
Diagnostic Accuracy of Dehydroepiandrosterone Sulfate and Corticotropin in Autonomous Cortisol Secretion

 ,
,
Abstract
:1. Introduction
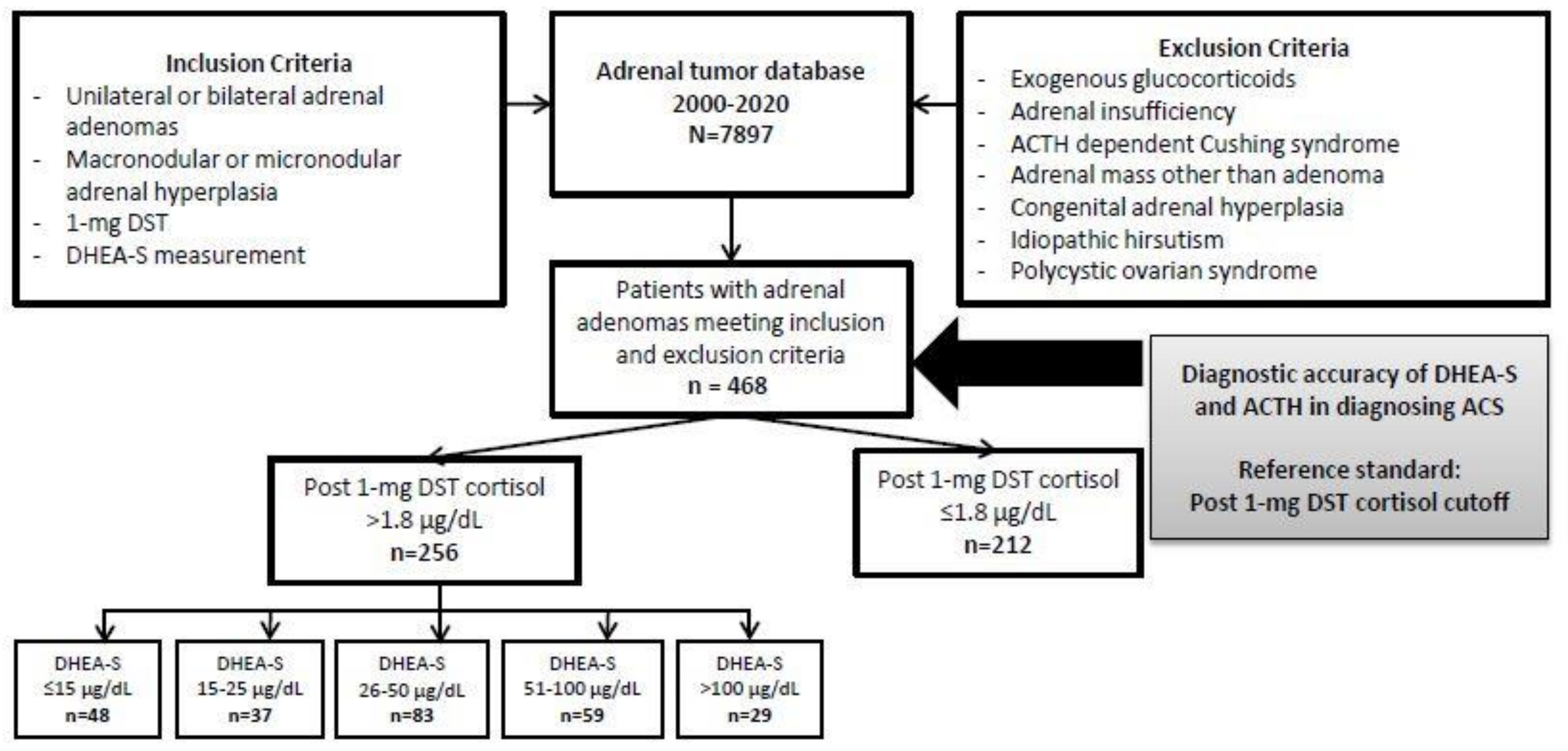
2. Materials and Methods
2.1. Biochemical Analysis
2.2. Statistics
3. Results
3.1. Patients
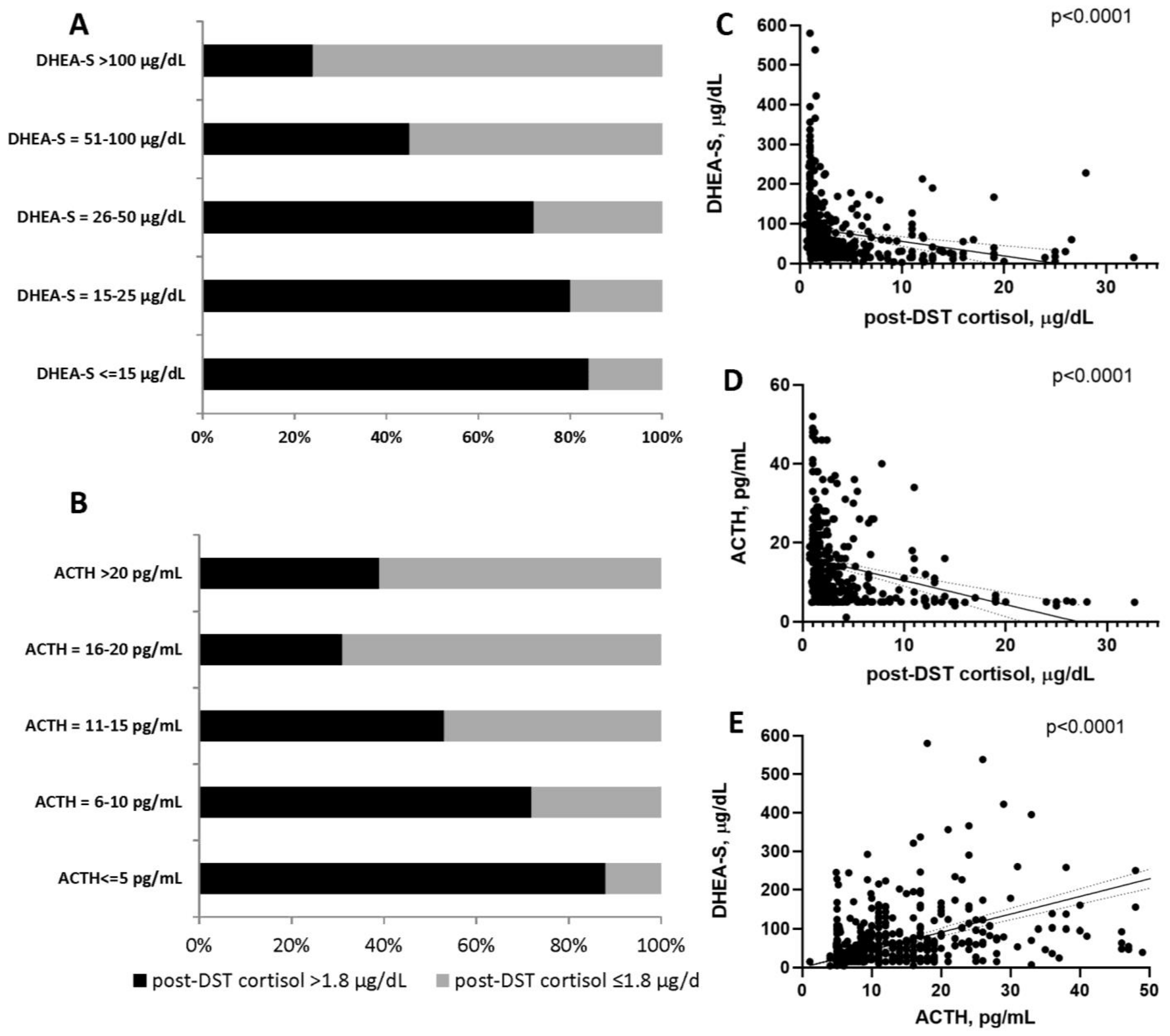
3.2. Accuracy of DHEA-S and ACTH in Diagnosing of ACSs
4. Discussion
4.1. Strengths and Limitations
4.2. Clinical Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Reimondo, G.M.; Castellano, E.; Grosso, M.; Priotto, R.; Puglisi, S.; Pia, A.; Pellegrino, M.; Borretta, G.; Terzolo, M. Adrenal Incidentalomas are Tied to Increased Risk of Diabetes: Findings from a Prospective Study. J. Clin. Endocrinol. Metab. 2020, 105, e973–e981. [Google Scholar] [CrossRef] [PubMed]
- Fassnacht, M.; Arlt, W.; Bancos, I.; Dralle, H.; Newell-Price, J.; Sahdev, A. Management of adrenal incidentalomas: European Society of Endocrinology Clinical Practice Guide-line in collaboration with the European Network for the Study of Adrenal Tumors. Eur. J. Endocrinol. 2016, 175, G1–G34. [Google Scholar] [CrossRef] [Green Version]
- Vaidya, A.; Hamrahian, A.; Bancos, I.; Fleseriu, M.; Ghayee, H.K. The Evaluation of Incidentally Discovered Adrenal Masses. Endocr. Pr. 2019, 25, 178–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ebbehoj, A.; Li, D.; Kaur, R.J.; Zhang, C.; Singh, S.; Li, T.; Atkinson, E.; Achenbach, S.; Khosla, S.; Arlt, W.; et al. Epidemiology of adrenal tumours in Olmsted County, Minnesota, USA: A population-based cohort study. Lancet Diabetes Endocrinol. 2020, 8, 894–902. [Google Scholar] [CrossRef]
- Nieman, L.K.; Biller, B.M.; Findling, J.W.; Newell-Price, J.; Savage, M.O.; Stewart, P.M.; Montori, V.M. The diagnosis of Cushing’s syndrome: An Endocrine Society Clinical Practice Guideline. J. Clin. Endo Crinol. Metab. 2008, 93, 1526–1540. [Google Scholar] [CrossRef]
- Delivanis, D.A.; Iñiguez-Ariza, N.M.; Zeb, M.H.; Moynagh, M.R.; Takahashi, N.; McKenzie, T.J.; Thomas, M.A.; Gogos, C.; Young, W.F.; Bancos, I.; et al. Impact of hypercortisolism on skeletal muscle mass and adipose tissue mass in patients with adrenal adenomas. Clin. Endocrinol 2017, 88, 209–216. [Google Scholar] [CrossRef] [Green Version]
- Di Dalmazi, G.; Vicennati, V.; Garelli, S.; Casadio, E.; Rinaldi, E.; Giampalma, E. Cardiovascular events and mortality in patients with adrenal incidentalomas that are either non-secreting or associated with intermediate phenotype or subclinical Cushing’s syndrome: A 15-year retrospective study. Lancet Diabetes Endocrinol. 2014, 2, 396–405. [Google Scholar] [CrossRef]
- Elhassan, Y.; Alahdab, F.; Prete, A.; Delivanis, D.; Khanna, A.; Murad, M.; O’Reilly, M.; Arlt, W.; Bancos, I. Natural history of adrenal incidentalomas with and without mild autonomous cortisol excess; a systematic review and meta-analysis. Endocr. Abstr. 2018, 171, 107–116. [Google Scholar] [CrossRef]
- Patrova, J.; Kjellman, M.; Wahrenberg, H.; Falhammar, H. Increased mortality in patients with adrenal incidentalomas and autonomous cortisol secretion: A 13-year retrospective study from one center. Endocrine 2017, 58, 267–275. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Atkinson, E.J.; Achenbach, S.J.; LeBrasseur, N.; Bancos, I. Frailty in Patients With Mild Autonomous Cortisol Secretion is Higher Than in Patients with Nonfunction-ing Adrenal Tumors. J. Clin. Endocrinol. Metab. 2020, 105, e3307–e3315. [Google Scholar] [CrossRef] [PubMed]
- Dennedy, M.C.; Annamalai, A.K.; Prankerd-Smith, O.; Freeman, N.; Vengopal, K.; Graggaber, J. Low DHEAS: A Sensitive and Specific Test for the Detection of Subclinical Hypercortisolism in Ad-renal Incidentalomas. J. Clin. Endocrinol. Metab. 2017, 102, 786–792. [Google Scholar] [CrossRef]
- Hána, V.; Ježková, J.; Kosák, M.; Kršek, M.; Hill, M. Novel GC-MS/MS Technique Reveals a Complex Steroid Fingerprint of Subclinical Hypercortisolism in Adrenal Incidentalomas. J. Clin. Endocrinol. Metab. 2019, 104, 3545–3556. [Google Scholar] [CrossRef] [PubMed]
- Yener, S.; Yilmaz, H.; Demir, T.; Secil, M.; Çömlekçi, A. DHEAS for the prediction of subclinical Cushing’s syndrome: Perplexing or advantageous? Endocrine 2014, 48, 669–676. [Google Scholar] [CrossRef] [PubMed]
- Ueland, G.Å.; Grinde, T.; Methlie, P.; Kelp, O.; Løvås, K.; Husebye, E.S. Diagnostic testing of autonomous cortisol secretion in adrenal incidentalomas. Endocr. Connect. 2020, 9, 963–970. [Google Scholar] [CrossRef] [PubMed]
- Mantero, F.; Terzolo, M.; Arnaldi, G.; Osella, G.; Masini, A.M.; Alì, A. A survey on adrenal incidentaloma in Italy. Study Group on Adrenal Tumors of the Italian Society of Endocrinology. J. Clin. Endocrinol. Metab. 2000, 85, 637–644. [Google Scholar]



{kind=link}
{kind=link}
| Total | Post-DST Cortisol ≤1.8 mcg/dL | Post-DST Cortisol >1.8 mcg/dL | p Value | |
|---|---|---|---|---|
| (n = 468) | (n = 212) | (n = 256) | ||
| Age, years | ||||
| Median (ranges) | 58 (18–89) | 57 (20–89) | 59 (18–87) | 0.0005 |
| Female, n (%) | 308 (66) | 133 (63) | 175 (68) | 0.2 |
| Bilateral, n (%) | 126 (27) | 40 (19) | 86 (34) | 0.0005 |
| Tumor size, mm | ||||
| Median (ranges) | 26 (5–135) | 19 (5–135) | 34 (5–128) | <0.0001 |
| Post-DST cortisol, mcg/dL | ||||
| Median (ranges) | 2.0 (0.5–32.7) | 1.2 (0.5–1.8) | 3.45 (1.9–32.7) | |
| DHEA-S, mcg/dL | ||||
| Median (ranges) | 53 (2.8–606) | 87.3 (11–606) | 35 (2.8–244) | <0.0001 |
| DHEA-S ratio a | 3.2 (0.1–33.6) | 4.6 (0.6–33.6) | 2.3 (0.1–23.3) | <0.0001 |
| Median (ranges) | ||||
| ACTH b, pg/mL | 11 (1.1–52) | 16 (4.9–52) | 8.3 (1.1–46) | <0.0001 |
| Median (ranges) | ||||
| Adrenalectomy, n (%) | 219 (47) | 59 (28) | 160 (63) | <0.0001 |
| Cutoff | Sensitivity, % (95% CI) | Specificity, % (95% CI) | PPV, % (95% CI) | NPV, % (95% CI) | False Positive Rate, % |
|---|---|---|---|---|---|
| DHEA-S | |||||
| <15 mcg/dL | 18.8 (14.2–24.1) | 95.8 (92.1–98.0) | 84.2 (72.8–91.4) | 49.4 (47.8–51.0) | 4.2 |
| <25 mcg/dL | 33.2 (27.4–39.3) | 91.5 (86.9–94.9) | 82.5 (74.6–88.4) | 53.2 (50.8–55.5) | 8.4 |
| <40 mcg/dL | 57.4 (51.1–63.6) | 83.5 (77.8–88.2) | 80.8 (75.3–85.3) | 61.9 (58.2–65.5) | 16.5 |
| <50 mcg/dL | 65.6 (59.5–71.4) | 76.4 (70.1–82.0) | 77.1 (72.2–81.3) | 64.8 (60.5–68.9) | 23.6 |
| <80 mcg/dL | 83.2 (78.1–87.6) | 53.8 (46.8–60.6) | 68.5 (65.1–71.7) | 72.6 (66.3–78.2) | 46.2 |
| <100 mcg/dL | 88.7 (84.1–92.3) | 42.9 (36.2–49.9) | 65.2 (62.4–68.0) | 75.8 (68.3–82.1) | 57.0 |
| DHEA-S ratio | |||||
| <1.2 | 32.0 (26.4–38.1) | 92.9 (88.6–96.0) | 84.5 (76.5–90.2) | 53.1 (50.8–55.4) | 7.0 |
| <1.8 | 42.2 (36.1–48.5) | 85.4 (79.9–89.8) | 77.7 (70.9–83.3) | 55.0 (52.1–57.9) | 14.6 |
| ACTH | |||||
| <10 pg/mL | 61.8 (54.9–68.3) | 75.3 (67.7–81.9) | 77.9 (72.4–82.6) | 58.3 (53.6–62.9) | 24.7 |
| <15 pg/mL | 79.3 (73.3–84.5) | 53.9 (45.7–62.0) | 70.8 (66.8–74.4) | 64.8 (57.8–71.3) | 46.1 |
| <20 pg/mL | 87.6 (82.4–91.6) | 27.3 (20.4–35.0) | 62.9 (60.3–65.4) | 60.9 (50.1–70.7) | 72.7 |
| DHEA-S and ACTH | |||||
| DHEA-S < 40 mcg/dL and ACTH < 10 pg/mL | 38.7 (32.2–45.5) | 91.6 (86.0–95.4) | 86.6 (78.9–91.8) | 51.5 (48.6–54.4) | 8.4 |
| DHEA-S < 40 mcg/dL and ACTH < 15 pg/mL | 49.3 (42.5–56.2) | 88.3 (82.2–92.9) | 85.6 (79.1–90.4) | 55.3 (51.7–58.8) | 11.7 |
| DHEA-S < 40 mcg/dL and ACTH < 20 pg/mL | 53.9 (47.0–60.7) | 85.7 (79.2–90.8) | 84.2 (78.0–88.9) | 56.9 (53.0–60.7) | 14.3 |
| DHEA-S < 25 mcg/dL and ACTH < 10 pg/mL | 26.3 (20.5–32.7) | 94.8 90.0-97.7 | 87.7 (77.8–93.6) | 47.7 (45.5–49.9) | 5.2 |
| DHEA-S < 25 mcg/dL and ACTH < 15 pg/mL | 31.3 (25.2–38.0) | 93.5 (88.4–96.8) | 87.2 (78.4–92.7) | 49.2 (46.7–51.6) | 6.5 |
| DHEA-S < 25 mcg/dL and ACTH < 20 pg/mL | 34.1 (27.8–40.8) | 91.6 (86.0–95.4) | 85.1 (76.6–90.8) | 49.7 (47.0–52.3) | 8.4 |
| Author, Year | Patients a,b n | Diagnosis of ACS | DHEA-S Assay | DHEA-S Cutoff | Accuracy |
|---|---|---|---|---|---|
| Yener, 2015 [13] | 38 ACS 141 NFAT | At least 2 of the following: Post-DST cortisol >3 mcg/dL ACTH <10 pg/mL 24 h urine cortisol >70 mcg/dL | Solid-phase, competitive, chemiluminescent enzyme immunoassay (Immulite 2000, Diagnostic Products Corporation, Los Angeles, CA, USA) | DHEA-S of 40 mcg/dL | AUC of 0.79 Sensitivity of 68% Specificity of 75% |
| Dennedy, 2017 [11] | 29 ACS 138 NFAT | At least 2 of the following: Post-DST cortisol >1.8 mcg/dL Sleeping midnight cortisol >1.8 mcg/dL or awake midnight cortisol >7.5 mcg/dL Elevated 24 h urine cortisol All patients had ACTH <10 pg/mL (not a definition criteria) | Solid-phase competitive immunoassay, Siemens (Surrey, UK) Immulite 2000 platform | DHEA-S ratio ≤1.12 | AUC of 0.95 Sensitivity of 100% Specificity of 91.9% |
| Ueland, 2020 [14] | 58 ACS 54 NFAT | Post-DST cortisol >1.8 mcg/Dl [2] | Chemiluminescent immunoassay (CLIA) using Siemens Immulite 2000 XPi | DHEA-S of 40 mcg/dL | AUC of 0.76 Sensitivity of 58% Specificity of 80% |
| DHEA-S ratio | AUC of 0.69 | ||||
| Current study | 256 ACS 212 NFAT | Post-DST cortisol >1.8 mcg/dL [2] | Chemiluminescent competitive binding immunoenzymatic assay (Access DHEA-S, Beckman-Coulter Inc., Fullerton, CA, USA 2017) | DHEA-S of 40 mcg/dL DHEA-S ratio | AUC of 0.767 Sensitivity of 57.4% Specificity of 83.5% AUC of 0.693 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carafone, L.E.; Zhang, C.D.; Li, D.; Lazik, N.; Hamidi, O.; Hurtado, M.D.; Young, W.F., Jr.; Thomas, M.A.; Dy, B.M.; Lyden, M.L.; et al. Diagnostic Accuracy of Dehydroepiandrosterone Sulfate and Corticotropin in Autonomous Cortisol Secretion. Biomedicines 2021, 9, 741. https://doi.org/10.3390/biomedicines9070741
Carafone LE, Zhang CD, Li D, Lazik N, Hamidi O, Hurtado MD, Young WF Jr., Thomas MA, Dy BM, Lyden ML, et al. Diagnostic Accuracy of Dehydroepiandrosterone Sulfate and Corticotropin in Autonomous Cortisol Secretion. Biomedicines. 2021; 9(7):741. https://doi.org/10.3390/biomedicines9070741
Chicago/Turabian StyleCarafone, Lindsay E., Catherine D. Zhang, Dingfeng Li, Natalia Lazik, Oksana Hamidi, Maria Daniela Hurtado, William F. Young, Jr., Melinda A. Thomas, Benzon M. Dy, Melanie L. Lyden, and et al. 2021. "Diagnostic Accuracy of Dehydroepiandrosterone Sulfate and Corticotropin in Autonomous Cortisol Secretion" Biomedicines 9, no. 7: 741. https://doi.org/10.3390/biomedicines9070741
APA StyleCarafone, L. E., Zhang, C. D., Li, D., Lazik, N., Hamidi, O., Hurtado, M. D., Young, W. F., Jr., Thomas, M. A., Dy, B. M., Lyden, M. L., Foster, T. R., McKenzie, T. J., & Bancos, I. (2021). Diagnostic Accuracy of Dehydroepiandrosterone Sulfate and Corticotropin in Autonomous Cortisol Secretion. Biomedicines, 9(7), 741. https://doi.org/10.3390/biomedicines9070741