
Malignancy and Inflammatory Bowel Disease (IBD): Incidence and Prevalence of Malignancy in Correlation to IBD Therapy and Disease Activity—A Retrospective Cohort Analysis over 5 Years


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Statistical Analysis
3. Results
3.1. Patient Cohort
3.2. IBD and Cancer
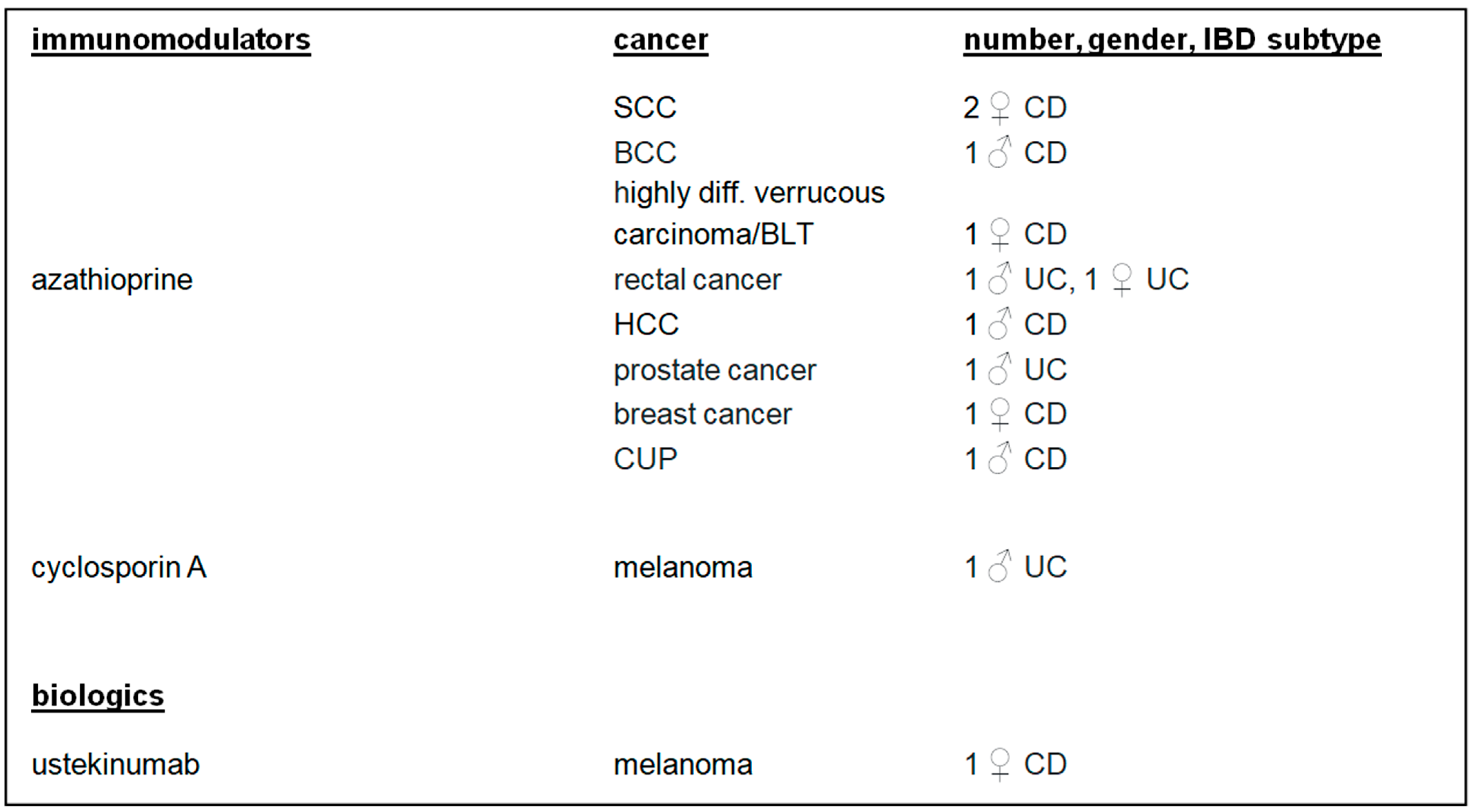
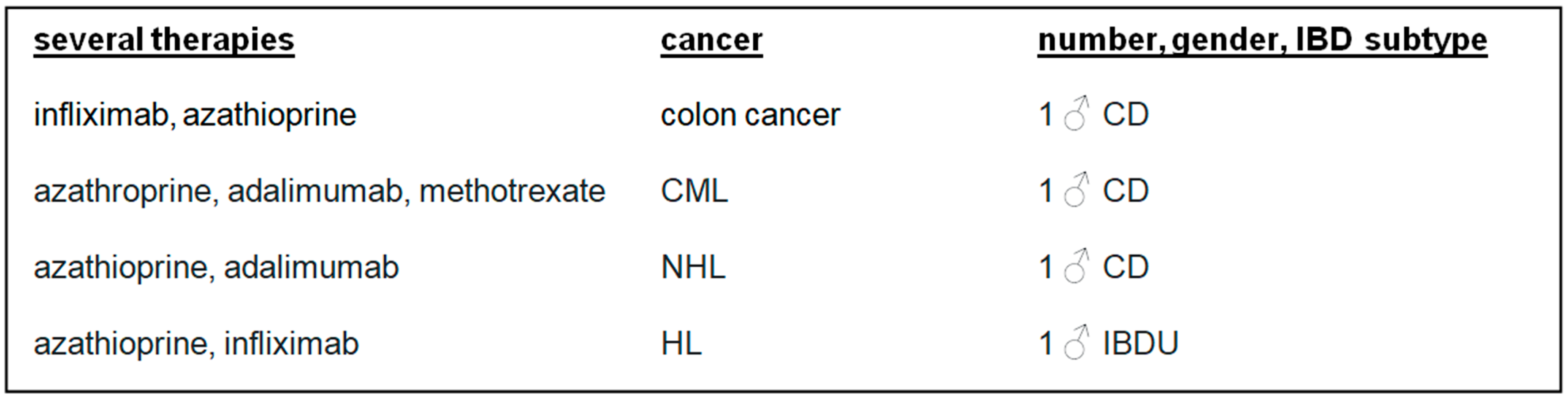
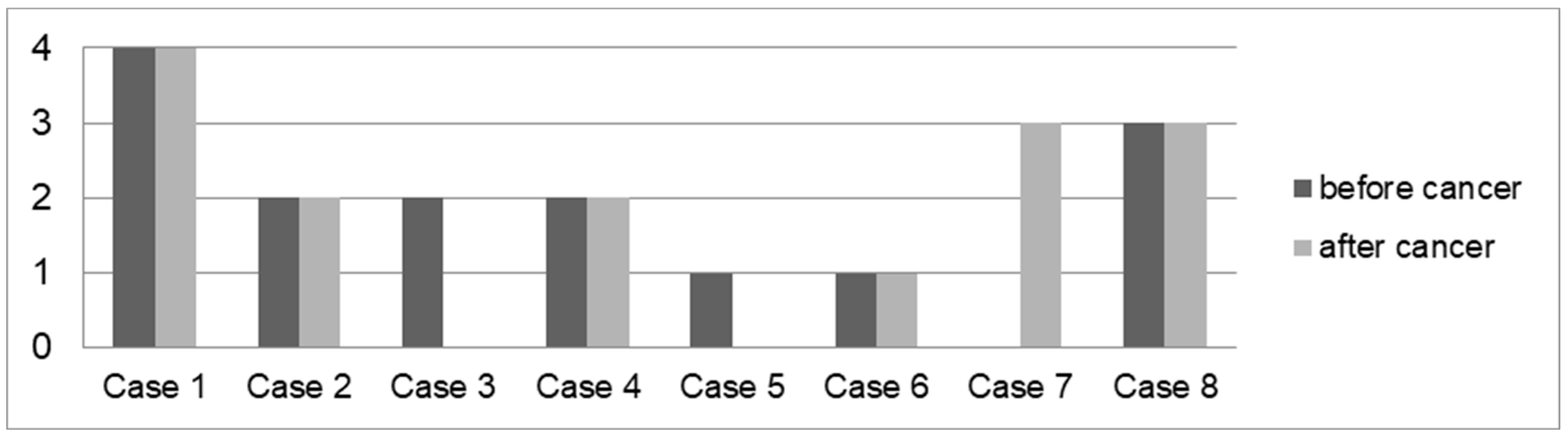
3.3. Cancer and IBD Therapy
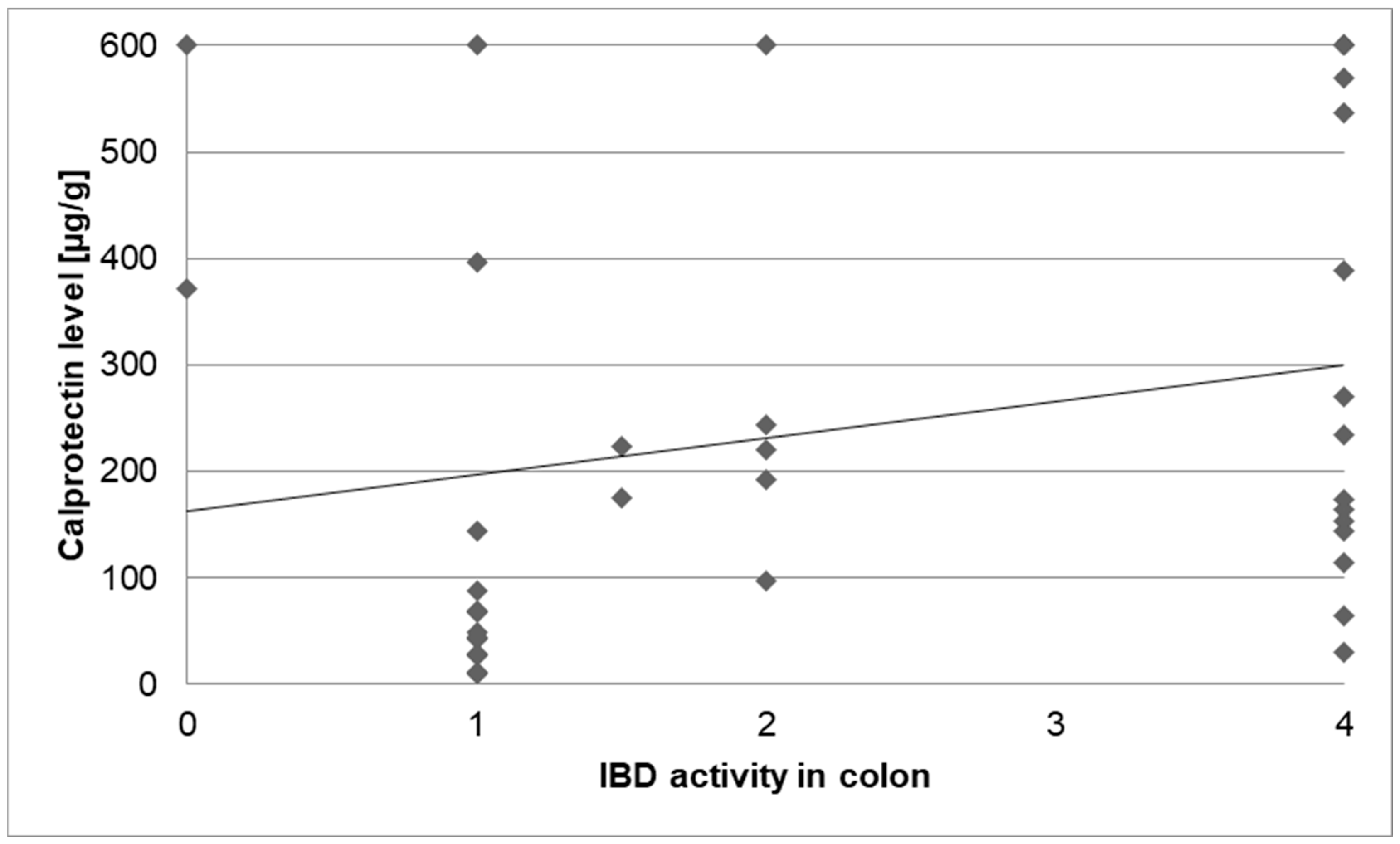
3.4. IBD Activity
4. Discussion
4.1. Patients with IBD and Cancer
4.2. Cancer Subtypes in Patients with IBD
4.3. Second Cancer in Patients with IBD
4.4. Cancer in IBD and Concomitant Medication
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AML | acute myeloid leukaemia (AML) |
| BCC | basal-cell carcinoma |
| BLT | Buschke–Löwenstein tumour |
| CD | Crohn’s disease |
| CML | chronic myeloid leukaemia |
| CUP | cancer of unknown primary |
| DGVS | German Society for Digestive and Metabolic Diseases; Deutsche Gesellschaft für Gastroenterologie, Verdauungs- und Stoffwechselkrankheiten |
| ECCO | European Crohn’s and Colitis Organisation |
| HL | Hodgkin lymphoma |
| HR | hazard ratio |
| HCC | hepatocellular carcinoma |
| IBD | inflammatory bowel disease |
| IBDU | inflammatory bowel disease unclassified |
| IQR | interquartile range |
| NET | neuroendocrine tumour |
| NHL | non-Hodgkin lymphoma |
| PBC | primary biliary cholangitis |
| PSC | primary sclerosing cholangitis |
| SD | standard deviation |
| SCC | squamous cell carcinoma |
| UC | ulcerative colitis |
References
- Seyedian, S.S.; Nokhostin, F.; Malamir, M.D. A review of the diagnosis, prevention, and treatment methods of inflammatory bowel disease. J. Med. Life 2019, 12, 113–122. [Google Scholar] [CrossRef] [PubMed]
- Olén, O.; Askling, J.; Sachs, M.; Frumento, P.; Neovius, M.; Smedby, K.; Ekbom, A.; Malmborg, P.; Ludvigsson, J. Childhood onset inflammatory bowel disease and risk of cancer: A Swedish nationwide cohort study 1964–2014. BMJ 2017, 358, j3951. [Google Scholar] [CrossRef] [PubMed]
- Wehkamp, J.; Götz, M.; Herrlinger, K.; Steurer, W.; Stange, E.F. Inflammatory Bowel Disease. Dtsch. Arztebl. Int. 2016, 113, 72–82. [Google Scholar] [CrossRef] [PubMed]
- Medycyna, P. (Ed.) Interna Szczeklika: Podręcznik Chorób Wewnętrznych; Medycyna Praktyczna: Kraków, Polen, 2014. [Google Scholar]
- Messmann, H.; Andus, T.; Baum, K. (Eds.) Klinische Gastroenterologie: Das Buch Für Fort-Und Weiterbildung; plus DVD mit über 1400 Befunden; 312 Tabellen; inklusive DVD.; Thieme: Stuttgart, Deutschland, 2012; 817p. [Google Scholar]
- Prelipcean, C.C.; Mihai, C.; Gogalniceanu, P.; Mihai, B. What is the Impact of Age on Adult Patients with Inflammatory Bowel Disease? Clujul Med. 2013, 86, 3–9. [Google Scholar] [PubMed] [PubMed Central]
- de Weerth, A.; Bläker, M. Chronisch-Entzündliche Darmerkrankungen. Hambg. Ärzteblatt 2016, 70, 12–17. [Google Scholar]
- Peppercorn, M.A.; Cheifetz, A.S. Definitions, Epidemiology, and Risk Factors for Inflammatory Bowel Disease in Adults. 2019. Available online: https://www.uptodate.com/contents/definitions-epidemiology-and-risk-factors-for-inflammatory-bowel-disease (accessed on 13 May 2025).
- Friedman, G.; Bitton, A. Overview of Hepatobiliary Disorders in Patients with Inflammatory Bowel Disease. 2020. Available online: https://www.uptodate.com/contents/overview-of-hepatobiliary-disorders-in-patients-with-inflammatory-bowel-disease (accessed on 8 July 2024).
- Lo, B.Z.S.; Zhao, M.; Vind, I.; Burisch, J. The risk of extra-intestinal cancer in inflammatory bowel disease (IBD): A systematic review and meta-analysis of population-based cohort studies. J. Crohn’s Colitis 2020, 14, S082. [Google Scholar] [CrossRef]
- Zisman, T.L.; Rubin, D.T. Colorectal cancer and dysplasia in inflammatory bowel disease. World J. Gastroenterol. 2008, 14, 2662–2669. [Google Scholar] [CrossRef] [PubMed]
- Timeus, S.; Laoun, R. Risk of colorectal cancer and other malignancies in association with the use of thiopurines, tumour necrosis factor antagonists or mesalazine. J. Crohn’s Colitis 2020, 14, S496–S497. [Google Scholar] [CrossRef]
- Horio, Y.; Uchino, M.; Bando, T.; Sasaki, H.; Goto, Y.; Kuwahara, R.; Minagawa, T.; Takesue, Y.; Ikeuchi, H. Incidence, Risk Factors and Outcomes of Cancer of the Anal Transitional Zone in Patients with Ulcerative Colitis. J. Crohn’s Colitis 2020, 14, 1565–1571. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Z.; Mei, Z.; Guo, Y.; Wang, G.; Wu, T.; Cui, X.; Huang, Z.; Zhu, Y.; Wen, D.; Song, J.; et al. Reduced Risk of Inflammatory Bowel Disease-associated Colorectal Neoplasia with Use of Thiopurines: A Systematic Review and Metaanalysis. J. Crohn’s Colitis 2018, 12, 546–558. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.R.; Chang, D.K. Colorectal cancer in inflammatory bowel disease: The risk, pathogenesis, prevention and diagnosis. World J. Gastroenterol. 2014, 20, 9872–9881. [Google Scholar] [CrossRef] [PubMed]
- Beaugerie, L.; Svrcek, M.; Seksik, P.; Bouvier, A.; Simon, T.; Allez, M.; Brixi, H.; Gornet, J.; Altwegg, R.; Beau, P.; et al. Risk of colorectal high-grade dysplasia and cancer in a prospective observational cohort of patients with inflammatory bowel disease. Gastroenterology 2013, 145, 166–175. [Google Scholar] [CrossRef] [PubMed]
- Kucharzik, T.; Dignass, A.U.; Atreya, R.; Bokemeyer, B.; Esters, P.; Herrlinger, K.; Kannengießer, K.; Kienle, P.; Langhorst, J.; Lügering, A.; et al. Aktualisierte S3-Leitlinie Colitis ulcerosa—Living Guideline. Z. Für Gastroenterologie 2020, 58, e241–e326. [Google Scholar] [CrossRef] [PubMed]
- Dyson, J.K.; Rutter, M.D. Colorectal cancer in inflammatory bowel disease: What is the real magnitude of the risk? World J Gastroenterol. 2012, 18, 3839–3848. [Google Scholar] [CrossRef] [PubMed]
- Pinczowski, D.; Ekbom, A.; Baron, J.; Yuen, J.; Adami, H.-O. Risk factors for colorectal cancer in patients with ulcerative colitis: A case-control study. Gastroenterology 1994, 107, 117–120. [Google Scholar] [CrossRef]
- Jackson, S.S.; Marks, M.A.; Katki, H.A.; Cook, M.B.; Hyun, N.; Freedman, N.D.; Kahle, L.L.; Castle, P.E.; Graubard, B.I.; Chaturvedi, A.K. Sex disparities in the incidence of 21 cancer types: Quantification of the contribution of risk factors. Cancer 2022, 128, 3531–3540. [Google Scholar] [CrossRef] [PubMed]
- Jung, Y.S.; Han, M.; Park, S.; Kim, W.H.; Cheon, J.H. Cancer Risk in the Early Stages of Inflammatory Bowel Disease in Korean Patients: A Nationwide Population-based Study. J. Crohn’s Colitis 2017, 11, 954–962. [Google Scholar] [CrossRef] [PubMed]
- Annese, V.; Beaugerie, L.; Egan, L.; Biancone, L.; Bolling, C.; Brandts, C.; Dierickx, D.; Dummer, R.; Fiorino, G.; Gornet, J.M.; et al. European Evidence-based Consensus: Inflammatory Bowel Disease and Malignancies. J. Crohn’s Colitis 2015, 9, 945–965. [Google Scholar] [CrossRef] [PubMed]
- Axelrad, J.; Olen, O.; Sachs, M.; Erichsen, R.; Pedersen, L.; Halfvarson, J.; Askling, J.; Ekbom, A.; Sørensen, H.T.; Ludvigsson, J. Inflammatory bowel disease and risk of small bowel cancer: A binational population-based cohort study from Denmark and Sweden. J. Crohn’s Colitis 2020, 14, S007–S009. [Google Scholar] [CrossRef]
- Fields, A.C.; Hu, F.Y.; Lu, P.; Irani, J.; Bleday, R.; Goldberg, J.E.; Melnitchouk, N. Small Bowel Adenocarcinoma: Is There a Difference in Survival for Crohn’s Versus Sporadic Cases? J. Crohn’s Colitis 2020, 14, 303–308. [Google Scholar] [CrossRef] [PubMed]
- Kannengiesser, K.; Torsten, K. Begleiterkrankungen bei CED Onkologische Fragen CED und Krebserkrankungen. Bauchredner 2018, 1, 2–7. [Google Scholar]
- Preiß, J.C.; Bokemeyer, B.; Buhr, H.J.; Dignaß, A.; Häuser, W.; Hartmann, F.; Herrlinger, K.R.; Kaltz, B.; Kienle, P.; Kruis, W.; et al. Aktualisierte S3-Leitlinie—”Diagnostik und Therapie des Morbus Crohn” 2014. Z. Für Gastroenterol. 2014, 52, 1431–1484. [Google Scholar] [CrossRef] [PubMed]
- Tassone, D.; Ding, N. A review of adverse events associated with immunosuppressive treatments in inflammatory bowel disease patients. J. Crohn’s Colitis 2020, 14, S453–S454. [Google Scholar] [CrossRef]
- A-Rahim, Y.I.; Farrell, R.J. Overview of Azathioprine and Mercaptopurine Use in Inflammatory Bowel Disease. 2019. Available online: http://112.2.34.14:9095/contents/overview-of-azathioprine-and-mercaptopurine-use-in-inflammatory-bowel-disease (accessed on 19 April 2024).
- Muller, M.; D’Amico, F.; Bonovas, S.; Danese, S.; Peyrin-Biroulet, L. TNF inhibitors and risk of malignancy in patients with inflammatory bowel diseases: A systematic review. J. Crohn’s Colitis 2020, 15, 840–859. [Google Scholar] [CrossRef] [PubMed]
- Hashash, J.A.; Regueito, M. Medical Management of Low-Risk Adult Patients with Mild to Moderate Ulcerative Colitis. 2019. Available online: https://www.uptodate.com/contents/medical-management-of-low-risk-adult-patients-with-mild-to-moderate-ulcerative-colitis (accessed on 22 May 2025).
- Sturm, A.; Atreya, R.; Bettenworth, D.; Bokemeyer, B.; Dignaß, A.; Ehehalt, R.; Germer, C.; Grunert, P.C.; Helwig, U.; Herrlinger, K.; et al. Aktualisierte S3-Leitlinie “Diagnostik und Therapie des Morbus Crohn” der Deutschen Gesellschaft für Gastroenterologie, Verdauungs- und Stoffwechselkrankheiten (DGVS)-August 2021-AWMF-Registernummer: 021-004. Z. Für Gastroenterol. 2022, 60, 332–418. [Google Scholar]
- Bongartz, T.; Sutton, A.J.; Sweeting, M.J.; Buchan, I.; Matteson, E.L.; Montori, V. Anti-TNF Antibody Therapy in rheumatoid arthritis and the risk of serious infections and malignancies: Systematic Review and Meta-analysis of rare harmful effects in randomized controlled trials. JAMA 2006, 295, 2275–2482. [Google Scholar] [CrossRef]
- Hyams, J.S.; Dubinsky, M.C.; Baldassano, R.N.; Colletti, R.B.; Cucchiara, S.; Escher, J.; Faubion, W.; Fell, J.; Gold, B.D.; Griffiths, A.; et al. Infliximab Is Not Associated With Increased Risk of Malignancy or Hemophagocytic Lymphohistiocytosis in Pediatric Patients With Inflammatory Bowel Disease. Gastroenterology 2017, 152, 1901–1914. [Google Scholar] [CrossRef] [PubMed]
- Kucharzik, T.; Koletzko, S.; Kannengießer, K.; Dignaß, A. Colitis ulcerosa—Diagnostische und therapeutische Algorithmen. Dtsch. Aerzteblatt Online 2020, 117, 564–574. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Macroscopic IBD Activity in Colon | Grade |
|---|---|
| No | 0 |
| Low | 1 |
| Mild | 2 |
| Significant | 3 |
| Pronounced | 4 |
| Hazard Ratio (HR) | Confidence Interval | p-Value | ||
|---|---|---|---|---|
| Lower Bound | Upper Bound | |||
| Gender: men | 2.412 | 0.914 | 6.367 | 0.075 |
| Age | 0.939 | 0.873 | 1.01 | 0.093 |
| Age at IBD diagnosis | 1.088 | 1.011 | 1.171 | 0.025 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kafel, A.J.; Muzalyova, A.; Schnoy, E. Malignancy and Inflammatory Bowel Disease (IBD): Incidence and Prevalence of Malignancy in Correlation to IBD Therapy and Disease Activity—A Retrospective Cohort Analysis over 5 Years. Biomedicines 2025, 13, 1395. https://doi.org/10.3390/biomedicines13061395
Kafel AJ, Muzalyova A, Schnoy E. Malignancy and Inflammatory Bowel Disease (IBD): Incidence and Prevalence of Malignancy in Correlation to IBD Therapy and Disease Activity—A Retrospective Cohort Analysis over 5 Years. Biomedicines. 2025; 13(6):1395. https://doi.org/10.3390/biomedicines13061395
Chicago/Turabian StyleKafel, Agnieszka Jowita, Anna Muzalyova, and Elisabeth Schnoy. 2025. "Malignancy and Inflammatory Bowel Disease (IBD): Incidence and Prevalence of Malignancy in Correlation to IBD Therapy and Disease Activity—A Retrospective Cohort Analysis over 5 Years" Biomedicines 13, no. 6: 1395. https://doi.org/10.3390/biomedicines13061395
APA StyleKafel, A. J., Muzalyova, A., & Schnoy, E. (2025). Malignancy and Inflammatory Bowel Disease (IBD): Incidence and Prevalence of Malignancy in Correlation to IBD Therapy and Disease Activity—A Retrospective Cohort Analysis over 5 Years. Biomedicines, 13(6), 1395. https://doi.org/10.3390/biomedicines13061395