
Clinical Utility of Trabecular Bone Score in Gastroenterology: A Narrative Review


Abstract
1. Introduction
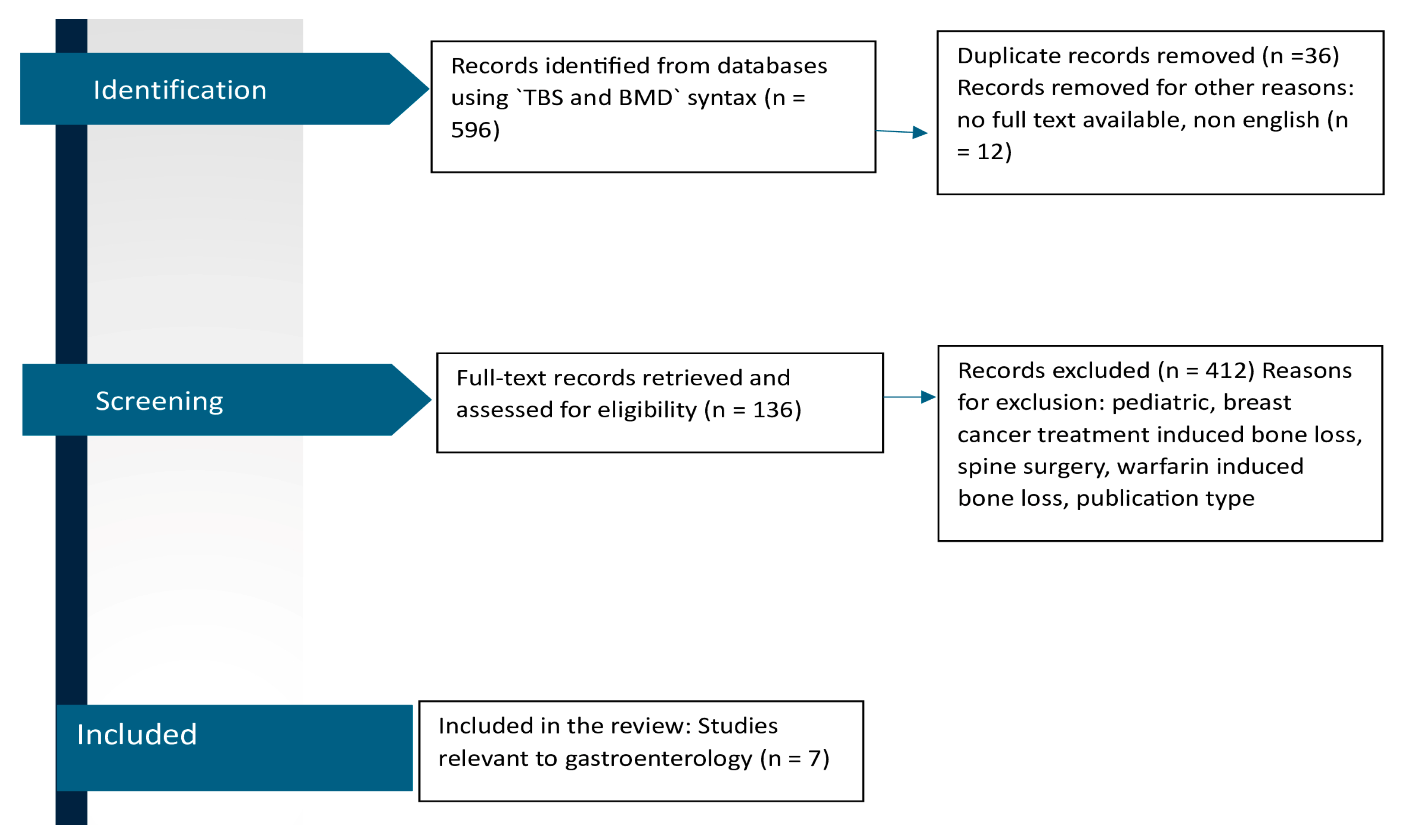
2. Materials and Methods
3. Results
3.1. TBS and IBD
3.2. TBS and Cirrhosis
3.3. TBS and Chronic Atrophic Gastritis
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| IBD | inflammatory bowel disease |
| EIMs | extra-intestinal manifestations |
| BMD | bone mineral density |
| DXA | dual-energy X-ray absorptiometry |
| TBS | trabecular bone score |
| PTH | parathyroid hormone |
| MASLD | metabolic-dysfunction-associated steatotic liver disease |
| CAG | chronic atrophic gastritis |
| UC | ulcerative colitis |
| CD | Crohn’s disease |
| WHO | World Health Organization |
| ISCD | The International Society for Clinical Densitometry |
| EoE | eosinophilic esophagitis |
References
- Larsen, S.; Bendtzen, K.; Nielsen, O.H. Extraintestinal manifestations of inflammatory bowel disease: Epidemiology, diagnosis, and management. Ann. Med. 2010, 42, 97–114. [Google Scholar] [CrossRef]
- Roda, G.; Ng, S.C.; Kotze, P.G.; Argollo, M.; Panaccione, R.; Spinelli, A.; Kaser, A.; Peyrin-Biroulet, L.; Danese, S. Crohn’s disease. Nat. Rev. Dis. Primers 2020, 6, 22. [Google Scholar] [CrossRef]
- Torres, J.; Mehandru, S.; Colombel, J.F.; Peyrin-Biroulet, L. Crohn’s disease. Lancet 2017, 389, 1741–1755. [Google Scholar] [CrossRef] [PubMed]
- Ungaro, R.; Mehandru, S.; Allen, P.B.; Peyrin-Biroulet, L.; Colombel, J.F. Ulcerative colitis. Lancet 2017, 389, 1756–1770. [Google Scholar] [CrossRef] [PubMed]
- Malik, T.F.; Aurelio, D.M. Extraintestinal Manifestations of Inflammatory Bowel Disease. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar] [PubMed]
- Kanis, J.; McCloskey, E.; Johansson, H.; Cooper, C.; Rizzoli, R.; Reginster, J.Y. European guidance for the diagnosis and management of osteoporosis in postmenopausal women. Osteoporos. Int. 2013, 24, 23–57. [Google Scholar] [CrossRef]
- Shen, Y.; Huang, X.; Wu, J.; Lin, X.; Zhou, X.; Zhu, Z.; Pan, X.; Xu, J.; Qiao, J.; Zhang, T.; et al. The global burden of osteoporosis, low bone mass, and its related fracture in 204 countries and territories, 1990–2019. Front. Endocrinol. 2022, 13, 882241. [Google Scholar] [CrossRef] [PubMed]
- Clynes, M.A.; Harvey, N.C.; Curtis, E.M.; Fuggle, N.R.; Dennison, E.M.; Cooper, C. The epidemiology of osteoporosis. Br. Med. Bull. 2020, 133, 105–117. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Du, D.; Zhou, Z.; Zhu, L.; Hu, X.; Lu, J.; Shi, C.; Chen, F.; Chen, A. TNF-α suppresses osteogenic differentiation of MSCs by accelerating P2Y2 receptor in estrogen-deficiency induced osteoporosis. Bone 2018, 117, 161–170. [Google Scholar] [CrossRef]
- Liu, H.; Dong, Y.; Gao, Y.; Zhao, L.; Cai, C.; Qi, D.; Zhu, M.; Zhao, L.; Liu, C.; Guo, F.; et al. Hesperetin suppresses RANKL-induced osteoclastogenesis and ameliorates lipopolysaccharide-induced bone loss. J. Cell. Physiol. 2019, 234, 11009–11022. [Google Scholar] [CrossRef]
- Saxena, Y.; Routh, S.; Mukhopadhaya, A. Immunoporosis: Role of innate immune cells in osteoporosis. Front. Immunol. 2021, 12, 687037. [Google Scholar] [CrossRef]
- Wu, D.; Cline-Smith, A.; Shashkova, E.; Perla, A.; Katyal, A.; Aurora, R. T-Cell mediated inflammation in postmenopausal osteoporosis. Front. Immunol. 2021, 12, 687551. [Google Scholar] [CrossRef]
- Kirkham-Wilson, F.; Dennison, E. Osteoporosis and Rheumatoid Arthritis: A Review of Current Understanding and Practice. Br. J. Hosp. Med. 2024, 85, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Penner, J.; Ombajo, L.A.; Nkuranga, J.; Otieno, E.; Nyakoe, D.; Wanjohi, R.; Mbewa, V.; Ndinya, F.; Eshiwani, S.; Wahome, S.; et al. High prevalence of osteoporosis among virally suppressed older people (≥60 years) living with HIV. HIV Med. 2024, 26, 382–389. [Google Scholar] [CrossRef] [PubMed]
- Kang, J.; Wu, X.; Li, Y.; Zhao, S.; Wang, S.; Yu, D. Association between inflammatory bowel disease and osteoporosis in European and East Asian populations: Exploring causality, mediation by nutritional status, and shared genetic architecture. Front. Immunol. 2024, 15, 1425610. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Wu, J.; Li, J.; Yan, Z.; Yu, X.; Huang, H. Higher prevalence of thyroid-specific autoantibodies (TPOAb and TgAb) is related to a higher prevalence of fractures in females: Results from NHANES 2007–2010. Osteoporos Int. 2024, 35, 1213–1221. [Google Scholar] [CrossRef] [PubMed]
- Leng, P.; Qiu, Y.; Zhou, M.; Zhu, Y.; Yin, N.; Zhou, M.; Wu, W.; Liu, M. Hypothyroidism correlates with osteoporosis: Potential involvement of lipid mediators. Front. Med. 2024, 11, 1453502. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Leungsuwan, D.S.; Chandran, M. Bone Fragility in Diabetes and its Management: A Narrative Review. Drugs 2024, 84, 1111–1134. [Google Scholar] [CrossRef] [PubMed]
- Zeng, M.; Lee, Y.H.; Wang, S.I.; Palmowski, A.; Chu, W.M.; Buttgereit, F. Fracture Risk Linked to Proton Pump Inhibitors Versus H2 Receptor Antagonists in Autoimmune Rheumatic and Gastrointestinal Disease Patients. Int. J. Rheum. Dis. 2025, 28, e70055. [Google Scholar] [CrossRef] [PubMed]
- Abraham, B.P.; Prasad, P.; Malaty, H.M. Vitamin D deficiency and corticosteroid use are risk factors for low bone mineral density in inflammatory bowel disease patients. Dig. Dis. Sci. 2014, 59, 1878–1884. [Google Scholar] [CrossRef]
- Davis, J.W.; Novotny, R.; Ross, P.D.; Wasnich, R.D. Anthropometric, lifestyle and menstrual factors influencing size-adjusted bone mineral content in a multiethnic population of premenopausal women. J. Nutr. 1996, 126, 2968–2976. [Google Scholar] [CrossRef]
- Patel, D.N.; Pettifor, J.M.; Becker, P.J. The effect of ethnicity on appendicular bone mass in white, coloured and Indian schoolchildren. S. Afr. Med. J. 1993, 83, 847–853. [Google Scholar]
- Dennison, E.; Yoshimura, N.; Hashimoto, T.; Cooper, C. Bone loss in Great Britain and Japan: A comparative longitudinal study. Bone 1998, 23, 379–382. [Google Scholar] [CrossRef] [PubMed]
- Burnham, J.M.; Shults, J.; Semeao, E.; Foster, B.; Zemel, B.S.; Stallings, V.A.; Leonard, M.B. Whole body BMC in pediatric Crohn disease: Independent effects of altered growth, maturation, and body composition. J. Bone Miner. Res. 2004, 19, 1961–1968. [Google Scholar] [CrossRef] [PubMed]
- Merlotti, D.; Mingiano, C.; Valenti, R.; Cavati, G.; Calabrese, M.; Pirrotta, F.; Bianciardi, S.; Palazzuoli, A.; Gennari, L. Bone Fragility in Gastrointestinal Disorders. Int. J. Mol. Sci. 2022, 23, 2713. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Adriani, A.; Pantaleoni, S.; Luchino, M.; Ribaldone, D.G.; Reggiani, S.; Sapone, N.; Sguazzini, C.; Isaia, G.; Pellicano, R.; Astegiano, M. Osteopenia and osteoporosis in patients with new diagnosis of inflammatory bowel disease. Panminerva Med. 2014, 56, 145–149. [Google Scholar] [PubMed]
- Targownik, L.E.; Bernstein, C.N.; Leslie, W.D. Risk factors and management of osteoporosis in inflammatory bowel disease. Curr. Opin. Gastroenterol. 2014, 30, 168–174. [Google Scholar] [CrossRef]
- Bernstein, C.N.; Leslie, W.D.; Leboff, M.S. AGA technical review on osteoporosis in gastrointestinal diseases. Gastroenterology 2003, 124, 795–841. [Google Scholar] [CrossRef]
- Schoon, E.; van Nunen, A.; Wouters, R.; Stockbrügger, R.; Russel, M. Osteopenia and osteoporosis in Crohn’s disease: Prevalence in a Dutch population-based cohort. Scand. J. Gastroenterol. Suppl. 2000, 232, 43–47. [Google Scholar]
- Geraci, A.; Tomasello, G.; Damiani, P.; Mazzoccato, G.; Marinato, L.; Gasparo, M. Bone loss in inflammatory Bowel disease: Our multicentric study. Endocrinol. Stud. 2011, 1, e3. [Google Scholar] [CrossRef]
- Boubaker, J.; Feki, M.; Hsairi, M.; Fekih, M.; Kaabachi, N.; Filali, A.; Mebazaa, A. Osteoporosis and inflammatory bowel disease: Prevalence and risk factors in Tunisian patients. Gastroenterol. Clin. Biol. 2003, 27, 901–907. [Google Scholar]
- Miznerova, E.; Hlavaty, T.; Koller, T.; Toth, J.; Holociova, K.; Huorka, M.; Killinger, Z.; Payer, J. The prevalence and risk factors for osteoporosis in patients with inflammatory bowel disease. Bratisl Lek Listy 2012, 114, 439–445. [Google Scholar] [CrossRef] [PubMed]
- Klaus, J.; Armbrecht, G.; Steinkamp, M.; Brückel, J.; Rieber, A.; Adler, G.; Reinshagen, M.; Felsenberg, D.; von Tirpitz, C. High prevalence of osteoporotic vertebral fractures in patients with Crohn’s disease. Gut 2002, 51, 654–658. [Google Scholar] [CrossRef] [PubMed]
- Vestergaard, P.; Krogh, K.; Rejnmark, L.; Laurberg, S.; Mosekilde, L. Fracture risk is increased in Crohn’s disease, but not in ulcerative colitis. Gut 2000, 46, 176–181. [Google Scholar] [CrossRef] [PubMed]
- van Staa, T.P.; Cooper, C.; Brusse, L.S.; Leufkens, H.; Javaid, M.K.; Arden, N.K. Inflammatory bowel disease and the risk of fracture. Gastroenterology 2003, 125, 1591–1597. [Google Scholar] [CrossRef]
- Choi, Y.J.; Ock, S.Y.; Chung, Y.S. Trabecular bone score (TBS) and TBS-adjusted fracture risk assessment tool are potential supplementary tools for the discrimination of morphometric vertebral fractures in postmenopausal women with type 2 diabetes. J. Clin. Densitom. 2016, 19, 507–514. [Google Scholar] [CrossRef]
- Jain, R.K.; Vokes, T. Dual-energy X-ray Absorptiometry. J. Clin. Densitom. 2017, 20, 291–303. [Google Scholar] [CrossRef] [PubMed]
- Silva, B.C.; Leslie, W.D.; Resch, H.; Lamy, O.; Lesnyak, O.; Binkley, N.; McCloskey, E.V.; Kanis, J.A.; Bilezikian, J.P. Trabecular bone score: A noninvasive analytical method based upon the DXA image. J. Bone Miner. Res. 2014, 29, 518–530. [Google Scholar] [CrossRef]
- Popp, A.W.; Meer, S.; Krieg, M.A.; Perrelet, R.; Hans, D.; Lippuner, K. Bone mineral density (BMD) and vertebral trabecular bone score (TBS) for the identifcation of elderly women at high risk for fracture: The SEMOF cohort study. Eur. Spine J. 2016, 25, 3432–3438. [Google Scholar] [CrossRef]
- Bonaccorsi, G.; Fila, E.; Messina, C.; Maietti, E.; Ulivieri, F.M.; Caudarella, R.; Greco, P.; Guglielmi, G. Comparison of trabecular bone score and hip structural analysis with FRAX® in postmenopausal women with type 2 diabetes mellitus. Aging Clin. Exp. Res. 2017, 29, 951–957. [Google Scholar] [CrossRef]
- Leslie, W.D.; Johansson, H.; McCloskey, E.V.; Harvey, N.C.; Kanis, J.A.; Hans, D. Comparison of methods for improving fracture risk assessment in diabetes: The Manitoba BMD Registry. J. Bone Miner. Res. 2018, 33, 1923–1930. [Google Scholar] [CrossRef]
- Krohn, K.; Schwartz, E.N.; Chung, Y.S.; Lewiecki, E.M. Dual-energy X-ray absorptiometry monitoring with trabecular bone score: 2019 ISCD Official Position. J. Clin. Densitom. 2019, 22, 501–505. [Google Scholar] [CrossRef] [PubMed]
- Muschitz, C.; Kocijan, R.; Haschka, J.; Pahr, D.; Kaider, A.; Pietschmann, P.; Hans, D.; Muschitz, G.K.; Fahrleitner-Pammer, A.; Resch, H. TBS reflects trabecular microarchitecture in premenopausal women and men with idiopathic osteoporosis and low-traumatic fractures. Bone 2015, 79, 259–266. [Google Scholar] [CrossRef]
- Ulivieri, F.M.; Silva, B.C.; Sardanelli, F.; Hans, D.; Bilezikian, J.P.; Caudarella, R. Utility of the trabecular bone score (TBS) in secondary osteoporosis. Endocrine 2014, 47, 435–448. [Google Scholar] [CrossRef]
- McCloskey, E.V.; Odén, A.; Harvey, N.C.; Leslie, W.D.; Hans, D.; Johansson, H.; Barkmann, R.; Boutroy, S.; Brown, J.; Chapurlat, R.; et al. A meta-analysis of trabecular bone score in fracture risk prediction and its relationship to FRAX. J. Bone Miner. Res. 2016, 31, 940–948. [Google Scholar] [CrossRef] [PubMed]
- Martineau, P.; Leslie, W. Trabecular bone score (TBS): Method and applications. Bone 2017, 104, 66–72. [Google Scholar] [CrossRef] [PubMed]
- Silva, B.C.; Broy, S.B.; Boutroy, S.; Schousboe, J.T.; Shepherd, J.A.; Leslie, W.D. Fracture risk prediction by non-BMD DXA measures: The 2015 ISCD official positions part 2: Trabecular bone score. J. Clin. Densitom. 2015, 18, 309–330. [Google Scholar] [CrossRef]
- Harvey, N.; Glüer, C.; Binkley, N.; McCloskey, E.; Brandi, M.-L.; Cooper, C.; Kendler, D.; Lamy, O.; Laslop, A.; Camargos, B.; et al. Trabecular bone score (TBS) as a new complementary approach for osteoporosis evaluation in clinical practice. Bone 2015, 78, 216–224. [Google Scholar] [CrossRef]
- Briot, K.; Paternotte, S.; Kolta, S.; Eastell, R.; Reid, D.M.; Felsenberg, D.; Glüer, C.C.; Roux, C. Added value of trabecular bone score to bone mineral density for prediction of osteoporotic fractures in postmenopausal women: The OPUS study. Bone 2013, 57, 232–236. [Google Scholar] [CrossRef]
- Nassar, K.; Paternotte, S.; Kolta, S.; Fechtenbaum, J.; Roux, C.; Briot, K. Added value of trabecular bone score over bone mineral density for identification of vertebral fractures in patients with areal bone mineral density in the non-osteoporotic range. Osteoporos. Int. 2014, 25, 243–249. [Google Scholar] [CrossRef]
- Chen, W.; Mao, M.; Fang, J.; Xie, Y.; Rui, Y. Fracture risk assessment in diabetes mellitus. Front. Endocrinol. 2022, 13, 961761. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Compston, J.E.; McClung, M.R.; Leslie, W.D. Osteoporosis. Lancet 2019, 393, 364–376. [Google Scholar] [CrossRef] [PubMed]
- Yu, T.; Bai, R.; Wang, Z.; Qin, Y.; Wang, J.; Wei, Y.; Zhao, R.; Nie, G.; Han, B. Colon-targeted engineered postbiotics nanoparticles alleviate osteoporosis through the gut-bone axis. Nat. Commun. 2024, 15, 10893. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Stockbrügger, R.; Schoon, E.; Bollani, S.; Mills, P.; Israeli, E.; Landgraf, L.; Felsenberg, D.; Ljunghall, S.; Nygard, G.; Persson, T.; et al. Discordance between the degree of osteopenia and the prevalence of spontaneous vertebral fractures in Crohn’s disease. Aliment. Pharmacol. Ther. 2002, 16, 1519–1527. [Google Scholar] [CrossRef] [PubMed]
- Soare, I.; Sirbu, A.; Popa, M.; Martin, S.; Tieranu, C.G.; Mateescu, B.; Diculescu, M.; Barbu, C.; Fica, S. Body Composition as a Modulator of Bone Health Changes in Patients with Inflammatory Bowel Disease. Life 2022, 12, 272. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Krajcovicova, A.; Kuzma, M.; Hlavaty, T.; Hans, D.; Koller, T.; Jackuliak, P.; Leskova, Z.; Sturdik, I.; Killinger, Z.; Payer, J. Decrease of trabecular bone score reflects severity of Crohn’s disease: Results of a case-control study. Eur. J. Gastroenterol. Hepatol. 2018, 30, 101–106. [Google Scholar] [CrossRef] [PubMed]
- Soare, I.; Sirbu, A.; Martin, S.; Diculescu, M.; Mateescu, B.; Tieranu, C.; Fica, S. Assessment of bone quality with trabecular bone score in patients with inflammatory bowel disease. Sci. Rep. 2021, 11, 20345. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Haschka, J.; Kraus, D.A.; Behanova, M.; Huber, S.; Bartko, J.; Schanda, J.E.; Meier, P.; Bahrami, A.; Zandieh, S.; Zwerina, J.; et al. Fractal-Based Analysis of Bone Microstructure in Crohn’s Disease: A Pilot Study. J. Clin. Med. 2020, 9, 4116. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ezzat, Y.; Hamdy, K. The frequency of low bone mineral density and its associated risk factors in patients with inflammatory bowel diseases. Int. J. Rheum. Dis. 2010, 13, 259–265. [Google Scholar] [CrossRef]
- Bjarnason, I.; Macpherson, A.; Mackintosh, C.; Buxton-Thomas, M.; Forgacs, I.; Moniz, C. Reduced bone density in patients with inflammatory bowel disease. Gut 1997, 40, 228–233. [Google Scholar] [CrossRef]
- Levy-Shraga, Y.; Megnazi, O.; Modan-Moses, D.; Tripto-Shkolnik, L.; Gruber, N.; Haberman, Y.; Shouval, D.S.; Weiss, B. Trabecular Bone Score in Children and Adolescents With Inflammatory Bowel Diseases. J. Clin. Densitom. 2021, 24, 243–251. [Google Scholar] [CrossRef] [PubMed]
- Lupoli, R.; Di Minno, A.; Spadarella, G.; Ambrosino, P.; Panico, A.; Tarantino, L.; Lupoli, G.; Lupoli, G.; Di Minno, M.N.D. The risk of osteoporosis in patients with liver cirrhosis: A meta-analysis of literature studies. Clin. Endocrinol. 2016, 84, 30–38. [Google Scholar] [CrossRef] [PubMed]
- Zavatta, G.; Vitale, G.; Morelli, M.C.; Pianta, P.; Turco, L.; Cappa, F.M.; Ravaioli, M.; Cescon, M.; Piscaglia, F.; Altieri, P.; et al. High bone fracture risk in a large modern cohort of liver transplant recipients. Intern. Emerg. Med. 2024, 20, 139–150. [Google Scholar] [CrossRef] [PubMed]
- Ogiso, Y.; Hanai, T.; Nishimura, K.; Miwa, T.; Maeda, T.; Imai, K.; Suetsugu, A.; Takai, K.; Shimizu, M. Usefulness of the Trabecular Bone Score in Assessing the Risk of Vertebral Fractures in Patients with Cirrhosis. J. Clin. Med. 2022, 11, 1562. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Stulic, M.; Jadzic, J.; Dostanic, N.; Zivkovic, M.; Stojkovic, T.; Aleksic, J.; Stojkovic, S.; Stojkovic Lalosevic, M.; Vojnovic, M.; Vlaisavljevic, Z.; et al. Clinical Indicators of Bone Deterioration in Alcoholic Liver Cirrhosis and Chronic Alcohol Abuse: Looking beyond Bone Fracture Occurrence. Diagnostics 2024, 14, 510. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Yokoyama, S.; Honda, T.; Ishizu, Y.; Imai, N.; Ito, T.; Yamamoto, K.; Mizuno, K.; Kojima, T.; Kariya, N.; Nakamura, M.; et al. Risk factors for decreased bone mineral density in patients with metabolic dysfunction-associated steatotic liver disease: A cross-sectional study at a health examination center. Clin. Nutr. 2024, 43, 1425–1432. [Google Scholar] [CrossRef] [PubMed]
- Cheung, Y.M.; Joham, A.; Marks, S.; Teede, H. The obesity paradox: An endocrine perspective. Intern. Med. J. 2017, 47, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.C.; Piazuelo, M.B.; Kuipers, E.J.; Li, D. AGA clinical practice update on the diagnosis and management of atrophic gastritis: Expert review. Gastroenterology 2021, 161, 1325–1332. [Google Scholar] [CrossRef]
- Massironi, S.; Cavalcoli, F.; Zilli, A.; Del Gobbo, A.; Ciafardini, C.; Bernasconi, S.; Felicetta, I.; Conte, D.; Peracchi, M. Relevance of vitamin D deficiency in patients with chronic autoimmune atrophic gastritis: A prospective study. BMC Gastroenterol. 2018, 18, 172. [Google Scholar] [CrossRef]
- Lee, S.; Yun, J.M.; Park, J.H.; Kwon, H. Association between Chronic Atrophic Gastritis and Bone Mineral Density among Women Older than 40 Years of Age in Korea. Korean J. Fam. Med. 2024, 45, 199–206. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Raza, M.; Bhatt, H. Atrophic Gastritis. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2025. [Google Scholar] [PubMed]
- Inoue, I.; Yoshimura, N.; Iidaka, T.; Horii, C.; Muraki, S.; Oka, H.; Kawaguchi, H.; Akune, T.; Maekita, T.; Mure, K.; et al. Helicobacter pylori-Related Chronic Gastritis as a Risk Factor for Lower Bone Mineral Density. Calcif. Tissue Int. 2025, 116, 16. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Shafrir, A.; Shauly-Aharonov, M.; Katz, L.H.; Paltiel, O.; Pickman, Y.; Ackerman, Z. The association between serum vitamin D levels and Helicobacter pylori presence and eradication. Nutrients 2021, 13, 278. [Google Scholar] [CrossRef] [PubMed]
- Aasarød, K.M.; Mosti, M.P.; Stunes, A.K.; Reseland, J.E.; Basso, T.; Syversen, U.; Fossmark, R. Impaired skeletal health in patients with chronic atrophic gastritis. Scand. J. Gastroenterol. 2016, 51, 774–781. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.A.; Slart, R.H.; Ali, D.S.; Bock, O.; Carey, J.J.; Camacho, P.; Engelke, K.; Erba, P.A.; Harvey, N.C.; Lems, W.F.; et al. Osteoporotic Fractures: Diagnosis, Evaluation, and Significance From the International Working Group on DXA Best Practices. Mayo Clin. Proc. 2024, 99, 1127–1141. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.Y.; Kim, K.M. Similarities and differences between bone quality parameters, trabecular bone score and femur geometry. PLoS ONE 2022, 17, e0260924. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Skoracka, K.; Marciniak, M.D.; Michalak, M.; Zawada, A.; Ratajczak-Pawłowska, A.E.; Dobrowolska, A.; Krela-Kaźmierczak, I. The other side of celiac disease—Assessment of bone mineral density and body composition in patients with celiac disease. Prz Gastroenterol. 2024, 16, 434–438. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ganji, A.; Esmaeilzadeh, A.; Hatef, M. Prevalence of Osteopenia and Osteoporosis in Patients with Celiac Disease in Northeastern Iran. Govaresh 2012, 16, 223–227. [Google Scholar]
- Garber, J.J.; Roelstraete, B.; Lochhead, P.J.; Uchida, A.M.; Michaëlsson, K.; Olén, O.; Ludvigsson, J.F. Risk of fractures in individuals with eosinophilic esophagitis: Nationwide population-based cohort study. Esophagus. 2022, 19, 542–553. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]

{kind=link}
| Design | CD * | UC † | Disease Activity | Disease Duration | Subgroups According to the Treatment | |
|---|---|---|---|---|---|---|
| Soare I, et al. [55] | Multicentric, cross-sectional | yes | yes | no | no | no |
| Krajcovicova A, et al. [56] | Single-center, cohort | yes | no | no | yes | yes |
| Soare I, et al. [57] | Single-center, cross-sectional | yes | yes | yes | yes | yes |
| Haschka J, et al. [58] | Single-center, cross-sectional | yes | no | no | yes | yes |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Olic, I.; Zivkovic, P.M.; Hadjina, I.T.; Zaja, I. Clinical Utility of Trabecular Bone Score in Gastroenterology: A Narrative Review. Biomedicines 2025, 13, 1331. https://doi.org/10.3390/biomedicines13061331
Olic I, Zivkovic PM, Hadjina IT, Zaja I. Clinical Utility of Trabecular Bone Score in Gastroenterology: A Narrative Review. Biomedicines. 2025; 13(6):1331. https://doi.org/10.3390/biomedicines13061331
Chicago/Turabian StyleOlic, Ivna, Piero Marin Zivkovic, Ivana Tadin Hadjina, and Ivan Zaja. 2025. "Clinical Utility of Trabecular Bone Score in Gastroenterology: A Narrative Review" Biomedicines 13, no. 6: 1331. https://doi.org/10.3390/biomedicines13061331
APA StyleOlic, I., Zivkovic, P. M., Hadjina, I. T., & Zaja, I. (2025). Clinical Utility of Trabecular Bone Score in Gastroenterology: A Narrative Review. Biomedicines, 13(6), 1331. https://doi.org/10.3390/biomedicines13061331