
Diagnostic Reference Levels in Interventional Pediatric Cardiology: Two-Year Experience in a Tertiary Referral Hospital in Latin America

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
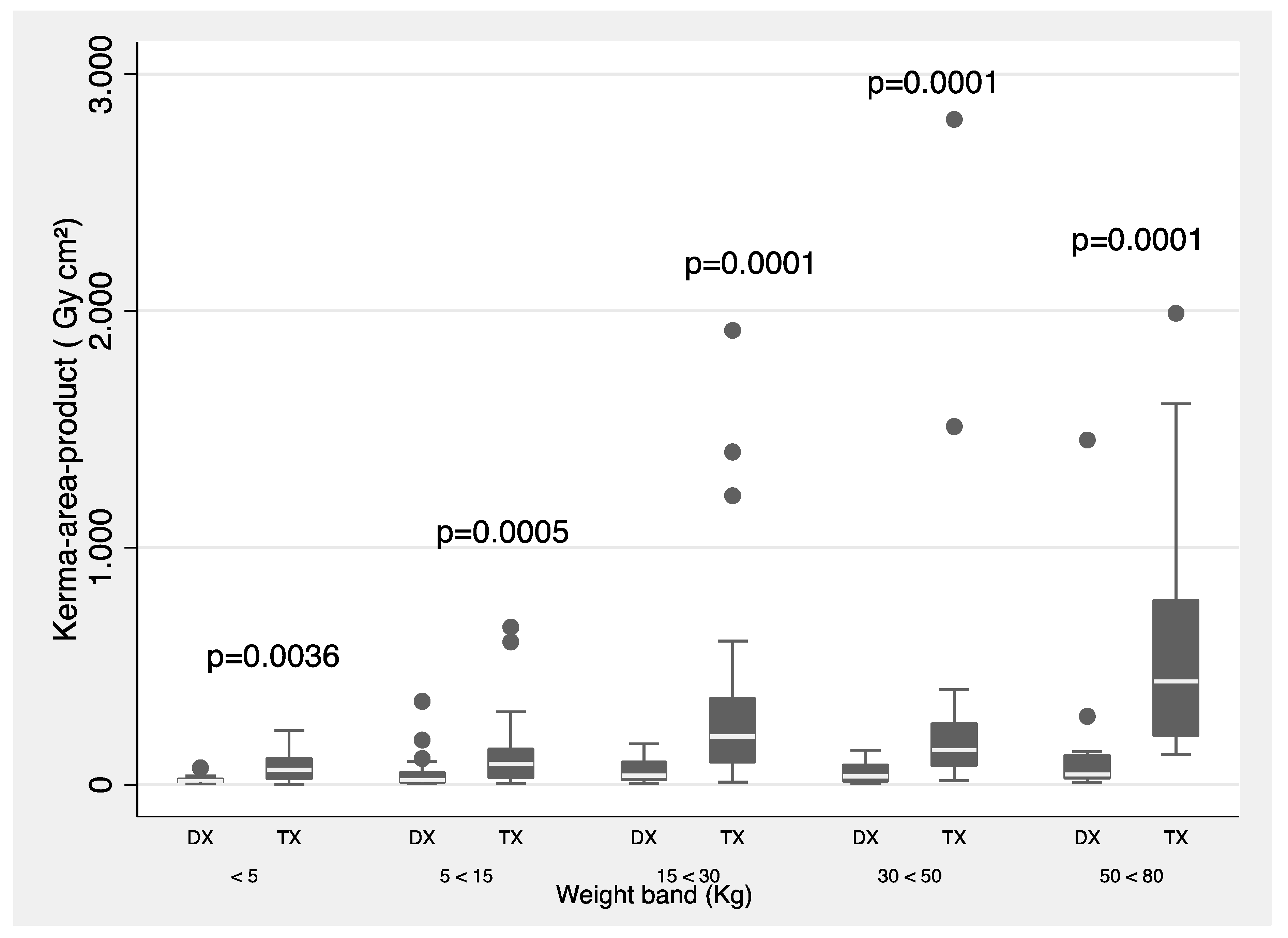
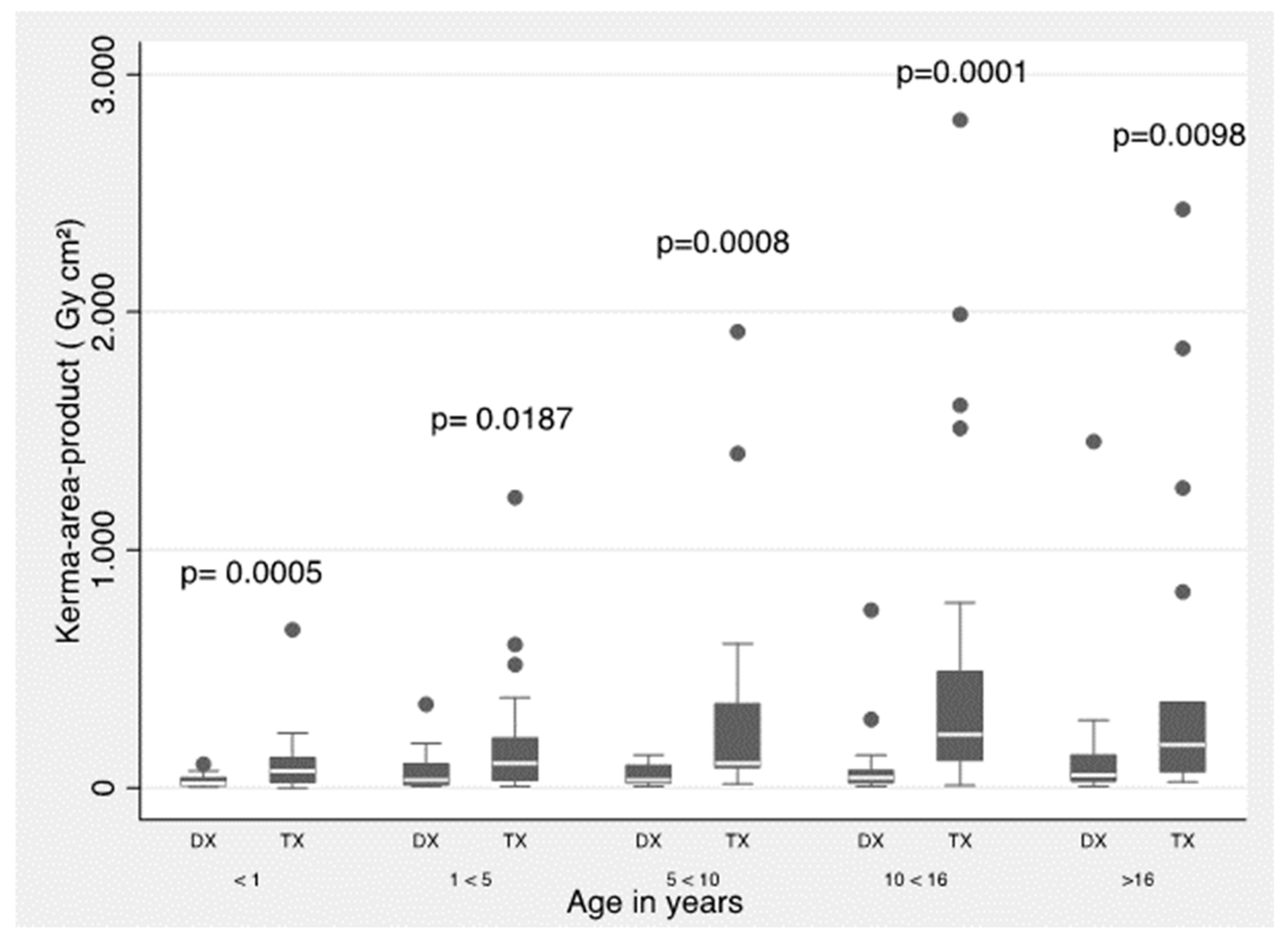
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kang, S.-L.; Benson, L. Recent advances in cardiac catheterization for congenital heart disease. F1000Research 2018, 7, 370. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.-H. Recent advances in pediatric interventional cardiology. Korean J. Pediatr. 2017, 60, 237–244. [Google Scholar] [CrossRef] [PubMed]
- ICRP. International Commission on Radiological Protection. The recommendations of the international commission on radiological protection. Ann. ICRP 2007, 37, 1–332. [Google Scholar]
- ICRP. International Commission on Radiological Protection. Radiological protection in paediatric diagnostic and interventional radiology. Ann. ICRP 2013, 42, 1–63. [Google Scholar] [CrossRef]
- Connolly, B.; Racadio, J.; Towbin, R. Practice of ALARA in the pediatric interventional suite. Pediatr. Radiol. 2006, 36 (Suppl. S2), 163–167. [Google Scholar] [CrossRef]
- Ubeda, C. New Optimization Strategies on Radiation Protection in Fluoroscopy-Guided Interventional Procedures in Pediatrics. Children 2023, 10, 883. [Google Scholar] [CrossRef]
- Ubeda, C.; Miranda, P.; Vano, E. Local patient dose diagnostic reference levels in pediatric interventional cardiology in Chile using age bands and patient weight values. Med. Phys. 2015, 42, 615–622. [Google Scholar] [CrossRef]
- Vañó, E.; Miller, D.L.; Martin, C.J.; Rehani, M.M.; Kang, K.; Rosenstein, M.; Ortiz-Lopez, S.; Mattson, S.; Padovani, R.; Rogers, A. ICRP Publication 135: Diagnostic Reference Levels in Medical Imaging. Ann. ICRP 2017, 46, 1–144. [Google Scholar] [CrossRef]
- Ubeda, C.; Vano, E.; Miranda, P.; Leyton, F. Pilot program on patient dosimetry in pediatric interventional cardiology in Chile. Med. Phys. 2012, 39, 2424–2430. [Google Scholar] [CrossRef]
- Ubeda, C.; Vano, E.; Perez, M.D.; Jímenez, P.; Ramirez, R.; Nader, A.; Miranda, P.; Azcurra, P.; Damsjy, J.; Capdevila, S. Setting up regional diagnostic reference levels for pediatric interventional cardiology in Latin America and the Caribbean countries: Preliminary results and identified challenges. J. Radiol. Prot. 2022, 42, ac87b7. [Google Scholar] [CrossRef]
- Kobayashi, D.; Meadows, J.; Forbes, T.J.; Moore, P.; Javois, A.J.; Pedra, C.A.; Du, W.; Gruenstein, D.H.; Wax, D.F.; Hill, J.A.; et al. Standardizing radiation dose reporting in the pediatric cardiac catheterization laboratory-a multicenter study by the CCISC (Congenital Cardiovascular Interventional Study Consortium). Catheter. Cardiovasc. Interv. 2014, 84, 785–793. [Google Scholar] [CrossRef]
- Ubeda, C.; Vano, E.; Perez, M.D.; Jímenez, P.; Ramirez, R.; Nader, A.; Miranda, P.; Azcurra, P.; Damsky, J.; Capdevila, S.; et al. Optimización de la protección en radiología y cardiología intervencionista pediatrica en América Latina y el Caribe (OPRIPALC). J. Health Med. Sci. 2021, 7, 215–221. [Google Scholar]
- Optimization of Protection in Pediatric Interventional Radiology in Latin America and the Caribbean (OPRIPALC). Available online: www.opripalc.org (accessed on 5 April 2023).
- Manterola, C.; Otzen, T. Checklist for reporting results using observational descriptive studies as research designs. The MInCir initiative. Int. J. Morphol. 2017, 35, 72–76. [Google Scholar] [CrossRef]
- Available online: https://www.pub.iaea.org/MTCD/Publications/PDF/TE-1958web.pdf (accessed on 10 April 2023).
- ICRU. Patient Dosimetry for X-rays Used in Medical Imaging ICRU Report 74; International Commission on Radiological Units and Measurements: Bethesda, MD, USA, 2005. [Google Scholar]
- IEC 60601-2-43:2010; Medical Electrical Equipment—Part 2-43: Particular Requirements for the Basic Safety and Essential Performance of X-ray Equipment for Interventional Procedures 60601-2-43 2nd ed. International Electrotechnical Commission: Geneva, Switzerland, 2010.
- Andrade, C. The P Value and Statistical Significance: Misunderstandings, Explanations, Challenges, and Alternatives. Indian J. Psychol. Med. 2019, 41, 210–215. [Google Scholar] [CrossRef] [PubMed]
- StataCorp. Stata Statistical Software: Release 16; StataCorp LLC.: College Station, TX, USA, 2019. [Google Scholar]
- Martinez, L.C.; Vano, E.; Gutierrez, F.; Rodriguez, C.; Gilarranz, R.; Manzanas, M.J. Patient doses from fluoroscopically guided cardiac procedures in pediatrics. Phys. Med. Biol. 2007, 52, 4749–4759. [Google Scholar] [CrossRef] [PubMed]
- Verghese, G.; McElhinney, D.B.; Strauss, K.J.; Bergersen, L. Characterization of radiation exposure and effect of a radiation monitoring policy in a large volume pediatric cardiac catheterization lab. Catheter. Cardiovasc. Interv. 2012, 79, 294–301. [Google Scholar] [CrossRef]
- Corredoira, E.; Vañó, E.; Ubeda, C.; Gutiérrez-Larraya, F. Patient doses in paediatric interventional cardiology: Impact of 3D rotational angiography. J. Radiol. Prot. 2015, 35, 179–195. [Google Scholar] [CrossRef]
- Kottou, S.; Kollaros, N.; Plemmenos, C.; Mastorakou, I.; Apostolopoulou, S.C.; Tsapaki, V. Towards the definition of Institutional diagnostic reference levels in paediatric interventional cardiology procedures in Greece. Phys. Med. 2018, 46, 52–58. [Google Scholar] [CrossRef]
- Ubeda, C.; Vano, E.; Riquelme, N.; Aguirre, D.; Vasquez, H.; Chavez, C.; Dalmazzo, D. Patient radiation doses in paediatric interventional cardiology and optimization actions. Radiat. Phys. Chem. 2020, 168, 108539. [Google Scholar] [CrossRef]
- Ishibashi, T.; Takei, Y.; Kato, M.; Yamashita, Y.; Tsukamoto, A.; Matsumoto, K.; Sakamoto, H.; Masuda, H.; Masuda, T.; Miyazaki, O. Pediatric diagnostic reference levels for diagnostic and therapeutic cardiac catheterization in Japan. Radiat. Prot. Dosim. 2023, 199, 1082–1089. [Google Scholar] [CrossRef]
- IAEA. Radiation Protection and Safety in Medical Uses of Ionizing Radiation; IAEA Safety Standards Series No. SSG-46; IAEA: Vienna, Austria, 2018.
- McFadden, S.; Hughes, C.; D’Helft, C.; McGee, A.; Rainford, L.; Brennan, P.; McCrum-Gardner, E.; Winder, R. The establishment of local diagnostic reference levels for paediatric interventional cardiology. Radiography 2013, 19, 295–301. [Google Scholar] [CrossRef]
- Barnaoui, S.; Rehel, J.L.; Baysson, H.; Boudjemline, Y.; Girodon, B.; Bernier, M.; Bonnet, D.; Aubert, B. Local reference levels and organ doses from paediatric cardiac interventional procedures. Pediatr. Cardiol. 2014, 35, 1037–1045. [Google Scholar] [CrossRef] [PubMed]
- Buytaert, D.; Vandekerckhove, K.; Panzer, J.; Rubbens, L.; De Wolf, D.; Bacher, K. Local DRLs and automated risk estimation in paediatric interventional cardiology. PLoS ONE 2019, 14, e0220359. [Google Scholar] [CrossRef] [PubMed]
- Hultenmo, M.; Nygren, A.; Söderberg, B.; Wåhlander, H. Dose evaluation and proposal of local diagnostic reference levels for paediatric cardiac catheterizations performed on a high-sensitivity angiographic system allowing low-dose imaging. Radiat. Prot. Dosim. 2021, 195, 279–288. [Google Scholar] [CrossRef] [PubMed]
- ICRP. Avoidance of radiation injuries from medical interventional procedures. Ann. ICRP 2000, 30, 7–67. [Google Scholar] [CrossRef]
- Steps for Radiation Safety in Pediatric Interventional Radiology. Available online: http://www.imagegently.org/Portals/6/Procedures/Steps%20for%20Radiation%20Safety%20in%20Pediatric%20Interventional%20Radiology.pdf?ver=FBueW4YF1I7F_V8nDrinbA%3d%3d (accessed on 2 August 2023).
- Andreassi, M.G. Radiation risk from pediatric cardiac catheterization: Friendly fire on children with congenital heart disease. Circulation 2009, 120, 1847–1849. [Google Scholar] [CrossRef]
- Sadick, V.; Reed, W.; Collins, L.; Sadick, N.; Heard, R.; Robinson, J. Impact of biplane versus single-plane imaging on radiation dose, contrast load and procedural time in coronary angioplasty. Br. J. Radiol. 2010, 83, 379–394. [Google Scholar] [CrossRef]
- Quinn, B.; Armstrong, A.; Bauser-Heaton, H.; Callahan, R.; El-Said, H.; Foerster, S.; Goldstein, B.; Goodman, A.; Gudausky, T.; Kreutzer, J. Congenital Cardiac Catheterization Project on Outcomes-Quality Improvement (C3PO-QI). Radiation Risk Categories in Cardiac Catheterization for Congenital Heart Disease: A Tool to Aid in the Evaluation of Radiation Outcomes. Pediatric. Cardiol. 2019, 40, 445–453. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Weight Band (kg) | N | Age in Years (yr) | Height (cm) | Weight (kg) |
|---|---|---|---|---|
| <5 | 43 | 0.63 | 50.37 | 3.33 |
| 5–<15 | 78 | 2.21 | 75.09 | 9.14 |
| 15–<30 | 59 | 6.05 | 112.40 | 20.01 |
| 30–<50 | 41 | 13.07 | 146.95 | 39.71 |
| 50–<80 | 34 | 17.72 | 161.13 | 57.99 |
| Weight Band (kg) | n | Pka (Gy·cm2) Median–3rd | Ka,r (mGy) Median–3rd | FT (min) Median–3rd |
|---|---|---|---|---|
| <5 | 43 | 1.69–3.82 | 37.00–86.88 | 13.27–19.73 |
| 5–<15 | 78 | 3.44–7.39 | 50.00–119.13 | 8.42–16.24 |
| 15–<30 | 41 | 8.87–19.72 | 95.80–211.0 | 7.00–18.01 |
| 30–<50 | 59 | 10.51–28.99 | 100.65–199.57 | 8.00–17.10 |
| 50–<80 | 34 | 22.61–81.71 | 171.00–491.35 | 12.05–21.58 |
| Age Band (yr) | n | Pka (Gy·cm2) Median–3rd | Ka,r (mGy) Median–3rd | FT (min) Median–3rd |
|---|---|---|---|---|
| <1 | 66 | 1.96–3.97 | 43.65–101.50 | 10.68–17.90 |
| 1–<5 | 68 | 4.67–9.94 | 73.30–133.65 | 8.37–15.36 |
| 5–<10 | 45 | 8.16–20.82 | 92.95–204.13 | 10.68–18.80 |
| 10–<16 | 46 | 14.76–58.00 | 124.30–319.20 | 11.41–23.77 |
| <16 | 30 | 17.52–31.56 | 103.80–205.35 | 8.29–14.27 |
| Age Group (years) | Martinez et al., 2007 [20] | Verghese et al., 2012 [21] | Ubeda et al., 2012 [9] | Corredoira et al., 2015 [22] | Kottou et al., 2018 [23] | Ubeda et al., 2020 [24] | Ishibashi et al., 2021 [25] | Ubeda et al., 2022 [10] | This Paper, 2023 |
|---|---|---|---|---|---|---|---|---|---|
| <1 | 1.9 | 4.6 | 0.9 | 1.8 | 2.0 | 2.1 | 4.3 | 1.9 | 1.8 |
| 1–<5 | 2.9 | 8.3 | 1.5 | 3.1 | 3.0 | 4.7 | 6.3 | 2.6 | 4.5 |
| 5–<10 | 4.5 | 11.5 | 2.1 | 6.0 | 7.0 | 6.3 | 10.9 | 3.6 | 7.5 |
| 10–<16 | 15.4 | 24.7 | 5.0 | 12.1 | 14.0 | 13.6 | 19.4 | 11.5 | 13.4 |
| Procedure Type | Procedure Name | Frequency | Pka (Gy·cm2) Median (1st–3rd) | FT (min) Median (1st–3rd) |
|---|---|---|---|---|
| Diagnostic | Non-complex | 61 | 2.0 (1.2–5.5) | 5.1 (3.5–9.4) |
| Complex | 37 | 4.5 (1.12–11.7) | 7.2 (5.2–14.4) | |
| Therapeutic | Atrial septal defect closure | 12 | 9.0 (3.7–10.8) | 6.7 (5.2–10.2) |
| Ventricular septal defect closure | 9 | 37.9 (6.1–74.2) | 30.3 (17.0–58.5) | |
| Patent ductus arteriosus closure | 51 | 7.3 (2.9–13.5) | 7.5 (5.4–11.9) | |
| Aortopulmonary collateral embolization | 22 | 8.6 (1.9–31.3) | 17.7 (10.2–26.8) | |
| Aortic coarctation angioplasty | 9 | 8.0 (0.7–25.4) | 12.8 (33.0–58.0) | |
| Aortic or pulmonary valvuloplasty | 33 | 9.7 (2.1–39.1) | 17.6 (9.5–26.4) | |
| Other | 21 | 3.9 (0.8–33.1) | 15.4 (11.3–30.6) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aristizabal, A.M.; Gutiérrez, J.A.; Ramirez, E.; Mejía-Quiñones, V.; Ubeda, C.; Mosquera, W.F.; Mosquera, W. Diagnostic Reference Levels in Interventional Pediatric Cardiology: Two-Year Experience in a Tertiary Referral Hospital in Latin America. Children 2023, 10, 1588. https://doi.org/10.3390/children10101588
Aristizabal AM, Gutiérrez JA, Ramirez E, Mejía-Quiñones V, Ubeda C, Mosquera WF, Mosquera W. Diagnostic Reference Levels in Interventional Pediatric Cardiology: Two-Year Experience in a Tertiary Referral Hospital in Latin America. Children. 2023; 10(10):1588. https://doi.org/10.3390/children10101588
Chicago/Turabian StyleAristizabal, Ana M., Jaiber A. Gutiérrez, Emmanuel Ramirez, Valentina Mejía-Quiñones, Carlos Ubeda, Walter Fernando Mosquera, and Walter Mosquera. 2023. "Diagnostic Reference Levels in Interventional Pediatric Cardiology: Two-Year Experience in a Tertiary Referral Hospital in Latin America" Children 10, no. 10: 1588. https://doi.org/10.3390/children10101588
APA StyleAristizabal, A. M., Gutiérrez, J. A., Ramirez, E., Mejía-Quiñones, V., Ubeda, C., Mosquera, W. F., & Mosquera, W. (2023). Diagnostic Reference Levels in Interventional Pediatric Cardiology: Two-Year Experience in a Tertiary Referral Hospital in Latin America. Children, 10(10), 1588. https://doi.org/10.3390/children10101588