer Survivor Study. JAMA 2003, 290, 1583–1592. [Google Scholar] [CrossRef]
- Ullrich, N.J.; Embry, L. Neurocognitive dysfunction in survivors of childhood brain tumors. Semin. Pediatr. Neurol. 2012, 19, 35–42. [Google Scholar] [CrossRef]
- Packer, R.J.; Gurney, J.G.; Punyko, J.A.; Donaldson, S.S.; Inskip, P.D.; Stovall, M.; Yasui, Y.; Mertens, A.C.; Sklar, C.A.; Nicholson, H.S.; et al. Long-term neurologic and neurosensory sequelae in adult survivors of a childhood brain tumor: Childhood cancer survivor study. J. Clin. Oncol. 2003, 21, 3255–3261. [Google Scholar] [CrossRef]
- Puhr, A.; Ruud, E.; Anderson, V.; Due-Tonnesen, B.J.; Skarbo, A.B.; Finset, A.; Andersson, S. Self-Reported Executive Dysfunction, Fatigue, and Psychological and Emotional Symptoms in Physically Well-Functioning Long-Term Survivors of Pediatric Brain Tumor. Dev. Neuropsychol. 2019, 44, 88–103. [Google Scholar] [CrossRef]
- Palmer, S.L.; Armstrong, C.; Onar-Thomas, A.; Wu, S.; Wallace, D.; Bonner, M.J.; Schreiber, J.; Swain, M.; Chapieski, L.; Mabbott, D.; et al. Processing speed, attention, and working memory after treatment for medulloblastoma: An international, prospective, and longitudinal study. J. Clin. Oncol. 2013, 31, 3494–3500. [Google Scholar] [CrossRef]
- Pietila, S.; Korpela, R.; Lenko, H.L.; Haapasalo, H.; Alalantela, R.; Nieminen, P.; Koivisto, A.M.; Makipernaa, A. Neurological outcome of childhood brain tumor survivors. J. Neurooncol. 2012, 108, 153–161. [Google Scholar] [CrossRef] [PubMed]
- Orkin, S.H.; Nathan, D.G.; Ginsburg, D.; Look, A.T.; Fisher, D.E.; Lux, S. Nathan and Oski’s Hematology and Oncology of Infancy and Childhood E-Book; Elsevier Health Sciences: Amsterdam, The Netherlands, 2014. [Google Scholar]
- Louis, D.N.; Perry, A.; Wesseling, P.; Brat, D.J.; Cree, I.A.; Figarella-Branger, D.; Hawkins, C.; Ng, H.K.; Pfister, S.M.; Reifenberger, G.; et al. The 2021 WHO Classification of Tumors of the Central Nervous System: A summary. Neuro-Oncology 2021, 23, 1231–1251. [Google Scholar] [CrossRef] [PubMed]
- Murphy, C.; Upshaw, N.C.; Thomas, A.S.; Fong, G.; Janss, A.; Mazewski, C.; Ingerski, L.M. Impact of executive functioning on health-related quality of life of pediatric brain tumor survivors. Pediatr. Blood Cancer 2021, 68, e29130. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, G.T.; Liu, Q.; Yasui, Y.; Huang, S.; Ness, K.K.; Leisenring, W.; Hudson, M.M.; Donaldson, S.S.; King, A.A.; Stovall, M.; et al. Long-term outcomes among adult survivors of childhood central nervous system malignancies in the Childhood Cancer Survivor Study. J. Natl. Cancer Inst. 2009, 101, 946–958. [Google Scholar] [CrossRef]
- Phillips, N.S.; Khan, R.B.; Li, C.; Mirzaei Salehabadi, S.; Brinkman, T.M.; Srivastava, D.; Robison, L.L.; Hudson, M.M.; Krull, K.R.; Sadighi, Z.S. Seizures’ impact on cognition and quality of life in childhood cancer survivors. Cancer 2022, 128, 180–191. [Google Scholar] [CrossRef]
- Brinkman, T.M.; Krasin, M.J.; Liu, W.; Armstrong, G.T.; Ojha, R.P.; Sadighi, Z.S.; Gupta, P.; Kimberg, C.; Srivastava, D.; Merchant, T.E.; et al. Long-Term Neurocognitive Functioning and Social Attainment in Adult Survivors of Pediatric CNS Tumors: Results From the St Jude Lifetime Cohort Study. J. Clin. Oncol. 2016, 34, 1358–1367. [Google Scholar] [CrossRef]
- Rey-Casserly, C.; Diver, T. Late effects of pediatric brain tumors. Curr. Opin. Pediatr. 2019, 31, 789–796. [Google Scholar] [CrossRef]
- Oyefiade, A.; Paltin, I.; De Luca, C.R.; Hardy, K.K.; Grosshans, D.R.; Chintagumpala, M.; Mabbott, D.J.; Kahalley, L.S. Cognitive Risk in Survivors of Pediatric Brain Tumors. J. Clin. Oncol. 2021, 39, 1718–1726. [Google Scholar] [CrossRef]
- Kros, C.J.; Steyger, P.S. Aminoglycoside- and Cisplatin-Induced Ototoxicity: Mechanisms and Otoprotective Strategies. Cold Spring Harb. Perspect. Med. 2019, 9, a033548. [Google Scholar] [CrossRef]
- Freyer, D.R.; Brock, P.R.; Chang, K.W.; Dupuis, L.L.; Epelman, S.; Knight, K.; Mills, D.; Phillips, R.; Potter, E.; Risby, D.; et al. Prevention of cisplatin-induced ototoxicity in children and adolescents with cancer: A clinical practice guideline. Lancet Child Adolesc. Health 2020, 4, 141–150. [Google Scholar] [CrossRef]
- Bass, J.K.; Hua, C.H.; Huang, J.; Onar-Thomas, A.; Ness, K.K.; Jones, S.; White, S.; Bhagat, S.P.; Chang, K.W.; Merchant, T.E. Hearing Loss in Patients Who Received Cranial Radiation Therapy for Childhood Cancer. J. Clin. Oncol. 2016, 34, 1248–1255. [Google Scholar] [CrossRef] [PubMed]
- Merchant, T.E.; Gould, C.J.; Xiong, X.; Robbins, N.; Zhu, J.; Pritchard, D.L.; Khan, R.; Heideman, R.L.; Krasin, M.J.; Kun, L.E. Early neuro-otologic effects of three-dimensional irradiation in children with primary brain tumors. Int. J. Radiat. Oncol. Biol. Phys. 2004, 58, 1194–1207. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Abongwa, C.; Ashwal, S.; Deming, D.D.; Winter, T.W. Referral for Ophthalmology Evaluation and Visual Sequelae in Children With Primary Brain Tumors. JAMA Netw. Open 2019, 2, e198273. [Google Scholar] [CrossRef]
- Sun, L.R.; Cooper, S. Neurological Complications of the Treatment of Pediatric Neoplastic Disorders. Pediatr. Neurol. 2018, 85, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Wells, E.M.; Ullrich, N.J.; Seidel, K.; Leisenring, W.; Sklar, C.A.; Armstrong, G.T.; Diller, L.; King, A.; Krull, K.R.; Neglia, J.P.; et al. Longitudinal assessment of late-onset neurologic conditions in survivors of childhood central nervous system tumors: A Childhood Cancer Survivor Study report. Neuro-Oncology 2018, 20, 132–142. [Google Scholar] [CrossRef]
- Castellino, S.M.; Ullrich, N.J.; Whelen, M.J.; Lange, B.J. Developing interventions for cancer-related cognitive dysfunction in childhood cancer survivors. J. Natl. Cancer Inst. 2014, 106, dju186. [Google Scholar] [CrossRef]
- Stavinoha, P.L.; Askins, M.A.; Powell, S.K.; Pillay Smiley, N.; Robert, R.S. Neurocognitive and Psychosocial Outcomes in Pediatric Brain Tumor Survivors. Bioengineering 2018, 5, 73. [Google Scholar] [CrossRef]
- Doger de Speville, E.; Kieffer, V.; Dufour, C.; Grill, J.; Noulhiane, M.; Hertz-Pannier, L.; Chevignard, M. Neuropsychological consequences of childhood medulloblastoma and possible interventions: A review. Neurochirurgie 2021, 67, 90–98. [Google Scholar] [CrossRef]
- Palmer, S.L.; Gajjar, A.; Reddick, W.E.; Glass, J.O.; Kun, L.E.; Wu, S.; Xiong, X.; Mulhern, R.K. Predicting intellectual outcome among children treated with 35-40 Gy craniospinal irradiation for medulloblastoma. Neuropsychology 2003, 17, 548–555. [Google Scholar] [CrossRef]
- Chevignard, M.; Camara-Costa, H.; Doz, F.; Dellatolas, G. Core deficits and quality of survival after childhood medulloblastoma: A review. Neurooncol. Pract. 2017, 4, 82–97. [Google Scholar] [CrossRef]
- Edelstein, K.; Spiegler, B.J.; Fung, S.; Panzarella, T.; Mabbott, D.J.; Jewitt, N.; D’Agostino, N.M.; Mason, W.P.; Bouffet, E.; Tabori, U.; et al. Early aging in adult survivors of childhood medulloblastoma: Long-term neurocognitive, functional, and physical outcomes. Neuro-Oncology 2011, 13, 536–545. [Google Scholar] [CrossRef] [PubMed]
- Meyers, C.A.; Perry, J.R. Cognition and Cancer; Cambridge University Press: Cambridge, UK, 2012. [Google Scholar]
- Margelisch, K.; Studer, M.; Ritter, B.C.; Steinlin, M.; Leibundgut, K.; Heinks, T. Cognitive dysfunction in children with brain tumors at diagnosis. Pediatr. Blood Cancer 2015, 62, 1805–1812. [Google Scholar] [CrossRef] [PubMed]
- Puhr, A.; Ruud, E.; Anderson, V.; Due-Tonnessen, B.J.; Skarbo, A.B.; Finset, A.; Andersson, S. Executive Function and Psychosocial Adjustment in Adolescent Survivors of Pediatric Brain Tumor. Dev. Neuropsychol. 2021, 46, 149–168. [Google Scholar] [CrossRef] [PubMed]
- Anderson, P.J.; Reidy, N. Assessing executive function in preschoolers. Neuropsychol. Rev. 2012, 22, 345–360. [Google Scholar] [CrossRef]
- De Ruiter, M.A.; van Mourik, R.; Schouten-van Meeteren, A.Y.N.; Grootenhuis, M.A.; Oosterlaan, J. Neurocognitive consequences of a paediatric brain tumour and its treatment: A meta-analysis. Dev. Med. Child Neurol. 2013, 55, 408–417. [Google Scholar] [CrossRef]
- Lafay-Cousin, L.; Fay-McClymont, T.; Johnston, D.; Fryer, C.; Scheinemann, K.; Fleming, A.; Hukin, J.; Janzen, L.; Guger, S.; Strother, D.; et al. Neurocognitive evaluation of long term survivors of atypical teratoid rhabdoid tumors (ATRT): The Canadian registry experience. Pediatr. Blood Cancer 2015, 62, 1265–1269. [Google Scholar] [CrossRef] [PubMed]
- Clark, K.N.; Ashford, J.M.; Pai Panandiker, A.S.; Klimo, P.; Merchant, T.E.; Billups, C.A.; Conklin, H.M. Cognitive outcomes among survivors of focal low-grade brainstem tumors diagnosed in childhood. J. Neurooncol. 2016, 129, 311–317. [Google Scholar] [CrossRef]
- Moxon-Emre, I.; Bouffet, E.; Taylor, M.D.; Laperriere, N.; Scantlebury, N.; Law, N.; Spiegler, B.J.; Malkin, D.; Janzen, L.; Mabbott, D. Impact of craniospinal dose, boost volume, and neurologic complications on intellectual outcome in patients with medulloblastoma. J. Clin. Oncol. 2014, 32, 1760–1768. [Google Scholar] [CrossRef]
- Roncadin, C.; Dennis, M.; Greenberg, M.L.; Spiegler, B.J. Adverse medical events associated with childhood cerebellar astrocytomas and medulloblastomas: Natural history and relation to very long-term neurobehavioral outcome. Childs Nerv. Syst. 2008, 24, 995–1002; discussion 1003. [Google Scholar] [CrossRef]
- Law, N.; Smith, M.L.; Greenberg, M.; Bouffet, E.; Taylor, M.D.; Laughlin, S.; Malkin, D.; Liu, F.; Moxon-Emre, I.; Scantlebury, N.; et al. Executive function in paediatric medulloblastoma: The role of cerebrocerebellar connections. J. Neuropsychol. 2017, 11, 174–200. [Google Scholar] [CrossRef]
- Heitzer, A.M.; Raghubar, K.; Ris, M.D.; Minard, C.G.; Gragert, M.N.; Stancel, H.H.; Orobio, J.; Xue, J.; Whitehead, W.; Okcu, M.F.; et al. Neuropsychological functioning following surgery for pediatric low-grade glioma: A prospective longitudinal study. J. Neurosurg. Pediatr. 2019, 25, 251–259. [Google Scholar] [CrossRef] [PubMed]
- Koustenis, E.; Hernaiz Driever, P.; de Sonneville, L.; Rueckriegel, S.M. Executive function deficits in pediatric cerebellar tumor survivors. Eur. J. Paediatr. Neurol. 2016, 20, 25–37. [Google Scholar] [CrossRef] [PubMed]
- Decker, A.L.; Szulc, K.U.; Bouffet, E.; Laughlin, S.; Chakravarty, M.M.; Skocic, J.; de Medeiros, C.B.; Mabbott, D.J. Smaller hippocampal subfield volumes predict verbal associative memory in pediatric brain tumor survivors. Hippocampus 2017, 27, 1140–1154. [Google Scholar] [CrossRef] [PubMed]
- Weusthof, K.; Luttich, P.; Regnery, S.; Konig, L.; Bernhardt, D.; Witt, O.; Herfarth, K.; Unterberg, A.; Jungk, C.; Farnia, B.; et al. Neurocognitive Outcomes in Pediatric Patients Following Brain Irradiation. Cancers 2021, 13, 3538. [Google Scholar] [CrossRef]
- King, T.Z.; Ailion, A.S.; Fox, M.E.; Hufstetler, S.M. Neurodevelopmental model of long-term outcomes of adult survivors of childhood brain tumors. Child Neuropsychol. 2019, 25, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Krull, K.R.; Hardy, K.K.; Kahalley, L.S.; Schuitema, I.; Kesler, S.R. Neurocognitive Outcomes and Interventions in Long-Term Survivors of Childhood Cancer. J. Clin. Oncol. 2018, 36, 2181–2189. [Google Scholar] [CrossRef]
- Corti, C.; Manfredi, V.; Massimino, M.; Bardoni, A.; Borgatti, R.; Poggi, G. Cognitive functioning of pediatric patients with brain tumor: An investigation of the role of gender. Childs Nerv. Syst. 2018, 34, 2415–2423. [Google Scholar] [CrossRef]
- Bledsoe, J.C.; Breiger, D.; Breiger, M.; Shonka, S.; Ermoian, R.P.; Ojemann, J.G.; Werny, D.M.; Leary, S.E.S.; Geyer, J.R. Differential trajectories of neurocognitive functioning in females versus males following treatment for pediatric brain tumors. Neuro-Oncology 2019, 21, 1310–1318. [Google Scholar] [CrossRef]
- Fouladi, M.; Gilger, E.; Kocak, M.; Wallace, D.; Buchanan, G.; Reeves, C.; Robbins, N.; Merchant, T.; Kun, L.E.; Khan, R.; et al. Intellectual and functional outcome of children 3 years old or younger who have CNS malignancies. J. Clin. Oncol. 2005, 23, 7152–7160. [Google Scholar] [CrossRef]
- Correa, D.D.; Satagopan, J.; Cheung, K.; Arora, A.K.; Kryza-Lacombe, M.; Xu, Y.; Karimi, S.; Lyo, J.; DeAngelis, L.M.; Orlow, I. COMT, BDNF, and DTNBP1 polymorphisms and cognitive functions in patients with brain tumors. Neuro-Oncology 2016, 18, 1425–1433. [Google Scholar] [CrossRef]
- Wefel, J.S.; Noll, K.R.; Scheurer, M.E. Neurocognitive functioning and genetic variation in patients with primary brain tumours. Lancet Oncol. 2016, 17, e97–e108. [Google Scholar] [CrossRef] [PubMed]
- Kamdar, K.Y.; Krull, K.R.; El-Zein, R.A.; Brouwers, P.; Potter, B.S.; Harris, L.L.; Holm, S.; Dreyer, Z.; Scaglia, F.; Etzel, C.J.; et al. Folate pathway polymorphisms predict deficits in attention and processing speed after childhood leukemia therapy. Pediatr. Blood Cancer 2011, 57, 454–460. [Google Scholar] [CrossRef] [PubMed]
- Oyefiade, A.; Erdman, L.; Goldenberg, A.; Malkin, D.; Bouffet, E.; Taylor, M.D.; Ramaswamy, V.; Scantlebury, N.; Law, N.; Mabbott, D.J. PPAR and GST polymorphisms may predict changes in intellectual functioning in medulloblastoma survivors. J. Neurooncol. 2019, 142, 39–48. [Google Scholar] [CrossRef]
- Barahmani, N.; Carpentieri, S.; Li, X.N.; Wang, T.; Cao, Y.; Howe, L.; Kilburn, L.; Chintagumpala, M.; Lau, C.; Okcu, M.F. Glutathione S-transferase M1 and T1 polymorphisms may predict adverse effects after therapy in children with medulloblastoma. Neuro-Oncology 2009, 11, 292–300. [Google Scholar] [CrossRef]
- Di Rocco, C.; Chieffo, D.; Pettorini, B.L.; Massimi, L.; Caldarelli, M.; Tamburrini, G. Preoperative and postoperative neurological, neuropsychological and behavioral impairment in children with posterior cranial fossa astrocytomas and medulloblastomas: The role of the tumor and the impact of the surgical treatment. Childs Nerv. Syst. 2010, 26, 1173–1188. [Google Scholar] [CrossRef]
- Lanier, J.C.; Abrams, A.N. Posterior fossa syndrome: Review of the behavioral and emotional aspects in pediatric cancer patients. Cancer 2017, 123, 551–559. [Google Scholar] [CrossRef]
- Riva, D.; Milani, N.; Giorgi, C.; Pantaleoni, C.; Zorzi, C.; Devoti, M. Intelligence outcome in children with shunted hydrocephalus of different etiology. Childs Nerv. Syst. 1994, 10, 70–73. [Google Scholar] [CrossRef]
- Hardy, K.K.; Bonner, M.J.; Willard, V.W.; Watral, M.A.; Gururangan, S. Hydrocephalus as a possible additional contributor to cognitive outcome in survivors of pediatric medulloblastoma. Psychooncology 2008, 17, 1157–1161. [Google Scholar] [CrossRef]
- Willard, V.W.; Berlin, K.S.; Conklin, H.M.; Merchant, T.E. Trajectories of psychosocial and cognitive functioning in pediatric patients with brain tumors treated with radiation therapy. Neuro-Oncology 2019, 21, 678–685. [Google Scholar] [CrossRef] [PubMed]
- Turner, C.D.; Chordas, C.A.; Liptak, C.C.; Rey-Casserly, C.; Delaney, B.L.; Ullrich, N.J.; Goumnerova, L.C.; Scott, R.M.; Begley, H.C.; Fletcher, W.J.; et al. Medical, psychological, cognitive and educational late-effects in pediatric low-grade glioma survivors treated with surgery only. Pediatr. Blood Cancer 2009, 53, 417–423. [Google Scholar] [CrossRef] [PubMed]
- Kahalley, L.S.; Douglas Ris, M.; Mahajan, A.; Fatih Okcu, M.; Chintagumpala, M.; Paulino, A.C.; Whitehead, W.E.; Minard, C.G.; Stancel, H.H.; Orobio, J.; et al. Prospective, longitudinal comparison of neurocognitive change in pediatric brain tumor patients treated with proton radiotherapy versus surgery only. Neuro-Oncology 2019, 21, 809–818. [Google Scholar] [CrossRef] [PubMed]
- Schreiber, J.E.; Palmer, S.L.; Conklin, H.M.; Mabbott, D.J.; Swain, M.A.; Bonner, M.J.; Chapieski, M.L.; Huang, L.; Zhang, H.; Gajjar, A. Posterior fossa syndrome and long-term neuropsychological outcomes among children treated for medulloblastoma on a multi-institutional, prospective study. Neuro-Oncology 2017, 19, 1673–1682. [Google Scholar] [CrossRef] [PubMed]
- Padovani, L.; Andre, N.; Constine, L.S.; Muracciole, X. Neurocognitive function after radiotherapy for paediatric brain tumours. Nat. Rev. Neurol. 2012, 8, 578–588. [Google Scholar] [CrossRef]
- Ajithkumar, T.; Price, S.; Horan, G.; Burke, A.; Jefferies, S. Prevention of radiotherapy-induced neurocognitive dysfunction in survivors of paediatric brain tumours: The potential role of modern imaging and radiotherapy techniques. Lancet Oncol. 2017, 18, e91–e100. [Google Scholar] [CrossRef] [PubMed]
- Kortmann, R.D.; Timmermann, B.; Taylor, R.E.; Scarzello, G.; Plasswilm, L.; Paulsen, F.; Jeremic, B.; Gnekow, A.K.; Dieckmann, K.; Kay, S.; et al. Current and future strategies in radiotherapy of childhood low-grade glioma of the brain. Part II: Treatment-related late toxicity. Strahlenther. Onkol. 2003, 179, 585–597. [Google Scholar] [CrossRef]
- Merchant, T.E.; Schreiber, J.E.; Wu, S.; Lukose, R.; Xiong, X.; Gajjar, A. Critical combinations of radiation dose and volume predict intelligence quotient and academic achievement scores after craniospinal irradiation in children with medulloblastoma. Int. J. Radiat. Oncol. Biol. Phys. 2014, 90, 554–561. [Google Scholar] [CrossRef]
- Plant-Fox, A.S.; O’Halloran, K.; Goldman, S. Pediatric brain tumors: The era of molecular diagnostics, targeted and immune-based therapeutics, and a focus on long term neurologic sequelae. Curr. Probl. Cancer 2021, 45, 100777. [Google Scholar] [CrossRef]
- Mulhern, R.K.; Merchant, T.E.; Gajjar, A.; Reddick, W.E.; Kun, L.E. Late neurocognitive sequelae in survivors of brain tumours in childhood. Lancet Oncol. 2004, 5, 399–408. [Google Scholar] [CrossRef]
- Merchant, T.E.; Kiehna, E.N.; Li, C.; Shukla, H.; Sengupta, S.; Xiong, X.; Gajjar, A.; Mulhern, R.K. Modeling radiation dosimetry to predict cognitive outcomes in pediatric patients with CNS embryonal tumors including medulloblastoma. Int. J. Radiat. Oncol. Biol. Phys. 2006, 65, 210–221. [Google Scholar] [CrossRef]
- Lawrence, Y.R.; Li, X.A.; el Naqa, I.; Hahn, C.A.; Marks, L.B.; Merchant, T.E.; Dicker, A.P. Radiation dose-volume effects in the brain. Int. J. Radiat. Oncol. Biol. Phys. 2010, 76, S20–S27. [Google Scholar] [CrossRef]
- O’Neil, S.H.; Whitaker, A.M.; Kayser, K.; Nelson, M.B.; Finlay, J.L.; Dhall, G.; Sands, S. Neuropsychological outcomes on Head Start III: A prospective, multi-institutional clinical trial for young children diagnosed with malignant brain tumors. Neurooncol. Pract. 2020, 7, 329–337. [Google Scholar] [CrossRef] [PubMed]
- Gondi, V.; Yock, T.I.; Mehta, M.P. Proton therapy for paediatric CNS tumours—Improving treatment-related outcomes. Nat. Rev. Neurol. 2016, 12, 334–345. [Google Scholar] [CrossRef] [PubMed]
- Ventura, L.M.; Grieco, J.A.; Evans, C.L.; Kuhlthau, K.A.; MacDonald, S.M.; Tarbell, N.J.; Yock, T.I.; Pulsifer, M.B. Executive functioning, academic skills, and quality of life in pediatric patients with brain tumors post-proton radiation therapy. J. Neurooncol. 2018, 137, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Gross, J.P.; Powell, S.; Zelko, F.; Hartsell, W.; Goldman, S.; Fangusaro, J.; Lulla, R.R.; Smiley, N.P.; Chang, J.H.; Gondi, V. Improved neuropsychological outcomes following proton therapy relative to X-ray therapy for pediatric brain tumor patients. Neuro-Oncology 2019, 21, 934–943. [Google Scholar] [CrossRef] [PubMed]
- Antonini, T.N.; Ris, M.D.; Grosshans, D.R.; Mahajan, A.; Okcu, M.F.; Chintagumpala, M.; Paulino, A.; Child, A.E.; Orobio, J.; Stancel, H.H.; et al. Attention, processing speed, and executive functioning in pediatric brain tumor survivors treated with proton beam radiation therapy. Radiother. Oncol. 2017, 124, 89–97. [Google Scholar] [CrossRef] [PubMed]
- Riva, D.; Giorgi, C.; Nichelli, F.; Bulgheroni, S.; Massimino, M.; Cefalo, G.; Gandola, L.; Giannotta, M.; Bagnasco, I.; Saletti, V.; et al. Intrathecal methotrexate affects cognitive function in children with medulloblastoma. Neurology 2002, 59, 48–53. [Google Scholar] [CrossRef]
- Rocque, B.G.; Cutillo, A.; Zimmerman, K.; Arynchyna, A.; Davies, S.; Landier, W.; Madan-Swain, A. Distress and psychosocial risk in families with newly diagnosed pediatric brain tumors. J. Neurosurg. Pediatr. 2018, 23, 40–47. [Google Scholar] [CrossRef]
- Berger, T.W.; Ahuja, A.; Courellis, S.H.; Deadwyler, S.A.; Erinjippurath, G.; Gerhardt, G.A.; Gholmieh, G.; Granacki, J.J.; Hampson, R.; Hsaio, M.C.; et al. Restoring lost cognitive function. IEEE Eng. Med. Biol. Mag. 2005, 24, 30–44. [Google Scholar] [CrossRef]
- Ismail, F.Y.; Fatemi, A.; Johnston, M.V. Cerebral plasticity: Windows of opportunity in the developing brain. Eur. J. Paediatr. Neurol. 2017, 21, 23–48. [Google Scholar] [CrossRef]
- Jones, R.M.; Pattwell, S.S. Future considerations for pediatric cancer survivorship: Translational perspectives from developmental neuroscience. Dev. Cogn. Neurosci. 2019, 38, 100657. [Google Scholar] [CrossRef]
- Marusak, H.A.; Iadipaolo, A.S.; Harper, F.W.; Elrahal, F.; Taub, J.W.; Goldberg, E.; Rabinak, C.A. Neurodevelopmental consequences of pediatric cancer and its treatment: Applying an early adversity framework to understanding cognitive, behavioral, and emotional outcomes. Neuropsychol. Rev. 2018, 28, 123–175. [Google Scholar] [CrossRef] [PubMed]
- Walsh, K.S.; Noll, R.B.; Annett, R.D.; Patel, S.K.; Patenaude, A.F.; Embry, L. Standard of Care for Neuropsychological Monitoring in Pediatric Neuro-Oncology: Lessons From the Children’s Oncology Group (COG). Pediatr. Blood Cancer 2016, 63, 191–195. [Google Scholar] [CrossRef] [PubMed]
- Slykerman, R.F.; Jenner, E.; Tsui, K.; Laughton, S. Neuropsychological assessment of paediatric brain tumour survivors: Factors associated with assessment. J. Paediatr. Child. Health 2021, 57, 1612–1616. [Google Scholar] [CrossRef] [PubMed]
- Limond, J.; Thomas, S.; Bull, K.S.; Calaminus, G.; Lemiere, J.; Traunwieser, T.; van Santen, H.M.; Weiler, L.; Spoudeas, H.A.; Chevignard, M. Quality of survival assessment in European childhood brain tumour trials, for children below the age of 5 years. Eur. J. Paediatr. Neurol. 2020, 25, 59–67. [Google Scholar] [CrossRef]
- Limond, J.A.; Bull, K.S.; Calaminus, G.; Kennedy, C.R.; Spoudeas, H.A.; Chevignard, M.P.; Brain Tumour Quality of Survival Group, I.S.o.P.O. Quality of survival assessment in European childhood brain tumour trials, for children aged 5 years and over. Eur. J. Paediatr. Neurol. 2015, 19, 202–210. [Google Scholar] [CrossRef]
- Soderstrom, H.; Brocki, K.; Kleberg, J.L.; Martinsson, U.; Ljungman, G. Neurocognitive Functions Before and After Radiotherapy in Pediatric Brain Tumor Survivors. Pediatr. Neurol. 2022, 133, 21–29. [Google Scholar] [CrossRef]
- Children’s Oncology Group. Long-Term Follow-Up Guidelines for Survivors of Childhood, Adolescent, and Young Adult Cancers. Available online: http://survivorshipguidelines.org/ (accessed on 19 October 2022).
- Leiss, U. Neuropsychological assessment and intervention in pediatric neuro-oncology. memo—Mag. Eur. Med. Oncol. 2012, 4, 24–25. [Google Scholar] [CrossRef]
- Irestorm, E.; Perrin, S.; Tonning Olsson, I. Pretreatment Cognition in Patients Diagnosed With Pediatric Brain Tumors. Pediatr. Neurol. 2018, 79, 28–33. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cognitive Domain | Author, Year | Population | Main Findings |
|---|---|---|---|
| Global intellectual functioning | De Ruiter et al. [38] | Meta-analysis summarizing neurocognitive outcomes of 1082 pediatric brain tumor survivors | PBTS scored on average 0.54SD to 0.90SD lower on the WISC-III scales than the normative sample, with PIQ scores being even more depressed than VIQ scores |
| Brinkman et al. [17] | 224 adult survivors of CNS pediatric tumors | 20–30% of survivors demonstrated impairment on performance-based measures of intellect compared to expected 2% in the general population | |
| Lafay-Cousin et al. [39] | 16 Atypical teratoid/rhabdoid tumor survivors | Overall impaired neurocognitive outcome while treated with a radiation sparing approach | |
| Clark et al. [40] | 43 survivors of focal low-grade brainstem gliomas | Measures of intelligence quotient significantly lower than normative, despite focal disease and treatment targeting subcortical areas | |
| Moxon-Emre et al. [41] | 113 patients treated for medulloblastoma | Patients treated with reduced dose craniospinal irradiation plus tumor bed boost showed stable intellectual trajectories while those treated with higher doses and larger boost experienced decline. | |
| Roncadin et al. [42] | 29 astrocytoma and 29 medulloblastoma survivors | Greater perioperative and short-term medical adversity contributes to lower IQ in the long term | |
| Margelisch et al. [35] | 20 CNS tumor patients compared to 27 control patients (other type of cancer) at diagnosis | Mean IQs of patients with brain tumor lie within the normal range at diagnosis | |
| Executive functions | Law et al. [43] | 25 children treated for medulloblastoma with surgery, CRT and chemotherapy and 20 healthy controls | EFs deficits are found children treated for medulloblastoma compared to age-matched peers. Selective deficits in cognitive efficiency, problem-solving and working memory. Specific damage to cerebrocerebellar circuitry. |
| Heitzer et al. [44] | 32 patients treated for LGG with surgery only | Supratentorial LGG and history of seizures: greater impact on executive functioning | |
| Koustenis et al. [45] | 42 pediatric posterior fossa tumor survivors (mean age 14.63 years | Pediatric cerebellar tumor survivors show similar pattern of impairment in executive functions in particular in forward-thinking, mental flexibility and inhibition | |
| Memory | Margelisch et al. [35] | 25 children treated for medulloblastoma with surgery, CRT, and chemotherapy and 20 healthy controls | Memory and attention are the principal domain found to be impaired at diagnosis before treatment |
| Decker et al. [46] | 29 PBTS treated with chemotherapy and CRT | Associations between hippocampal subfield volumes and short-term verbal memory | |
| Attention | Margelisch et al. [35] | 25 children treated for medulloblastoma with surgery, CRT, and chemotherapy and 20 healthy controls | Memory and attention are the principal domain found to be impaired at diagnosis before treatment |
| Processing speed | Weusthof et al. [47] | 103 CNS pediatric patients treated with photon therapy, proton therapy or surgery alone | Processing speed is the most vulnerable domain with decline over time in both photon and surgery cohorts |
| King et al. [48] | 57 neurotypical controls and 57 survivors of childhood brain tumors | Processing speed appears to be the central cognitive skill that disrupts the other core cognitive skills of attention span and working memory, and all three make a unique contribution to IQ and academic achievement |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pancaldi, A.; Pugliese, M.; Migliozzi, C.; Blom, J.; Cellini, M.; Iughetti, L. Neuropsychological Outcomes of Children Treated for Brain Tumors. Children 2023, 10, 472. https://doi.org/10.3390/children10030472
Pancaldi A, Pugliese M, Migliozzi C, Blom J, Cellini M, Iughetti L. Neuropsychological Outcomes of Children Treated for Brain Tumors. Children. 2023; 10(3):472. https://doi.org/10.3390/children10030472
Chicago/Turabian StylePancaldi, Alessia, Marisa Pugliese, Camilla Migliozzi, Johanna Blom, Monica Cellini, and Lorenzo Iughetti. 2023. "Neuropsychological Outcomes of Children Treated for Brain Tumors" Children 10, no. 3: 472. https://doi.org/10.3390/children10030472
APA StylePancaldi, A., Pugliese, M., Migliozzi, C., Blom, J., Cellini, M., & Iughetti, L. (2023). Neuropsychological Outcomes of Children Treated for Brain Tumors. Children, 10(3), 472. https://doi.org/10.3390/children10030472