
Oral Antibiotic Prophylaxis Reduces Surgical Site Infection and Anastomotic Leakage in Patients Undergoing Colorectal Cancer Surgery

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
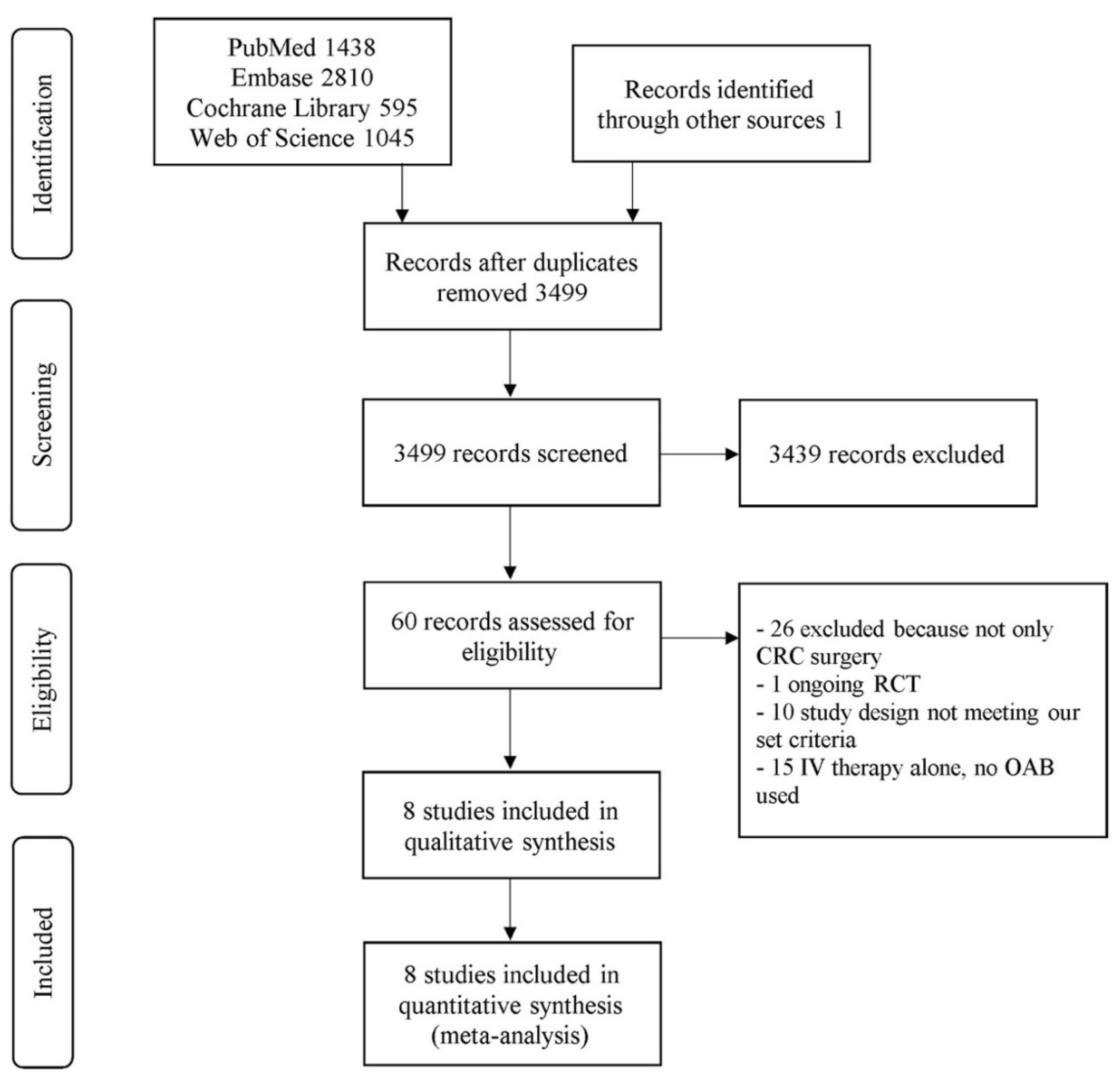
2.1. Search Strategy
2.2. Selection of Articles
2.3. Endpoints
2.4. Antibiotic Definitions
2.5. Data Extraction and Management
2.6. Statistical Analysis
3. Results
3.1. Quality Assessment and Patient Demographics
3.1.1. Antibiotic Regimes
3.1.2. MBP
3.1.3. Type of Surgery
3.2. Primary Outcome: Anastomotic Leakage and Surgical Site Infection
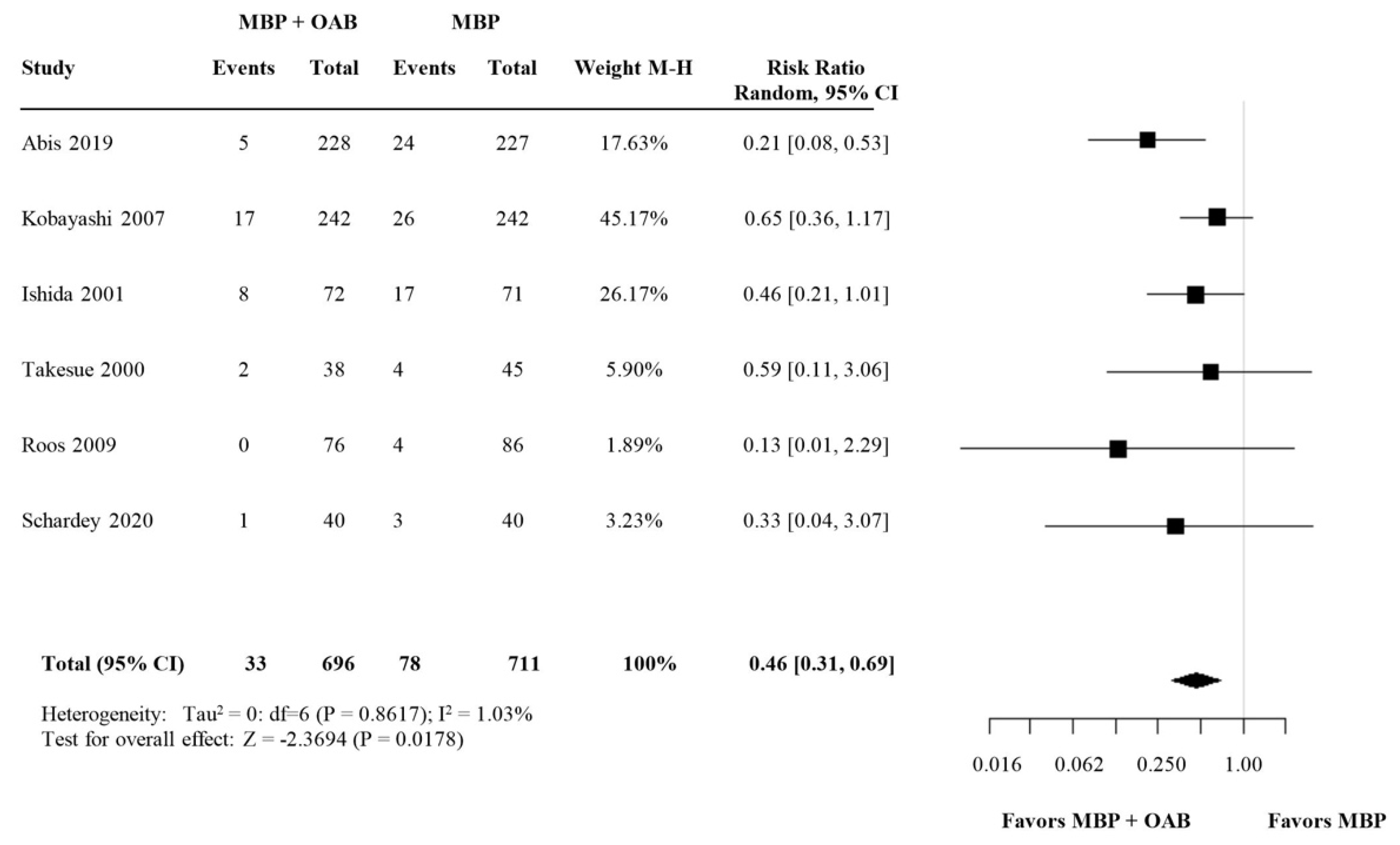
3.2.1. Anastomotic Leakage (AL)
3.2.2. Surgical Site Infection (SSI)
3.2.3. Subgroup Analysis: SDD versus Broad-Spectrum OABs
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Gessler, B.; Eriksson, O.; Angenete, E. Diagnosis, treatment, and consequences of anastomotic leakage in colorectal surgery. Int. J. Colorectal Dis. 2017, 32, 549–556. [Google Scholar] [CrossRef] [Green Version]
- Koedam, T.W.A.; Bootsma, B.T.; Deijen, C.L.; van de Brug, T.; Kazemier, G.; Cuesta, M.A.; Fürst, A.; Lacy, A.M.; Haglind, E.; Tuynman, J.B.; et al. Oncological Outcomes after Anastomotic Leakage after Surgery for Colon or Rectal Cancer: Increased Risk of Local Recurrence. Ann. Surg. 2020, 3. [Google Scholar] [CrossRef]
- Bakker, I.S.; Grossmann, I.; Henneman, D.; Havenga, K.; Wiggers, T. Risk factors for anastomotic leakage and leak-related mortality after colonic cancer surgery in a nationwide audit. Br. J. Surg. 2014, 101, 424–432. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.-W.; Lian, P.; Huang, B.; Zheng, H.-T.; Wang, M.-H.; Gu, W.-L.; Li, X.-X.; Xu, Y.; Cai, S.-J. Very Early Colorectal Anastomotic Leakage within 5 Post-operative Days: A More Severe Subtype Needs Relaparatomy. Sci. Rep. 2017, 7, 39936. [Google Scholar] [CrossRef] [Green Version]
- Wenzel, R.P. Surgical site infections and the microbiome: An updated perspective. Infect. Control Hosp. Epidemiol. 2019, 40, 590–596. [Google Scholar] [CrossRef]
- Bachmann, R.; Leonard, D.; Delzenne, N.; Kartheuser, A.; Cani, P.D. Novel insight into the role of microbiota in colorectal surgery. Gut 2017, 66, 738–749. [Google Scholar] [CrossRef]
- Allaband, C.; McDonald, D.; Vázquez-Baeza, Y.; Minich, J.J.; Tripathi, A.; Brenner, D.A.; Loomba, R.; Smarr, L.; Sandborn, W.J.; Schnabl, B.; et al. Microbiome 101: Studying, Analyzing, and Interpreting Gut Microbiome Data for Clinicians. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2019, 17, 218–230. [Google Scholar] [CrossRef]
- Thursby, E.; Juge, N. Introduction to the human gut microbiota. Biochem. J. 2017, 474, 1823–1836. [Google Scholar] [CrossRef]
- de Smet, A.M.; Kluytmans, J.A.; Cooper, B.S.; Mascini, E.M.; Benus, R.F.; van der Werf, T.S.; van der Hoeven, J.G.; Pickkers, P.; Bogaers-Hofman, D.; van der Meer, N.J.; et al. Decontamination of the digestive tract and oropharynx in ICU patients. N. Engl. J. Med. 2009, 360, 20–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liberati, A.; D’Amico, R.; Pifferi, S.; Torri, V.; Brazzi, L.; Parmelli, E. Antibiotic prophylaxis to reduce respiratory tract infections and mortality in adults receiving intensive care. Cochrane Database Syst. Rev. 2009, Cd000022. [Google Scholar] [CrossRef] [Green Version]
- Ohigashi, S.; Sudo, K.; Kobayashi, D.; Takahashi, T.; Nomoto, K.; Onodera, H. Significant changes in the intestinal environment after surgery in patients with colorectal cancer. J. Gastrointest. Surg. Off. J. Soc. Surg. Aliment. Tract 2013, 17, 1657–1664. [Google Scholar] [CrossRef]
- Zoetendal, E.G.; Rajilic-Stojanovic, M.; de Vos, W.M. High-throughput diversity and functionality analysis of the gastrointestinal tract microbiota. Gut 2008, 57, 1605–1615. [Google Scholar] [CrossRef] [PubMed]
- Guyton, K.; Alverdy, J.C. The gut microbiota and gastrointestinal surgery. Nat. Rev. Gastroenterol. Hepatol. 2017, 14, 43–54. [Google Scholar] [CrossRef]
- Bucher, P.; Gervaz, P.; Egger, J.F.; Soravia, C.; Morel, P. Morphologic alterations associated with mechanical bowel preparation before elective colorectal surgery: A randomized trial. Dis. Colon Rectum. 2006, 49, 109–112. [Google Scholar] [CrossRef] [PubMed]
- Shobar, R.M.; Velineni, S.; Keshavarzian, A.; Swanson, G.; DeMeo, M.T.; Melson, J.E.; Losurdo, J.; Engen, P.A.; Sun, Y.; Koenig, L.; et al. The Effects of Bowel Preparation on Microbiota-Related Metrics Differ in Health and in Inflammatory Bowel Disease and for the Mucosal and Luminal Microbiota Compartments. Clin. Transl. Gastroenterol. 2016, 7, e143. [Google Scholar] [CrossRef]
- Abis, G.S.A.; Stockmann, H.; Bonjer, H.J.; van Veenendaal, N.; van Doorn-Schepens, M.L.M.; Budding, A.E.; Wilschut, J.A.; van Egmond, M.; Oosterling, S.J.; SELECT Trial Study Group. Randomized clinical trial of selective decontamination of the digestive tract in elective colorectal cancer surgery (SELECT trial). Br. J. Surg. 2019, 106, 355–363. [Google Scholar] [CrossRef]
- Cong, J.; Zhu, H.; Liu, D.; Li, T.; Zhang, C.; Zhu, J.; Lv, H.; Liu, K.; Hao, C.; Tian, Z.; et al. A Pilot Study: Changes of Gut Microbiota in Post-surgery Colorectal Cancer Patients. Front. Microbiol. 2018, 9, 2777. [Google Scholar] [CrossRef]
- Nelson, R.L.; Gladman, E.; Barbateskovic, M. Antimicrobial prophylaxis for colorectal surgery. Cochrane Database Syst. Rev. 2014, 5, CD001181. [Google Scholar] [CrossRef] [Green Version]
- Nelson, R.L.; Glenny, A.M.; Song, F. Antimicrobial prophylaxis for colorectal surgery. Cochrane Database Syst. Rev. 2009, 1, CD001181. [Google Scholar] [CrossRef]
- Güenaga, K.F.; Matos, D.; Wille-Jørgensen, P. Mechanical bowel preparation for elective colorectal surgery. Cochrane Database Syst. Rev. 2011, 9. [Google Scholar] [CrossRef]
- Chen, M.; Song, X.; Chen, L.Z.; Lin, Z.D.; Zhang, X.L. Comparing Mechanical Bowel Preparation With Both Oral and Systemic Antibiotics Versus Mechanical Bowel Preparation and Systemic Antibiotics Alone for the Prevention of Surgical Site Infection After Elective Colorectal Surgery: A Meta-Analysis of Randomized Controlled Clinical Trials. Dis. Colon Rectum 2016, 59, 70–78. [Google Scholar] [CrossRef]
- Dahabreh, I.J.; Steele, D.W.; Shah, N.; Trikalinos, T.A. Oral Mechanical Bowel Preparation for Colorectal Surgery: Systematic Review and Meta-Analysis. Dis. Colon Rectum 2015, 58, 698–707. [Google Scholar] [CrossRef]
- Kim, E.K.; Sheetz, K.H.; Bonn, J.; DeRoo, S.; Lee, C.; Stein, I.; Zarinsefat, A.; Cai, S.; Campbell, D.A., Jr.; Englesbe, M.J. A statewide colectomy experience: The role of full bowel preparation in preventing surgical site infection. Ann. Surg. 2014, 259, 310–314. [Google Scholar] [CrossRef]
- Kiran, R.P.; Murray, A.C.; Chiuzan, C.; Estrada, D.; Forde, K. Combined preoperative mechanical bowel preparation with oral antibiotics significantly reduces surgical site infection, anastomotic leak, and ileus after colorectal surgery. Ann. Surg. 2015, 262, 416–425; discussion 423–425. [Google Scholar] [CrossRef] [Green Version]
- Dolejs, S.C.; Guzman, M.J.; Fajardo, A.D.; Robb, B.W.; Holcomb, B.K.; Zarzaur, B.L.; Waters, J.A. Bowel Preparation Is Associated with Reduced Morbidity in Elderly Patients Undergoing Elective Colectomy. J. Gastrointest. Surg. Off. J. Soc. Surg. Aliment. Tract 2017, 21, 372–379. [Google Scholar] [CrossRef] [PubMed]
- Morris, M.S.; Graham, L.A.; Chu, D.I.; Cannon, J.A.; Hawn, M.T. Oral Antibiotic Bowel Preparation Significantly Reduces Surgical Site Infection Rates and Readmission Rates in Elective Colorectal Surgery. Ann. Surg. 2015, 261, 1034–1040. [Google Scholar] [CrossRef]
- Cannon, J.A.; Altom, L.K.; Deierhoi, R.J.; Morris, M.; Richman, J.S.; Vick, C.C.; Itani, K.M.; Hawn, M.T. Preoperative oral antibiotics reduce surgical site infection following elective colorectal resections. Dis. Colon Rectum 2012, 55, 1160–1166. [Google Scholar] [CrossRef]
- Scarborough, J.E.; Mantyh, C.R.; Sun, Z.; Migaly, J. Combined Mechanical and Oral Antibiotic Bowel Preparation Reduces Incisional Surgical Site Infection and Anastomotic Leak Rates After Elective Colorectal Resection: An Analysis of Colectomy-Targeted ACS NSQIP. Ann. Surg. 2015, 262, 331–337. [Google Scholar] [CrossRef] [PubMed]
- Althumairi, A.A.; Canner, J.K.; Pawlik, T.M.; Schneider, E.; Nagarajan, N.; Safar, B.; Efron, J.E. Benefits of Bowel Preparation Beyond Surgical Site Infection: A Retrospective Study. Ann. Surg. 2016, 264, 1051–1057. [Google Scholar] [CrossRef]
- Rollins, K.E.; Javanmard-Emamghissi, H.; Acheson, A.G.; Lobo, D.N. The Role of Oral Antibiotic Preparation in Elective Colorectal Surgery: A Meta-analysis. Ann. Surg. 2019, 270, 43–58. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ (Clin. Res. Ed.) 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ (Clin. Res. Ed.) 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Takesue, Y.; Yokoyama, T.; Akagi, S.; Ohge, H.; Murakami, Y.; Sakashita, Y.; Miyamoto, K.; Uemura, K.; Itaha, H.; Matsuura, Y. A brief course of colon preparation with oral antibiotics. Surg. Today 2000, 30, 112–116. [Google Scholar] [CrossRef]
- Ishida, H.; Yokoyama, M.; Nakada, H.; Inokuma, S.; Hashimoto, D. Impact of oral antimicrobial prophylaxis on surgical site infection and methicillin-resistant Staphylococcus aureus infection after elective colorectal surgery. Results of a prospective randomized trial. Surg. Today 2001, 31, 979–983. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, M.; Mohri, Y.; Tonouchi, H.; Miki, C.; Nakai, K.; Kusunoki, M.; Mie Surgical Infection Research, G. Randomized clinical trial comparing intravenous antimicrobial prophylaxis alone with oral and intravenous antimicrobial prophylaxis for the prevention of a surgical site infection in colorectal cancer surgery. Surg. Today 2007, 37, 383–388. [Google Scholar] [CrossRef]
- Hata, H.; Yamaguchi, T.; Hasegawa, S.; Nomura, A.; Hida, K.; Nishitai, R.; Yamanokuchi, S.; Yamanaka, T.; Sakai, Y. Oral and Parenteral Versus Parenteral Antibiotic Prophylaxis in Elective Laparoscopic Colorectal Surgery (JMTO PREV 07-01): A Phase 3, Multicenter, Open-label, Randomized Trial. Ann. Surg. 2016, 263, 1085–1091. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, A.; Konishi, T.; Ueno, M.; Fukunaga, Y.; Nagayama, S.; Fujimoto, Y.; Akiyoshi, T.; Yamaguchi, T. Randomized clinical trial of oral and intravenous versus intravenous antibiotic prophylaxis for laparoscopic colorectal resection. Br. J. Surg. 2016, 103, 1608–1615. [Google Scholar] [CrossRef]
- Roos, D.; Dijksman, L.M.; Sondermeijer, B.M.; Oudemans-van Straaten, H.M.; de Wit, L.T.; Gerhards, M.F. Perioperative selective decontamination of the digestive tract (SDD) in elective colorectal surgery. J. Gastrointest. Surg. 2009, 13, 1839–1844. [Google Scholar] [CrossRef]
- Schardey, H.M.; Wirth, U.; Strauss, T.; Kasparek, M.S.; Schneider, D.; Jauch, K.W. Prevention of anastomotic leak in rectal cancer surgery with local antibiotic decontamination: A prospective, randomized, double-blind, placebo-controlled single center trial. Int. J. Colorectal Dis. 2020, 35, 847–857. [Google Scholar] [CrossRef]
- Anjum, N.; Ren, J.; Wang, G.; Li, G.; Wu, X.; Dong, H.; Wu, Q.; Li, J. A Randomized Control Trial of Preoperative Oral Antibiotics as Adjunct Therapy to Systemic Antibiotics for Preventing Surgical Site Infection in Clean Contaminated, Contaminated, and Dirty Type of Colorectal Surgeries. Dis. Colon Rectum 2017, 60, 1291–1298. [Google Scholar] [CrossRef] [PubMed]
- Uchino, M.; Ikeuchi, H.; Bando, T.; Chohno, T.; Sasaki, H.; Horio, Y.; Nakajima, K.; Takesue, Y. Efficacy of Preoperative Oral Antibiotic Prophylaxis for the Prevention of Surgical Site Infections in Patients With Crohn Disease: A Randomized Controlled Trial. Ann. Surg. 2019, 269, 420–426. [Google Scholar] [CrossRef]
- Association of mechanical bowel preparation with oral antibiotics and anastomotic leak following left sided colorectal resection: An international, multi-centre, prospective audit. Colorectal Dis. Off. J. Assoc. Coloproctology Great Br. Irel. 2018, 20 (Suppl. 6), 15–32. [CrossRef] [Green Version]
- Bellows, C.F.; Mills, K.T.; Kelly, T.N.; Gagliardi, G. Combination of oral non-absorbable and intravenous antibiotics versus intravenous antibiotics alone in the prevention of surgical site infections after colorectal surgery: A meta-analysis of randomized controlled trials. Tech. Coloproctology 2011, 15, 385–395. [Google Scholar] [CrossRef]
- Battersby, C.L.F.; Hajibandeh, S.; Hajibandeh, S. Oral Antibiotics as Adjunct to Systemic Antibiotics and Mechanical Bowel Preparation for Prevention of Surgical Site Infections in Colorectal Surgery. Do We Really Need More Trials? Dis. Colon Rectum 2018, 61, e341–e342. [Google Scholar] [CrossRef]
- Toh, J.W.T.; Phan, K.; Hitos, K.; Pathma-Nathan, N.; El-Khoury, T.; Richardson, A.J.; Morgan, G.; Engel, A.; Ctercteko, G. Association of Mechanical Bowel Preparation and Oral Antibiotics Before Elective Colorectal Surgery With Surgical Site Infection: A Network Meta-analysis. JAMA Netw. Open 2018, 1, e183226. [Google Scholar] [CrossRef] [Green Version]
- McSorley, S.T.; Steele, C.W.; McMahon, A.J. Meta-analysis of oral antibiotics, in combination with preoperative intravenous antibiotics and mechanical bowel preparation the day before surgery, compared with intravenous antibiotics and mechanical bowel preparation alone to reduce surgical-site infections in elective colorectal surgery. BJS Open 2018, 2, 185–194. [Google Scholar] [CrossRef] [PubMed]
- McSorley, S.T.; Watt, D.G.; Horgan, P.G.; McMillan, D.C. Postoperative Systemic Inflammatory Response, Complication Severity, and Survival Following Surgery for Colorectal Cancer. Ann. Surg. Oncol. 2016, 23, 2832–2840. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Artinyan, A.; Orcutt, S.T.; Anaya, D.A.; Richardson, P.; Chen, G.J.; Berger, D.H. Infectious postoperative complications decrease long-term survival in patients undergoing curative surgery for colorectal cancer: A study of 12,075 patients. Ann. Surg. 2015, 261, 497–505. [Google Scholar] [CrossRef]
- Schardey, H.M.; Kamps, T.; Rau, H.G.; Gatermann, S.; Baretton, G.; Schildberg, F.W. Bacteria: A major pathogenic factor for anastomotic insufficiency. Antimicrob. Agents Chemother. 1994, 38, 2564–2567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olivas, A.D.; Shogan, B.D.; Valuckaite, V.; Zaborin, A.; Belogortseva, N.; Musch, M.; Meyer, F.; Trimble, W.L.; An, G.; Gilbert, J.; et al. Intestinal tissues induce an SNP mutation in Pseudomonas aeruginosa that enhances its virulence: Possible role in anastomotic leak. PLoS ONE 2012, 7, e44326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiegerinck, M.; Hyoju, S.K.; Mao, J.; Zaborin, A.; Adriaansens, C.; Salzman, E.; Hyman, N.H.; Zaborina, O.; van Goor, H.; Alverdy, J.C. Novel de novo synthesized phosphate carrier compound ABA-PEG20k-Pi20 suppresses collagenase production in Enterococcus faecalis and prevents colonic anastomotic leak in an experimental model. Br. J. Surg. 2018, 105, 1368–1376. [Google Scholar] [CrossRef] [PubMed]
- Gioia, M.; Monaco, S.; Van Den Steen, P.E.; Sbardella, D.; Grasso, G.; Marini, S.; Overall, C.M.; Opdenakker, G.; Coletta, M. The collagen binding domain of gelatinase A modulates degradation of collagen IV by gelatinase B. J. Mol. Biol. 2009, 386, 419–434. [Google Scholar] [CrossRef] [Green Version]
- Braskén, P.; Renvall, S.; Sandberg, M. Fibronectin and collagen gene expression in healing experimental colonic anastomoses. Br. J. Surg. 1991, 78, 1048–1052. [Google Scholar] [CrossRef] [PubMed]
- Evans, M.E.; Feola, D.J.; Rapp, R.P. Polymyxin B sulfate and colistin: Old antibiotics for emerging multiresistant gram-negative bacteria. Ann. Pharmacother. 1999, 33, 960–967. [Google Scholar] [CrossRef]
- Nathens, A.B.; Marshall, J.C. Selective decontamination of the digestive tract in surgical patients: A systematic review of the evidence. Arch. Surg. 1999, 134, 170–176. [Google Scholar] [CrossRef] [Green Version]
- Nelson, R.L.; Hassan, M.; Grant, M.D. Antibiotic prophylaxis in colorectal surgery: Are oral, intravenous or both best and is mechanical bowel preparation necessary? Tech. Coloproctology 2020, 24, 1233–1246. [Google Scholar] [CrossRef]
- Zelhart, M.D.; Hauch, A.T.; Slakey, D.P.; Nichols, R.L. Preoperative antibiotic colon preparation: Have we had the answer all along? J. Am. Coll. Surg. 2014, 219, 1070–1077. [Google Scholar] [CrossRef]
- Koller, S.E.; Bauer, K.W.; Egleston, B.L.; Smith, R.; Philp, M.M.; Ross, H.M.; Esnaola, N.F. Comparative Effectiveness and Risks of Bowel Preparation Before Elective Colorectal Surgery. Ann. Surg. 2018, 267, 734–742. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference and Year of Publication | Study Methodology | Number of Patients | Intervention Group (N) | Control Group (N) | Endpoint SSI | Endpoint AL | Type of Resection | Laparoscopic/Open Surgery | OAB Agent | MBP Agent | Intravenous (i.v) Antibiotics | Comparison Included |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Takesue et al., 2000 [35] | RCT | 83 | 38 | 45 | Yes | Yes | Ileocecal resection–5 Right colectomy–14 Left colectomy–3 Transverse colectomy–6 Sigmoidectomy–24 LAR–24 Miles’ APR–7 | Open | Kanamycin 500 mg + Metronidazole 500 mg at 2 p.m., 3 p.m. and 11 p.m. when surgery was scheduled on 9 a.m. + control group treatment | Polyethylene glycol at 10 a.m. the day before surgery | Cefmetazole 1 g after induction of anesthesia, administered three times a day for 3 consecutive days | MBP + OAB vs. MBP |
| Ishida et al., 2001 [36] | RCT | 143 | 72 | 71 | Yes | Yes | Colectomy–76 Anterior resection–47 APR–9 Total proctectomy with J pouch–3 Total pelvic exenteration–4 Other–4 | Unknown | Kanamycin 500 mg + Erythromycin 400 mg in 4 daily doses, started 2 days preoperatively + control group treatment | Polyethylene glycol 2 L given the day before surgery | Cefotiam 1 g in 2 daily doses for 48 h | MBP+OAB vs. MBP |
| Kobayashi et al., 2007 [37] | RCT | 484 | 242 | 242 | Yes | No | Surgical procedure: Colon–241 Rectum–243 | Unknown | Kanamycin 1 gr + Erythromicin 400 mg at 14:00, 15:00, and 23:00 + control group treatment | Polyethylene glycol 2 L given the day before surgery | Cefmetazole 1 g after the induction of anesthesia, additional dose if the operation was prolonged beyond 3 h. Again twice daily for 3 consecutive days | MBP+OAB vs. MBP |
| Roos et al., 2009 [40] | Cohort | 162 | 76 | 86 | Yes | Yes | Hemicolectomy (right sided)–42 Hemicolectomy (left sided)–15 Transversectomy–4 (Subtotal) colectomy–3 Sigmoid resection–38 LAR–43 | Combination | Polymyxin B sulphate 100 mg + Tobramycin 80 mg + Amphotericin B 500 mg 4 daily doses, started 2 days preoperatively + control group treatment | Two to 4 L of Klean-Prep® were administered in 24 h and/or a fluid diet was given starting 1 day before surgery. In rectal surgery, also an enema was applied | Cefuroxime 1500 mg + metronidazole 500 mg 3 doses in 24 h | MBP+OAC vs. MBP |
| Hata et al., 2016 [38] | RCT | 579 | 289 | 290 | No | Yes | Colectomy–376 Anterior resection–183 APR–20 | Laparoscopic | Kanamycin 1 g + Metronidazole 750 mg at 13 h and 9 h before the surgery + control group treatment | Sodium picosulphate 75 mg and magnesium citrate 34 g with 180 mL water the day before surgery | Cefmetazole 1 g was administered intravenously 30 min before the skin incision, additional dose was given every 3 h during the surgery | MBP+OAB vs. MBP |
| Ikeda et al., 2016 [39] | RCT | 511 | 255 | 256 | No | Yes | Colonic surgery–309 Anterior resection–177 APR–25 | Laparoscopic | Kanamycin 1000 mg 2 doses + Metronidazole 750 mg, started 1 day preoperative + control group treatment | Magnesium citrate and sodium picosulphate the day before surgery | Cefmetazole 1 g 3 doses in 24 h | MBP+OAB vs. MBP |
| Abis et al., 2019 [17] | RCT | 455 | 228 | 227 | Yes | Yes | Right hemicolectomy–162 Transverse colectomy–17 Left hemicolectomy–41 Sigmoid resection–124 Low anterior resection–103 Other–8 | Combination 98.2% laparo-scopic and 1.8% open in both groups | SDD 3 days prior to surgery until 3 days after surgery or when normal bowel motion occured + control group treatment | Klean-Prep | Cefazoline 1 gr + Metronidazol 500 mg, intravenously, 30 min prior to skin incision | MBP+OAB vs. MBP |
| Schardey et al., 2020 [41] | RCT | 80 | 40 | 40 | Yes | Yes | (low anterior resection with TME–80 | Unknown | Polymyxin B sulphate 100 mg + Tobramycin 80 mg + Vancomycin 125 mg + Amphotericin B 500 mg 4 daily doses, started 1 day preoperatively till day 7 postoperatively. | Klean-Prep | Amphotericin B 500 mg + Lactulose 305 mg | MBP+OAB vs. MBP |
| Reference | Random Sequence Generation | Allocation Concealment | Blinding of Participant and Personnel | Blinding of Outcome Assessment | Incomplete Outcome Data | Selective Reporting |
|---|---|---|---|---|---|---|
| Takesue et al. [35] | unclear | unclear | unclear | unclear | high | unclear |
| Ishida et al. [36] | low | high | high | high | low | unclear |
| Kobayashi et al. [37] | low | unclear | high | high | high | high |
| Hata et al. [38] | low | low | high | high | low | low |
| Ikeda et al. [39] | low | low | high | low | low | low |
| Abis et al. [17] | low | low | high | low | low | low |
| Schardey et al. [41] | low | low | low | low | high | high |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grewal, S.; Reuvers, J.R.D.; Abis, G.S.A.; Otten, R.H.J.; Kazemier, G.; Stockmann, H.B.A.C.; van Egmond, M.; Oosterling, S.J. Oral Antibiotic Prophylaxis Reduces Surgical Site Infection and Anastomotic Leakage in Patients Undergoing Colorectal Cancer Surgery. Biomedicines 2021, 9, 1184. https://doi.org/10.3390/biomedicines9091184
Grewal S, Reuvers JRD, Abis GSA, Otten RHJ, Kazemier G, Stockmann HBAC, van Egmond M, Oosterling SJ. Oral Antibiotic Prophylaxis Reduces Surgical Site Infection and Anastomotic Leakage in Patients Undergoing Colorectal Cancer Surgery. Biomedicines. 2021; 9(9):1184. https://doi.org/10.3390/biomedicines9091184
Chicago/Turabian StyleGrewal, Simran, J. Reinder D. Reuvers, Gabor S. A. Abis, René H. J. Otten, Geert Kazemier, Hein B. A. C. Stockmann, Marjolein van Egmond, and Steven J. Oosterling. 2021. "Oral Antibiotic Prophylaxis Reduces Surgical Site Infection and Anastomotic Leakage in Patients Undergoing Colorectal Cancer Surgery" Biomedicines 9, no. 9: 1184. https://doi.org/10.3390/biomedicines9091184
APA StyleGrewal, S., Reuvers, J. R. D., Abis, G. S. A., Otten, R. H. J., Kazemier, G., Stockmann, H. B. A. C., van Egmond, M., & Oosterling, S. J. (2021). Oral Antibiotic Prophylaxis Reduces Surgical Site Infection and Anastomotic Leakage in Patients Undergoing Colorectal Cancer Surgery. Biomedicines, 9(9), 1184. https://doi.org/10.3390/biomedicines9091184