
Developmental Trajectory of Depressive Symptoms from Early Childhood through High School in Children and Adolescents with a High Intellectual Potential


Abstract
:1. Introduction
2. Material and Methods
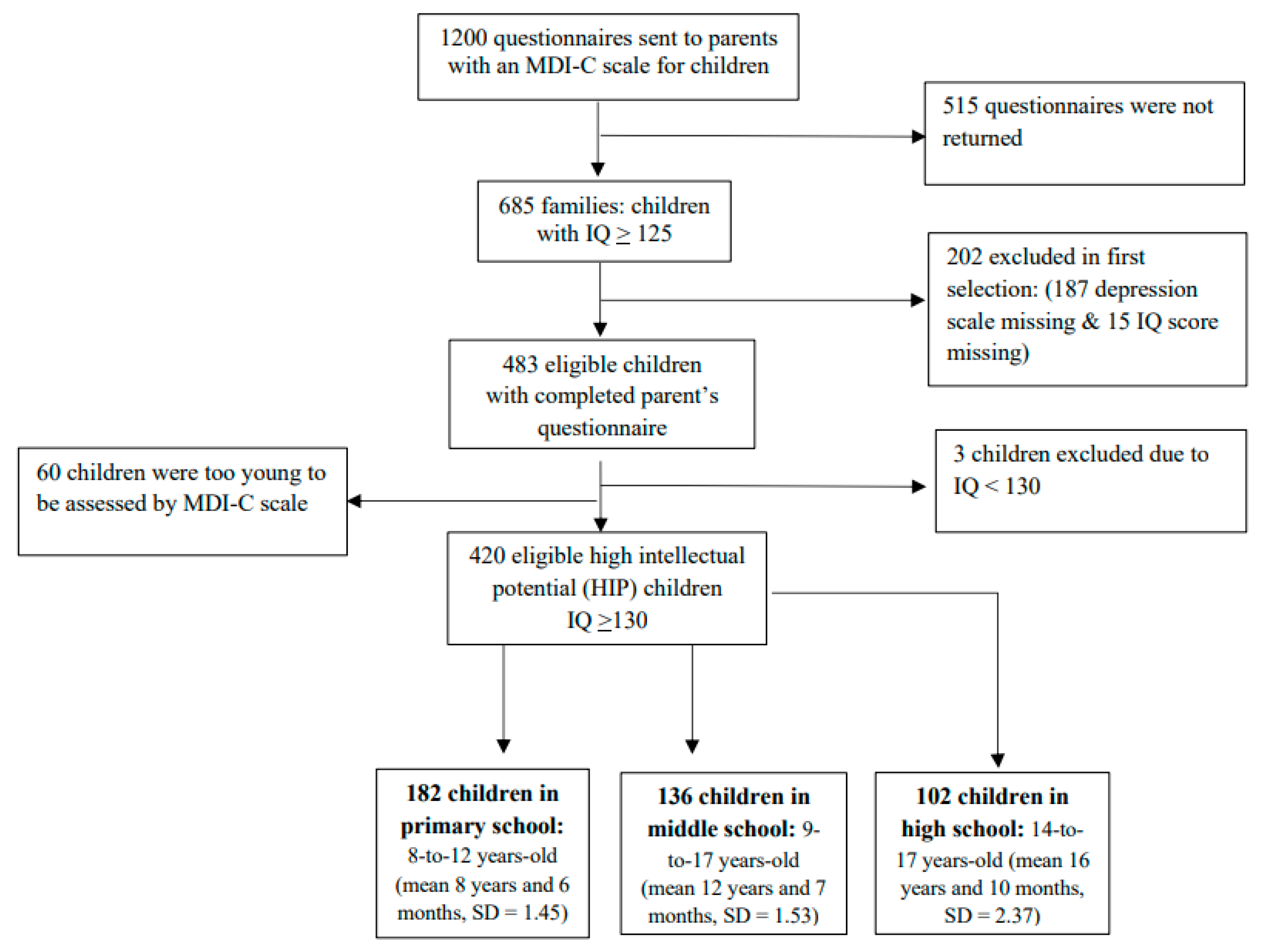
2.1. Participants
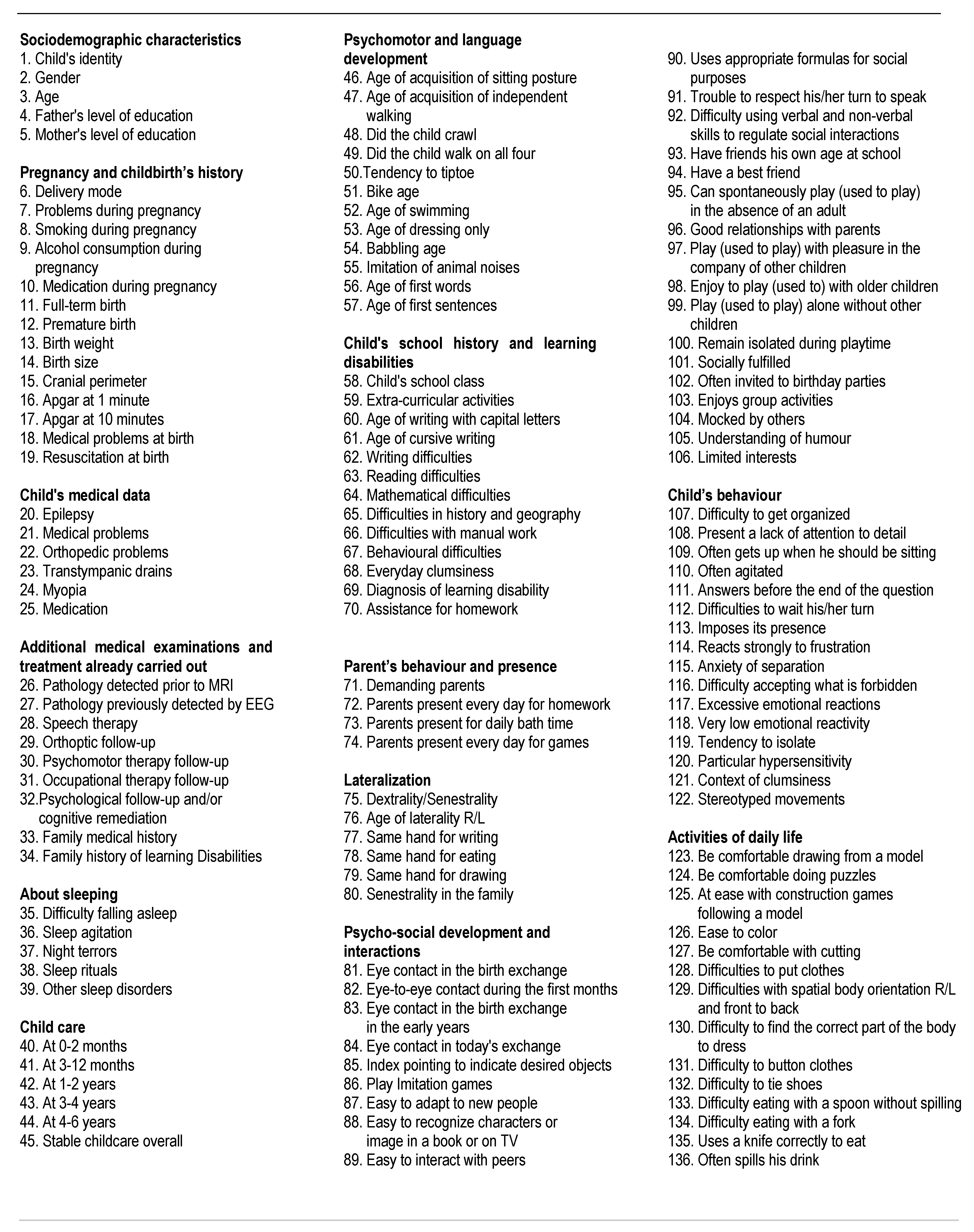
2.2. Design and Measures
2.3. Statistical Analysis Procedure
3. Results
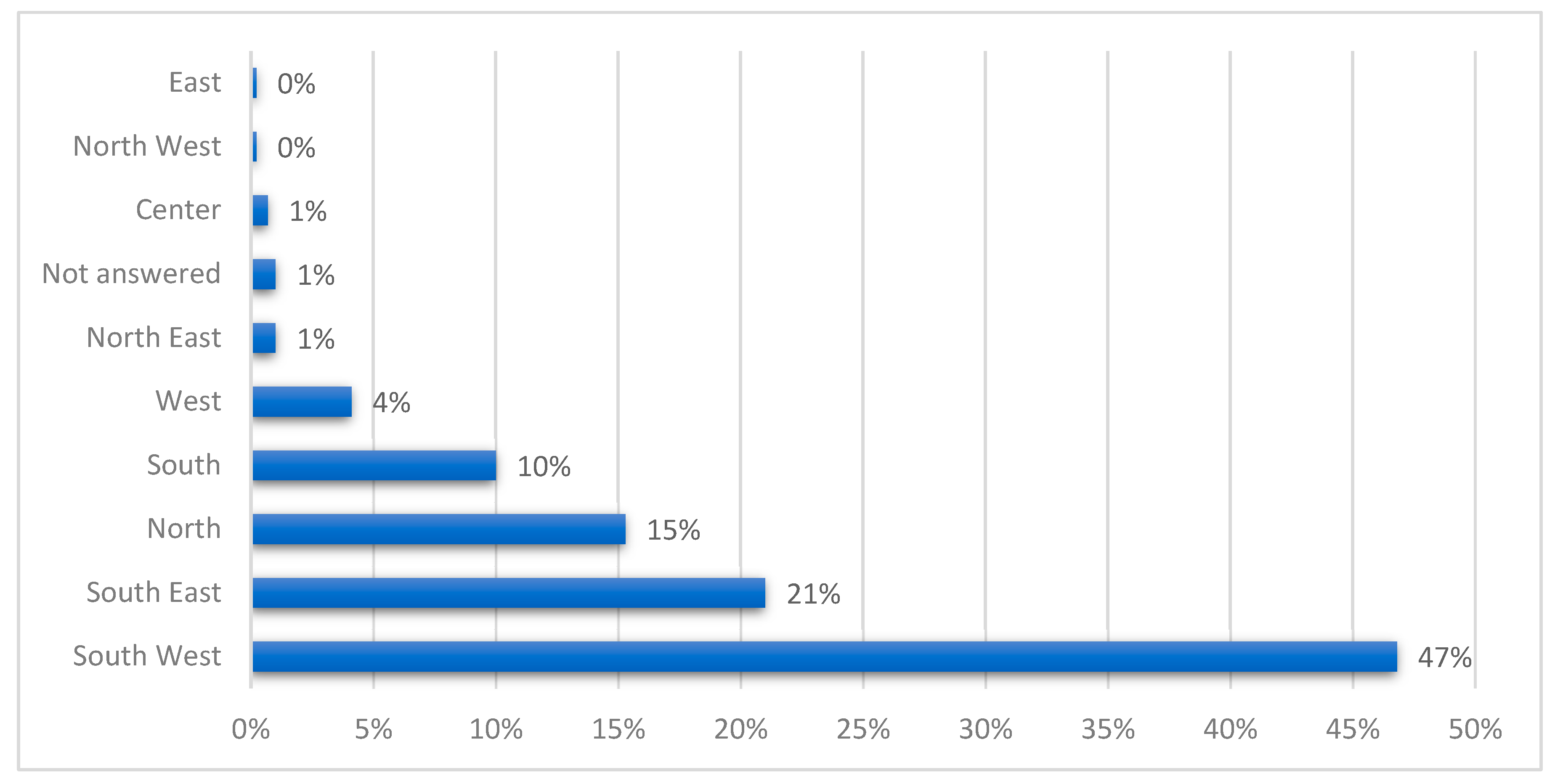
3.1. Sample Characteristics: Socio-Demographic and Clinical Data
3.2. Developmental Trajectory of Depressive Symptoms from Early Childhood through High School in HIP Children: Relationship between IQ and Depressive Symptoms and Role of Anamnestic Features
3.3. Difference between Primary, Middle and High School Groups of HIP Children Regarding MDI-C Subtest Scale
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- APA. Diagnostic and Statistical Manual of Mental Disorders, DSM-5, 5th ed.; American Psychiatric Publishing: Washington, DC, USA, 2013. [Google Scholar]
- World Health Organization. Depression and Other Common Mental Disorders: Global Health Estimates; World Health Organization: Geneva, Switzerland, 2017. Available online: https://apps.who.int/iris/bitstream/handle/10665/254610/WHO-MSD-MER-2017.2-eng.pdf (accessed on 10 June 2023).
- Haute Autorité de Santé (HAS). Recommandation de Bonne Pratique. Manifestations Dépressives à L’adolescence: Repérage, Diagnostic et Prise en Charge en Soins de Premier Recours; HAS: Paris, France, 2014; Available online: https://www.has-sante.fr/upload/docs/application/pdf/2014-12/manifestations_depressives_recommandations.pdf (accessed on 10 June 2023).
- Santomauro, D.F. COVID-19. Mental Disorders Collaborators. Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. Lancet 2021, 398, 1700–1712. [Google Scholar] [CrossRef] [PubMed]
- Pfeiffer, S.I.; Stocking, V.B. Vulnerabilities of academically gifted students. Spec. Serv. Sch. 2000, 16, 83–93. [Google Scholar] [CrossRef]
- Vaivre-Douret, L. Le développement de l’enfant aux “aptitude hautement performantes” (surdoués): Importance des fonctions neuro-psychomotrices. ANAE 2002, 67, 95–110. [Google Scholar]
- Vaivre-Douret, L. Les caractéristiques développementales d’un échantillon d’enfants tout venant “à hautes potentialités” (surdoués): Suivi prophylactique. Neuropsychiatr. Enfance Adolesc. 2004, 52, 129–141. [Google Scholar] [CrossRef]
- Alsop, G. Asynchrony: Intuitively valid and theoretically reliable. Roeper Rev. 2003, 25, 118. [Google Scholar] [CrossRef]
- Gagné, F. Talent development as seen through the differentiated model of giftedness and talent. In The Routledge International Companion to Gifted Education; Balchin, T., Hymer, B., Matthews, D.J., Balchin, T., Hymer, B., Matthews, D.J., Eds.; Routledge/Taylor & Francis Group: New York, NY, USA, 2009; pp. 32–41. [Google Scholar]
- Bénony, H.; van der Elst, D.; Chahraoui, K.; Bénony, C.; Marnier, J.P. Lien entre dépression et estime de soi scolaire chez les enfants intellectuellement précoces. L’Encéphale 2007, 33, 11–20. [Google Scholar] [CrossRef]
- Bailey, C.L. An examination of the relationships between ego development, Dabrowski’s theory of positive disintegration, and the behavioral characteristics of gifted adolescents. Gift. Child Quart. 2011, 55, 208–222. [Google Scholar] [CrossRef]
- Mueller, C.E.; Winsor, D.L. Depression, Suicide, and Giftedness: Disentangling Risk Factors, Protective Factors, and Implications for Optimal Growth. In Handbook of Giftedness in Children; Pfeiffer, S., Ed.; Springer Nature: Cham, Switzerland, 2018; pp. 255–284. [Google Scholar]
- Neihart, M. High intellectual potential children and depression. In The Social and Emotional Development of High Intellectual Potential Children: What Do We Know? Neihart, M., Reis, S., Robinson, N., Moon, S., Eds.; Prufrock Press: Waco, TX, USA, 2002; pp. 93–102. [Google Scholar]
- Mueller, C.E. Protective factors as barriers to depression in gifted and nongifted adolescents. Gift. Child Quart. 2009, 53, 3–14. [Google Scholar] [CrossRef]
- Jackson, P.S.; Peterson, J. Depressive disorder highly gifted adolescents. J. Second Gift. Educ. 2003, 14, 175–186. [Google Scholar] [CrossRef]
- Martin, L.T.; Burns, R.M.; Schonlau, M. Mental Disorders Among Gifted and Nongifted Youth: A Selected Review of the Epidemiologic Literature. Gift. Child Quart. 2010, 54, 31–41. [Google Scholar] [CrossRef]
- Cook, F.; Hippmann, D.; Omerovic, E. The sleep and mental health of gifted children: A prospective, longitudinal, community cohort study. Gift. Talent. Int. 2020, 135, 16–26. [Google Scholar] [CrossRef]
- Kermarrec, S.; Attinger, L.; Guignard, J.H.; Tordjman, S. Anxiety disorders in children with high intellectual potential. Neuropsychiatry 2018, 8, 739–744. [Google Scholar] [CrossRef]
- Roome, J.R.; Romney, D.M. Reducing anxiety in high intellectual potential children by inducing relaxation. Roeper Rev. 1985, 7, 177–179. [Google Scholar] [CrossRef]
- Guénolé, F.; Louis, J.; Creveuil, C.; Montlahuc, C.; Baleyte, J.M.; Fourneret, P.; Revol, O. Étude transversale de l’anxiété-trait dans un groupe de 111 enfants intellectuellement surdoués. L’Encéphale 2013, 39, 278–283. [Google Scholar] [CrossRef] [PubMed]
- Vaivre-Douret, L. Caractéristiques développementales de l’enfant à “hautes potentialités” et compréhension de trajectoires vers la dépression à l’âge scolaire en primaire et au collège. Neuropsychiatr. Enfance Adolesc. 2019, 67, 140–151. [Google Scholar] [CrossRef]
- Riedl-Cross, J.; Cross, T. Clinical and mental health issues in the counseling the gifted individual. J. Couns. Dev. 2015, 93, 163–172. [Google Scholar] [CrossRef]
- Hamdioui, S.; Vaivre-Douret, L. Clinical markers of dysgraphia according to intellectual quotient in children with Developmental Coordination Disorder. J. Psychiatry Psychiatr. Disord. 2020, 4, 366–382. [Google Scholar] [CrossRef]
- Hahn, L.; Eickhoff, S.B.; Habel, U.; Stickeler, E.; Schnakenberg, P.; Goecke, T.W.; Stickel, S.; Franz, M.; Dukart, J.; Chechko, N. Early identification of postpartum depression using demographic, clinical, and digital phenotyping. Transl. Psychiatry 2021, 11, 121. [Google Scholar] [CrossRef]
- Tordjman, S.; Kermarrec, S. Mythes et réalités sur les enfants à haut potentiel intellectuel en difficulté: Les apports de la recherche. Neuropsychiatr. Enfance Adolesc. 2019, 67, 130–139. [Google Scholar] [CrossRef]
- Guignard, J.H.; Kermarrec, S.; Tordjman, S. Relationships between intelligence and creativity in gifted and non-gifted children. Learn. Individ. Differ. 2016, 52, 209–215. [Google Scholar] [CrossRef]
- Vaivre-Douret, L.; Hamdioui, S.; Cannafarina, A. Some gifted children are diagnosed with developmental coordination disorder (DCD) but have they identical clinical features compared to typical children with DCD? Eur. Psychiatry 2020, 63, S676. [Google Scholar]
- Tordjman, S. Gifted children in difficulty: From attention deficit hyperactivity disorder to depression and school failure. Rev. Med. Suisse 2006, 2, 533–537. [Google Scholar]
- Simoes-Loureiro, I.; Lowenthal, L.; Lefebvre, L.; Vaivre-Douret, L. Le trouble déficitaire de l’attention chez l’enfant à haut potentiel: Étude exploratoire. ANAE 2009, 101, 317–322. [Google Scholar]
- Cordeiro, M.L.; Farias, A.C.; Cunha, A.; Benko, C.R.; Farias, L.G.; Costa, M.T.; Martins, L.F.; McCracken, J.T. Co-occurrence of ADHD and high IQ: A case series empirical study. J. Atten. Disord. 2011, 15, 485–490. [Google Scholar] [CrossRef] [PubMed]
- Van Viersen, S.; de Bree, E.H.; Kroesbergen, E.H.; Slot, E.M.; de Jong, P.F. Risk and protective factors in gifted children with dyslexia. Ann. Dyslexia 2015, 65, 178–198. [Google Scholar] [CrossRef] [PubMed]
- Tordjman, S.; Vaivre-Douret, L.; Chokron, S.; Kermarrec, S. Les enfants à haut potentiel intellectuel en difficulté: Apports de la recherche clinique. L’Encéphale 2018, 44, 445–456. [Google Scholar] [CrossRef] [PubMed]
- Vaivre-Douret, L.; Planche, P. Homogeneous or heterogenous I.Q. profile; Some clinical Characteristics to Differentiate high intellectual potential and Asperger’s syndrom in children. J. Psychiatry Psychiatr. Disord. 2020, 4, 191–217. [Google Scholar] [CrossRef]
- Bernd, D.; Kaiser, C.F. Echelle Composite de Dépression Pour Enfants: MDI-C; ECPA-Pearson: Paris, France, 1999. [Google Scholar]
- Hamdioui, S.; Cannafarina, A.; Vaivre-Douret, L. Do children with high intellectual potential have an early motor development and what is the impact on IQ profile? J. Pediatr. Perinatol. Child Health 2021, 5, 52–71. [Google Scholar] [CrossRef]
- Peyre, H.; Ramus, F.; Melchior, M.; Forhan, A.; Heude, B.; Gauvrit, N. Emotional, behavioral and social difficulties among high-IQ children during the preschool period: Results of the EDEN mother-child cohort. Pers. Individ. Differ. 2016, 94, 366–371. [Google Scholar] [CrossRef]
- Bildiren, A. Developmental characteristics of gifted children aged 0–6 years: Parental observations. Early Child Dev. Care 2017, 188, 997–1011. [Google Scholar] [CrossRef]
- Kitano, M.K.; Lewis, R.B. Resilience and coping: Implications for gifted children and youth at risk. Roeper Rev. 2005, 27, 200–205. [Google Scholar] [CrossRef]
- World Health Organization. International Statistical Classification of Diseases and Related Health Problems; 10th Revision (ICD-10); Diagnostic Criteria for Research; World Health Organization: Geneva, Switzerland, 1993.
- INSEE. ACT4 V2—Population active de 15 ans ou plus ayant un emploi par sexe, catégorie socioprofessionnelle et secteur d’activité économique en 2016. In Caractéristiques de L’emploi en 2016; INSEE: Paris, France, 2019. Available online: https://www.insee.fr/fr/statistiques/4177119?sommaire=4177250&geo=FE-1 (accessed on 10 June 2023).
- Baker, J.A. Depression and suicidal ideation among academically talented adolescents high intellectual potential. Gift. Child Quart. 1995, 39, 218–223. [Google Scholar] [CrossRef]
- Cross, T.L.; Cross, J.R. Suicide among students with gifts and talents. In APA Handbook of Giftedness and Talent; Pfeiffer, S.I., Shaunessy-Dedrick, E., Foley-Nicpon, M., Eds.; American Psychological Association: Washington, DC, USA, 2018; pp. 601–614. [Google Scholar] [CrossRef]
- Beckmann, E.; Minnaert, A. Non-cognitive characteristics of gifted students with learning disabilities: An In-depth systematic review. Front. Psychol. 2018, 9, 504. [Google Scholar] [CrossRef]
- Vaivre-Douret, L.; Lalanne, C.; Charlemaine, C.; Cabrol, D.; Keita, G.; Sebbane, O.; Golse, B.; Falissard, B. Relationship between growth status at birth and motor and cognitive development in a French sample of gifted children. Eur. Rev. Appl. Psychol. 2010, 60, 1–9. [Google Scholar] [CrossRef]
- Bowlby, J. Attachment and Loss: Attachment; Basic Books: New York, NY, USA, 1969. [Google Scholar]
- Speranza, M.; Debbané, M. Attachement, mentalisation et conséquences des contextes d’adversité. Bull. Acad. Natl. Méd. 2021, 205, 912–920. [Google Scholar] [CrossRef]
- Karpinski, R.I.; Kinase Kolb, A.M.; Tetreault, N.A.; Borowski, T.B. High intelligence: A risk factor for psychological and physiological overexcitabilities. Intelligence 2018, 66, 8–23. [Google Scholar] [CrossRef]
- Cummings, E.M.; Cicchetti, D. Toward a transactional model of relations between attachment and depression. In Attachment in the Preschool Years: Theory, Research, and Intervention; Greenberg, M.T., Cicchetti, D., Cummings, E.M., Eds.; MacArthur Foundation Series on Mental Health and Development; University of Chicago Press: Chicago, IL, USA, 1990; pp. 339–372. [Google Scholar]
- Jacobson, K.C.; Rowe, D.C. Genetic and environmental influences on the relationships between family connectedness, school connectedness, and adolescent depressed mood: Sex differences. Dev. Psychol. 1999, 35, 926–939. [Google Scholar] [CrossRef] [PubMed]
- Joiner, T.; Coyne, J.C. The Interactional Nature of Depression; American Psychological Association: Washington, DC, USA, 1999. [Google Scholar]
- Guénolé, F.; Speranza, M.; Louis, J.; Fourneret, P.; Revol, O.; Baleyte, J.M. Wechsler profiles in referred children with intellectual giftedness: Associations with trait-anxiety, emotional dysregulation, and heterogeneity of Piaget-like reasoning processes. Eur. J. Paediatr. Neurol. 2015, 19, 402–410. [Google Scholar] [CrossRef]
- Boschi, A.; Planche, P.; Henimou, C.; Demily, C.; Vaivre-Douret, L. From high Intellectual Potential to Asperger Syndrome: Evidence for a fundamental overlap—A systematic review. Front. Psychol. Cogn. Sci. 2016, 7, 1605. [Google Scholar] [CrossRef] [PubMed]
- Achenbach, T.M. Manual for Child Behavior Checklist/4–18 and 1991 Profile; University of Vermont Department of Psychiatry: Burlington, NJ, USA, 1991. [Google Scholar]
- Garland, A.F.; Zigler, E. Emotional and behavioral problems among highly intellectually gifted youth. Roeper Rev. J. Gift. Educ. 1999, 22, 41–44. [Google Scholar] [CrossRef]
- Neihart, M. The impact of giftedness on psychological well-being: What does the empirical literature say? Roeper Rev. J. Gift. Educ. 1999, 22, 10–17. [Google Scholar] [CrossRef]
- Versteynen, L. Issues in the social and emotional adjustment of gifted children: What does the literature say? New Zealand J. Gift. Educ. 2001, 13, 4. Available online: https://www.giftedchildren.org.nz/apex/v13art04.php (accessed on 15 June 2023).
- Papadopoulos, D. Parenting the exceptional social-emotional needs of gifted and talented Children: What DoWe Know? Children 2021, 8, 953. [Google Scholar] [CrossRef] [PubMed]
- Bozoglan, B.A. Systemic intervention model for the parents of gifted children. Curr. Psychol. 2023, 42, 4821–4829. [Google Scholar] [CrossRef]
- Renati, R.; Bonfiglio, N.S.; Dilda, M.; Mascia, M.L.; Penna, M.P. Gifted Children through the Eyes of Their Parents: Talents, Social-Emotional Challenges, and Educational Strategies from Preschool through Middle School. Children 2023, 10, 42. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sociodemographic and Clinical Data N = 420 | |||||
|---|---|---|---|---|---|
| Depressive Symptoms N = 205 (%) | Non-Depressive Symptoms N =215 (%) | χ2 or T-Score | Df | p-Value (95% CI) | |
| Age (months): mean (SD) | 140 (3.3) | 126 (3.19) | −2.99 | 419 | 0.3 (−1.13 to −5.04) |
| IQ mean (SD) | 138.76 (6.21) | 138.65 (5.53) | −0.08 | 419 | 0.94 (−0.03 to 2.08) |
| Gender | |||||
| Male | 156 (76.1%) | 174 (74.68%) | 0.98 | 419 | 0.35 (0.58 to 2.21) |
| Female | 49 (23.9%) | 41 (19.07%) | 0.93 | 0.39 (0.17 to 2.12) | |
| Weight at born (kg): mean (SD) | 3.33 (0.47) | 3.33 (0.51) | 0.18 | 419 | 0.86 (0.13 to 2.17) |
| Height at born (cm): mean (SD) | 49.92 (2.45) | 49.93 (0.25) | 0.15 | 419 | 0.87 (0.13 to 2.01) |
| Delivery mode (n) | |||||
| Cesarean | 33 | 37 | 0.63 | 417 | 0.725 (0.45 to 2.13) |
| Vaginal | 169 | 178 | 0.19 | 0.205 (0.11 to 2.22) | |
| Period | MDI-C Subscale Scores | Depressive Symptoms Group (N = 205) Average Score | Non-Depressive Symptoms Group (N = 215) Average Score | Kruskal-Wallis Score | df | p-Value | 95% CI |
|---|---|---|---|---|---|---|---|
| Primary school | Anxiety | 60 | 37 | 100.64 | 240 | <0.0001 | 98.12 to 104.12 |
| Self-esteem | 54 | 27 | 114.19 | 240 | <0.0001 | 112.34 to 116.34 | |
| Sad mood | 62 | 47 | 121.51 | 145.12 | <0.0001 | 119.11 to 123.71 | |
| Powerlessness | 58 | 40 | 123.29 | 165.62 | <0.0001 | 121.14 to 125.24 | |
| Social Introversion | 63 | 43 | 71.26 | 153.91 | <0.0001 | 69.16 to 73.17 | |
| Low energy | 59 | 34 | 72.46 | 152.73 | <0.0001 | 70.35 to 74.67 | |
| Pessimism | 58 | 25 | 109.79 | 142.67 | <0.0001 | 107.34 to 111.78 | |
| Provocation | 55 | 41 | 82.43 | 234 | <0.0001 | 80.45 to 85.98 | |
| Middle school | Anxiety | 60 | 42 | 35.82 | 135 | <0.0001 | 32.78 to 38.14 |
| Self-esteem | 61 | 41 | 58.82 | 135 | <0.0001 | 56.87 to 61.87 | |
| Sad mood | 62 | 45 | 54.24 | 128.21 | <0.0001 | 52.76 to 56.76 | |
| Powerlessness | 61 | 46 | 65.27 | 135 | <0.0001 | 63.56 to 67.83 | |
| Social Introversion | 63 | 41 | 29.62 | 13.72 | <0.0001 | 27.54 to 31.65 | |
| Low energy | 58 | 29 | 31.31 | 134 | <0.0001 | 29.76 to 33.45 | |
| Pessimism | 58 | 41 | 52.45 | 13.31 | 0.013 | 54.78 to 54.65 | |
| Provocation | 64 | 36 | 32.24 | 134 | <0.0001 | 34.92 to 35.73 | |
| High school | Anxiety | 59 | 38 | 20.57 | 53.84 | <0.0001 | 18.46 to 22.34 |
| Self-esteem | 77 | 35 | 15.67 | 58 | <0.0001 | 12.35 to 17.87 | |
| Sad mood | 60 | 37 | 19.06 | 58 | <0.0001 | 17.84 to 21.46 | |
| Powerlessness | 60 | 41 | 19.68 | 58 | <0.0001 | 17.83 to 21.78 | |
| Social Introversion | 62 | 40 | 11.89 | 58 | <0.0001 | 9.84 to 13.49 | |
| Low energy | 58 | 42 | 14.74 | 58 | <0.0001 | 12.84 to 16.78 | |
| Pessimism | 65 | 41 | 5.83 | 58 | <0.0001 | 3.79 to 7.94 | |
| Provocation | 56 | 41 | 16.15 | 54.18 | <0.0001 | 14.74 to 18.74 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vaivre-Douret, L.; Hamdioui, S. Developmental Trajectory of Depressive Symptoms from Early Childhood through High School in Children and Adolescents with a High Intellectual Potential. Children 2023, 10, 1738. https://doi.org/10.3390/children10111738
Vaivre-Douret L, Hamdioui S. Developmental Trajectory of Depressive Symptoms from Early Childhood through High School in Children and Adolescents with a High Intellectual Potential. Children. 2023; 10(11):1738. https://doi.org/10.3390/children10111738
Chicago/Turabian StyleVaivre-Douret, Laurence, and Soukaina Hamdioui. 2023. "Developmental Trajectory of Depressive Symptoms from Early Childhood through High School in Children and Adolescents with a High Intellectual Potential" Children 10, no. 11: 1738. https://doi.org/10.3390/children10111738
APA StyleVaivre-Douret, L., & Hamdioui, S. (2023). Developmental Trajectory of Depressive Symptoms from Early Childhood through High School in Children and Adolescents with a High Intellectual Potential. Children, 10(11), 1738. https://doi.org/10.3390/children10111738