
Congenital Diaphragmatic Hernia: Perinatal Prognostic Factors and Short-Term Outcomes in a Single-Center Series

 , , ,
, , , 
Abstract
:1. Introduction
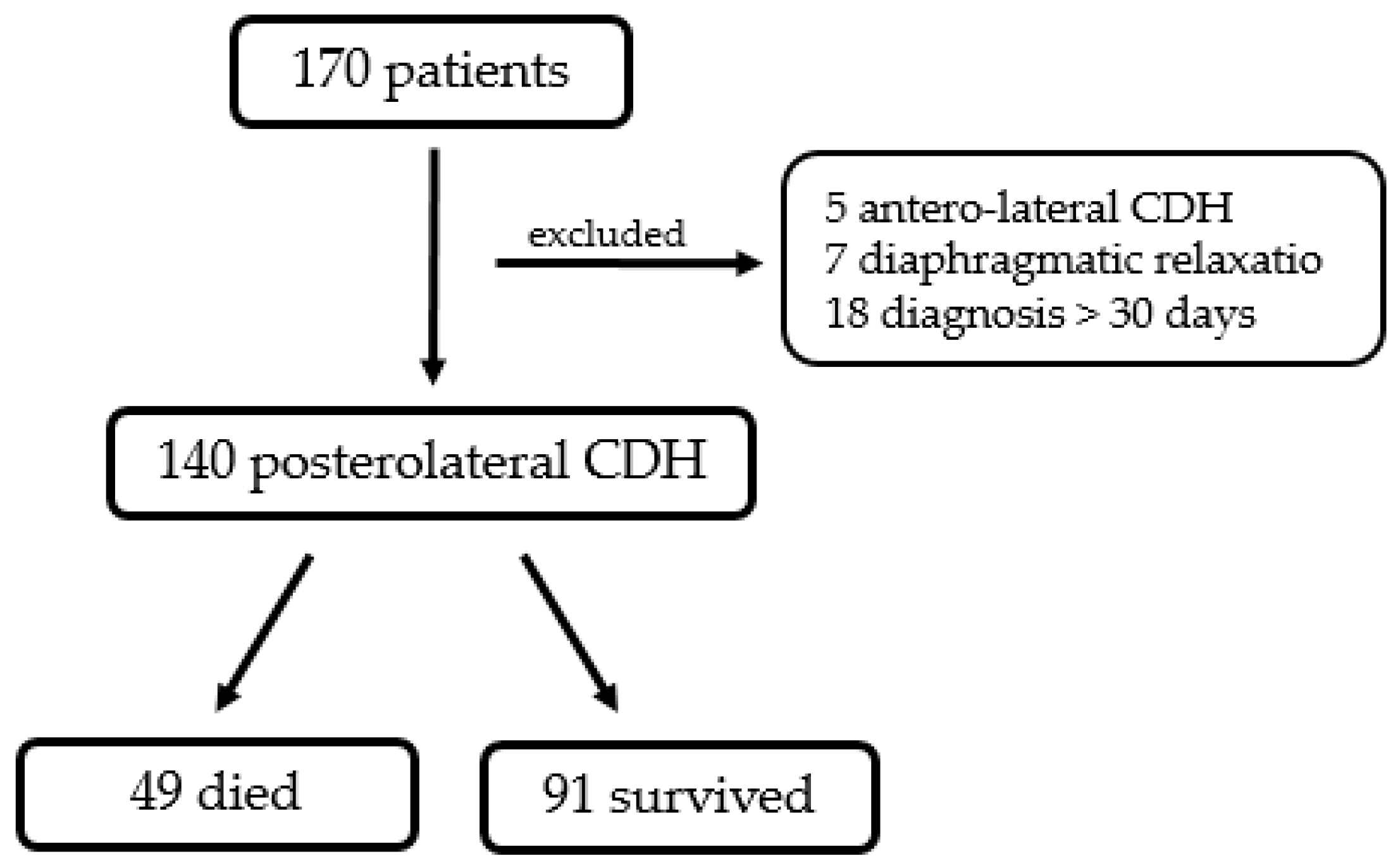
2. Materials and Methods
3. Results
3.1. Demographics
3.2. Intraoperatives
3.3. Postoperatives
3.4. Predictors of Outcomes
3.5. Multivariable Logistic Regression
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Leeuwen, L.; Fitzgerald, D.A. Congenital diaphragmatic hernia. J. Paediatr. Child Health 2014, 50, 667–673. [Google Scholar] [CrossRef] [PubMed]
- Wright, J.C.; Budd, J.L.; Field, D.J.; Draper, E.S. Epidemiology and outcome of congenital diaphragmatic hernia: A 9-year experience. Paediatr. Perinat. Epidemiol. 2011, 25, 144–149. [Google Scholar] [CrossRef] [PubMed]
- Kosiński, P.; Wielgoś, M. Congenital diaphragmatic hernia: Pathogenesis, prenatal diagnosis and management—Literature review. Ginekol. Pol. 2017, 88, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Snoek, K.G.; Reiss, I.K.; Greenough, A.; Capolupo, I.; Urlesberger, B.; Wessel, L.; Storme, L.; Deprest, J.; Schaible, T.; van Heijst, A.; et al. Standardized Postnatal Management of Infants with Congenital Diaphragmatic Hernia in Europe: The CDH EURO Consortium Consensus—2015 Update. Neonatology 2016, 110, 66–74. [Google Scholar] [CrossRef]
- Jancelewicz, T.; Brindle, M.E.; Guner, Y.S.; Lally, P.A.; Lally, K.P.; Harting, M.T.; Congenital Diaphragmatic Hernia Study Group (CDHSG); Pediatric Surgery Research Collaborative (PedSRC). Toward Standardized Management of Congenital Diaphragmatic Hernia: An Analysis of Practice Guidelines. J. Surg. Res. 2019, 243, 229–235. [Google Scholar] [CrossRef]
- Lusk, L.A.; Wai, K.C.; Moon-Grady, A.J.; Steurer, M.A.; Keller, R.L. Persistence of pulmonary hypertension by echocardiography predicts short-term outcomes in congenital diaphragmatic hernia. J. Pediatr. 2015, 166, 251–256.e1. [Google Scholar] [CrossRef]
- Zambaiti, E.; Bussani, R.; Calcaterra, V.; Zandonà, L.; Silvestri, F.; Peiró, J.L.; Marotta, M.; Andreatta, E.; Pelizzo, G. Myocardial effects of fetal endoscopic tracheal occlusion in lambs with CDH. Prenat. Diagn. 2016, 36, 362–367. [Google Scholar] [CrossRef]
- Stefanutti, G.; Filippone, M.; Tommasoni, N.; Midrio, P.; Zucchetta, P.; Moreolo, G.S.; Toffolutti, T.; Baraldi, E.; Gamba, P. Cardiopulmonary anatomy and function in long-term survivors of mild to moderate congenital diaphragmatic hernia. J. Pediatr. Surg. 2004, 39, 526–531. [Google Scholar] [CrossRef]
- Brindle, M.E.; Brar, M.; Skarsgard, E.D.; Canadian Pediatric Surgery Network (CAPSNet). Patch repair is an independent predictor of morbidity and mortality in congenital diaphragmatic hernia. Pediatr. Surg. Int. 2011, 27, 969–974. [Google Scholar] [CrossRef]
- Ruano, R.; Benachi, A.; Joubin, L.; Aubry, M.C.; Thalabard, J.C.; Dumez, Y.; Dommergues, M. Three-dimensional ultrasonographic assessment of fetal lung volume as prognostic factor in isolated congenital diaphragmatic hernia. BJOG 2004, 111, 423–429. [Google Scholar] [CrossRef]
- Mahieu-Caputo, D.; Sonigo, P.; Dommergues, M.; Fournet, J.C.; Thalabard, J.C.; Abarca, C.; Benachi, A.; Brunelle, F.; Dumez, Y. Fetal lung volume measurement by magnetic resonance imaging in congenital diaphragmatic hernia. BJOG 2001, 108, 863–868. [Google Scholar] [PubMed]
- Aggarwal, S.; Stockmann, P.; Klein, M.D.; Natarajan, G. Echocardiographic measures of ventricular function and pulmonary artery size: Prognostic markers of congenital diaphragmatic hernia? J. Perinatol. 2011, 31, 561–566. [Google Scholar] [CrossRef] [PubMed]
- Masumoto, K.; Teshiba, R.; Esumi, G.; Nagata, K.; Takahata, Y.; Hikino, S.; Hara, T.; Hojo, S.; Tsukimori, K.; Wake, N.; et al. Improvement in the outcome of patients with antenatally diagnosed congenital diaphragmatic hernia using gentle ventilation and circulatory stabilization. Pediatr. Surg. Int. 2009, 25, 487–492. [Google Scholar] [CrossRef] [PubMed]
- Kehl, S.; Eckert, S.; Berlit, S.; Tuschy, B.; Sütterlin, M.; Siemer, J. New formulas for calculating the lung-to-head ratio in healthy fetuses between 20 and 40 weeks’ gestation. J. Ultrasound Med. 2013, 32, 1939–1943. [Google Scholar] [CrossRef] [PubMed]
- Congenital Diaphragmatic Hernia Study Group. Estimating disease severity of congenital diaphragmatic hernia in the first 5 minutes of life. J. Pediatr. Surg. 2001, 36, 141–145. [Google Scholar] [CrossRef] [PubMed]
- American Academy of Pediatrics Committee on Fetus and Newborn; American College of Obstetricians and Gynecologists Committee on Obstetric Practice. The APGAR Score. Pediatrics 2015, 136, 819–822. [Google Scholar] [CrossRef] [PubMed]
- Morini, F.; Lally, P.A.; Lally, K.P.; Bagolan, P. The Congenital Diaphragmatic Hernia Study Group Registry. Eur. J. Pediatr. Surg. 2015, 25, 488–496. [Google Scholar] [CrossRef]
- Brownlee, E.M.; Howatson, A.G.; Davis, C.F.; Sabharwal, A.J. The hidden mortality of congenital diaphragmatic hernia: A 20-year review. J. Pediatr. Surg. 2009, 44, 317–320. [Google Scholar] [CrossRef]
- Aydın, E.; Nolan, H.; Peiró, J.L.; Burns, P.; Rymeski, B.; Lim, F.Y. When primary repair is not enough: A comparison of synthetic patch and muscle flap closure in congenital diaphragmatic hernia? Pediatr. Surg. Int. 2020, 36, 485–491. [Google Scholar] [CrossRef]
- Langwieler, T.; Fiegel, H.C.; Alaamian, M.; Mann, O.; Beshir, I.; Izbicki, J.R.; Kluth, D. The relationship of diaphragmatic defect, liver growth, and lung hypoplasia in nitrofen-induced congenital diaphragmatic hernia in the rat. Pediatr. Surg. Int. 2004, 20, 509–514. [Google Scholar] [CrossRef]
- Midrio, P.; Gobbi, D.; Baldo, V.; Gamba, P. Right congenital diaphragmatic hernia: An 18-year experience. J. Pediatr. Surg. 2007, 42, 517–521. [Google Scholar] [CrossRef]
- Panda, S.S.; Bajpai, M.; Srinivas, M. Presence of hernia sac in prediction of postoperative outcome in congenital diaphragmatic hernia. Indian Pediatr. 2013, 50, 1041–1043. [Google Scholar] [CrossRef] [PubMed]
- Oliver, E.R.; De Bari, S.E.; Adams, S.E.; Didier, R.A.; Horii, S.C.; Victoria, T.; Hedrick, H.L.; Adzick, N.S.; Howell, L.J.; Moldenhauer, J.S.; et al. Congenital diaphragmatic hernia sacs: Prenatal imaging and associated postnatal outcomes. Pediatr. Radiol. 2019, 49, 593–599. [Google Scholar] [CrossRef] [PubMed]
- Bouchghoul, H.; Marty, O.; Fouquet, V.; Cordier, A.G.; Senat, M.V.; Saada, J.; Mokhtari, M.; Le Saché, N.; Martinovic, J.; Benachi, A. Congenital diaphragmatic hernia has a better prognosis when associated with a hernia sac. Prenat. Diagn. 2018, 38, 638–644. [Google Scholar] [CrossRef] [PubMed]
- Losty, P.D. Congenital diaphragmatic hernia: Where and what is the evidence? Semin. Pediatr. Surg. 2014, 23, 278–282. [Google Scholar] [CrossRef]
- Gupta, V.S.; Harting, M.T. Congenital diaphragmatic hernia-associated pulmonary hypertension. Semin. Perinatol. 2020, 44, 151167. [Google Scholar] [CrossRef] [PubMed]
- Dao, D.T.; Patel, N.; Harting, M.T.; Lally, K.P.; Lally, P.A.; Buchmiller, T.L. Early Left Ventricular Dysfunction and Severe Pulmonary Hypertension Predict Adverse Outcomes in “Low-Risk” Congenital Diaphragmatic Hernia. Pediatr. Crit. Care Med. 2020, 21, 637–646. [Google Scholar] [CrossRef]
- Tiryaki, S.; Ozcan, C.; Erdener, A. Initial oxygenation response to inhaled nitric oxide predicts improved outcome in congenital diaphragmatic hernia. Drugs R&D 2014, 14, 215–219. [Google Scholar]
- Marinosci, G.Z.; De Robertis, E.; De Benedictis, G.; Piazza, O. Dopamine Use in Intensive Care: Are We Ready to Turn it Down? Transl. Med. UniSa 2012, 4, 90–94. [Google Scholar]
- Joynt, C.; Cheung, P.Y. Treating Hypotension in Preterm Neonates With Vasoactive Medications. Front. Pediatr. 2018, 6, 86. [Google Scholar] [CrossRef]
- Lakshminrusimha, S.; Keszler, M.; Kirpalani, H.; Van Meurs, K.; Chess, P.; Ambalavanan, N.; Yoder, B.; Fraga, M.V.; Hedrick, H.; Lally, K.P.; et al. Milrinone in congenital diaphragmatic hernia—A randomized pilot trial: Study protocol, review of literature and survey of current practices. Matern. Health Neonatol. Perinatol. 2017, 3, 27. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Pulmonary Hypertension | Definition |
|---|---|
| Low Pulmonary Hypertension | Tricuspid insufficiency, right-to-left shunt through patent arteriosus duct |
| Mild Pulmonary Hypertension | Tricuspid insufficiency, right-to-left shunt through patent arteriosus duct, right-to-left shunt through patent foramen ovale. NO < 20 ppm |
| Severe Pulmonary Hypertension | Tricuspid insufficiency, right-to-left shunt through patent arteriosus duct, right-to-left shunt through patent foramen ovale. NO > 20 ppm, sildenafil. |
| Overall (140) | Dead (49) | Survivor (91) | p Value | |
|---|---|---|---|---|
| Prenatal Diagnosis, n (%) | 90 (64.2%) | 42 (85.7%) | 48 (52.7%) | <0.001 * |
| O/E LHR, %, median (IQR) | 33 (27–47) | 30 (25–34) | 44 (30–49.5) | 0.018 # |
| Associated Anomalies, n (%) | 33 (23.5%) | 21 (42.8%) | 12 (13.1%) | <0.001 * |
| GA at Birth, weeks, median (IQR) | 38 (36.5–39) | 37 (35.5–39) | 38 (37–39) | 0.002 # |
| Weight, grams, median (IQR) | 2900 (2428–3265) | 2620 (2135–3105) | 3000 (2655–3358) | 0.023 # |
| Male, n (%) | 85 (60.7%) | 30 (61.2%) | 55 (60%) | 0.927 * |
| POS, %, median (IQR) | 75 (51–85) | 57 (34–73.25) | 80 (68.25–86) | <0.001 # |
| ECMO, n (%) | 8 (5.7%) | 6 (12.2%) | 2 (2.1%) | 0.22 ° |
| Overall (140) | Dead (49) | Survivor (91) | p Value | |
|---|---|---|---|---|
| Side | 0.095 ° | |||
| Left, n (%) | 117 (83.6%) | 38 (77.6%) | 79 (86.8%) | |
| Right, n (%) | 21 (15%) | 9 (18.3%) | 12 (13.2%) | |
| Bilateral, n (%) | 2 (1.4%) | 2 (4.1%) | 0 (0%) | |
| Hernia Sac, n (%) | 18 (12.8%) | 3 (6.1%) | 15 (16.4%) | 0.08 * |
| Size | <0.001 * | |||
| A, n (%) | 17 (12.1%) | 2 (4.1%) | 15 (16.5%) | |
| B, n (%) | 42 (30%) | 4 (8.2%) | 38 (41.7%) | |
| C, n (%) | 52 (37.2%) | 24 (48.9%) | 28 (30.8%) | |
| D, n (%) | 29 (20.7%) | 19 (38.8%) | 10 (11%) | |
| Liver-up, n (%) | 64 (45.7%) | 34 (69.3%) | 30 (32.9%) | <0.001 * |
| Spleen-up, n (%) | 86 (61.4%) | 29 (59.1%) | 57 (62.6%) | 0.97 * |
| Patch, n (%) | 40 (37.7%) | 11 (73.3%) | 29 (31.8%) | 0.002 * |
| Overall (140) | Death (49) | Survival (91) | p Value | |
|---|---|---|---|---|
| PH | <0.001 ° | |||
| None, n (%) | 64 (45.7%) | 1 (2%) | 63 (69.2%) | |
| Mild, n (%) | 10 (7.1%) | 0 (0%) | 10 (11%) | |
| Moderate, n (%) | 21 (15%) | 14 (28.6%) | 7 (7.7%) | |
| Severe, n (%) | 44 (31.4%) | 34 (69.4%) | 10 (11%) | |
| Unknown, n (%) | 1 (0.8%) | 0 (0%) | 1 (1.1%) | |
| iNO2, n (%) | 62 (44.2%) | 46 (93.8%) | 16 (10.9%) | <0.001 * |
| Sildenafil, n (%) | 14 (10%) | 11 (22.4%) | 3 (3.2%) | <0.001 ° |
| Inotropes, n (%) | 110 (78.5%) | 46 (93.8%) | 64 (70.3%) | 0.002 * |
| Dopamine, γ/kg/min, median (IQR) | 10 (1–14) | 14 (10–14.5) | 7 (0–10) | <0.001 # |
| Overall (91) | >3 Weeks (54) | ≤3 Weeks (37) | p Value | |
|---|---|---|---|---|
| Prenatal Diagnosis, n (%) | 48 (52.7%) | 33 (61.1%) | 15 (40.5%) | 0.53 * |
| O/E LHR, %, median (IQR) | 26 (10–45) | 45 (30–49.5) | 34.5 (27–58.5) | 0.67 # |
| Associated Anomalies, n (%) | 12 (13.1%) | 10 (18.5%) | 2 (5.4%) | 0.11 ° |
| GA at Birth, weeks, median (IQR) | 38 (36–39) | 38 (37–39) | 38 (37–39) | 0.25 # |
| Weight, grams, median (IQR) | 3000 (2620–3470) | 2980 (2520–3270) | 3100 (2885–3400) | 0.23 # |
| Male, n (%) | 55 (60%) | 32 (59.2%) | 23 (62.1%) | 0.78 * |
| POS, %, median (IQR) | 80 (66–89) | 74 (59–84) | 85 (78–90) | 0.12 # |
| ECMO, n (%) | 2 (2.1%) | 2 (3.7%) | 0 (0%) | 0.51 ° |
| Overall (91) | >3 Weeks (54) | ≤3 Weeks (37) | p Value | |
|---|---|---|---|---|
| Side | 0.18 * | |||
| Left, n (%) | 79 (86.8%) | 49 (90.7%) | 30 (81%) | |
| Right, n (%) | 12 (13.2%) | 5 (9.3%) | 7 (19%) | |
| Hernia Sac, n (%) | 15 (16.4%) | 7 (12.9%) | 8 (21.6%) | 0.27 * |
| Size | <0.001 * | |||
| A, n (%) | 15 (16.5%) | 6 (11.1%) | 9 (24.3%) | |
| B, n (%) | 38 (41.7%) | 16 (29.6%) | 22 (59.5%) | |
| C, n (%) | 28 (30.8%) | 23 (42.6%) | 5 (13.5%) | |
| D, n (%) | 10 (11%) | 9 (16.7%) | 1 (2.7%) | |
| Liver-up, n (%) | 30 (32.9%) | 19 (35.1%) | 11 (29.7%) | 0.59 * |
| Spleen-up, n (%) | 57 (62.6%) | 39 (72.2%) | 18 (48.6%) | 0.15 * |
| Patch, n (%) | 29 (31.8%) | 27 (50%) | 2 (5.4%) | <0.001 * |
| Time for Surgery, minutes, median (IQR) | 102 (75–130) | 120 (101–160) | 95 (81–120) | 0.001 # |
| Overall (91) | >3 Weeks (54) | ≤3 Weeks (37) | p Value | |
|---|---|---|---|---|
| PH | 0.004 ° | |||
| None, n (%) | 63 (69.2%) | 32 (59.3%) | 31 (83.7%) | |
| Mild, n (%) | 10 (11%) | 7 (12.9%) | 3 (8.2%) | |
| Moderate, n (%) | 7 (7.7%) | 6 (11.1%) | 1 (2.7%) | |
| Severe, n (%) | 10 (11%) | 9 (16.7%) | 1 (2.7%) | |
| Unknown, n (%) | 1 (1.1%) | 0 (0%) | 1 (2.7%) | |
| iNO2, n (%) | 16 (10.9%) | 15 (27.7%) | 1 (2.7%) | 0.002 * |
| Sildenafil, n (%) | 3 (3.2%) | 3 (5.5%) | 0 (0%) | 0.268 ° |
| Inotropes, n (%) | 64 (70.3%) | 45 (83.3%) | 19 (51.3%) | 0.002 * |
| Dopamine, γ/kg/min, median (IQR) | 8 (0–10) | 10 (5–12) | 6 (0–10) | <0.001 # |
| O2 at 30 days, n (%) | 7 (7.6%) | 7 (12.9%) | 0 (0%) | 0.04 ° |
| Mechanical Ventilation, days, median (IQR) | 9 (6–14) | 12 (7–20) | 6 (5–8) | <0.001 # |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pagliara, C.; Zambaiti, E.; Brooks, G.; Bonadies, L.; Tognon, C.; Salvadori, S.; Sgrò, A.; Leon, F.F. Congenital Diaphragmatic Hernia: Perinatal Prognostic Factors and Short-Term Outcomes in a Single-Center Series. Children 2023, 10, 315. https://doi.org/10.3390/children10020315
Pagliara C, Zambaiti E, Brooks G, Bonadies L, Tognon C, Salvadori S, Sgrò A, Leon FF. Congenital Diaphragmatic Hernia: Perinatal Prognostic Factors and Short-Term Outcomes in a Single-Center Series. Children. 2023; 10(2):315. https://doi.org/10.3390/children10020315
Chicago/Turabian StylePagliara, Camilla, Elisa Zambaiti, Giulia Brooks, Luca Bonadies, Costanza Tognon, Sabrina Salvadori, Alberto Sgrò, and Francesco Fascetti Leon. 2023. "Congenital Diaphragmatic Hernia: Perinatal Prognostic Factors and Short-Term Outcomes in a Single-Center Series" Children 10, no. 2: 315. https://doi.org/10.3390/children10020315
APA StylePagliara, C., Zambaiti, E., Brooks, G., Bonadies, L., Tognon, C., Salvadori, S., Sgrò, A., & Leon, F. F. (2023). Congenital Diaphragmatic Hernia: Perinatal Prognostic Factors and Short-Term Outcomes in a Single-Center Series. Children, 10(2), 315. https://doi.org/10.3390/children10020315