
Characteristics of Dental Resin-Based Composites in Leukemia Saliva: An In Vitro Analysis

 , ,
, ,  , , , and
, , , and 
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Population and Saliva Sampling
2.2. Resin Based Composite Systems
2.3. Preparation of RBCs Sample in Saliva Samples
2.4. Water Sorption and Solubility
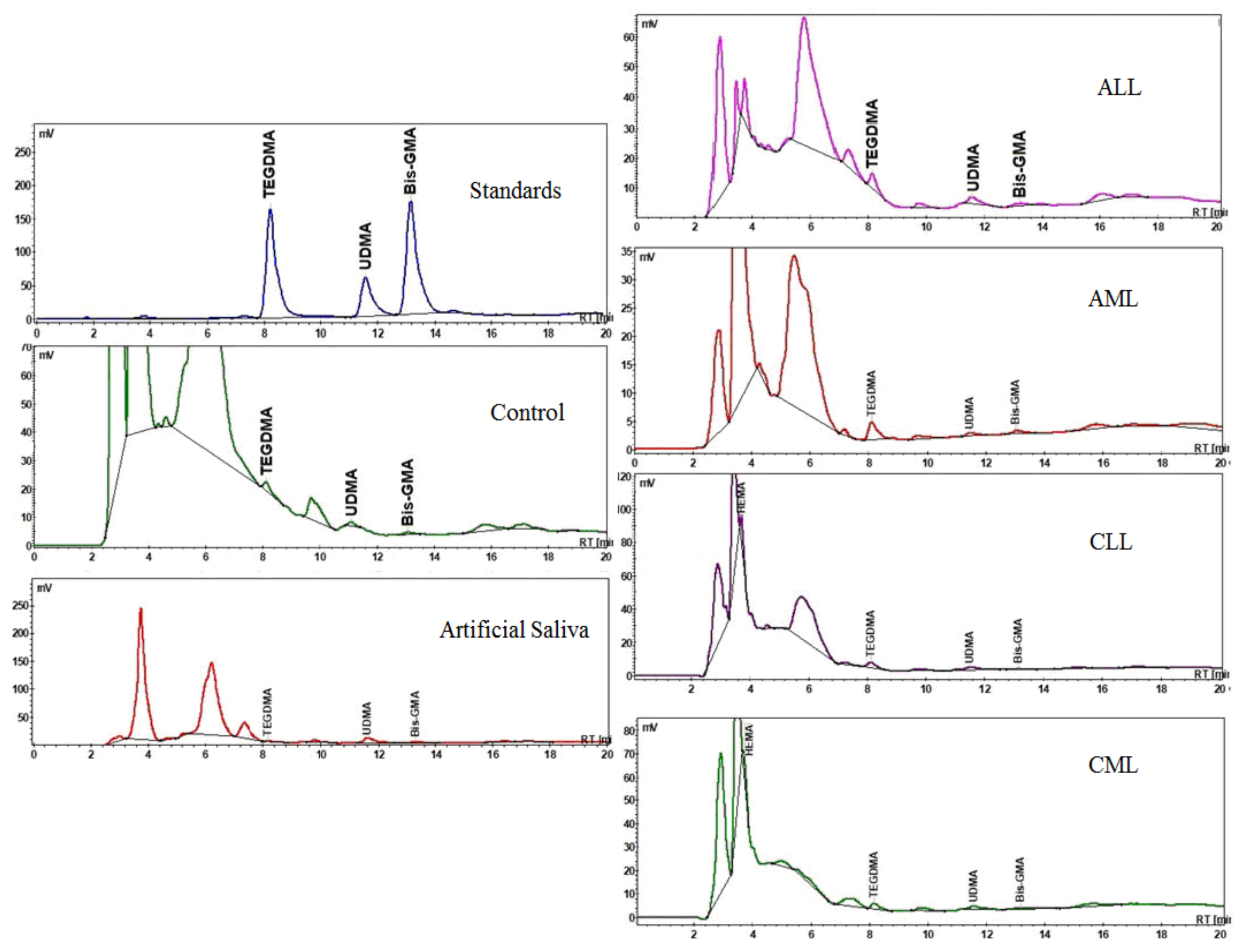
2.5. Residual Monomer
2.6. Scanning Electron Microscopy Analysis
2.7. Statistical Analysis
3. Results
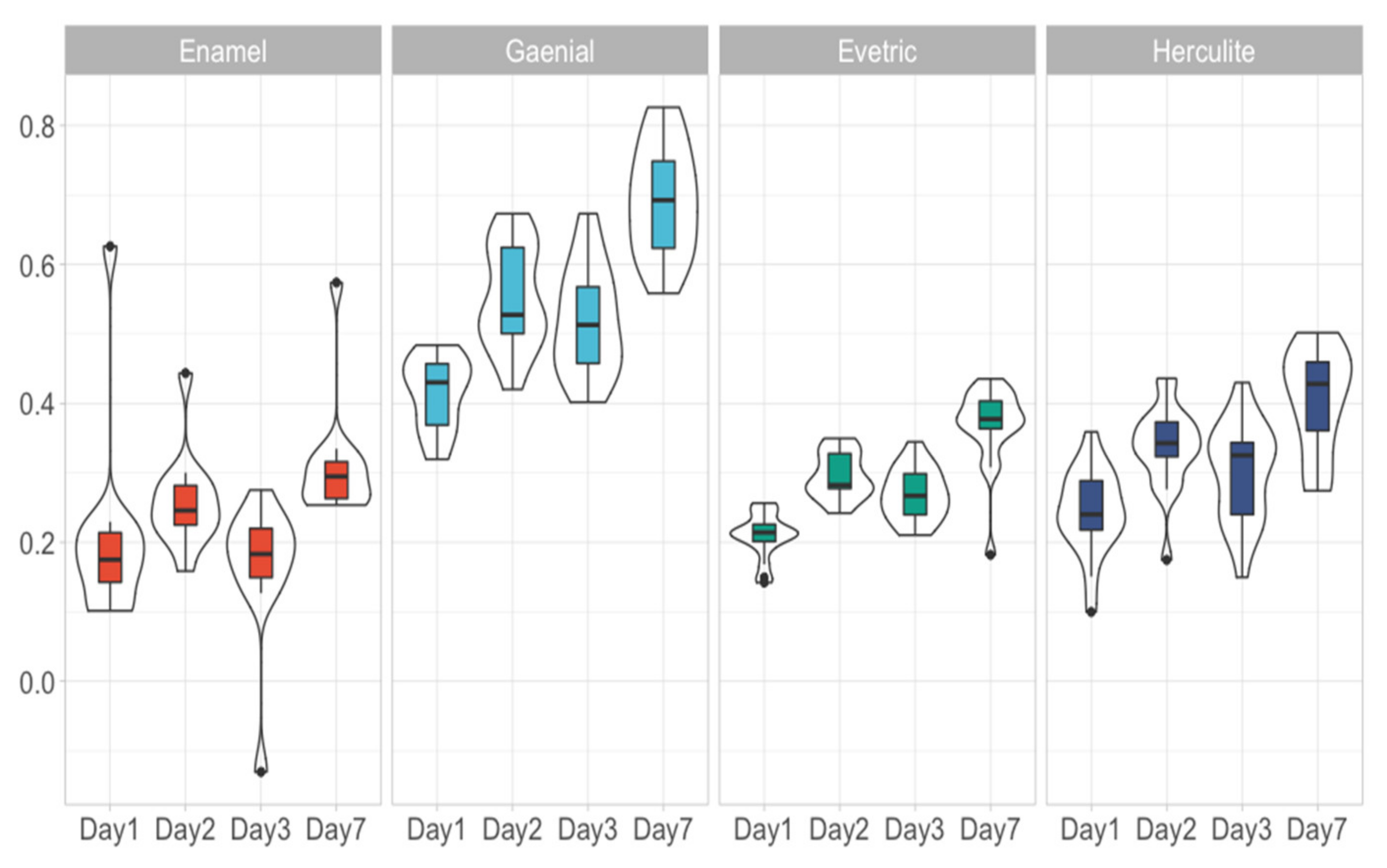
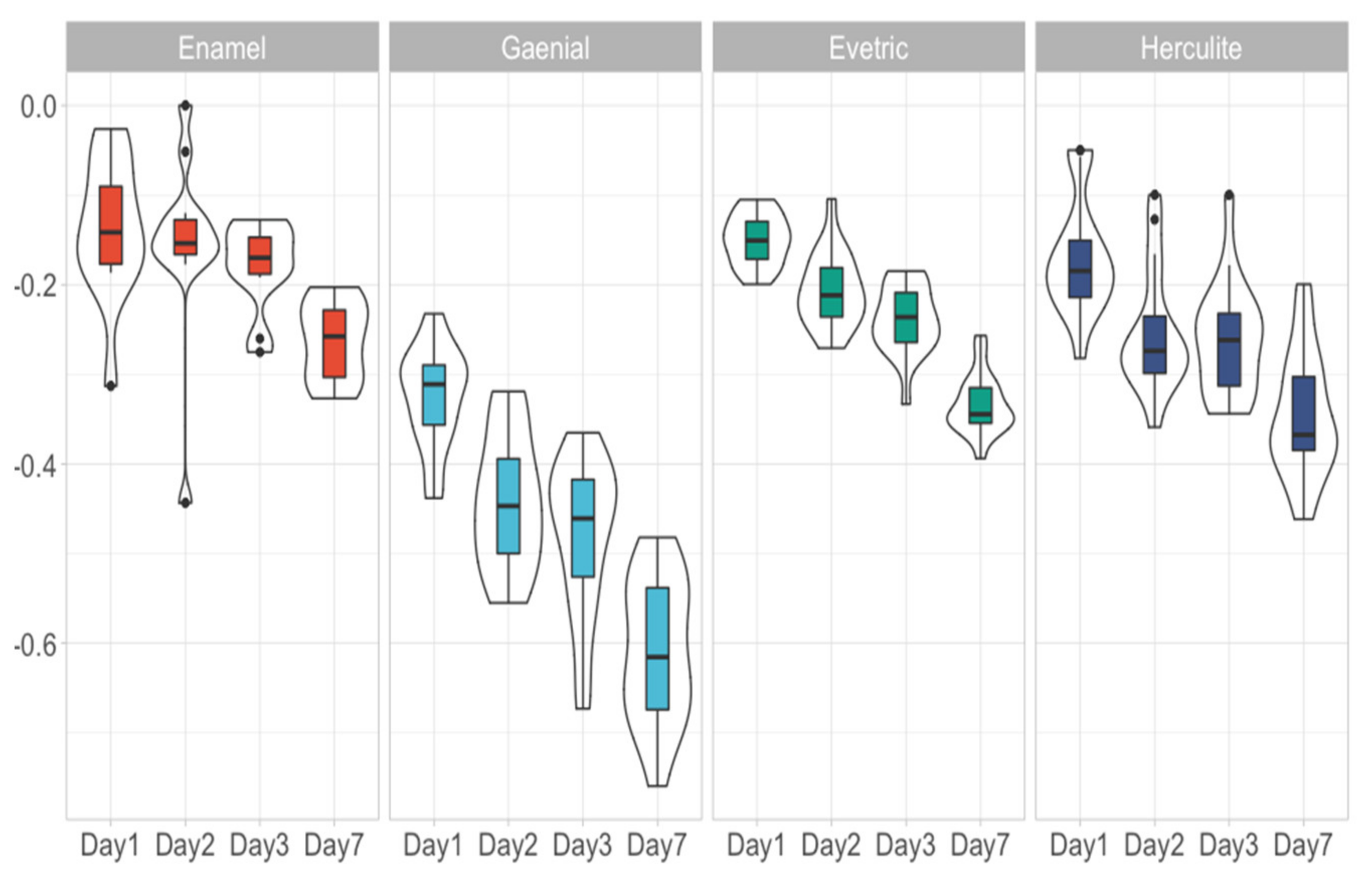
3.1. Water Sorption, Water Solubility and Residual Monomer
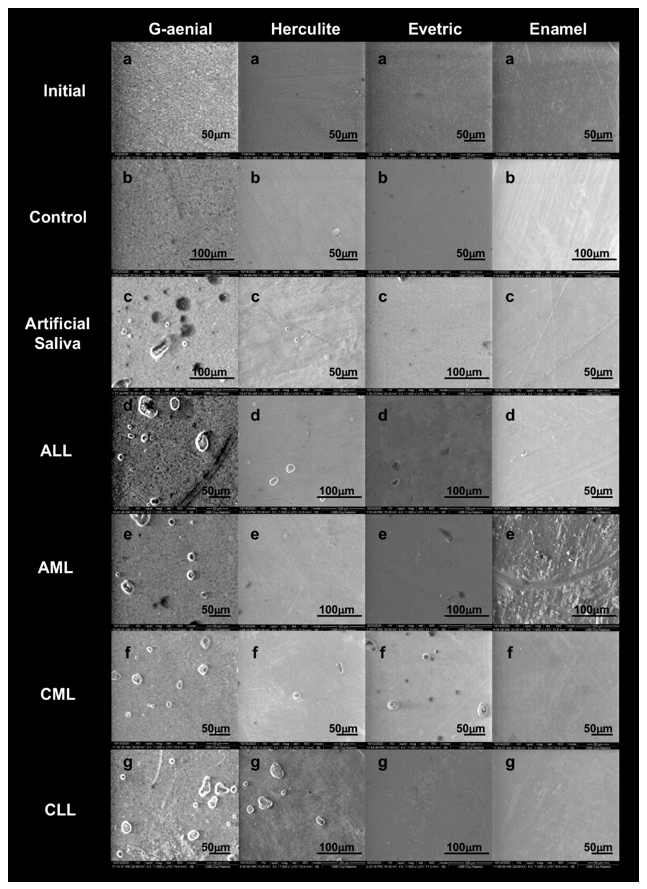
3.2. Scanning Electron Microscopy Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zimmermann, C.; Meurer, M.I.; Grando, L.J.; Gonzaga Del Moral, J.Â.; da Silva Rath, I.B.; Schaefer Tavares, S. Dental treatment in patients with leukemia. J. Oncol. 2015, 2015, 571739. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mester, A.; Irimie, A.; Oprita, L.; Dima, D.; Petrushev, B.; Lucaciu, O.; Campian, R.-S.; Tanase, A. Oral manifestations in stem cell transplantation for acute myeloid leukemia. Med. Hypotheses 2018, 121, 191–194. [Google Scholar] [CrossRef]
- Mester, A.; Irimie, A.I.; Tanase, A.; Tranca, S.; Campian, R.S.; Tomuleasa, C.; Dima, D.; Piciu, A.; Lucaciu, O. Periodontal disease might be a risk factor for graft versus host disease. A systematic review. Crit. Rev. Oncol. Hematol. 2020, 147, 102878. [Google Scholar] [CrossRef] [PubMed]
- Elad, S.; Raber-Durlacher, J.E.; Brennan, M.T.; Saunders, D.P.; Mank, A.P.; Zadik, Y.; Quinn, B.; Epstein, J.B.; Blijlevens, N.M.A.; Waltimo, T.; et al. Basic oral care for hematology-oncology patients and hematopoietic stem cell transplantation recipients: A position paper from the joint task force of the Multinational Association of Supportive Care in Cancer/International Society of Oral Oncology (MASCC). Support. Care Cancer 2015, 23, 223–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Comba, A.; Scotti, N.; Maravić, T.; Mazzoni, A.; Carossa, M.; Breschi, L.; Cadenaro, M. Vickers Hardness and Shrinkage Stress Evaluation of Low and High Viscosity Bulk-Fill Resin Composite. Polymers 2020, 12, 1477. [Google Scholar] [CrossRef]
- Aminoroaya, A.; Esmaeely Neisiany, R.; Nouri Khorasani, S.; Panahi, P.; Das, O.; Ramakrishna, S. A Review of Dental Composites: Methods of Characterizations. ACS Biomater. Sci. Eng. 2020, 6, 3713–3744. [Google Scholar] [CrossRef]
- Ausiello, P.; Cassese, A.; Miele, C.; Beguinot, F.; Garcia-Godoy, F.; Di Jeso, B.; Ulianich, L. Cytotoxicity of dental resin composites: An in vitro evaluation. J. Appl. Toxicol. 2013, 33, 451–457. [Google Scholar] [CrossRef] [PubMed]
- Treglia, A.S.; Turco, S.; Ulianich, L.; Ausiello, P.; Lofrumento, D.D.; Nicolardi, G.; Miele, C.; Garbi, C.; Beguinot, F.; Di Jeso, B. Cell fate following ER stress: Just a matter of “quo ante” recovery or death? Histol. Histopathol. 2012, 27, 1–12. [Google Scholar]
- Șaramet, V.; Meleșcanu-Imre, M.; Țâncu, A.M.C.; Albu, C.C.; Ripszky-Totan, A.; Pantea, M. Molecular Interactions between Saliva and Dental Composites Resins: A Way Forward. Materials 2021, 14, 2537. [Google Scholar] [CrossRef] [PubMed]
- Dentistry—Polymer-Based Filling, Restorative and Luting Materials; ISO 4049:2000; ISO: Geneva, Switzerland, 2000.
- Hegde, A.M.; Joshi, S.; Rai, K.; Shetty, S. Evaluation of oral hygiene status, salivary characteristics and dental caries experience in acute lymphoblastic leukemic (ALL) children. J. Clin. Pediatr. Dent. 2011, 35, 319–323. [Google Scholar] [CrossRef]
- Wang, D.; He, K.; Sroussi, H.; Treister, N.; Luskin, M.; Villa, A.; Woo, S.-B.; Shazib, M.A. Oral myeloid sarcoma as an uncommon manifestation of acute myeloid leukemia: A case series and review of the literature. J. Am. Dent. Assoc. 2021, 152, 393–400.e8. [Google Scholar] [CrossRef] [PubMed]
- Reuter, S.; Gupta, S.C.; Chaturvedi, M.M.; Aggarwal, B.B. Oxidative stress, inflammation, and cancer: How are they linked? Free Radic. Biol. Med. 2010, 49, 1603–1616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pyati, S.A.; Naveen Kumar, R.; Kumar, V.; Praveen Kumar, N.H.; Parveen Reddy, K.M. Salivary Flow Rate, pH, Buffering Capacity, Total Protein, Oxidative Stress and Antioxidant Capacity in Children with and without Dental Caries. J. Clin. Pediatr. Dent. 2018, 42, 445–449. [Google Scholar] [CrossRef]
- Farklı, D.; Materyalinin, K.; Emilim Ve Çözünürlük, S.; Karşılaştırılması, D.; Cangül, S.; Adigüzel, Ö.; Tekin, S.; Öztekin, F.; Satici, Ö. A Comparison of the Water Absorption and Water Solubility Values of Four Different Composite Resin Materials. Cumhur. Dent. J. 2018, 21, 335–342. [Google Scholar]
- Peutzfeldt, A. Resin composites in dentistry: The monomer systems. Eur. J. Oral Sci. 1997, 105, 97–116. [Google Scholar] [CrossRef] [PubMed]
- Sideridou, I.; Tserki, V.; Papanastasiou, G. Study of water sorption, solubility and modulus of elasticity of light-cured dimethacrylate-based dental resins. Biomaterials 2003, 24, 655–665. [Google Scholar] [CrossRef]
- Palin, W.M.; Fleming, G.J.P.; Burke, F.J.T.; Marquis, P.M.; Randall, R.C. The influence of short and medium-term water immersion on the hydrolytic stability of novel low-shrink dental composites. Dent. Mater. 2005, 21, 852–863. [Google Scholar] [CrossRef] [PubMed]
- Ortengren, U.; Andersson, F.; Elgh, U.; Terselius, B.; Karlsson, S. Influence of pH and storage time on the sorption and solubility behaviour of three composite resin materials. J. Dent. 2001, 29, 35–41. [Google Scholar] [CrossRef]
- Ferracane, J.L. Hygroscopic and hydrolytic effects in dental polymer networks. Dent. Mater. 2006, 22, 211–222. [Google Scholar] [CrossRef] [PubMed]
- Fabre, H.S.C.; Fabre, S.; Cefaly, D.F.G.; de Oliveira Carrilho, M.R.; Garcia, F.C.P.; Wang, L. Water sorption and solubility of dentin bonding agents light-cured with different light sources. J. Dent. 2007, 35, 253–258. [Google Scholar] [CrossRef]
- Bettencourt, A.F.; Neves, C.B.; de Almeida, M.S.; Pinheiro, L.M.; e Oliveira, S.A.; Lopes, L.P.; Castro, M.F. Biodegradation of acrylic based resins: A review. Dent. Mater. 2010, 26, e171–e180. [Google Scholar] [CrossRef] [PubMed]
- Kawahara, T.; Nomura, Y.; Tanaka, N.; Teshima, W.; Okazaki, M.; Shintani, H. Leachability of plasticizer and residual monomer from commercial temporary restorative resins. J. Dent. 2004, 32, 277–283. [Google Scholar] [CrossRef] [PubMed]
- Faltermeier, A.; Rosentritt, M.; Müssig, D. Acrylic removable appliances: Comparative evaluation of different postpolymerization methods. Am. J. Orthod. Dentofac. Orthop. 2007, 131, 301.e16–301.e22. [Google Scholar] [CrossRef]
- Santerre, J.P.; Shajii, L.; Leung, B.W. Relation of dental composite formulations to their degradation and the release of hydrolyzed polymeric-resin-derived products. Crit. Rev. Oral Biol. Med. 2001, 12, 136–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Finer, Y.; Santerre, J.P. Salivary esterase activity and its association with the biodegradation of dental composites. J. Dent. Res. 2004, 83, 22–26. [Google Scholar] [CrossRef] [PubMed]
- Lin, B.A.; Jaffer, F.; Duff, M.D.; Tang, Y.W.; Santerre, J.P. Identifying enzyme activities within human saliva which are relevant to dental resin composite biodegradation. Biomaterials 2005, 26, 4259–4264. [Google Scholar] [CrossRef] [PubMed]
- Lempel, E.; Czibulya, Z.; Kunsági-Máté, S.; Szalma, J.; Sümegi, B.; Böddi, K. Quantification of Conversion Degree and Monomer Elution from Dental Composite Using HPLC and Micro-Raman Spectroscopy. Chromatographia 2014, 77, 1137–1144. [Google Scholar] [CrossRef]
- Craciun, A.; Prodan, D.; Constantiniuc, M.; Ispas, A.; Filip, M.; Moldovan, M.; Badea, M.; Petean, I.; Crisan, M. Stability of dental composites in water and artificial saliva. Mater. Plast. 2020, 57, 57–66. [Google Scholar] [CrossRef]
- Manso, A.P.; Carvalho, R.M. Dental Cements for Luting and Bonding Restorations: Self-Adhesive Resin Cements. Dent. Clin. North Am. 2017, 61, 821–834. [Google Scholar] [CrossRef] [PubMed]
- Figuerôa, R.M.S.; Conterno, B.; Arrais, C.A.G.; Sugio, C.Y.C.; Urban, V.M.; Neppelenbroek, K.H. Porosity, water sorption and solubility of denture base acrylic resins polymerized conventionally or in microwave. J. Appl. Oral Sci. 2018, 26, e20170383. [Google Scholar] [CrossRef] [PubMed]
- Sahibzada, H.A.; Khurshid, Z.; Khan, R.S.; Naseem, M.; Siddique, K.M.; Mali, M.; Zafar, M.S. Salivary IL-8, IL-6 and TNF-α as Potential Diagnostic Biomarkers for Oral Cancer. Diagnostics 2017, 7, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costantini, E.; Sinjari, B.; Piscopo, F.; Porreca, A.; Reale, M.; Caputi, S.; Murmura, G. Evaluation of Salivary Cytokines and Vitamin D Levels in Periodontopathic Patients. Int. J. Mol. Sci. 2020, 21, 2669. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Addazio, G.; Artese, L.; Traini, T.; Rubini, C.; Caputi, S.; Sinjari, B. Immunohistochemical study of osteopontin in oral squamous cell carcinoma allied to fractal dimension. J. Biol. Regul. Homeost. Agents 2018, 32, 1033–1038. [Google Scholar] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Composite | Resins | Fillers |
|---|---|---|
| G-aenial Anterior A2,GC corporation, Tokyo, Japan | UDMA, dimethacrylate co-monomers (Bis-GMA) (37%) | Pre-polymerized fillers containing silica (19–17 µ), pre-polymerized particles containing strontium (400 nm) and lanthanoid fluoride (100 nm), silica (16 nm), fumed silica (63%) |
| Herculite XRV Ultra A2; Kerr; Italy | Bis-GMA, TEGDMA (41%) | Al-B-Si glass, SiO2 (59% by volume, particles 0.6 microns) |
| Evetric filling material A2, Ivoclar Vivadent | Dimethacrylates (19–20%) | Barium glass, ytterbium trifluoride, mixed oxide, copolymers (80–81 wt.%; 55–57 vol.%, size 40–3000 nm)), additives, catalysts, stabilizers, pigments (80%) |
| Enamel Plus HRi, UD2, Micerium | UDMA, BisGMA, 1,4-butandiol-dimethacrylate (45%) | Glass filler (0.7 µ), highly dispersed silicone dioxide (0.04 µ) (55%) |
| Material | Day | Measured | p-Value | Measured | p-Value |
|---|---|---|---|---|---|
| Gaenial | Day1 | Water Sorption | 0.708 | Water Solubility | 0.632 |
| Gaenial | Day2 | Water Sorption | 0.174 | Water Solubility | 0.098 |
| Gaenial | Day3 | Water Sorption | 0.188 | Water Solubility | 0.012 |
| Gaenial | Day7 | Water Sorption | 0.065 | Water Solubility | 0.304 |
| Herculite | Day1 | Water Sorption | 0.315 | Water Solubility | 0.467 |
| Herculite | Day2 | Water Sorption | 0.404 | Water Solubility | 0.184 |
| Herculite | Day3 | Water Sorption | 0.154 | Water Solubility | 0.218 |
| Herculite | Day7 | Water Sorption | 0.199 | Water Solubility | 0.132 |
| Evetric | Day1 | Water Sorption | 0.073 | Water Solubility | 0.060 |
| Evetric | Day2 | Water Sorption | 0.415 | Water Solubility | 0.060 |
| Evetric | Day3 | Water Sorption | 0.160 | Water Solubility | 0.131 |
| Evetric | Day7 | Water Sorption | 0.904 | Water Solubility | 0.451 |
| Enamel | Day1 | Water Sorption | 0.669 | Water Solubility | 0.481 |
| Enamel | Day2 | Water Sorption | 0.705 | Water Solubility | 0.129 |
| Enamel | Day3 | Water Sorption | 0.133 | Water Solubility | 0.005 |
| Enamel | Day7 | Water Sorption | 0.680 | Water Solubility | 0.809 |
| Variable | Day | Measured | Enamel | Evetric | G-aenial |
|---|---|---|---|---|---|
| Evetric | Day 1 | Water Sorption | 0.623 | NA | NA |
| Gaenial | Day 1 | Water Sorption | <0.001 | <0.0001 | NA |
| Herculite | Day 1 | Water Sorption | 0.079 | 0.123 | <0.0001 |
| Evetric | Day 2 | Water Sorption | 0.102 | NA | NA |
| G-aenial | Day 2 | Water Sorption | <0.0001 | <0.0001 | NA |
| Herculite | Day 2 | Water Sorption | <0.01 | 0.025 | <0.0001 |
| Evetric | Day 3 | Water Sorption | <0.001 | NA | NA |
| G-aenial | Day 3 | Water Sorption | <0.0001 | <0.0001 | NA |
| Herculite | Day 3 | Water Sorption | <0.001 | 0.709 | <0.0001 |
| Evetric | Day 7 | Water Sorption | <0.01 | NA | NA |
| G-aenial | Day 7 | Water Sorption | <0.0001 | <0.0001 | NA |
| Herculite | Day 7 | Water Sorption | 0.014 | 0.411 | <0.0001 |
| Evetric | Day 1 | Water Solubility | 1 | NA | NA |
| G-aenial | Day 1 | Water Solubility | <0.0001 | <0.0001 | NA |
| Herculite | Day 1 | Water Solubility | 0.68 | 0.382 | <0.0001 |
| Evetric | Day 2 | Water Solubility | <0.01 | NA | NA |
| G-aenial | Day 2 | Water Solubility | <0.0001 | <0.0001 | NA |
| Herculite | Day 2 | Water Solubility | 0.012 | 0.031 | <0.0001 |
| Evetric | Day 3 | Water Solubility | <0.01 | NA | NA |
| G-aenial | Day 3 | Water Solubility | <0.0001 | <0.0001 | NA |
| Herculite | Day 3 | Water Solubility | 0.011 | 0.773 | <0.0001 |
| Evetric | Day 7 | Water Solubility | <0.001 | NA | NA |
| G-aenial | Day 7 | Water Solubility | <0.0001 | <0.0001 | NA |
| Herculite | Day 7 | Water Solubility | 0.012 | 1 | <0.0001 |
| Material | Measured | p-Value | Tau |
|---|---|---|---|
| G-aenial | Water Sorption | <0.0001 | 0.58 |
| Herculite | Water Sorption | <0.0001 | 0.44 |
| Evetric | Water Sorption | <0.0001 | 0.56 |
| Enamel | Water Sorption | <0.01 | 0.36 |
| G-aenial | Water Solubility | <0.0001 | −0.65 |
| Herculite | Water Solubility | <0.0001 | −0.54 |
| Evetric | Water Solubility | <0.0001 | −0.73 |
| Enamel | Water Solubility | <0.0001 | −0.48 |
| Sample | TEGDMA [%] × 10−6 | UDMA [%] × 10−6 | Bis-GMA [%] × 10−6 | Total Residual Monomer × 10−6 |
|---|---|---|---|---|
| Artificial saliva | 4.881776707 | 5.94775482 | 2.900303374 | 13.729833488 |
| Control | 6.61202044 | 5.567923011 | 1.795024772 | 13.97496822 |
| ALL | 13.64720043 | 5.478786195 | 2.502141055 | 21.62812768 |
| AML | 16.9537037 | 29.26157407 | 4.212962963 | 50.42824074 |
| CLL | 4.609006307 | 7.747100075 | 2.355224276 | 14.71133066 |
| CML | 7.051773396 | 21.27610155 | 1.435440039 | 29.76331498 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mester, A.; Moldovan, M.; Cuc, S.; Tomuleasa, C.; Pasca, S.; Filip, M.; Piciu, A.; Onisor, F. Characteristics of Dental Resin-Based Composites in Leukemia Saliva: An In Vitro Analysis. Biomedicines 2021, 9, 1618. https://doi.org/10.3390/biomedicines9111618
Mester A, Moldovan M, Cuc S, Tomuleasa C, Pasca S, Filip M, Piciu A, Onisor F. Characteristics of Dental Resin-Based Composites in Leukemia Saliva: An In Vitro Analysis. Biomedicines. 2021; 9(11):1618. https://doi.org/10.3390/biomedicines9111618
Chicago/Turabian StyleMester, Alexandru, Marioara Moldovan, Stanca Cuc, Ciprian Tomuleasa, Sergiu Pasca, Miuta Filip, Andra Piciu, and Florin Onisor. 2021. "Characteristics of Dental Resin-Based Composites in Leukemia Saliva: An In Vitro Analysis" Biomedicines 9, no. 11: 1618. https://doi.org/10.3390/biomedicines9111618
APA StyleMester, A., Moldovan, M., Cuc, S., Tomuleasa, C., Pasca, S., Filip, M., Piciu, A., & Onisor, F. (2021). Characteristics of Dental Resin-Based Composites in Leukemia Saliva: An In Vitro Analysis. Biomedicines, 9(11), 1618. https://doi.org/10.3390/biomedicines9111618