
Artificial Intelligence Algorithm to Screen for Diabetic Neuropathy: A Pilot Study

 ,
,  , , ,
, , , 
Abstract

1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Anthropometric and Biochemical Parameters
2.3. Artificial Intelligence (AI) Software
2.4. Peripheral Neuropathy Measurement
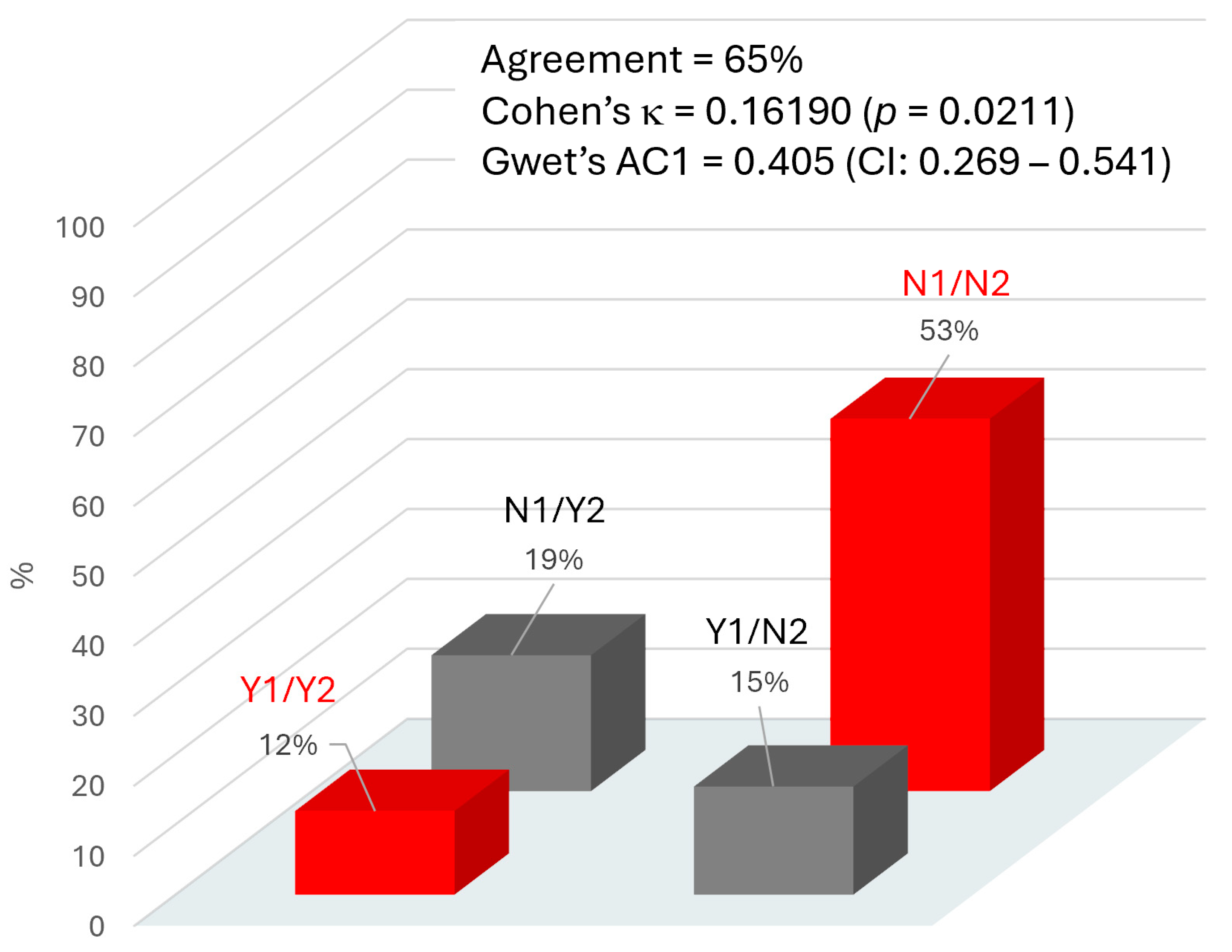
2.5. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AI | Artificial intelligence |
| ALT | Alanine aminotransferase |
| AST | Aspartate aminotransferase |
| BMI | Body mass index |
| CPK | Creatine phosphokinase |
| DPN | Diabetic polyneuropathy |
| GGT | Gamma-glutamyl transferase |
| HDL | High-density lipoprotein |
| LDL | Low-density lipoprotein |
| T2D | Type 2 diabetes |
| VPT | Vibratory perception threshold |
References
- Cicek, M.; Buckley, J.; Pearson-Stuttard, J.; Gregg, E.W. Characterizing Multimorbidity from Type 2 Diabetes: Insights from Clustering Approaches. Endocrinol. Metab. Clin. N. Am. 2021, 50, 531–558. [Google Scholar] [CrossRef] [PubMed]
- Shah, M.; Vella, A. What is type 2 diabetes? Medicine 2014, 42, 687–691. [Google Scholar] [CrossRef]
- Van Acker, K.; Bouhassira, D.; De Bacquer, D.; Weiss, S.; Matthys, K.; Raemen, H.; Mathieu, C.; Colin, I.M. Prevalence and impact on quality of life of peripheral neuropathy with or without neuropathic pain in type 1 and type 2 diabetic patients attending hospital outpatients’ clinics. Diabetes Metab. 2009, 35, 206–213. [Google Scholar] [CrossRef]
- Callaghan, B.; Kerber, K.; Langa, K.M.; Banerjee, M.; Rodgers, A.; McCammon, R.; Burke, J.; Feldman, E. Longitudinal patient-oriented outcomes in neuropathy: Importance of early detection and falls. Neurology 2015, 85, 71–79. [Google Scholar] [CrossRef] [PubMed]
- Feldman, E.L.; Callaghan, B.C.; Pop-Busui, R.; Zochodne, D.W.; Wright, D.E.; Bennett, D.L.; Bril, V.; Russell, J.W.; Viswanathan, V. Diabetic neuropathy. Nat. Rev. Dis. Primers 2019, 5, 42. [Google Scholar] [CrossRef]
- Ang, L.; Jaiswal, M.; Martin, C.; Pop-Busui, R. Glucose control and diabetic neuropathy: Lessons from recent large clinical trials. Curr. Diabetes Rep. 2014, 14, 528. [Google Scholar] [CrossRef]
- Pop-Busui, R.; Boulton, A.J.M.; Feldman, E.L.; Bril, V.; Freeman, R.; Malik, R.A.; Sosenko, J.M.; Ziegler, D. Diabetic Neuropathy: A Position Statement by the American Diabetes Association. Diabetes Care 2017, 40, 136–154. [Google Scholar] [CrossRef]
- Franklin, G.M.; Kahn, L.B.; Baxter, J.; Marshall, J.A.; Hamman, R.F. Sensory neuropathy in non-insulin-dependent diabetes mellitus. The San Luis Valley Diabetes Study. Am. J. Epidemiol. 1990, 131, 633–643. [Google Scholar] [CrossRef] [PubMed]
- Dyck, P.J.; Kratz, K.M.; Karnes, J.L.; Litchy, W.J.; Klein, R.; Pach, J.M.; Wilson, D.M.; O’Brien, P.C.; Melton, L.J., 3rd; Service, F.J. The prevalence by staged severity of various types of diabetic neuropathy, retinopathy, and nephropathy in a population-based cohort: The Rochester Diabetic Neuropathy Study. Neurology 1993, 43, 817–824. [Google Scholar] [CrossRef]
- Partanen, J.; Niskanen, L.; Lehtinen, J.; Mervaala, E.; Siitonen, O.; Uusitupa, M. Natural history of peripheral neuropathy in patients with non-insulin-dependent diabetes mellitus. N. Engl. J. Med. 1995, 333, 89–94. [Google Scholar] [CrossRef]
- Boulton, A.J.; Knight, G.; Drury, J.; Ward, J.D. The prevalence of symptomatic, diabetic neuropathy in an insulin-treated population. Diabetes Care 1985, 8, 125–128. [Google Scholar] [CrossRef] [PubMed]
- Tesfaye, S.; Chaturvedi, N.; Eaton, S.E.; Ward, J.D.; Manes, C.; Ionescu-Tirgoviste, C.; Witte, D.R.; Fuller, J.H.; EURODIAB Prospective Complications Study Group. Vascular risk factors and diabetic neuropathy. N. Engl. J. Med. 2005, 352, 341–350. [Google Scholar] [CrossRef]
- Boyle, J.P.; Thompson, T.J.; Gregg, E.W.; Barker, L.E.; Williamson, D.F. Projection of the year 2050 burden of diabetes in the US adult population: Dynamic modeling of incidence, mortality, and prediabetes prevalence. Popul. Health Metr. 2010, 8, 29. [Google Scholar] [CrossRef]
- Bril, V.; Breiner, A.; Perkins, B.A.; Zochodne, D. Neuropathy. Can. J. Diabetes 2018, 42, S217–S221. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association (ADA) Professional Practice Committee. 12. Retinopathy, Neuropathy, and Foot Care: Standards of Care in Diabetes-2024. Diabetes Care 2024, 47 (Suppl. S1), S231–S243. [Google Scholar] [CrossRef]
- Sharma, K.N.S.; Kumar, H.A. Assessment of the diagnostic accuracy of Vibrasense compared to a biothesiometer and nerve conduction study for screening diabetic peripheral neuropathy. J. Foot Ankle Res. 2023, 16, 65. [Google Scholar] [CrossRef] [PubMed]
- Kelshikar, S.; Athavale, V.; Parekh, R.A.; Ranka, M. The Role of a Biothesiometer in Early Detection and Management of Diabetic Neuropathy. Cureus 2024, 16, e70588. [Google Scholar] [CrossRef]
- Chemello, G.; Salvatori, B.; Morettini, M.; Tura, A. Artificial Intelligence Methodologies Applied to Technologies for Screening, Diagnosis and Care of the Diabetic Foot: A Narrative Review. Biosensors 2022, 12, 985. [Google Scholar] [CrossRef]
- Dagliati, A.; Marini, S.; Sacchi, L.; Cogni, G.; Teliti, M.; Tibollo, V.; De Cata, P.; Chiovato, L.; Bellazzi, R. Machine Learning Methods to Predict Diabetes Complications. J. Diabetes Sci. Technol. 2018, 12, 295–302. [Google Scholar] [CrossRef]
- Aminian, A.; Zajichek, A.; Arterburn, D.E.; Wolski, K.E.; Brethauer, S.A.; Schauer, P.R.; Nissen, S.E.; Kattan, M.W. Predicting 10-Year Risk of End-Organ Complications of Type 2 Diabetes with and without Metabolic Surgery: A Machine Learning Approach. Diabetes Care 2020, 43, 852–859. [Google Scholar] [CrossRef]
- Fan, Y.; Long, E.; Cai, L.; Cao, Q.; Wu, X.; Tong, R. Machine Learning Approaches to Predict Risks of Diabetic Complications and Poor Glycemic Control in Nonadherent Type 2 Diabetes. Front. Pharmacol. 2021, 12, 665951. [Google Scholar] [CrossRef]
- Svedberg, P.; Reed, J.; Nilsen, P.; Barlow, J.; Macrae, C.; Nygren, J. Toward Successful Implementation of Artificial Intelligence in Health Care Practice: Protocol for a Research Program. JMIR Res. Protoc. 2022, 11, e34920. [Google Scholar] [CrossRef]
- Nicolucci, A.; Romeo, L.; Bernardini, M.; Vespasiani, M.; Rossi, M.C.; Petrelli, M.; Ceriello, A.; Di Bartolo, P.; Frontoni, E.; Vespasiani, G. Prediction of complications of type 2 Diabetes: A Machine learning approach. Diabetes Res. Clin. Pract. 2022, 190, 110013. [Google Scholar] [CrossRef] [PubMed]
- Goyal, M.; Reeves, N.D.; Rajbhandari, S.; Yap, M.H. Robust Methods for Real-Time Diabetic Foot Ulcer Detection and Localization on Mobile Devices. IEEE J. Biomed. Health Inform. 2019, 23, 1730–1741. [Google Scholar] [CrossRef]
- Williams, B.M.; Borroni, D.; Liu, R.; Zhao, Y.; Zhang, J.; Lim, J.; Ma, B.; Romano, V.; Qi, H.; Ferdousi, M.; et al. An artificial intelligence-based deep learning algorithm for the diagnosis of diabetic neuropathy using corneal confocal microscopy: A development and validation study. Diabetologia 2020, 63, 419–430. [Google Scholar] [CrossRef] [PubMed]
- Salahouddin, T.; Petropoulos, I.N.; Ferdousi, M.; Ponirakis, G.; Asghar, O.; Alam, U.; Kamran, S.; Mahfoud, Z.R.; Efron, N.; Malik, R.A.; et al. Artificial Intelligence–Based Classification of Diabetic Peripheral Neuropathy from Corneal Confocal Microscopy Images. Diabetes Care 2021, 44, e151–e153. [Google Scholar] [CrossRef]
- Chen, W.; Liao, D.; Deng, Y.; Hu, J. Development of a transformer-based deep learning algorithm for diabetic peripheral neuropathy classification using corneal confocal microscopy images. Front. Cell Dev. Biol. 2024, 12, 1484329. [Google Scholar] [CrossRef] [PubMed]
- Lai, Y.R.; Chiu, W.C.; Huang, C.C.; Cheng, B.C.; Kung, C.T.; Lin, T.Y.; Chiang, H.C.; Tsai, C.J.; Kung, C.F.; Lu, C.H. Longitudinal artificial intelligence-based deep learning models for diagnosis and prediction of the future occurrence of polyneuropathy in diabetes and prediabetes. Clin. Neurophysiol. 2024, 54, 102982. [Google Scholar] [CrossRef]
- Teh, K.; Armitage, P.; Tesfaye, S.; Selvarajah, D. Deep Learning Classification of Treatment Response in Diabetic Painful Neuropathy: A Combined Machine Learning and Magnetic Resonance Neuroimaging Methodological Study. Neuroinformatics 2023, 21, 35–43. [Google Scholar] [CrossRef]
- Qiao, Q.; Cao, J.; Xue, W.; Qian, J.; Wang, C.; Pan, Q.; Lu, B.; Xiong, Q.; Chen, L.; Hou, X. Deep learning-based automated tool for diagnosing diabetic peripheral neuropathy. Digit. Health 2024, 10, 20552076241307573. [Google Scholar] [CrossRef]
- Huang, J.; Yeung, A.M.; Armstrong, D.G.; Battarbee, A.N.; Cuadros, J.; Espinoza, J.C.; Kleinberg, S.; Mathioudakis, N.; Swerdlow, M.A.; Klonoff, D.C. Artificial Intelligence for Predicting and Diagnosing Complications of Diabetes. J. Diabetes Sci. Technol. 2023, 17, 224–238. [Google Scholar] [CrossRef]
- Chen, T.; Guestrin, C. XGBoost: A scalable tree boosting system. In Proceedings of the 22nd ACM SIGKDD International Conference on Knowledge Discovery and Data Mining (KDD ’16); ACM: New York, NY, USA, 2016; pp. 785–794. [Google Scholar] [CrossRef]
- METEDA S.r.l. MetaClinic User Guide: AI Prediction Module, Version 2.1; METEDA S.r.l.: Milan, Italy, 2022; Section 3, “Risk Stratification”. [Google Scholar]
- Young, M.J.; Breddy, J.L.; Veves, A.; Boulton, A.J.M. The Prediction of Diabetic Neuropathic Foot Ulceration Using Vibration Perception Thresholds: A prospective study. Diabetes Care 1994, 17, 557–560. [Google Scholar] [CrossRef]
- Pham, H.; Armstrong, D.G.; Harvey, C.; Harkless, L.B.; Giurini, J.M.; Veves, A. Screening techniques to identify people at high risk for diabetic foot ulceration: A prospective multicenter trial. Diabetes Care 2000, 23, 606–611. [Google Scholar] [CrossRef]
- Mooi, C.S.; Lee, K.W.; Yusof Khan, A.H.K.; Devaraj, N.K.; Cheong, A.T.; Hoo, F.K.; Sulaiman, W.A.W.; Loh, W.C.; Jian, L.Y.; Hui, T.X.; et al. Using biothesiometer, Neuropathy Symptom Score, and Neuropathy Disability Score for the early detection of peripheral neuropathy: A cross-sectional study. Qatar Med. J. 2024, 2024, 24. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. A coefficient of agreement for nominal scales. Educ. Psychol. Meas. 1960, 20, 37–46. [Google Scholar] [CrossRef]
- Gwet, K.L. Computing inter-rater reliability and its variance in the presence of high agreement. Br. J. Math. Stat. Psychol. 2008, 61, 29–48. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [PubMed]
- Vach, W.; Gerke, O. Gwet’s AC1 is not a substitute for Cohen’s kappa—A comparison of basic properties. MethodsX 2023, 10, 102212. [Google Scholar] [CrossRef]
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem. Med. 2012, 22, 276–282. [Google Scholar] [CrossRef]
- Groener, J.B.; Jende, J.M.E.; Kurz, F.T.; Kender, Z.; Treede, R.D.; Schuh-Hofer, S.; Nawroth, P.P.; Bendszus, M.; Kopf, S. Understanding Diabetic Neuropathy-From Subclinical Nerve Lesions to Severe Nerve Fiber Deficits: A Cross-Sectional Study in Patients with Type 2 Diabetes and Healthy Control Subjects. Diabetes 2020, 69, 436–447. [Google Scholar] [CrossRef]
- Preston, F.G.; Meng, Y.; Burgess, J.; Ferdousi, M.; Azmi, S.; Petropoulos, I.N.; Kaye, S.; Malik, R.A.; Zheng, Y.; Alam, U. Artificial intelligence utilising corneal confocal microscopy for the diagnosis of peripheral neuropathy in diabetes mellitus and prediabetes. Diabetologia 2022, 65, 457–466. [Google Scholar] [CrossRef]
- Xiao, M.X.; Lu, C.H.; Ta, N.; Wei, H.C.; Yang, C.C.; Wu, H.T. Toe PPG sample extension for supervised machine learning approaches to simultaneously predict type 2 diabetes and peripheral neuropathy. Biomed. Signal Process. Control 2022, 71, 103236. [Google Scholar] [CrossRef]
- Vincent, A.M.; Callaghan, B.C.; Smith, A.L.; Feldman, E.L. Diabetic neuropathy: Cellular mechanisms as therapeutic targets. Nat. Rev. Neurol. 2011, 7, 573–583. [Google Scholar] [CrossRef] [PubMed]
- Callaghan, B.C.; Cheng, H.T.; Stables, C.L.; Smith, A.L.; Feldman, E.L. Diabetic neuropathy: Clinical manifestations and current treatments. Lancet Neurol. 2012, 11, 521–534. [Google Scholar] [CrossRef]
- Bönhof, G.J.; Herder, C.; Strom, A.; Papanas, N.; Roden, M.; Ziegler, D. Emerging Biomarkers, Tools, and Treatments for Diabetic Polyneuropathy. Endocr. Rev. 2019, 40, 153–192. [Google Scholar] [CrossRef] [PubMed]
- Guan, Z.; Li, H.; Liu, R.; Cai, C.; Liu, Y.; Li, J.; Wang, X.; Huang, S.; Wu, L.; Liu, D.; et al. Artificial intelligence in diabetes management: Advancements, opportunities, and challenges. Cell Rep. Med. 2023, 4, 101213. [Google Scholar] [CrossRef]
- Char, D.S.; Shah, N.H.; Magnus, D. Implementing machine learning in health care—Addressing ethical challenges. N. Engl. J. Med. 2018, 378, 981–983. [Google Scholar] [CrossRef]
- Obermeyer, Z.; Powers, B.; Vogeli, C.; Mullainathan, S. Dissecting racial bias in an algorithm used to manage the health of populations. Science 2019, 366, 447–453. [Google Scholar] [CrossRef]
- Čartolovni, A.; Tomičić, A.; Lazić Mosler, E. Ethical, legal, and social considerations of AI-based medical decision-support tools: A scoping review. Int. J. Med. Inform. 2022, 161, 104738. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| DPN Risk (AI Algorithm) | DPN Present (VPT ≥ 25 V) | DPN Absent (VPT < 25 V) | p * | ||||||
|---|---|---|---|---|---|---|---|---|---|
| n | VPT (V) | n | VPT (V) | ||||||
| Low | 26 (41.27%) | 29.23 ± 2.80 |  | p = 0.3093 † | 81 (58.70%) | 14.91 ± 4.82 |  | p = 0.9895 † | p = 0.0920 |
| Moderate | 13 (20.63%) | 30.23 ± 2.62 | 26 (18.84%) | 14.88 ± 4.42 | |||||
| High | 13 (20.63%) | 30.69 ± 1.84 | 16 (11.59%) | 14.87 ± 4.29 | |||||
| Very high | 11 (17.46%) | 29.18 ± 2.89 | 15 (10.87%) | 14.47 ± 4.58 | |||||
| Total | 63 (100%) | 29.73 ± 2.63 | 138 (100%) | 14.86 ± 4.62 | |||||
| Parameter | DPN Present (n = 63) | DPN Absent (n = 138) | p * |
|---|---|---|---|
| Age, y | 72.7 ± 6.7 | 66.6 ± 9.9 | <0.0001 |
| Sex, M/F | 41/22 | 77/61 | 0.2150 |
| Disease duration, y | 14.4 ± 8.9 | 11.0 ± 8.4 | 0.0110 |
| BMI, kg/m2 | 28.9 ± 4.8 | 28.3 ± 4.7 | 0.4369 |
| Systolic blood pressure, mmHg | 144.3 ± 18.5 | 139.6 ± 18.4 | 0.0910 |
| Diastolic blood pressure, mmHg | 77.2 ± 10.5 | 80.5 ± 10.3 | 0.0356 |
| HbA1c, mmol/mol | 52.6 ± 10.8 | 56.0 ± 14.1 | 0.0927 |
| Fasting blood glucose, mg/dL | 139.1 ± 38.0 | 137.6 ± 39.1 | 0.8023 |
| Total cholesterol, mg/dL | 161.6 ± 44.6 | 159.2 ± 39.0 | 0.7026 |
| HDL cholesterol, mg/dL | 50.0 ± 13.2 | 51.1 ± 14.6 | 0.6050 |
| LDL cholesterol, mg/dL | 91.5 ± 40.9 | 88.7 ± 29.9 | 0.5954 |
| Triglycerides, mg/dL | 114.7 ± 51.9 | 112.5 ± 58.3 | 0.7951 |
| AST, IU/L | 23.5 ± 10.0 | 24.9 ± 10.7 | 0.4560 |
| ALT, IU/L | 22.5 ± 10.9 | 25.1 ± 14.5 | 0.2709 |
| Serum creatinine, mg/dL | 0.97 ± 0.36 | 0.88 ± 0.30 | 0.0788 |
| Microalbuminuria, mg/L | 62.5 ± 136.1 | 53.2 ± 230.0 | 0.7811 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sartore, G.; Ragazzi, E.; Pegoraro, F.; Pagno, M.G.; Lapolla, A.; Piarulli, F. Artificial Intelligence Algorithm to Screen for Diabetic Neuropathy: A Pilot Study. Biomedicines 2025, 13, 1075. https://doi.org/10.3390/biomedicines13051075
Sartore G, Ragazzi E, Pegoraro F, Pagno MG, Lapolla A, Piarulli F. Artificial Intelligence Algorithm to Screen for Diabetic Neuropathy: A Pilot Study. Biomedicines. 2025; 13(5):1075. https://doi.org/10.3390/biomedicines13051075
Chicago/Turabian StyleSartore, Giovanni, Eugenio Ragazzi, Francesco Pegoraro, Mario German Pagno, Annunziata Lapolla, and Francesco Piarulli. 2025. "Artificial Intelligence Algorithm to Screen for Diabetic Neuropathy: A Pilot Study" Biomedicines 13, no. 5: 1075. https://doi.org/10.3390/biomedicines13051075
APA StyleSartore, G., Ragazzi, E., Pegoraro, F., Pagno, M. G., Lapolla, A., & Piarulli, F. (2025). Artificial Intelligence Algorithm to Screen for Diabetic Neuropathy: A Pilot Study. Biomedicines, 13(5), 1075. https://doi.org/10.3390/biomedicines13051075