
Dose-Dependent Effects of a Novel Selective EP4 Prostaglandin Receptor Agonist on Treatment of Critical Size Femoral Bone Defects in a Rat Model

 , , and
, , and
Abstract
:
1. Introduction
2. Materials and Methods
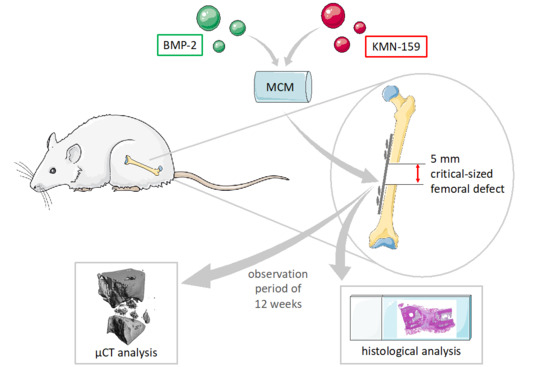
2.1. Study Design
2.2. Preparation of the Implants
2.3. Animals
2.4. Surgical Procedure
2.5. Preparations for Micro-Computed Tomography (µCT) and Histology
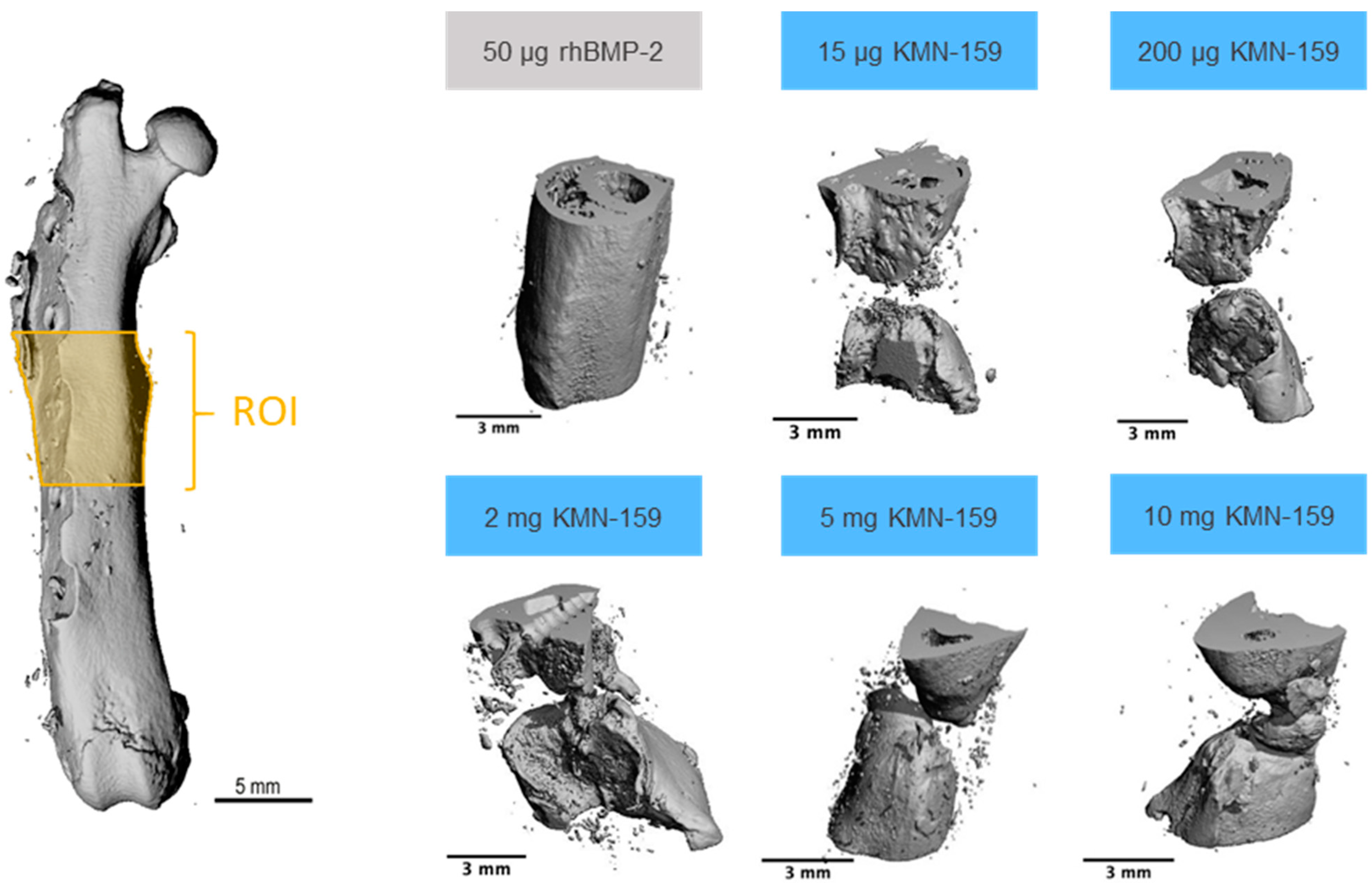
2.6. High-Resolution µCT Analysis
2.7. Histological Examination
2.8. Statistics
3. Results
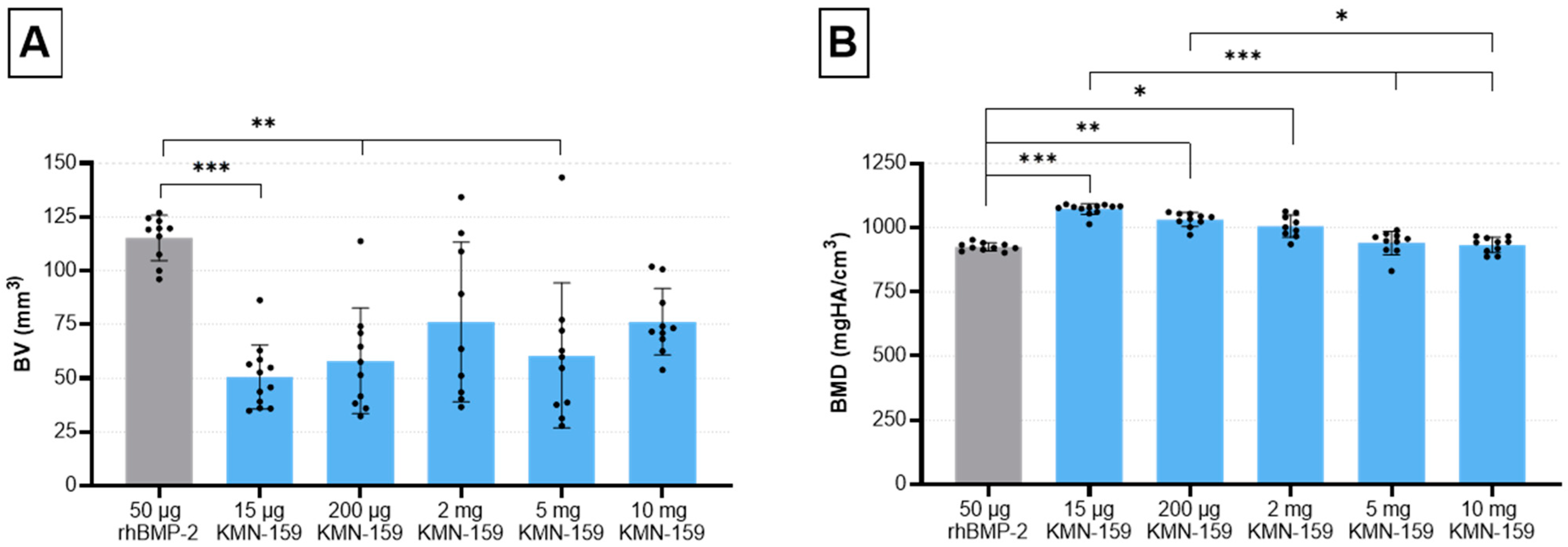
3.1. µCT Analysis
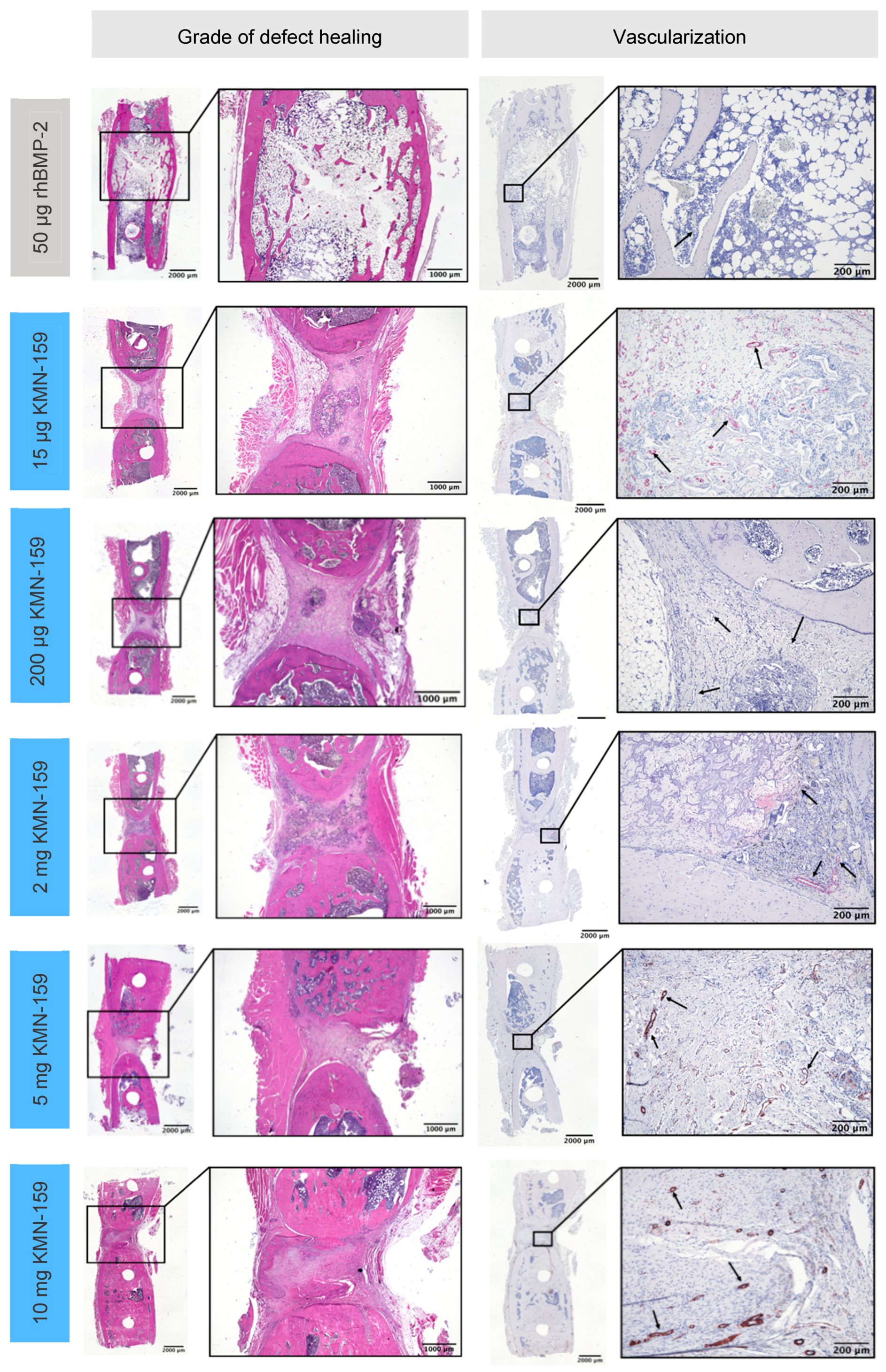
3.2. Histological Analysis
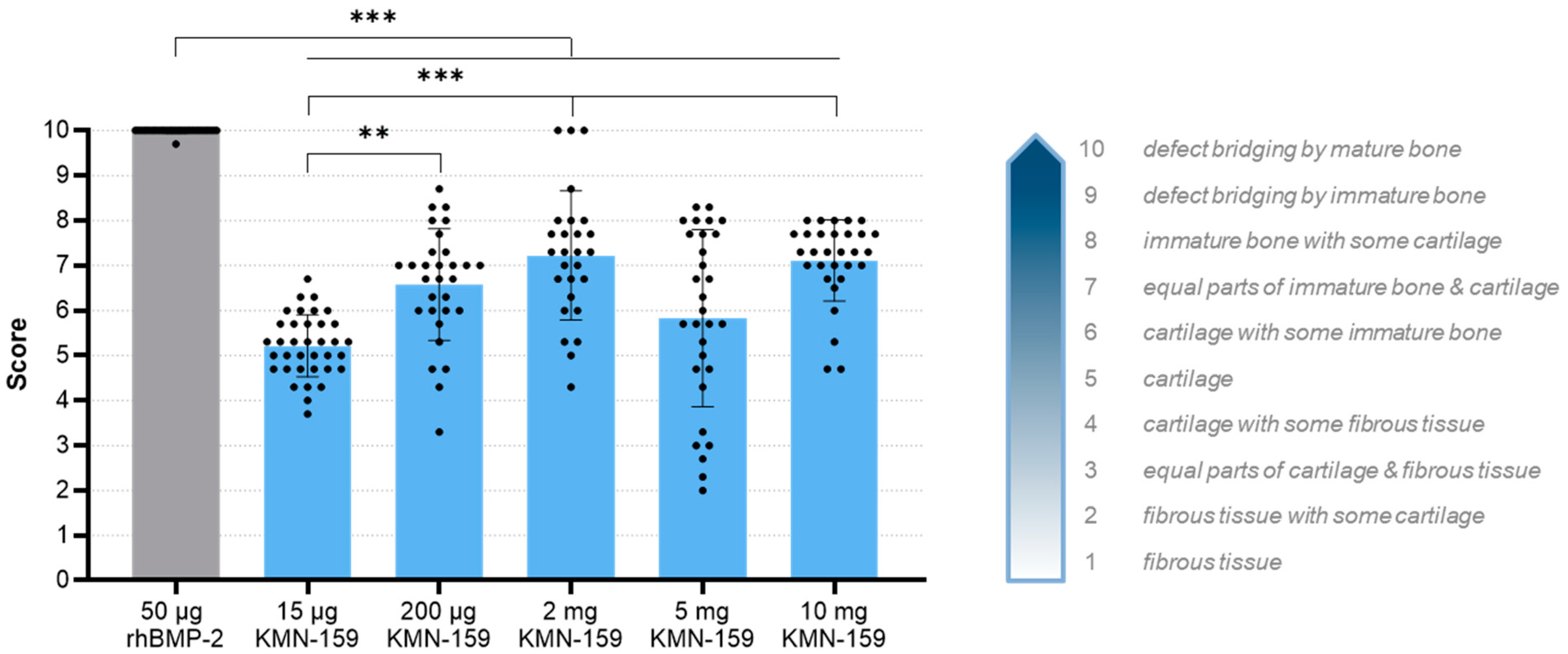
3.2.1. Histological Grade of Defect Healing
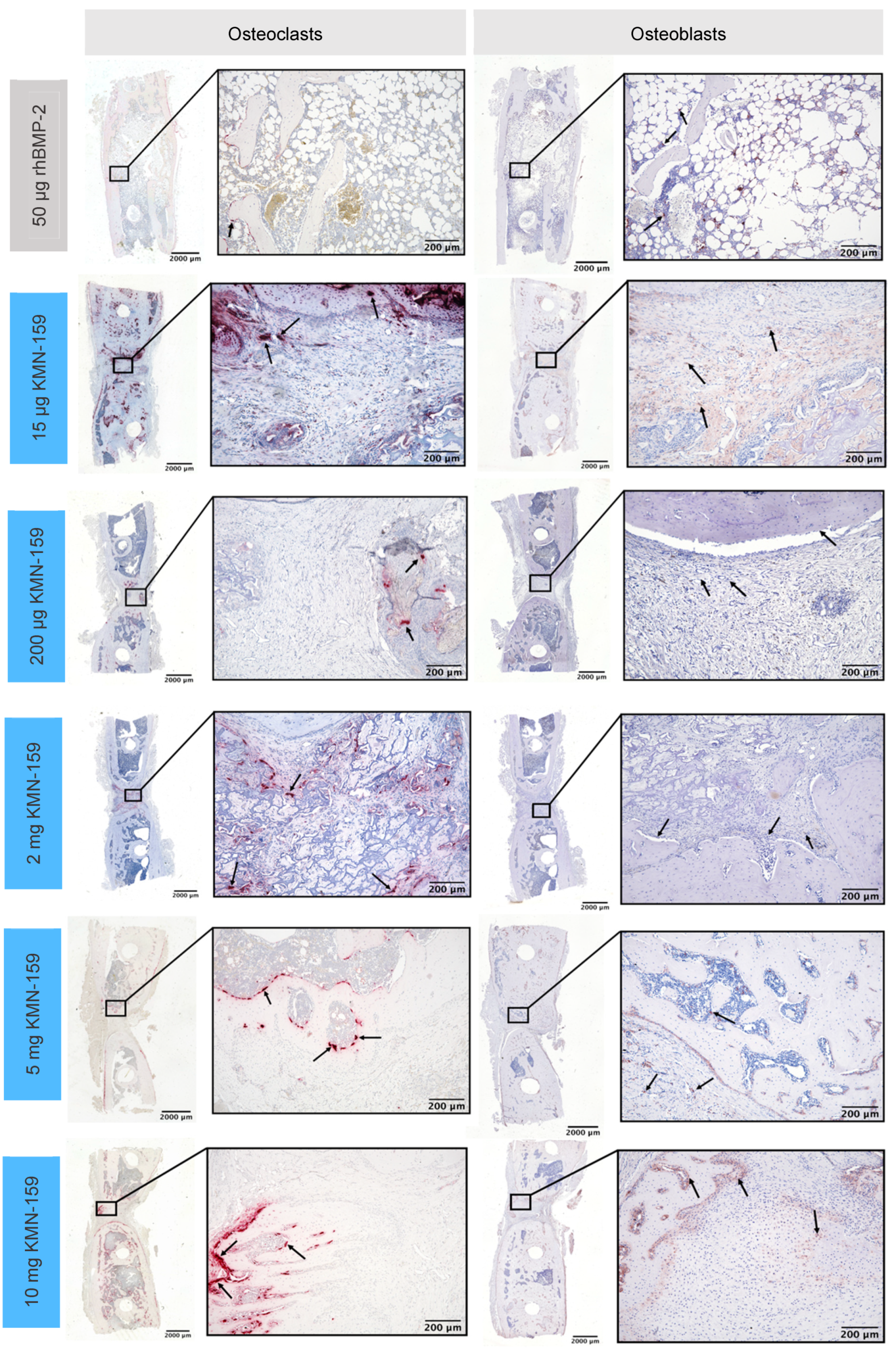
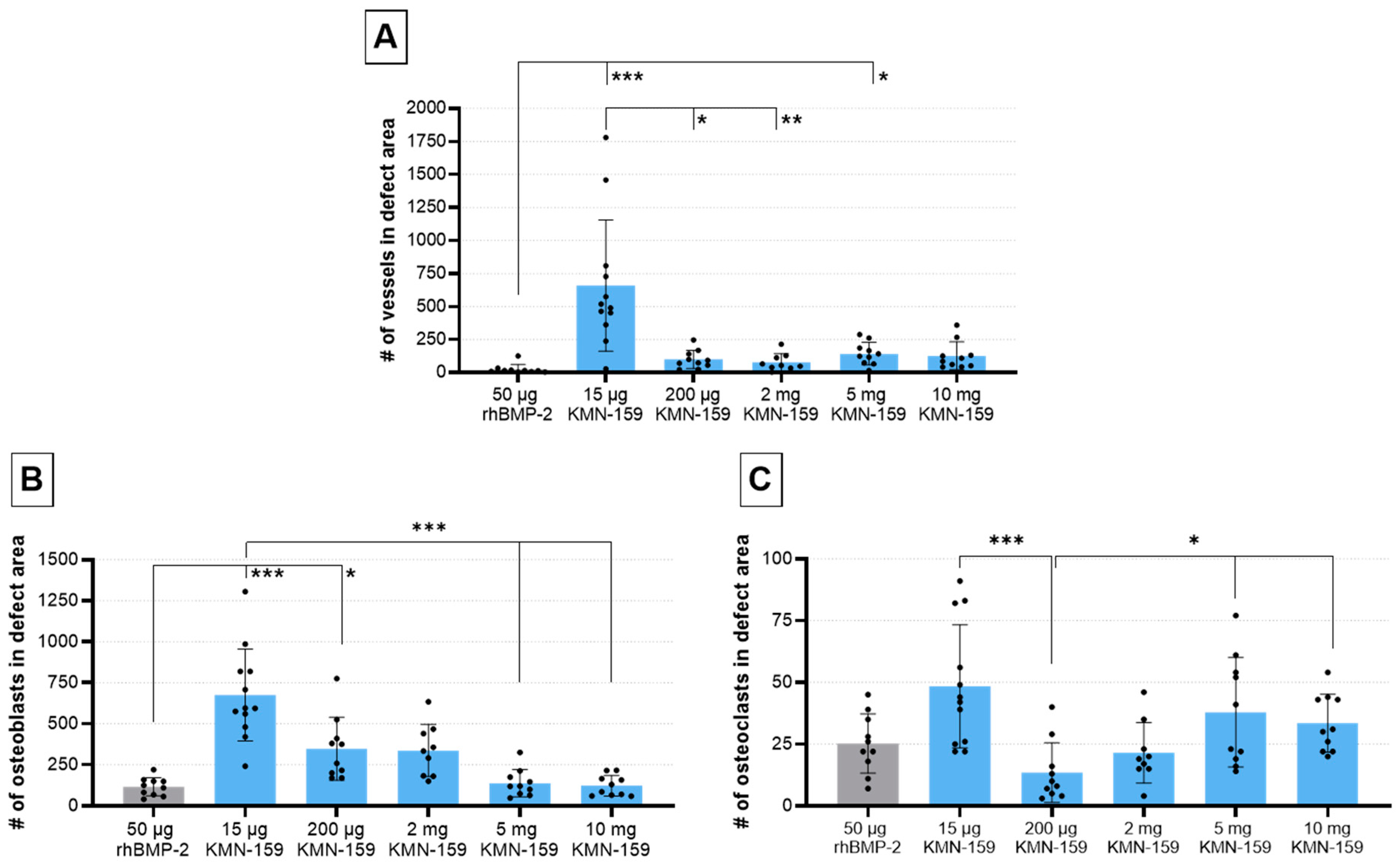
3.2.2. Histological Analysis of Vascularization and Bone Cell Markers
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Khan, S.N.; Cammisa, F.P.; Sandhu, H.S.; Diwan, A.D.; Girardi, F.P.; Lane, J.M. The Biology of Bone Grafting. J. Am. Acad. Orthop. Surg. 2005, 13, 77–86. [Google Scholar] [CrossRef]
- Dimitriou, R.; Jones, E.; McGonagle, D.; Giannoudis, P.V. Bone Regeneration: Current Concepts and Future Directions. BMC Med. 2011, 9, 66. [Google Scholar] [CrossRef] [Green Version]
- Chenard, K.E.; Teven, C.M.; He, T.-C.; Reid, R.R. Bone Morphogenetic Proteins in Craniofacial Surgery: Current Techniques, Clinical Experiences, and the Future of Personalized Stem Cell Therapy. J. Biomed. Biotechnol. 2012, 2012, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Roberts, T.T.; Rosenbaum, A.J. Bone Grafts, Bone Substitutes and Orthobiologics. Organogenesis 2012, 8, 114–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cahill, K.S.; Chi, J.H.; Day, A.; Claus, E.B. Prevalence, Complications, and Hospital Charges Associated with Use of Bone-Morphogenetic Proteins in Spinal Fusion Procedures. JAMA 2009, 302, 58–66. [Google Scholar] [CrossRef] [Green Version]
- Carragee, E.J.; Hurwitz, E.L.; Weiner, B.K. A Critical Review of Recombinant Human Bone Morphogenetic Protein-2 Trials in Spinal Surgery: Emerging Safety Concerns and Lessons Learned. Spine J. 2011, 11, 471–491. [Google Scholar] [CrossRef] [PubMed]
- Epstein, N.E. Pros, Cons, and Costs of INFUSE in Spinal Surgery. Surg. Neurol. Int. 2011, 2, 10. [Google Scholar] [CrossRef] [Green Version]
- Suzawa, T.; Miyaura, C.; Inada, M.; Maruyama, T.; Sugimoto, Y.; Ushikubi, F.; Ichikawa, A.; Narumiya, S.; Suda, T. The Role of Prostaglandin E Receptor Subtypes (EP1, EP2, EP3, and EP4) in Bone Resorption: An Analysis Using Specific Agonists for the Respective EPs. Endocrinology 2000, 141, 1554–1559. [Google Scholar] [CrossRef]
- Namkoong, S.; Lee, S.-J.; Kim, C.-K.; Kim, Y.-M.; Chung, H.-T.; Lee, H.; Han, J.-A.; Ha, K.-S.; Kwon, Y.-G.; Kim, Y.-M. Prostaglandin E2 Stimulates Angiogenesis by Activating the Nitric Oxide/CGMP Pathway in Human Umbilical Vein Endothelial Cells. Exp. Mol. Med. 2005, 37, 588–600. [Google Scholar] [CrossRef] [Green Version]
- Schell, H.; Duda, G.N.; Peters, A.; Tsitsilonis, S.; Johnson, K.A.; Schmidt-Bleek, K. The Haematoma and Its Role in Bone Healing. J. Exp. Orthop. 2017, 4, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lisowska, B.; Kosson, D.; Domaracka, K. Lights and Shadows of NSAIDs in Bone Healing: The Role of Prostaglandins in Bone Metabolism. Drug Des. Dev. Ther. 2018, 12, 1753–1758. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanchanale, V.; Eardley, I. Alprostadil for the Treatment of Impotence. Expert Opin. Pharm. 2014, 15, 421–428. [Google Scholar] [CrossRef] [PubMed]
- Matsou, A.; Anastasopoulos, E. Investigational Drugs Targeting Prostaglandin Receptors for the Treatment of Glaucoma. Expert Opin. Investig. Drugs 2018, 27, 777–785. [Google Scholar] [CrossRef] [PubMed]
- Scally, B.; Emberson, J.R.; Spata, E.; Reith, C.; Davies, K.; Halls, H.; Holland, L.; Wilson, K.; Bhala, N.; Hawkey, C.; et al. Effects of Gastroprotectant Drugs for the Prevention and Treatment of Peptic Ulcer Disease and Its Complications: A Meta-Analysis of Randomised Trials. Lancet Gastroenterol. Hepatol. 2018, 3, 231–241. [Google Scholar] [CrossRef] [Green Version]
- Duarte, A.C.; Barbosa, L.; Santos, M.J.; Cordeiro, A. Iloprost Infusion through Elastomeric Pump for the Outpatient Treatment of Severe Raynaud’s Phenomenon and Digital Ulcers—A Single Centre Experience. Acta Reum. Port 2018, 43, 237–238. [Google Scholar]
- Wendler, S.; Schlundt, C.; Bucher, C.H.; Birkigt, J.; Schipp, C.J.; Volk, H.-D.; Duda, G.N.; Schmidt-Bleek, K. Immune Modulation to Enhance Bone Healing—A New Concept to Induce Bone Using Prostacyclin to Locally Modulate Immunity. Front. Immunol. 2019, 10, 713. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoshida, K.; Oida, H.; Kobayashi, T.; Maruyama, T.; Tanaka, M.; Katayama, T.; Yamaguchi, K.; Segi, E.; Tsuboyama, T.; Matsushita, M.; et al. Stimulation of Bone Formation and Prevention of Bone Loss by Prostaglandin E EP4 Receptor Activation. Proc. Natl. Acad. Sci. USA 2002, 99, 4580–4585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barrett, S.D.; Holt, M.C.; Kramer, J.B.; Germain, B.; Ho, C.S.; Ciske, F.L.; Kornilov, A.; Colombo, J.M.; Uzieblo, A.; O’Malley, J.P.; et al. Difluoromethylene at the γ-Lactam α-Position Improves 11-Deoxy-8-Aza-PGE1 Series EP4 Receptor Binding and Activity: 11-Deoxy-10,10-Difluoro-8-Aza-PGE1 Analog (KMN-159) as a Potent EP4 Agonist. J. Med. Chem. 2019, 62, 4731–4741. [Google Scholar] [CrossRef]
- Owen, T.A.; Patel, C.; Wei, S.; Ho, C.S.; Birmingham, K.; Sanchez, S.; Chung, N.; Cahill, A.; O’Malley, J.P.; Barrett, S.D.; et al. KMN-159, a Novel EP4 Receptor Selective Agonist, Stimulates Osteoblastic Differentiation in Cultured Whole Rat Bone Marrow. Gene 2020, 748, 144668. [Google Scholar] [CrossRef]
- Gelinsky, M.; Welzel, P.B.; Simon, P.; Bernhardt, A.; König, U. Porous Three-Dimensional Scaffolds Made of Mineralised Collagen: Preparation and Properties of a Biomimetic Nanocomposite Material for Tissue Engineering of Bone. Chem. Eng. J. 2008, 137, 84–96. [Google Scholar] [CrossRef]
- Bernhardt, A.; Wehrl, M.; Paul, B.; Hochmuth, T.; Schumacher, M.; Schütz, K.; Gelinsky, M. Improved Sterilization of Sensitive Biomaterials with Supercritical Carbon Dioxide at Low Temperature. PLoS ONE 2015, 10, e0129205. [Google Scholar] [CrossRef] [Green Version]
- Raina, D.B.; Matuszewski, L.-M.; Vater, C.; Bolte, J.; Isaksson, H.; Lidgren, L.; Tägil, M.; Zwingenberger, S. A Facile One-Stage Treatment of Critical Bone Defects Using a Calcium Sulfate/Hydroxyapatite Biomaterial Providing Spatiotemporal Delivery of Bone Morphogenic Protein–2 and Zoledronic Acid. Sci. Adv. 2020, 6, eabc1779. [Google Scholar] [CrossRef] [PubMed]
- Huo, M.H.; Troiano, N.W.; Pelker, R.R.; Gundberg, C.M.; Friedlaender, G.E. The Influence of Ibuprofen on Fracture Repair: Biomechanical, Biochemical, Histologic, and Histomorphometric Parameters in Rats. J. Orthop. Res. 1991, 9, 383–390. [Google Scholar] [CrossRef] [PubMed]
- Henry, J.P.; Bordoni, B. Histology, Osteoblasts. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2020. [Google Scholar]
- Kleinhans, C.; Schmid, F.F.; Schmid, F.V.; Kluger, P.J. Comparison of Osteoclastogenesis and Resorption Activity of Human Osteoclasts on Tissue Culture Polystyrene and on Natural Extracellular Bone Matrix in 2D and 3D. J. Biotechnol. 2015, 205, 101–110. [Google Scholar] [CrossRef] [PubMed]
- James, A.W.; LaChaud, G.; Shen, J.; Asatrian, G.; Nguyen, V.; Zhang, X.; Ting, K.; Soo, C. A Review of the Clinical Side Effects of Bone Morphogenetic Protein-2. Tissue Eng. Part B Rev. 2016, 22, 284–297. [Google Scholar] [CrossRef] [PubMed]
- Ehnert, S.; Aspera-Werz, R.H.; Freude, T.; Reumann, M.K.; Ochs, B.G.; Bahrs, C.; Schröter, S.; Wintermeyer, E.; Nussler, A.K.; Pscherer, S. Distinct Gene Expression Patterns Defining Human Osteoblasts’ Response to BMP2 Treatment: Is the Therapeutic Success All a Matter of Timing? Eur. Surg. Res. 2016, 57, 197–210. [Google Scholar] [CrossRef]
- Konya, V.; Marsche, G.; Schuligoi, R.; Heinemann, A. E-Type Prostanoid Receptor 4 (EP4) in Disease and Therapy. Pharmacol. Ther. 2013, 138, 485–502. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, M.; Sakai, A.; Uchida, S.; Tanaka, S.; Nagashima, M.; Katayama, T.; Yamaguchi, K.; Nakamura, T. Prostaglandin E2 Receptor (EP4) Selective Agonist (ONO-4819.CD) Accelerates Bone Repair of Femoral Cortex after Drill-Hole Injury Associated with Local Upregulation of Bone Turnover in Mature Rats. Bone 2004, 34, 940–948. [Google Scholar] [CrossRef]
- Kirkby Shaw, K.; Rausch-Derra, L.C.; Rhodes, L. Grapiprant: An EP4 Prostaglandin Receptor Antagonist and Novel Therapy for Pain and Inflammation. Vet. Med. Sci. 2016, 2, 3–9. [Google Scholar] [CrossRef]
- Owen, T.A.; Patel, C.; Cahill, A.; Barrett, S.D.; Morano, M.I. Release of the EP4 Receptor Agonist KMN-159 from Scaffolds In Vitro. In Proceedings of the ORS 2020 Annual Meeting, Phoenix, AZ, USA, 8 February 2020; Available online: https://www.caymanchem.com/literature/release-of-the-ep4-receptor-agonist (accessed on 9 November 2021).
- Boerckel, J.D.; Kolambkar, Y.M.; Dupont, K.M.; Uhrig, B.A.; Phelps, E.A.; Stevens, H.Y.; García, A.J.; Guldberg, R.E. Effects of Protein Dose and Delivery System on BMP-Mediated Bone Regeneration. Biomaterials 2011, 32, 5241–5251. [Google Scholar] [CrossRef] [Green Version]
- Zara, J.N.; Siu, R.K.; Zhang, X.; Shen, J.; Ngo, R.; Lee, M.; Li, W.; Chiang, M.; Chung, J.; Kwak, J.; et al. High Doses of Bone Morphogenetic Protein 2 Induce Structurally Abnormal Bone and Inflammation In Vivo. Tissue Eng. Part A 2011, 17, 1389–1399. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Treatment | Animals Operated (n) | Animals for Analysis (n) |
|---|---|---|---|
| 1 | MCM + 50 µg rhBMP-2 | 10 | 10 |
| 2 | MCM + 15 µg KMN-159 | 12 | 12 |
| 3 | MCM + 200 µg KMN-159 | 10 | 10 |
| 4 | MCM + 2 mg KMN-159 | 10 | 9 |
| 5 | MCM + 5 mg KMN-159 | 11 | 10 |
| 6 | MCM + 10 mg KMN-159 | 11 | 10 |
| 50 µg rhBMP-2 | 15 µg KMN-159 | 200 µg KMN-159 | 2 mg KMN-159 | 5 mg KMN-159 | 10 mg KMN-159 | ||
|---|---|---|---|---|---|---|---|
| animals (n) | 10 | 12 | 10 | 9 | 10 | 10 | |
| defect bridging | 10/10 | 0/12 | 0/10 | 3/9 | 1/10 | 1/10 | |
| BV (mm3) | mean ± SD | 115.2 ± 10.6 | 50.6 ± 14.9 | 58.1 ± 24.6 | 76.1 ± 37.1 | 60.5 ± 33.8 | 76.2 ± 15.5 |
| 95% CI | 107.7–122.8 | 41.1–60.0 | 40.5–75.6 | 47.6–104.7 | 36.4–84.7 | 65.2–87.3 | |
| BMD (mgHA/cm3) | mean ± SD | 925 ± 15 | 1072 ± 21 | 1031 ± 27 | 1006 ± 43 | 940 ± 46 | 933 ± 30 |
| 95% CI | 914–936 | 1059–1086 | 1011–1050 | 972–1039 | 908–973 | 911–955 | |
| 50 µg rhBMP-2 | 15 µg KMN-159 | 200 µg KMN-159 | 2 mg KMN-159 | 5 mg KMN-159 | 10 mg KMN-159 | ||
|---|---|---|---|---|---|---|---|
| animals (n) | 10 | 12 | 10 | 9 | 10 | 10 | |
| grade of defect healing | mean ± SD | 10.0 ± 0.1 | 5.2 ± 0.7 | 6.6 ± 1.2 | 7.2 ± 1.4 | 5.8 ± 2.0 | 7.1 ± 0.9 |
| 95% CI | 10.0–10.1 | 5.0–5.4 | 6.1–7.0 | 6.7–7.8 | 5.1–6.6 | 6.8–7.4 | |
| vessels | mean ± SD | 24 ± 37 | 659 ± 497 | 100 ± 69 | 78 ± 64 | 144 ± 85 | 128 ± 105 |
| 95% CI | 0–51 | 343–974 | 50–149 | 28–127 | 83–205 | 52–203 | |
| osteoblasts | mean ± SD | 116 ± 56 | 676 ± 280 | 349 ± 192 | 338 ± 159 | 139 ± 83 | 123 ± 63 |
| 95% CI | 76–156 | 498–854 | 212–486 | 216–460 | 79–198 | 78–168 | |
| osteoclasts | mean ± SD | 25 ± 12 | 48 ± 25 | 14 ± 12 | 22 ± 12 | 38 ± 22 | 34 ± 12 |
| 95% CI | 17–34 | 33–64 | 5–22 | 12–31 | 22–54 | 25–42 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vater, C.; Mehnert, E.; Bretschneider, H.; Bolte, J.; Findeisen, L.; Matuszewski, L.-M.; Zwingenberger, S. Dose-Dependent Effects of a Novel Selective EP4 Prostaglandin Receptor Agonist on Treatment of Critical Size Femoral Bone Defects in a Rat Model. Biomedicines 2021, 9, 1712. https://doi.org/10.3390/biomedicines9111712
Vater C, Mehnert E, Bretschneider H, Bolte J, Findeisen L, Matuszewski L-M, Zwingenberger S. Dose-Dependent Effects of a Novel Selective EP4 Prostaglandin Receptor Agonist on Treatment of Critical Size Femoral Bone Defects in a Rat Model. Biomedicines. 2021; 9(11):1712. https://doi.org/10.3390/biomedicines9111712
Chicago/Turabian StyleVater, Corina, Elisabeth Mehnert, Henriette Bretschneider, Julia Bolte, Lisa Findeisen, Lucas-Maximilian Matuszewski, and Stefan Zwingenberger. 2021. "Dose-Dependent Effects of a Novel Selective EP4 Prostaglandin Receptor Agonist on Treatment of Critical Size Femoral Bone Defects in a Rat Model" Biomedicines 9, no. 11: 1712. https://doi.org/10.3390/biomedicines9111712
APA StyleVater, C., Mehnert, E., Bretschneider, H., Bolte, J., Findeisen, L., Matuszewski, L.-M., & Zwingenberger, S. (2021). Dose-Dependent Effects of a Novel Selective EP4 Prostaglandin Receptor Agonist on Treatment of Critical Size Femoral Bone Defects in a Rat Model. Biomedicines, 9(11), 1712. https://doi.org/10.3390/biomedicines9111712