
Adapting the Motivated Strategies for Learning Questionnaire to the Japanese Problem-Based Learning Context: A Validation Study


Abstract
1. Introduction
2. Materials and Methods
2.1. Design and Participants
2.2. Measurements
2.3. Context
2.4. The Theoretical Framework of Validation
2.5. Analysis
2.6. Ethics
3. Results
3.1. Factor Analysis
3.2. Internal Reliability of the Motivation Scale and Subscales
4. Discussion
4.1. Scoring Inference
4.2. Generalization Inference
4.3. Implication Inference
4.4. Extrapolation Inference
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hayashi, M.; Nishiya, K.; Kaneko, K. Transition from undergraduates to residents: A SWOT analysis of the expectations and concerns of Japanese medical graduates during the COVID-19 pandemic. PLoS ONE 2022, 17, e0266284. [Google Scholar] [CrossRef]
- Rose, S. Medical Student Education in the Time of COVID-19. JAMA 2020, 323, 2131–2132. [Google Scholar] [CrossRef]
- Jumreornvong, O.; Yang, E.; Race, J.; Appel, J. Telemedicine and Medical Education in the Age of COVID-19. Acad. Med. 2020, 95, 1838–1843. [Google Scholar] [CrossRef] [PubMed]
- Lajoie, S.P.; Gube, M. Adaptive expertise in medical education: Accelerating learning trajectories by fostering self-regulated learning. Med. Teach. 2018, 40, 809–812. [Google Scholar] [CrossRef]
- Zheng, J.; Li, S.; Lajoie, S.P. The Role of Achievement Goals and Self-regulated Learning Behaviors in Clinical Reasoning. Technol. Knowl. Learn. 2020, 25, 541–556. [Google Scholar] [CrossRef]
- Lajoie, S.P.; Zheng, J.; Li, S.; Jarrell, A.; Gube, M. Examining the interplay of affect and self regulation in the context of clinical reasoning. Learn. Instr. 2021, 72, 101219. [Google Scholar] [CrossRef]
- Azevedo, R.; Bouchet, F.; Duffy, M.; Harley, J.; Taub, M.; Trevors, G.; Cloude, E.; Dever, D.; Wiedbusch, M.; Wortha, F.; et al. Lessons Learned and Future Directions of MetaTutor: Leveraging Multichannel Data to Scaffold Self-Regulated Learning with an Intelligent Tutoring System. Front. Psychol. 2022, 13, 813632. [Google Scholar] [CrossRef]
- Zimmerman, B.J. Self-Regulated Learning and Academic Achievement: An Overview. Educ. Psychol. 1990, 25, 3–17. [Google Scholar] [CrossRef]
- Artino, A.R., Jr.; Jones, K.D. AM last page: Self-regulated learning—A dynamic, cyclical perspective. Acad. Med. 2013, 88, 1048. [Google Scholar] [CrossRef]
- Cook, D.A.; Thompson, W.G.; Thomas, K.G. The Motivated Strategies for Learning Questionnaire: Score validity among medicine residents. Med. Educ. 2011, 45, 1230–1240. [Google Scholar] [CrossRef]
- Cho, K.K.; Marjadi, B.; Langendyk, V.; Hu, W. Medical student changes in self-regulated learning during the transition to the clinical environment. BMC Med. Educ. 2017, 17, 59. [Google Scholar] [CrossRef]
- Pintrich, P.R.; Smith, D.A.F.; Duncan, T.; Mckeachie, W.J. A Manual for the Use of the Motivated Strategies for Learning Questionnaire (MSLQ). 1991. Available online: https://www.researchgate.net/publication/271429287_A_Manual_for_the_Use_of_the_Motivated_Strategies_for_Learning_Questionnaire_MSLQ (accessed on 1 December 2022). [CrossRef]
- Matsuyama, Y.; Nakaya, M.; Leppink, J.; van der Vleuten, C.; Asada, Y.; Lebowitz, A.J.; Sasahara, T.; Yamamoto, Y.; Matsumura, M.; Gomi, A.; et al. Limited effects from professional identity formation-oriented intervention on self-regulated learning in a preclinical setting: A randomized-controlled study in Japan. BMC Med. Educ. 2021, 21, 30. [Google Scholar] [CrossRef]
- Kane, M.T. Validating the Interpretations and Uses of Test Scores. J. Educ. Meas. 2013, 50, 1–73. [Google Scholar] [CrossRef]
- Cook, D.A.; Brydges, R.; Ginsburg, S.; Hatala, R. A contemporary approach to validity arguments: A practical guide to K ane’s framework. Med. Educ. 2015, 49, 560–575. [Google Scholar] [CrossRef]
- Nomura, O.; Itoh, T.; Mori, T.; Ihara, T.; Tsuji, S.; Inoue, N.; Carrière, B. Creating Clinical Reasoning Assessment Tools in Different Languages: Adaptation of the Pediatric Emergency Medicine Script Concordance Test to Japanese. Front. Med. 2021, 8, 765489. [Google Scholar] [CrossRef]
- Soemantri, D.; McColl, G.; Dodds, A. Measuring medical students’ reflection on their learning: Modification and validation of the motivated strategies for learning questionnaire (MSLQ). BMC Med. Educ. 2018, 18, 274. [Google Scholar] [CrossRef]
- Nomura, O.; Wiseman, J.; Sunohara, M.; Akatsu, H.; Lajoie, S.P. Japanese medical learners’ achievement emotions: Accounting for culture in translating Western medical educational theories and instruments into an asian context. Adv. Health Sci. Educ. Theory Pract. 2021, 26, 1255–1276. [Google Scholar] [CrossRef] [PubMed]
- Miyabe, A.; Togashi, C.; Sakuma, K.; Sato, C. Reliability and validity of a Japanese version of the Motivated Strategies for Learning Questionnaire for motivation scales. J. Jpn. Health Med. Assoc. 2016, 25, 276–286. [Google Scholar]
- Onishi, H.; Yoshida, I. Rapid change in Japanese medical education. Med. Teach. 2004, 26, 403–408. [Google Scholar] [CrossRef]
- Saiki, T.; Imafuku, R.; Suzuki, Y.; Ban, N. The truth lies somewhere in the middle: Swinging between globalization and regionalization of medical education in Japan. Med. Teach. 2017, 39, 1016–1022. [Google Scholar] [CrossRef]
- Niwa, M.; Saiki, T.; Fujisaki, K.; Suzuki, Y.; Evans, P. The Effects of Problem-Based-Learning on the Academic Achievements of Medical Students in One Japanese Medical School, Over a Twenty-Year Period. Health Prof. Educ. 2016, 2, 3–9. [Google Scholar] [CrossRef]
- Nakao, H.; Nomura, O.; Kubota, M.; Ishiguro, A. Long-term impact of overnight shiftwork implementation on pediatric residents’ mental wellness: A repeated cross-sectional survey. J. Occup. Health 2022, 64, 12349. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| No. | Items | Mean | SD | Median | 25th–75th Percentile |
|---|---|---|---|---|---|
| Q1 | In a class like this, I prefer course material that really challenges me so I can learn new things. | 3.393 | 1.618 | 3 | 2–4.25 |
| Q2 | If I study in appropriate ways, then I will be able to learn the material in the medical course. | 5.134 | 1.319 | 5 | 4–6 |
| Q3 | When I take a test, I think about how poorly I am doing compared to other students. | 4.330 | 1.862 | 4.5 | 3–6 |
| Q4 | I think I will be able to use what I learn in the medical course in other courses. | 5.089 | 1.545 | 5 | 4–6 |
| Q5 | I believe I will receive an excellent grade in this class. | 2.991 | 1.580 | 3 | 2–4 |
| Q6 | I’m certain I can understand the most difficult material presented in the readings for the medical course. | 2.732 | 1.530 | 2 | 2–3 |
| Q7 | Getting a good grade in this class is the most satisfying thing for me right now. | 3.161 | 1.669 | 3 | 2–4 |
| Q8 | When I take a test, I think about items on other parts of the test I can’t answer. | 4.179 | 1.715 | 5 | 3–5 |
| Q9 | It is my own fault if I don’t learn the material in the medical course. | 4.277 | 1.623 | 4 | 3–5 |
| Q10 | It is important for me to learn the course material in the medical class. | 4.714 | 1.290 | 5 | 4–5.25 |
| Q11 | The most important thing for me right now is improving my overall grade point average, so my main concern in this class is getting a good grade. | 3.482 | 1.524 | 3 | 2–4.25 |
| Q12 | I’m confident I can learn the basic concepts taught in the medical course. | 4.036 | 1.445 | 4 | 3–5 |
| Q13 | If I can, I want to get better grades in this class than most of the other students. | 4.304 | 1.898 | 4 | 3–6 |
| Q14 | When I take tests, I think of the consequences of failing. | 3.491 | 1.959 | 3 | 2–5 |
| Q15 | I’m confident I can understand the most complex material presented by the instructor in this course. | 2.661 | 1.516 | 2 | 1.75–4 |
| Q16 | In a class like this, I prefer course material that arouses my curiosity, even if it is difficult to learn. | 4.545 | 1.638 | 5 | 3–6 |
| Q17 | I am very interested in the content area of the medical course. | 5.071 | 1.400 | 5 | 4–6 |
| Q18 | If I try hard enough, then I will understand the course material. | 4.991 | 1.424 | 5 | 4–6 |
| Q19 | I have an uneasy upset feeling when I take an exam. | 3.786 | 1.747 | 3.5 | 3–5 |
| Q20 | I’m confident I can do an excellent job on the assignments and tests in the medical course. | 3.054 | 1.512 | 3 | 2–4 |
| Q21 | I expect to do well in this course. | 3.188 | 1.685 | 3 | 2–4 |
| Q22 | The most satisfying thing for me in the medical course is trying to understand the content as thoroughly as possible. | 3.982 | 1.483 | 4 | 3–5 |
| Q23 | I think the material for the PBL course is useful for me to learn. | 5.420 | 1.235 | 6 | 5–6 |
| Q24 | When I have the opportunity in this class, I choose course assignments that I can learn from, even if they don’t guarantee a good grade. | 3.804 | 1.734 | 4 | 2–5 |
| Q25 | If I don’t understand the course material, it is because I didn’t try hard enough. | 4.000 | 1.458 | 4 | 3–5 |
| Q26 | I like the subject matter of the medical course. | 4.607 | 1.311 | 5 | 4–6 |
| Q27 | Understanding the subject matter of the medical course is very important to me. | 4.920 | 1.246 | 5 | 4–6 |
| Q28 | I feel my heart beating fast when I take an exam. | 3.911 | 1.920 | 4 | 2–5.25 |
| Q29 | I’m certain I can master the skills being taught in this class. | 3.411 | 1.480 | 3 | 2–4 |
| Q30 | I want to do well in this class because it is important to show my ability to my family, friends, employer, or others. | 3.089 | 1.696 | 3 | 2–4 |
| Q31 | Considering the difficulty of the medical course, the teacher, and my skills, I think I will do well in this course. | 2.893 | 1.538 | 3 | 2–4 |
| No. | Items | Mean | SD | Median | 25th–75th Percentile |
|---|---|---|---|---|---|
| Q32 | When I study the readings for the medical course, I outline the material to help me organize my thoughts. | 4.009 | 1.690 | 4 | 3–5 |
| Q33 | During class time, I often miss important points because I’m thinking of other things. | 3.366 | 1.483 | 3 | 2–4 |
| Q34 | When studying for the medical course, I often try to explain the material to a classmate or friend. | 3.759 | 1.607 | 4 | 2–5 |
| Q35 | I usually study in a place where I can concentrate on my course work. | 4.821 | 1.584 | 5 | 4–6 |
| Q36 | When reading for the medical course, I make up questions to help focus my reading. | 3.188 | 1.492 | 3 | 2–4 |
| Q37 | I often feel so lazy or bored when I study for this PBL course that I quit before I finish what I planned to do. | 4.518 | 1.548 | 5 | 4–6 |
| Q38 | I often find myself questioning things I hear or read in the medical course to decide if I find them convincing. | 4.179 | 1.472 | 4 | 3–5 |
| Q39 | When I study for this PBL course, I practice saying the material to myself over and over. | 2.955 | 1.491 | 3 | 2–4 |
| Q40 | Even if I have trouble learning the material in this class, I try to do the work on my own, without help from anyone. | 4.902 | 1.682 | 5 | 4–6 |
| Q41 | When I become confused about something I’m reading for this PBL course, I go back and try to figure it out. | 4.679 | 1.543 | 5 | 4–6 |
| Q42 | When I study for the medical course, I go through the readings and my class notes and try to find the most important ideas. | 4.518 | 1.513 | 5 | 4–6 |
| Q43 | I make good use of my study time for the medical course. | 4.304 | 1.476 | 4 | 3–5 |
| Q44 | If the medical course readings are difficult to understand, I change the way I read the material. | 4.509 | 1.427 | 5 | 4–5 |
| Q45 | I try to work with other students from this PBL course to complete the course assignments. | 5.259 | 1.457 | 6 | 4–6 |
| Q46 | When studying for the medical course, I read my class notes and the course readings over and over again. | 4.750 | 1.574 | 5 | 4–6 |
| Q47 | When a theory, interpretation, or conclusion is presented in class or in the readings, I try to decide if there is good supporting evidence. | 4.089 | 1.534 | 4 | 3–5 |
| Q48 | I work hard to do well in this PBL course, even if I don’t like what we are doing. | 4.813 | 1.353 | 5 | 4–6 |
| Q49 | I make simple charts, diagrams, or tables to help me organize the course material. | 3.821 | 1.667 | 4 | 2.75–5 |
| Q50 | When studying for the medical course, I often set aside time to discuss the course material with a group of students from the class. | 4.580 | 1.493 | 5 | 4–6 |
| Q51 | I treat the course material as a starting point and try to develop my own ideas about it. | 4.196 | 1.334 | 4 | 3–5 |
| Q52 | I find it hard to stick to a study schedule. | 3.366 | 1.577 | 3 | 2–5 |
| Q53 | When I study for this PBL course, I pull together information from different sources, such as lectures, readings, and discussions. | 4.643 | 1.328 | 5 | 4–6 |
| Q54 | Before I study new course material thoroughly, I often skim it to see how it is organized. | 4.402 | 1.557 | 5 | 3–5.25 |
| Q55 | I ask myself questions to make sure I understand the material I have been studying in this PBL course. | 4.054 | 1.426 | 4 | 3–5 |
| Q56 | I try to change the way I study in order to fit the course requirements and the instructor’s teaching style. | 4.259 | 1.354 | 4 | 3–5 |
| Q57 | I often find that I have been reading for this PBL course but don’t know what it was all about. | 3.929 | 1.609 | 4 | 3–5 |
| Q58 | I ask the instructor to clarify concepts I don’t understand well. | 3.295 | 1.540 | 3 | 2–4 |
| Q59 | I memorize key words to remind me of important concepts in this class. | 4.438 | 1.406 | 5 | 3–5 |
| Q60 | When course work is difficult, I either give up or only study the easy parts. | 3.830 | 1.542 | 4 | 3–5 |
| Q61 | I try to think through a topic and decide what I am supposed to learn from it rather than just reading it over when studying for the medical course. | 3.964 | 1.506 | 4 | 3–5 |
| Q62 | I try to relate ideas in this subject to those in other courses whenever possible. | 4.777 | 1.380 | 5 | 4–6 |
| Q63 | When I study for medical course, I go over my class notes and make an outline of important concepts. | 4.188 | 1.630 | 4 | 3–5.25 |
| Q64 | When reading for this this PBL course, I try to relate the material to what I already know. | 4.964 | 1.420 | 5 | 4–6 |
| Q65 | I have a regular place set aside for studying. | 4.679 | 1.731 | 5 | 3–6 |
| Q66 | I try to play around with ideas of my own related to what I am learning in the medical course. | 4.384 | 1.377 | 4 | 3–5 |
| Q67 | When I study for the medical course, I write brief summaries of the main ideas from the readings and my class notes. | 3.920 | 1.730 | 4 | 3–5 |
| Q68 | When I can’t understand the material in the medical course, I ask another student in this class for help. | 5.482 | 1.315 | 6 | 5–6.25 |
| Q69 | I try to understand the material in this PBL course by making connections between the readings and the concepts from the lectures. | 5.089 | 1.305 | 5 | 5–6 |
| Q70 | I make sure that I keep up with the weekly readings and assignments for the medical course. | 3.696 | 1.547 | 4 | 3–5 |
| Q71 | Whenever I read or hear an assertion or conclusion in this class, I think about possible alternatives. | 3.866 | 1.417 | 4 | 3–5 |
| Q72 | I make lists of important items for the medical course and memorize the lists. | 3.304 | 1.765 | 3 | 2–5 |
| Q73 | I attend this class regularly. | 4.536 | 1.869 | 5 | 3–6 |
| Q74 | Even when the course materials are dull and uninteresting, I manage to keep working until I finish. | 4.402 | 1.479 | 5 | 3–5 |
| Q75 | I try to identify students in this class to ask for help if necessary. | 4.384 | 1.767 | 5 | 3–6 |
| Q76 | When studying for the medical course, I try to determine which concepts I don’t understand well. | 4.625 | 1.396 | 5 | 4–5 |
| Q77 | I often find that I don’t spend very much time on the medical course because of other activities. | 3.384 | 1.590 | 3 | 2–4 |
| Q78 | When I study for this PBL course, I set goals for myself in order to direct my activities in each study period. | 3.875 | 1.440 | 4 | 3–5 |
| Q79 | If I get confused taking notes in class, I make sure I sort it out afterward. | 3.732 | 1.644 | 4 | 2.75–5 |
| Q80 | I rarely find time to review my notes or readings before an exam. | 4.786 | 1.608 | 5 | 4–6 |
| Q81 | I try to apply ideas from the course readings in other class activities such as lectures and discussions. | 4.545 | 1.451 | 5 | 4–5 |
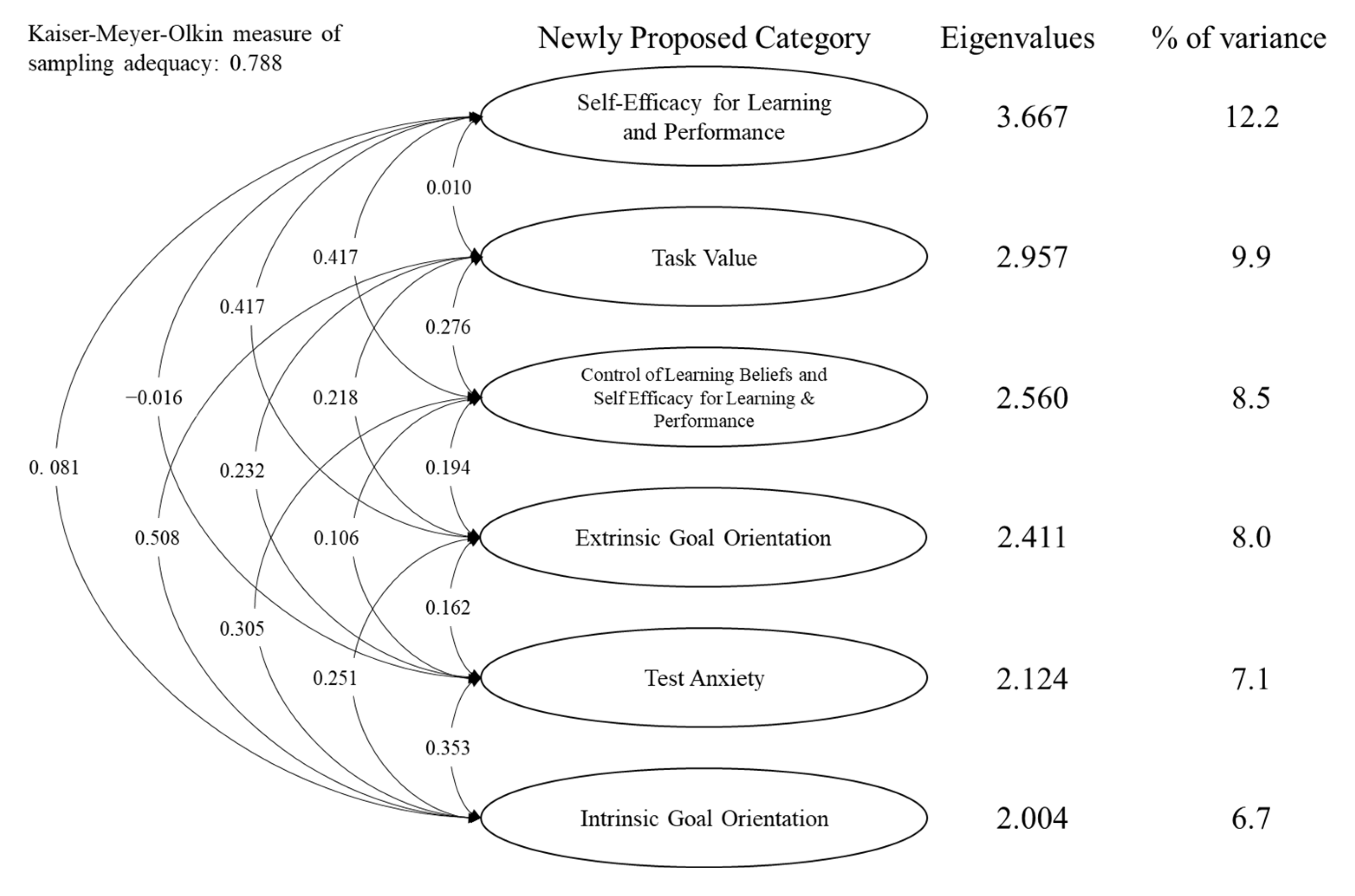
| No. | Self-Efficacy for Learning and Performance | Task Value | Control of Learning Beliefs and Self-Efficacy for Learning and Performance | Extrinsic Goal Orientation | Test Anxiety | Intrinsic Goal Orientation |
|---|---|---|---|---|---|---|
| Cronbach’s α | 0.875 | |||||
| Q15 | 0.908 | 0.075 | –0.113 | 0.001 | –0.013 | 0.147 |
| Q6 | 0.873 | 0.101 | –0.080 | –0.078 | 0.090 | 0.066 |
| Q31 | 0.679 | –0.011 | 0.131 | 0.185 | 0.106 | –0.096 |
| Q20 | 0.620 | 0.146 | 0.246 | 0.006 | –0.081 | –0.159 |
| Q12 | 0.395 | 0.150 | 0.183 | –0.032 | –0.015 | 0.173 |
| Cronbach’s α | 0.805 | |||||
| Q17 | 0.051 | 0.827 | 0.069 | 0.048 | –0.177 | –0.091 |
| Q26 | 0.273 | 0.817 | –0.078 | –0.029 | –0.074 | –0.007 |
| Q27 | 0.209 | 0.716 | –0.052 | –0.020 | 0.210 | –0.025 |
| Q23 | –0.263 | 0.513 | 0.142 | 0.021 | 0.009 | 0.133 |
| Q9 | –0.129 | 0.240 | –0.091 | 0.101 | 0.239 | 0.159 |
| Cronbach’s α | 0.800 | |||||
| Q21 | 0.221 | –0.073 | 0.729 | 0.253 | –0.036 | –0.313 |
| Q5 | 0.344 | –0.298 | 0.610 | 0.151 | –0.031 | 0.069 |
| Q18 | –0.042 | 0.260 | 0.570 | –0.050 | –0.025 | 0.136 |
| Q29 | 0.313 | –0.046 | 0.511 | 0.075 | 0.002 | –0.039 |
| Q2 | 0.053 | 0.096 | 0.436 | –0.104 | 0.197 | 0.104 |
| Q4 | –0.068 | 0.251 | 0.317 | –0.225 | 0.102 | 0.160 |
| Cronbach’s α | 0.792 | |||||
| Q7 | 0.117 | –0.165 | 0.084 | 0.730 | –0.053 | 0.170 |
| Q13 | –0.074 | 0.298 | 0.180 | 0.653 | –0.007 | –0.246 |
| Q30 | –0.003 | –0.285 | 0.181 | 0.621 | 0.138 | 0.158 |
| Q11 | 0.103 | 0.148 | –0.315 | 0.599 | 0.165 | 0.084 |
| Q22 | 0.083 | 0.258 | –0.099 | 0.426 | –0.048 | 0.256 |
| Cronbach’s α | 0.720 | |||||
| Q19 | 0.126 | 0.038 | 0.025 | 0.022 | 0.873 | –0.261 |
| Q28 | –0.095 | 0.130 | 0.098 | 0.150 | 0.844 | –0.344 |
| Q8 | 0.212 | –0.059 | 0.081 | –0.034 | 0.480 | 0.107 |
| Q14 | –0.122 | –0.194 | –0.042 | 0.017 | 0.452 | 0.194 |
| Cronbach’s α | 0.638 | |||||
| Q1 | 0.307 | –0.064 | 0.035 | 0.006 | –0.128 | 0.621 |
| Q25 | –0.037 | –0.001 | –0.114 | 0.037 | –0.105 | 0.595 |
| Q24 | 0.044 | –0.041 | 0.113 | –0.034 | 0.089 | 0.523 |
| Q10 | –0.158 | 0.179 | 0.024 | 0.209 | –0.060 | 0.455 |
| Q16 | –0.018 | 0.197 | 0.270 | 0.075 | –0.159 | 0.393 |
| Eigenvalues | 3.667 | 2.957 | 2.560 | 2.411 | 2.124 | 2.004 |
| Percentage of total variance | 0.122 | 0.099 | 0.085 | 0.080 | 0.071 | 0.067 |
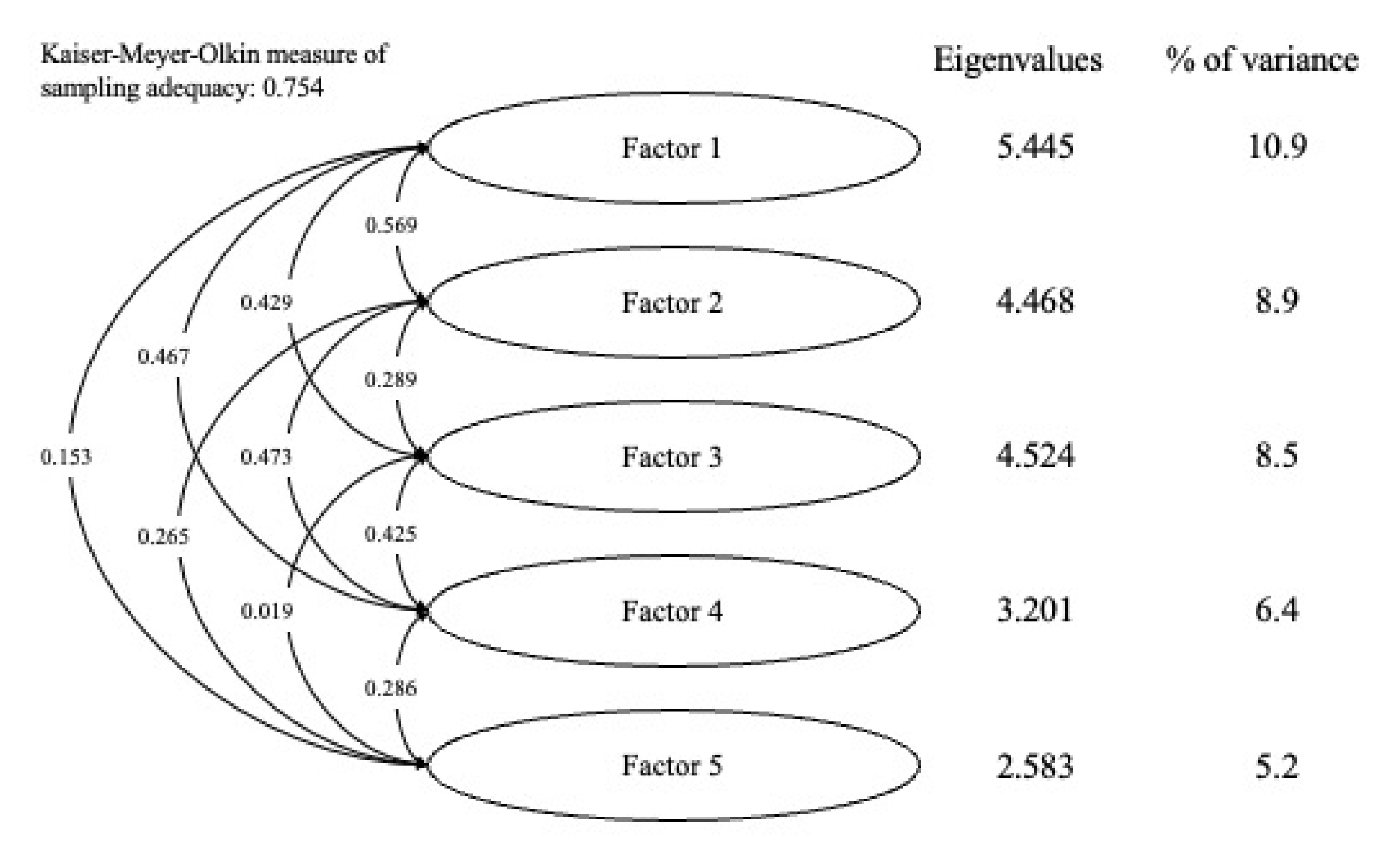
| No. | Factor 1 | Factor 2 | Factor 3 | Factor 4 | Factor 5 |
|---|---|---|---|---|---|
| Cronbach’s α | 0.805 | ||||
| Q42 | 0.715 | –0.101 | –0.128 | 0.167 | –0.144 |
| Q74 | 0.684 | –0.148 | –0.017 | 0.043 | –0.034 |
| Q73 | 0.674 | –0.298 | 0.156 | –0.177 | 0.074 |
| Q48 | 0.654 | 0.093 | 0.011 | –0.238 | 0.014 |
| Q76 | 0.620 | 0.105 | –0.051 | –0.117 | –0.039 |
| Q41 | 0.574 | 0.190 | –0.195 | 0.022 | –0.134 |
| Q67 | 0.565 | –0.275 | 0.209 | 0.108 | 0.306 |
| Q51 | 0.548 | 0.057 | 0.098 | 0.065 | –0.174 |
| Q59 | 0.526 | 0.264 | –0.072 | –0.088 | –0.120 |
| Q52 | –0.482 | 0.009 | –0.135 | 0.475 | 0.399 |
| Q32 | 0.441 | –0.055 | –0.093 | 0.315 | 0.125 |
| Q81 | 0.400 | 0.146 | 0.002 | 0.177 | 0.023 |
| Q35 | 0.392 | 0.094 | –0.328 | 0.359 | –0.048 |
| Q62 | 0.365 | 0.183 | 0.137 | 0.135 | 0.038 |
| Q47 | 0.295 | 0.090 | 0.213 | 0.081 | –0.138 |
| Cronbach’s α | 0.824 | ||||
| Q45 | –0.196 | 0.963 | –0.109 | –0.153 | –0.266 |
| Q68 | 0.046 | 0.835 | 0.034 | –0.290 | –0.030 |
| Q50 | –0.192 | 0.650 | 0.284 | 0.182 | –0.220 |
| Q46 | 0.122 | 0.462 | 0.021 | 0.145 | 0.056 |
| Q64 | 0.219 | 0.442 | –0.013 | 0.160 | 0.014 |
| Q44 | 0.121 | 0.423 | 0.099 | 0.026 | –0.067 |
| Q43 | 0.027 | 0.409 | 0.189 | 0.187 | 0.022 |
| Q69 | 0.348 | 0.372 | 0.097 | 0.028 | 0.086 |
| Q66 | 0.080 | 0.310 | 0.208 | 0.209 | 0.020 |
| Cronbach’s α | 0.650 | ||||
| Q78 | –0.049 | 0.015 | 0.683 | –0.097 | 0.144 |
| Q57 | –0.101 | 0.028 | –0.603 | 0.379 | 0.260 |
| Q72 | –0.201 | –0.088 | 0.589 | 0.330 | 0.161 |
| Q55 | –0.034 | 0.223 | 0.573 | 0.071 | –0.120 |
| Q58 | –0.070 | –0.031 | 0.559 | 0.042 | –0.199 |
| Q71 | –0.118 | 0.302 | 0.466 | –0.029 | –0.019 |
| Q79 | 0.122 | −0.023 | 0.453 | 0.211 | 0.391 |
| Q75 | 0.105 | 0.288 | 0.446 | –0.231 | 0.056 |
| Q39 | 0.161 | –0.198 | 0.399 | 0.203 | –0.272 |
| Q53 | 0.201 | 0.083 | 0.383 | 0.005 | 0.080 |
| Q54 | 0.163 | 0.093 | 0.324 | 0.063 | 0.112 |
| Cronbach’s α | 0.496 | ||||
| Q36 | –0.022 | –0.291 | 0.084 | 0.845 | –0.337 |
| Q61 | 0.204 | 0.170 | –0.083 | 0.459 | –0.309 |
| Q70 | –0.031 | –0.023 | 0.216 | 0.446 | 0.054 |
| Q34 | –0.138 | 0.301 | 0.228 | 0.324 | –0.010 |
| Q56 | 0.086 | 0.225 | 0.197 | 0.293 | 0.002 |
| Q38 | 0.080 | 0.108 | 0.155 | 0.281 | 0.045 |
| Q65 | 0.120 | 0.167 | –0.028 | 0.266 | 0.034 |
| Cronbach’s α | 0.685 | ||||
| Q37 | –0.060 | 0.178 | –0.087 | –0.227 | 0.661 |
| Q77 | –0.096 | –0.137 | 0.074 | –0.219 | 0.624 |
| Q33 | 0.228 | –0.313 | –0.115 | 0.059 | 0.559 |
| Q60 | –0.158 | –0.175 | 0.146 | 0.037 | 0.488 |
| Q63 | 0.223 | 0.165 | 0.255 | 0.062 | 0.366 |
| Q80 | 0.090 | 0.300 | –0.283 | –0.111 | 0.318 |
| Eigenvalues | 5.445 | 4.468 | 4.254 | 3.201 | 2.583 |
| Percentage of total variance | 0.109 | 0.089 | 0.085 | 0.064 | 0.052 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nomura, O.; Soma, Y.; Kijima, H.; Matsuyama, Y. Adapting the Motivated Strategies for Learning Questionnaire to the Japanese Problem-Based Learning Context: A Validation Study. Children 2023, 10, 154. https://doi.org/10.3390/children10010154
Nomura O, Soma Y, Kijima H, Matsuyama Y. Adapting the Motivated Strategies for Learning Questionnaire to the Japanese Problem-Based Learning Context: A Validation Study. Children. 2023; 10(1):154. https://doi.org/10.3390/children10010154
Chicago/Turabian StyleNomura, Osamu, Yuki Soma, Hiroshi Kijima, and Yasushi Matsuyama. 2023. "Adapting the Motivated Strategies for Learning Questionnaire to the Japanese Problem-Based Learning Context: A Validation Study" Children 10, no. 1: 154. https://doi.org/10.3390/children10010154
APA StyleNomura, O., Soma, Y., Kijima, H., & Matsuyama, Y. (2023). Adapting the Motivated Strategies for Learning Questionnaire to the Japanese Problem-Based Learning Context: A Validation Study. Children, 10(1), 154. https://doi.org/10.3390/children10010154