

Screen Time and Its Health Consequences in Children and Adolescents

Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search and Study Selection
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
3. Results
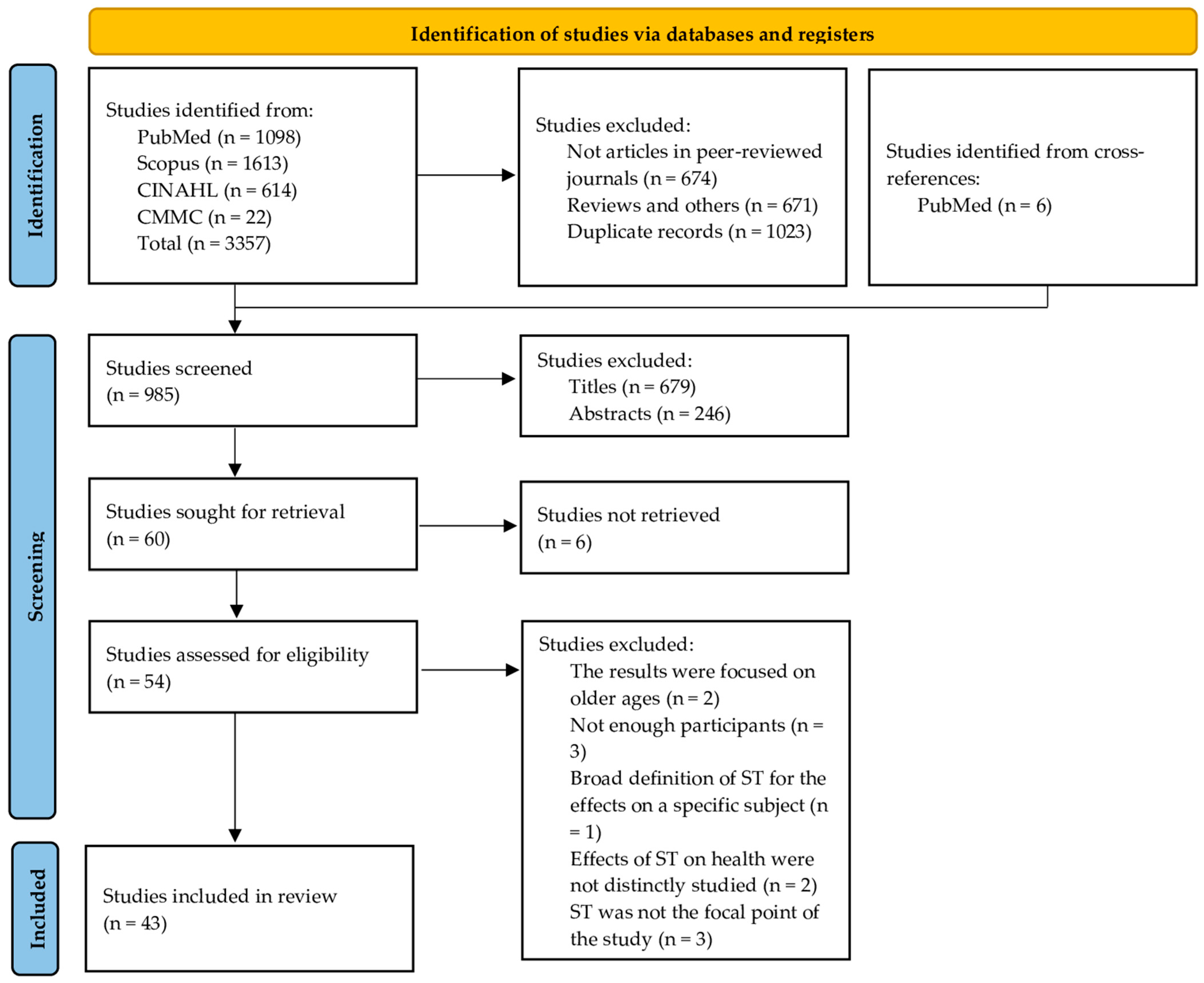
3.1. Selection of Studies
3.2. Obesity
3.3. Other Cardiometabolic Risk Factors
3.4. Mental Health
3.4.1. Internalising Symptoms
3.4.2. Externalising Symptoms
3.4.3. Suicidal Behaviours
3.4.4. Healthcare Setting
3.5. Dietary Habits and Eating Disorders
3.6. Development
3.7. Child–Parent Relationship
3.8. Sleep and Physical Activity
3.9. Eyesight and Headaches
3.10. Musculoskeletal System
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ADHD | attention-deficit/hyperactivity disorder |
| AIS | Adolescent idiopathic scoliosis |
| ASD | Autism spectrum disorder |
| BP | Blood pressure |
| CVD | Cardiovascular disease |
| CVF | Cardiovascular fitness |
| DES | Digital eye strain |
| DM | Digital media |
| ED(s) | Eating disorder(s) |
| EFE | Emotion-focused engagement coping |
| h | Hour(s) |
| IR | Insulin resistance |
| mo | month(s) old |
| PA | Physical activity |
| PF | Protective factor |
| PFE | Problem-focused engagement coping |
| RF | Risk factor |
| SA | Suicide attempt |
| SB | Suicidal behaviour |
| SH | Self-harm |
| SI | Suicidal ideation |
| SM | Social media |
| ST | Screen time |
| UPF | Ultra-processed foods |
| VG(s) | Video game(s) |
| WHO | World Health Organization |
| yo | year(s) old |
References
- World Health Organization. Guidelines on Physical Activity, Sedentary Behaviour and Sleep for Children under 5 Years of Age; WHO: Geneva, Switzerland, 2019. [Google Scholar]
- Madigan, S.; Eirich, R.; Pador, P.; McArthur, B.A.; Neville, R.D. Assessment of Changes in Child and Adolescent Screen Time During the COVID-19 Pandemic: A Systematic Review and Meta-analysis. JAMA Pediatr. 2022, 176, 1188–1198. [Google Scholar] [CrossRef]
- Dietz, W.H.; Gortmaker, S.L. Do we fatten our children at the television set? Obesity and television viewing in children and adolescents. Pediatrics 1985, 75, 807–812. [Google Scholar] [CrossRef] [PubMed]
- Dy, A.B.C.; Santos, S.K. Measuring effects of screen time on the development of children in the Philippines: A cross-sectional study. BMC Public Health 2023, 23, 1261. [Google Scholar] [CrossRef]
- Hinten, A.E.; Wolsey, K.; Henderson, A.M.E.; Scarf, D. A Survey of Screen Media Access and Use in Primary School Children’s Households. Children 2022, 10, 28. [Google Scholar] [CrossRef]
- Pedersen, J.; Rasmussen, M.G.; Neland, M.; Gr¯ntved, A. Screen-based media use and blood pressure in preschool-aged children: A prospective study in the Odense Child Cohort. Scand. J. Public Health 2021, 49, 495–502. [Google Scholar] [CrossRef]
- Ponti, M. Screen time and preschool children: Promoting health and development in a digital world. Paediatr. Child Health 2023, 28, 184–202. [Google Scholar] [CrossRef]
- Bozzola, E.; Spina, G.; Agostiniani, R.; Barni, S.; Russo, R.; Scarpato, E.; Di Mauro, A.; Di Stefano, A.V.; Caruso, C.; Corsello, G.; et al. The Use of Social Media in Children and Adolescents: Scoping Review on the Potential Risks. Int. J. Environ. Res. Public Health 2022, 19, 9960. [Google Scholar] [CrossRef]
- Stiglic, N.; Viner, R.M. Effects of screentime on the health and well-being of children and adolescents: A systematic review of reviews. BMJ Open 2019, 9, e023191. [Google Scholar] [CrossRef] [PubMed]
- Fang, K.; Mu, M.; Liu, K.; He, Y. Screen time and childhood overweight/obesity: A systematic review and meta-analysis. Child Care Health Dev. 2019, 45, 744–753. [Google Scholar] [CrossRef] [PubMed]
- Zhang, G.; Wu, L.; Zhou, L.; Lu, W.; Mao, C. Television watching and risk of childhood obesity: A meta-analysis. Eur. J. Public Health 2016, 26, 13–18. [Google Scholar] [CrossRef]
- Khajeheian, D.; Colabi, A.M.; Ahmad Kharman Shah, N.B.; Bt Wan Mohamed Radzi, C.W.J.; Jenatabadi, H.S. Effect of Social Media on Child Obesity: Application of Structural Equation Modeling with the Taguchi Method. Int. J. Environ. Res. Public Health 2018, 15, 1343. [Google Scholar] [CrossRef]
- Haghjoo, P.; Siri, G.; Soleimani, E.; Farhangi, M.A.; Alesaeidi, S. Screen time increases overweight and obesity risk among adolescents: A systematic review and dose-response meta-analysis. BMC Prim. Care 2022, 23, 161. [Google Scholar] [CrossRef]
- Mineshita, Y.; Kim, H.K.; Chijiki, H.; Nanba, T.; Shinto, T.; Furuhashi, S.; Oneda, S.; Kuwahara, M.; Suwama, A.; Shibata, S. Screen time duration and timing: Effects on obesity, physical activity, dry eyes, and learning ability in elementary school children. BMC Public Health 2021, 21, 422. [Google Scholar] [CrossRef]
- Schwarzfischer, P.; Gruszfeld, D.; Socha, P.; Luque, V.; Closa-Monasterolo, R.; Rousseaux, D.; Moretti, M.; ReDionigi, A.; Verduci, E.; Koletzko, B.; et al. Effects of screen time and playing outside on anthropometric measures in preschool aged children. PLoS ONE 2020, 15, e0229708. [Google Scholar] [CrossRef]
- Nightingale, C.M.; Rudnicka, A.R.; Donin, A.S.; Sattar, N.; Cook, D.G.; Whincup, P.H.; Owen, C.G. Screen time is associated with adiposity and insulin resistance in children. Arch. Dis. Child. 2017, 102, 612–616. [Google Scholar] [CrossRef] [PubMed]
- Bellissimo, N.; Pencharz, P.B.; Thomas, S.G.; Anderson, G.H. Effect of television viewing at mealtime on food intake after a glucose preload in boys. Pediatr. Res. 2007, 61, 745–749. [Google Scholar] [CrossRef] [PubMed]
- Russell, S.J.; Croker, H.; Viner, R.M. The effect of screen advertising on children’s dietary intake: A systematic review and meta-analysis. Obes. Rev. 2019, 20, 554–568. [Google Scholar] [CrossRef]
- Shaban Mohamed, M.A.; AbouKhatwa, M.M.; Saifullah, A.A.; Hareez Syahmi, M.; Mosaad, M.; Elrggal, M.E.; Dehele, I.S.; Elnaem, M.H. Risk Factors, Clinical Consequences, Prevention, and Treatment of Childhood Obesity. Children 2022, 9, 1975. [Google Scholar] [CrossRef] [PubMed]
- Tremblay, M.S.; LeBlanc, A.G.; Kho, M.E.; Saunders, T.J.; Larouche, R.; Colley, R.C.; Goldfield, G.; Connor Gorber, S. Systematic review of sedentary behaviour and health indicators in school-aged children and youth. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 98. [Google Scholar] [CrossRef]
- Cureau, F.V.; Ekelund, U.; Bloch, K.V.; Schaan, B.D. Does body mass index modify the association between physical activity and screen time with cardiometabolic risk factors in adolescents? Findings from a country-wide survey. Int. J. Obes. 2017, 41, 551–559. [Google Scholar] [CrossRef]
- Sina, E.; Buck, C.; Veidebaum, T.; Siani, A.; Reisch, L.; Pohlabeln, H.; Pala, V.; Moreno, L.A.; Molnar, D.; Lissner, L.; et al. Media use trajectories and risk of metabolic syndrome in European children and adolescents: The IDEFICS/I. Family cohort. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 134. [Google Scholar] [CrossRef] [PubMed]
- Kjellenberg, K.; Ekblom, Ö.; Stålman, C.; Helgadóttir, B.; Nyberg, G. Associations between Physical Activity Patterns, Screen Time and Cardiovascular Fitness Levels in Swedish Adolescents. Children 2021, 8, 998. [Google Scholar] [CrossRef] [PubMed]
- Hardy, L.L.; Ding, D.; Peralta, L.R.; Mihrshahi, S.; Merom, D. Association Between Sitting, Screen Time, Fitness Domains, and Fundamental Motor Skills in Children Aged 5-16†Years: Cross-Sectional Population Study. J. Phys. Act. Health 2018, 15, 933–940. [Google Scholar] [CrossRef] [PubMed]
- Vanderloo, L.M.; Keown-Stoneman, C.D.G.; Sivanesan, H.; Parkin, P.C.; Maguire, J.L.; Anderson, L.N.; Tremblay, M.S.; Birken, C.S.; Collaborative, T.K. Association of screen time and cardiometabolic risk in school-aged children. Prev. Med. Rep. 2020, 20, 101183. [Google Scholar] [CrossRef] [PubMed]
- Tandon, P.S.; Zhou, C.; Johnson, A.M.; Gonzalez, E.S.; Kroshus, E. Association of Children’s Physical Activity and Screen Time with Mental Health During the COVID-19 Pandemic. JAMA Netw. Open 2021, 4, e2127892. [Google Scholar] [CrossRef]
- Marin-Dragu, S.; Forbes, A.; Sheikh, S.; Iyer, R.S.; Pereira Dos Santos, D.; Alda, M.; Hajek, T.; Uher, R.; Wozney, L.; Paulovich, F.V.; et al. Associations of active and passive smartphone use with measures of youth mental health during the COVID-19 pandemic. Psychiatry Res. 2023, 326, 115298. [Google Scholar] [CrossRef]
- Liu, M.; Kamper-DeMarco, K.E.; Zhang, J.; Xiao, J.; Dong, D.; Xue, P. Time Spent on Social Media and Risk of Depression in Adolescents: A Dose-Response Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 5164. [Google Scholar] [CrossRef]
- Hökby, S.; Westerlund, J.; Alvarsson, J.; Carli, V.; Hadlaczky, G. Longitudinal Effects of Screen Time on Depressive Symptoms among Swedish Adolescents: The Moderating and Mediating Role of Coping Engagement Behavior. Int. J. Environ. Res. Public Health 2023, 20, 3771. [Google Scholar] [CrossRef]
- Hilty, D.M.; Stubbe, D.; McKean, A.J.; Hoffman, P.E.; Zalpuri, I.; Myint, M.T.; Joshi, S.V.; Pakyurek, M.; Li, S.T. A scoping review of social media in child, adolescents and young adults: Research findings in depression, anxiety and other clinical challenges. BJPsych Open 2023, 9, e152. [Google Scholar] [CrossRef]
- Zink, J.; Belcher, B.R.; Kechter, A.; Stone, M.D.; Leventhal, A.M. Reciprocal associations between screen time and emotional disorder symptoms during adolescence. Prev. Med. Rep. 2019, 13, 281–288. [Google Scholar] [CrossRef]
- Kahn, M.; Schnabel, O.; Gradisar, M.; Rozen, G.S.; Slone, M.; Atzaba-Poria, N.; Tikotzky, L.; Sadeh, A. Sleep, screen time and behaviour problems in preschool children: An actigraphy study. Eur. Child Adolesc. Psychiatry 2021, 30, 1793–1802. [Google Scholar] [CrossRef]
- Tamana, S.K.; Ezeugwu, V.; Chikuma, J.; Lefebvre, D.L.; Azad, M.B.; Moraes, T.J.; Subbarao, P.; Becker, A.B.; Turvey, S.E.; Sears, M.R.; et al. Screen-time is associated with inattention problems in preschoolers: Results from the CHILD birth cohort study. PLoS ONE 2019, 14, e0213995. [Google Scholar] [CrossRef]
- Lin, W.H.; Liu, C.H.; Yi, C.C. Exposure to sexually explicit media in early adolescence is related to risky sexual behavior in emerging adulthood. PLoS ONE 2020, 15, e0230242. [Google Scholar] [CrossRef]
- John, A.; Glendenning, A.C.; Marchant, A.; Montgomery, P.; Stewart, A.; Wood, S.; Lloyd, K.; Hawton, K. Self-Harm, Suicidal Behaviours, and Cyberbullying in Children and Young People: Systematic Review. J. Med. Internet Res. 2018, 20, e129. [Google Scholar] [CrossRef] [PubMed]
- Rodrigo-Yanguas, M.; Gonz·lez-TardÛn, C.; Bella-Fern·ndez, M.; Blasco-Fontecilla, H. Serious Video Games: Angels or Demons in Patients with Attention-Deficit Hyperactivity Disorder? A Quasi-Systematic Review. Front. Psychiatry 2022, 13, 798480. [Google Scholar] [CrossRef] [PubMed]
- Sajeev, M.F.; Kelada, L.; Yahya Nur, A.B.; Wakefield, C.E.; Wewege, M.A.; Karpelowsky, J.; Akimana, B.; Darlington, A.S.; Signorelli, C. Interactive video games to reduce paediatric procedural pain and anxiety: A systematic review and meta-analysis. Br. J. Anaesth. 2021, 127, 608–619. [Google Scholar] [CrossRef]
- Rocha, L.L.; Gratão, L.H.A.; Carmo, A.S.D.; Costa, A.B.P.; Cunha, C.F.; Oliveira, T.R.P.R.; Mendes, L.L. School Type, Eating Habits, and Screen Time are Associated with Ultra-Processed Food Consumption Among Brazilian Adolescents. J. Acad. Nutr. Diet. 2021, 121, 1136–1142. [Google Scholar] [CrossRef]
- Tambalis, K.D.; Panagiotakos, D.B.; Psarra, G.; Sidossis, L.S. Screen time and its effect on dietary habits and lifestyle among schoolchildren. Cent. Eur. J. Public Health 2020, 28, 260–266. [Google Scholar] [CrossRef]
- Helgadóttir, B.; BaurÈn, H.; Kjellenberg, K.; Ekblom, Ö.; Nyberg, G. Breakfast Habits and Associations with Fruit and Vegetable Intake, Physical Activity, Sedentary Time, and Screen Time among Swedish 13–14-Year-Old Girls and Boys. Nutrients 2021, 13, 4467. [Google Scholar] [CrossRef]
- Mougharbel, F.; Goldfield, G.S. Psychological Correlates of Sedentary Screen Time Behaviour Among Children and Adolescents: A Narrative Review. Curr. Obes. Rep. 2020, 9, 493–511. [Google Scholar] [CrossRef]
- Wilksch, S.M.; O’Shea, A.; Ho, P.; Byrne, S.; Wade, T.D. The relationship between social media use and disordered eating in young adolescents. Int. J. Eat. Disord. 2020, 53, 96–106. [Google Scholar] [CrossRef] [PubMed]
- Lonergan, A.R.; Bussey, K.; Fardouly, J.; Griffiths, S.; Murray, S.B.; Hay, P.; Mond, J.; Trompeter, N.; Mitchison, D. Protect me from my selfie: Examining the association between photo-based social media behaviors and self-reported eating disorders in adolescence. Int. J. Eat. Disord. 2020, 53, 485–496. [Google Scholar] [CrossRef] [PubMed]
- Chong, S.C.; Teo, W.Z.; Shorey, S. Exploring the perception of parents on children’s screentime: A systematic review and meta-synthesis of qualitative studies. Pediatr. Res. 2023, 94, 915–925. [Google Scholar] [CrossRef] [PubMed]
- Kerai, S.; Almas, A.; Guhn, M.; Forer, B.; Oberle, E. Screen time and developmental health: Results from an early childhood study in Canada. BMC Public Health 2022, 22, 310. [Google Scholar] [CrossRef]
- Madigan, S.; McArthur, B.A.; Anhorn, C.; Eirich, R.; Christakis, D.A. Associations Between Screen Use and Child Language Skills: A Systematic Review and Meta-analysis. JAMA Pediatr. 2020, 174, 665–675. [Google Scholar] [CrossRef] [PubMed]
- Pagani, L.S.; Fitzpatrick, C.; Barnett, T.A. Early childhood television viewing and kindergarten entry readiness. Pediatr. Res. 2013, 74, 350–355. [Google Scholar] [CrossRef] [PubMed]
- Sugiyama, M.; Tsuchiya, K.J.; Okubo, Y.; Rahman, M.S.; Uchiyama, S.; Harada, T.; Iwabuchi, T.; Okumura, A.; Nakayasu, C.; Amma, Y.; et al. Outdoor Play as a Mitigating Factor in the Association Between Screen Time for Young Children and Neurodevelopmental Outcomes. JAMA Pediatr. 2023, 177, 303–310. [Google Scholar] [CrossRef]
- Edelson, L.R.; Mathias, K.C.; Fulgoni, V.L.; Karagounis, L.G. Screen-based sedentary behavior and associations with functional strength in 6-15 year-old children in the United States. BMC Public Health 2016, 16, 116. [Google Scholar] [CrossRef]
- Lin, L.Y.; Cherng, R.J.; Chen, Y.J.; Yang, H.M. Effects of television exposure on developmental skills among young children. Infant Behav. Dev. 2015, 38, 20–26. [Google Scholar] [CrossRef]
- Heffler, K.F.; Sienko, D.M.; Subedi, K.; McCann, K.A.; Bennett, D.S. Association of Early-Life Social and Digital Media Experiences with Development of Autism Spectrum Disorder-Like Symptoms. JAMA Pediatr. 2020, 174, 690–696. [Google Scholar] [CrossRef]
- Manwell, L.A.; Tadros, M.; Ciccarelli, T.M.; Eikelboom, R. Digital dementia in the internet generation: Excessive screen time during brain development will increase the risk of Alzheimer’s disease and related dementias in adulthood. J. Integr. Neurosci. 2022, 21, 28. [Google Scholar] [CrossRef] [PubMed]
- Moon, J.H.; Cho, S.Y.; Lim, S.M.; Roh, J.H.; Koh, M.S.; Kim, Y.J.; Nam, E. Smart device usage in early childhood is differentially associated with fine motor and language development. Acta Paediatr. 2019, 108, 903–910. [Google Scholar] [CrossRef] [PubMed]
- Myers, L.J.; LeWitt, R.B.; Gallo, R.E.; Maselli, N.M. Baby FaceTime: Can toddlers learn from online video chat? Dev. Sci. 2017, 20, e12430. [Google Scholar] [CrossRef]
- Zhu, Y.; Deng, L.; Wan, K. The association between parent-child relationship and problematic internet use among English- and Chinese-language studies: A meta-analysis. Front. Psychol. 2022, 13, 885819. [Google Scholar] [CrossRef]
- Jago, R.; Zahra, J.; Edwards, M.J.; Kesten, J.M.; Solomon-Moore, E.; Thompson, J.L.; Sebire, S.J. Managing the screen-viewing behaviours of children aged 5-6 years: A qualitative analysis of parental strategies. BMJ Open 2016, 6, e010355. [Google Scholar] [CrossRef]
- Lin, Y.; Zhang, X.; Huang, Y.; Jia, Z.; Chen, J.; Hou, W.; Zhao, L.; Wang, G.; Zhu, J. Relationships between screen viewing and sleep quality for infants and toddlers in China: A cross-sectional study. Front. Pediatr. 2022, 10, 987523. [Google Scholar] [CrossRef]
- Zhu, R.; Fang, H.; Chen, M.; Hu, X.; Cao, Y.; Yang, F.; Xia, K. Screen time and sleep disorder in preschool children: Identifying the safe threshold in a digital world. Public Health 2020, 186, 204–210. [Google Scholar] [CrossRef]
- Chang, A.M.; Aeschbach, D.; Duffy, J.F.; Czeisler, C.A. Evening use of light-emitting eReaders negatively affects sleep, circadian timing, and next-morning alertness. Proc. Natl. Acad. Sci. USA 2015, 112, 1232–1237. [Google Scholar] [CrossRef]
- Higuchi, S.; Motohashi, Y.; Liu, Y.; Maeda, A. Effects of playing a computer game using a bright display on presleep physiological variables, sleep latency, slow wave sleep and REM sleep. J. Sleep Res. 2005, 14, 267–273. [Google Scholar] [CrossRef]
- Exelmans, L.; Van den Bulck, J. Bedtime, shuteye time and electronic media: Sleep displacement is a two-step process. J. Sleep Res. 2017, 26, 364–370. [Google Scholar] [CrossRef]
- Jain, S.; Shrivastava, S.; Mathur, A.; Pathak, D.; Pathak, A. Prevalence and Determinants of Excessive Screen Viewing Time in Children Aged 3-15 Years and Its Effects on Physical Activity, Sleep, Eye Symptoms and Headache. Int. J. Environ. Res. Public Health 2023, 20, 3449. [Google Scholar] [CrossRef]
- Dahlgren, A.; Sjöblom, L.; Eke, H.; Bonn, S.E.; Trolle Lagerros, Y. Screen time and physical activity in children and adolescents aged 10-15 years. PLoS ONE 2021, 16, e0254255. [Google Scholar] [CrossRef]
- Azevedo, N.; Ribeiro, J.C.; Machado, L. Back pain in children and adolescents: A cross-sectional study. Eur. Spine J. 2023, 32, 3280–3289. [Google Scholar] [CrossRef]
- Foreman, J.; Salim, A.T.; Praveen, A.; Fonseka, D.; Ting, D.S.W.; Guang He, M.; Bourne, R.R.A.; Crowston, J.; Wong, T.Y.; Dirani, M. Association between digital smart device use and myopia: A systematic review and meta-analysis. Lancet Digit. Health 2021, 3, e806–e818. [Google Scholar] [CrossRef]
- Kaur, K.; Gurnani, B.; Nayak, S.; Deori, N.; Kaur, S.; Jethani, J.; Singh, D.; Agarkar, S.; Hussaindeen, J.R.; Sukhija, J.; et al. Digital Eye Strain- A Comprehensive Review. Ophthalmol. Ther. 2022, 11, 1655–1680. [Google Scholar] [CrossRef]
- Himebaugh, N.L.; Begley, C.G.; Bradley, A.; Wilkinson, J.A. Blinking and tear break-up during four visual tasks. Optom. Vis. Sci. 2009, 86, E106–E114. [Google Scholar] [CrossRef]
- Attygalle, U.R.; Hewawitharana, G.; Wijesinghe, C.J. Migraine, attention deficit hyperactivity disorder and screen time in children attending a Sri Lankan tertiary care facility: Are they associated? BMC Neurol. 2020, 20, 275. [Google Scholar] [CrossRef]
- Lund, J.; Berring-Uldum, A.; Colak, M.; Debes, N.M.M. Headache in Children and Adolescents: The Association between Screen Time and Headache within a Clinical Headache Population. Neuropediatrics 2022, 53, 221–226. [Google Scholar] [CrossRef]
- Montagni, I.; Guichard, E.; Carpenet, C.; Tzourio, C.; Kurth, T. Screen time exposure and reporting of headaches in young adults: A cross-sectional study. Cephalalgia 2016, 36, 1020–1027. [Google Scholar] [CrossRef]
- Baradaran Mahdavi, S.; Mazaheri-Tehrani, S.; Riahi, R.; Vahdatpour, B.; Kelishadi, R. Sedentary behavior and neck pain in children and adolescents; a systematic review and meta-analysis. Health Promot. Perspect. 2022, 12, 240–248. [Google Scholar] [CrossRef]
- Dou, Q.; Zhu, Z.; Zhu, L.; Wang, W.; Guo, L.; Ru, S.; Chen, X.; Yang, L.; Lu, C.; Yan, B. Academic-related factors and daily lifestyle habits associated with adolescent idiopathic scoliosis: A case-control study. Environ. Health Prev. Med. 2023, 28, 23. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author | Year | Type | Sample (N) | Main Findings |
|---|---|---|---|---|
| Dy ABC et al. [4] | 2023 | Cross-sectional | 419 | More than 2 h of daily ST was negatively associated with toddler development. Co-viewing was a protective factor against excessive ST, while background media and parents with excessive ST were risk factors. |
| Hinten AE et al. [5] | 2022 | Cross-sectional | 356 | Daily activities of primary school children were studied by analysing diary entries filled out by parents. |
| Fang K et al. [10] | 2019 | Meta-analysis | n/a 1 | More than 2 h of daily ST, TV, or ST and computer use was associated with obesity. |
| Zhang G et al. [11] | 2015 | Meta-analysis | n/a 1 | Excessive ST was positively associated with obesity. For every hour of ST, the risk of obesity increased by 13%. |
| Khajeheian D et al. [12] | 2018 | Cross-sectional | 1569 | Excessive ST was positively associated with obesity. The association was stronger amongst high school students when compared to primary school students. |
| Haghjoo, P et al. [13] | 2023 | Meta-analysis | n/a 1 | Excessive ST was associated with a 20% higher risk for obesity. No dose-dependent effect could be established. |
| Mineshita Y et al. [14] | 2021 | Cross-sectional | 6334 | Longer ST duration was positively associated with obesity and negatively associated with PA and learning ability. ST before bedtime was positively associated with obesity and negatively associated with dry eyes and learning ability. |
| Schwarzfischer P et al. [15] | 2020 | Longitudinal | 526 | More than 1 h of daily ST was positively associated with obesity in children aged 3–6 yo. At the ages of 3–6 yo, 1 h of additional ST led to increased risk for obesity at the age of 6 yo. |
| Nightingale CM et al. [16] | 2017 | Cross-sectional | 4495 | More than 3 h of daily ST was positively associated with adiposity and type 2 diabetes risk factors in children aged 9–10 yo. |
| Bellissimo N et al. * [17] | 2007 | Case control | 14 | TV ST affects satiation signals, leading to higher caloric intake during lunchtime in boys. |
| Russell SJ et al. [18] | 2018 | Meta-analysis | n/a 1 | TV viewing and advertisements in VGs were associated with higher caloric intake in children and adolescents. |
| Cureau FV et al. [21] | 2016 | Cross-sectional | 36,956 | Equal or more than 6 h daily of ST was positively associated with cardiometabolic risk in overweight adolescents aged 12–17 yo. |
| Sina E et al. [22] | 2021 | Longitudinal | 10,359 | DM use increases with age. Excessive ST was positively associated with metabolic syndrome and cardiometabolic risk in both sexes. More than normal ST increase was positively associated with metabolic syndrome in both sexes and insulin resistance in boys. PA was a protective mechanism. |
| Kjellenberg K et al. [23] | 2021 | Cross-sectional | 884 | More than 5 h of ST on weekends was negatively associated with cardiovascular fitness levels in boys aged 13 yo; 3–4 h or more of ST on weekends was negatively associated with cardiovascular fitness levels in girls aged 13 yo. |
| Hardy LL et al. [24] | 2018 | Cross-sectional | 6405 | Longer ST was negatively associated with PA attributes; the association was stronger for adolescents, girls, and weekday ST. |
| Pedersen J et al. [6] | 2021 | Longitudinal | 628 | The change in total ST from the age 3 yo to 5 yo was not associated with increased BP or increased BMI measurements. |
| Pedersen J et al. [6] | 2021 | Cross-sectional | 964 | Excessive ST was not associated with increased BP in children aged 5 yo. |
| Pedersen J et al. [6] | 2021 | Cross-sectional | 963 | With ST before bedtime, 2–5 days per week or more was positively associated with increased BP in children aged 5 yo. |
| Vanderloo LM et al. [25] | 2020 | Cross-sectional | 567 | Excessive ST was negatively associated with HDL-c. For every hour of ST, HDL-c decreased by 0.008 mmol/l. Excessive ST was not associated with other individual cardiometabolic risk factors. |
| Tandon PS et al. [26] | 2021 | Cross-sectional | 1000 | Excessive ST was negatively associated with mental health and externalising and internalising symptoms in children and adolescents. |
| Marin-Dragu S et al. [27] | 2023 | Cross-sectional | 451 | Subjective ways of measuring active and passive smartphone use were studied. The metric corresponding to passive use was positively associated with externalising and internalising symptoms. The metric corresponding to active use was negatively associated with externalising symptoms. |
| Liu M et al. [28] | 2022 | Meta-analysis | n/a 1 | Time spent on social media was positively associated with depression. A linear, dose-dependent correlation was established, and it was more prominent in girls. |
| Hökby S et al. [29] | 2023 | Longitudinal | 4793 | Coping mechanisms were studied. Excessive ST was only associated with depression when problem-focused engagement coping was poor. Excessive ST’s association with depression was not moderated by emotion-focused engagement coping. |
| Zink J et al. [31] | 2019 | Longitudinal | 2525 | TV, computer use, and video games were partially bidirectionally linked with emotional disorder symptoms. The relationship was moderated by PA. |
| Kahn M et al. [32] | 2021 | Cross-sectional | 145 | Excessive ST was negatively associated with sleep duration. Excessive ST was positively associated with behavioural problems and externalising symptoms in children aged 3–6 yo only when sleep duration was short. |
| Tamana SK et al. [33] | 2019 | Longitudinal | 2427 | More than 2 h of ST at the age of 3 or 5 was associated with externalising behaviour problems, and attention problems at the age of 5 yo. ST was not associated with internalising behaviour problems. |
| Lin WH et al. [34] | 2020 | Longitudinal | 2054 | Exposure to sexually explicit media at the age of 14 yo was positively associated with early sex debut and unsafe sex at the age of 20 yo. |
| Lin WH et al. [34] | 2020 | Longitudinal | 1477 | Exposure to sexually explicit media at the age of 14 yo was positively associated with multiple sexual partners by the age of 24 yo. |
| Sajeev MF et al. [37] | 2021 | Meta-analysis | n/a 1 | Special VGs were positively associated with less in-hospital paediatric anxiety and pain. They were not associated with less caregiver anxiety. |
| Rocha LL et al. [38] | 2021 | Cross-sectional | 71,553 | More than 2 h of daily ST and eating in front of a TV, computer, or VG was positively associated with ultra-processed food consumption. |
| Tambalis KD et al. [39] | 2020 | Cross-sectional | 177,091 | Excessive ST was positively associated with unhealthy dietary choices, obesity, and adiposity. Excessive ST was negatively associated with sleep duration, PA attributes, and cardiorespiratory fitness. |
| Helgadóttir B et al. [40] | 2021 | Cross-sectional | 1137 | More than 2 h of daily ST was positively associated with skipping breakfast. |
| Wilksch SM et al. [42] | 2019 | Cross-sectional | 996 | Certain social media (differentiated by gender) were associated with thoughts and actions related to eating disorders. Duration of Instagram use was positively associated with eating disorders. Different types of pictures posted on social media were associated differently with eating disorders. |
| Lonergan AR et al. [43] | 2020 | Cross-sectional | 4209 | Certain social media behaviours were positively associated with eating disorders. These behaviours nullified the effect of gender as a moderator. |
| Kerai S et al. [45] | 2022 | Cross-sectional | 2983 | More than 1 h of daily ST was negatively associated with social skills, language and cognitive development, and communication skills in children aged 5 yo. |
| Madigan S et al. [46] | 2020 | Meta-analysis | n/a 1 | Background TV and duration of ST were negatively associated with language skills. Co-viewing, educational ST, and later onset of ST were positively associated with language skills. |
| Sugiyama M et al. [48] | 2023 | Longitudinal | 885 | More than 1 h of ST at the age of 2 y and 8 m was negatively associated with language and daily life skills. The association with daily life skills was mediated by play outside. |
| Heffler KF et al. [51] | 2020 | Longitudinal | 2152 | Passive ST at the age of 12 mo was positively associated with ADHD-like symptoms at the age of 2 yo and not associated with higher ADHD risk at the age of 2 yo. More than 4 h (compared to 3 or less) of passive ST at the age of 18 mo was positively associated with ADHD-like symptoms at the age of 2 yo and not associated with higher ADHD risk at the age of 2 yo. |
| Moon JH et al. [53] | 2018 | Cross-sectional | 117 | Smart-device usage frequency was positively associated with fine motor skills at the age of 3 yo. Appropriate smart-device usage duration was positively associated with social skills at the age of 3 yo. Excessive smart-device usage was negatively associated with expressive (but not total) language skills. |
| Myers LJ et al. [54] | 2016 | Longitudinal | 60 | Video chatting was positively associated with learning and socialising in children aged 2 yo compared to interactive videos. The results were more evident in the middle (17–21 mo) and oldest (aged 22–25 mo) age groups. |
| Zhu Y et al. [55] | 2022 | Meta-analysis | n/a 1 | Parent–child relationship was negatively associated with problematic internet behaviours. |
| Lin Y et al. [57] | 2022 | Cross-sectional | 827 | ST was negatively associated with total sleep time, nighttime sleep, and daytime sleep in infants. It was also negatively associated with total sleep time, nighttime sleep, and daytime sleep in children aged 13–36 mo. |
| Zhu R et al. [58] | 2020 | Cross-sectional | 2278 | More than 1 h of TV ST was positively associated with sleep problems in children aged 3–5 yo. No association was found between computer, iPad, or phone use and sleep problems. |
| Chang AM et al. * [59] | 2015 | Random crossover clinical trial | 12 | e-book reading was negatively associated with melatonin levels and REM sleep compared to print-book reading in young adults. |
| Higuchi S et al. * [60] | 2005 | Random crossover clinical trial | 7 | VGs before sleep were associated with CNS and ANS arousal. |
| Exelmans L et al. * [61] | 2017 | Cross-sectional | 338 | DM displaced sleep in two ways: (i) by delaying bedtime, (ii) by delaying sleeptime |
| Jain S et al. [62] | 2023 | Cross-sectional | 600 | Excessive ST was positively associated with less reading and outdoor play in children. Eye pain was a protective factor against excessive ST. |
| Dahlgren A et al. [63] | 2021 | Cross-sectional | 121 | Objectively measured smartphone use was not associated with PA levels. |
| Azevedo N et al. [64] | 2023 | Cross-sectional | 1463 | Excessive ST was positively associated with back pain in children and adolescents aged 9–19 yo. |
| Foreman J et al. [65] | 2021 | Meta-analysis | n/a 1 | ST was associated with myopia when analysing cross-sectional studies alone (n = 13,431) or cross-sectional and prospective studies combined. ST was not associated when analysing prospective studies alone (n = 3262). |
| Himebaugh NL et al. * [67] | 2009 | Case control | 32 | Excessive ST was negatively associated with blinking rate and tear break-up time. |
| Attygalle UR et al. [68] | 2020 | Cross-sectional | 226 | Excessive ST was positively associated with migraine headaches in children. It was not associated with clinically diagnosed ADHD. |
| Lund J et al. [69] | 2022 | Cross-sectional | 139 | Excessive ST was positively associated with migraine headaches with aura in children and adolescents. |
| Montagni I et al. * [70] | 2016 | Cross-sectional | 4927 | Excessive ST was positively associated with migraine headaches, and more specifically with migraine headaches without aura in university students. |
| Baradaran Mahdavi S et al. [71] | 2022 | Meta-analysis | n/a 1 | Mobile phone use was positively associated with neck pain in children and adolescents. |
| Dou Q et al. [72] | 2023 | Case control | 1837 | More than 2 h of ST was positively associated with adolescent idiopathic scoliosis in children and adolescents aged 10–18 yo. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Priftis, N.; Panagiotakos, D. Screen Time and Its Health Consequences in Children and Adolescents. Children 2023, 10, 1665. https://doi.org/10.3390/children10101665
Priftis N, Panagiotakos D. Screen Time and Its Health Consequences in Children and Adolescents. Children. 2023; 10(10):1665. https://doi.org/10.3390/children10101665
Chicago/Turabian StylePriftis, Nikos, and Demosthenes Panagiotakos. 2023. "Screen Time and Its Health Consequences in Children and Adolescents" Children 10, no. 10: 1665. https://doi.org/10.3390/children10101665
APA StylePriftis, N., & Panagiotakos, D. (2023). Screen Time and Its Health Consequences in Children and Adolescents. Children, 10(10), 1665. https://doi.org/10.3390/children10101665