
Chronic Urticaria Biomarkers IL-6, ESR and CRP in Correlation with Disease Severity and Patient Quality of Life—A Pilot Study

 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. The Ethical Statement
2.3. Methods
2.3.1. Serum Parameters
2.3.2. Questionnaires
2.3.3. Statistical Analysis
3. Results
3.1. Study Population
3.2. Descriptive Statistics
3.3. Results for ESR
3.4. Results for IL-6
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Zuberbier, T.; Latiff, A.H.A.; Abuzakouk, M.; Aquilina, S.; Asero, R.; Baker, D.; Bangert, C.; Ben-Shoshan, M.; Bernstein, J.A.; Bindslev-Jensen, C.; et al. The international EAACI/GA2LEN/EuroGuiDerm/APAAACI guideline for the definition, classification, diagnosis, and management of urticaria. Allergy 2022, 77, 734–766. [Google Scholar] [CrossRef] [PubMed]
- Pozderac, I.; Lugović-Mihić, L.; Artuković, M.; Stipić-Marković, A.; Kuna, M.; Ferček, I. Chronic inducible urticaria: Classification and prominent features of physical and non-physical types. Acta Dermatovenerol. Alp. Pannonica Adriat. 2020, 29, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Fricke, J.; Ávila, G.; Keller, T.; Weller, K.; Lau, S.; Maurer, M.; Zuberbier, T.; Keil, T. Prevalence of chronic urticaria in children and adults across the globe: Systematic review with meta-analysis. Allergy 2020, 75, 423–432. [Google Scholar] [CrossRef]
- Bracken, S.J.; Abraham, S.; MacLeod, A.S. Autoimmune theories of chronic spontaneous urticaria. Front. Immunol. 2019, 10, 627. [Google Scholar] [CrossRef]
- Kolkhir, P.; Giménez-Arnau, A.M.; Kulthanan, K.; Peter, J.; Metz, M.; Maurer, M. Urticaria. Nat. Rev. Dis. Primers 2022, 8, 61. [Google Scholar] [CrossRef]
- Poddighe, D. The prevalence of chronic spontaneous urticaria (CSU) in the pediatric population. J. Am. Acad. Dermatol. 2019, 81, e149. [Google Scholar] [CrossRef]
- Saini, S.S.; Kaplan, A.P. Chronic spontaneous urticaria: The Devil’s itch. J. Allergy Clin. Immunol. Pract. 2018, 6, 1097. [Google Scholar] [CrossRef] [PubMed]
- Zhou, B.; Li, J.; Liu, R.; Zhu, L.; Peng, C. The role of crosstalk of immune cells in pathogenesis of chronic spontaneous Urticaria. Front. Immunol. 2022, 31, 879754. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, A.P.; Horáková, Z.; Katz, S.I. Assessment of tissue fluid histamine levels in patients with urticaria. J. Allergy Clin. Immunol. 1978, 61, 350–354. [Google Scholar] [CrossRef]
- Sánchez-Borges, M.; Ansotegui, I.J.; Baiardini, I.; Bernstein, J.; Canonica, G.W.; Ebisawa, M.; Gomez, M.; Gonzalez-Diaz, S.N.; Martin, B.; Morais-Almeida, M.; et al. The challenges of chronic urticaria part 1: Epidemiology, immunopathogenesis, comorbidities, quality of life, and management. World Allergy Organ. J. 2021, 14, 100533. [Google Scholar] [CrossRef]
- Dos Santos, J.C.; Azor, M.H.; Nojima, V.Y.; Lourenço, F.D.; Prearo, E.; Maruta, C.W.; Rivitti, E.A.; da Silva Duarte, A.J.; Sato, M.N. Increased circulating pro-inflammatory cytokines and imbalanced regulatory T-cell cytokines production in chronic idiopathic urticaria. Int. Immunopharmacol. 2008, 8, 1433–1440. [Google Scholar] [CrossRef]
- Toubi, E.; Vadasz, Z. Highlights in autoimmunity: 2020. Isr. Med. Assoc. J. 2020, 11, 717–719. [Google Scholar] [PubMed]
- Lugović-Mihić, L.; Bukvić, I.; Bulat, V.; Japundžić, I. Factors contributing to chronic urticaria/angioedema and nummular eczema resolution—Which findings are crucial? Acta Clin. Croat. 2019, 58, 595–603. [Google Scholar] [CrossRef] [PubMed]
- Lugović-Mihić, L.; Mandušić, N.; Dasović, M.; Pondeljak, N.; Kuna, M.; Pozderac, I. Vitamin D supplementation in patients with atopic dermatitis, chronic urticaria and contact irritant and allergic dermatitis—Possible improvement without risk. Folia Med. 2022, 64, 467–477. [Google Scholar] [CrossRef] [PubMed]
- Aleem, S.; Masood, Q.; Hassan, I. Correlation of C-reactive protein levels with severity—Of chronic urticaria. Indian J. Dermatol. 2014, 59, 636. [Google Scholar] [CrossRef]
- Kasperska-Zajac, A.; Sztylc, J.; Machura, E.; Jop, G. Plasma IL-6 concentration correlates with clinical disease activity and serum C-reactive protein concentration in chronic urticaria patients. Clin. Exp. Allergy 2011, 41, 1386–1391. [Google Scholar] [CrossRef] [PubMed]
- Ucmak, D.; Akkurt, M.; Toprak, G.; Yesilova, Y.; Turan, E.; Yildiz, I. Determination of dermatology life quality index, and serum C-reactive protein and plasma interleukin-6 levels in patients with chronic urticaria. Postep. Dermatol. Alergol. 2013, 30, 146–151. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Zhang, H.; Du, S.; Yan, S.; Zeng, J. Advanced Biomarkers: Therapeutic and diagnostic targets in urticaria. Int. Arch. Allergy Immunol. 2021, 182, 917–931. [Google Scholar] [CrossRef]
- Rajappa, M.; Chandrashekar, L.; Sundar, I.; Munisamy, M.; Ananthanarayanan, P.H.; Thappa, D.M.; Ch Toi, P. Platelet oxidative stress and systemic inflammation in chronic spontaneous urticaria. Clin. Chem. Lab. Med. 2013, 9, 1789–1794. [Google Scholar] [CrossRef]
- Stull, D.E.; McBride, D.; Houghton, K.; Finlay, A.Y.; Gnanasakthy, A.; Balp, M.M. Assessing changes in chronic spontaneous/idiopathic urticaria: Comparisons of patient -reported outcomes using latent growth modeling. Adv. Ther. 2016, 33, 214–224. [Google Scholar] [CrossRef]
- Kasperska-Zajac, A.; Grzanka, A.; Machura, E.; Mazur, B.; Misiolek, M.; Czecior, E.; Kasperski, J.; Jochem, J. Analysis of procalcitonin and CRP concentrations in serum of patients with chronic spontaneous urticaria. Inflamm. Res. 2013, 62, 309–312. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Hirano, T. IL-6 in inflammation, autoimmunity and cancer. Int. Immunol. 2021, 33, 127–148. [Google Scholar] [CrossRef] [PubMed]
- Weller, K.; Groffik, A.; Church, M.K.; Hawro, T.; Krause, K.; Metz, M.; Martus, P.; Casale, T.B.; Staubach, P.; Maurer, M. Development and validation of the Urticaria Control Test: A patient-reported outcome instrument for assessing urticaria control. J. Allergy Clin. Immunol. 2014, 133, 1365–1372.e6. [Google Scholar] [CrossRef]
- Finlay, A.Y.; Khan, G.K. Dermatology Life Quality Index (DLQI)—A simple practical measure for routine clinical use. Clin. Exp. Dermatol. 1994, 19, 210–216. [Google Scholar] [CrossRef]
- Stullui, I.; Gimenez-Arnau, A.; Bartra, J.; Labrador-Horrillo, M.; de Frutos, J.O.; Silvestre, J.F.; Sastre, J.; Velasco, M.; Ferrer, M.; Ballesteros, C.; et al. Psychometric properties of the Spanish version of the once-daily Urticaria Activity Score (UAS) in patients with chronic spontaneous urticaria managed in clinical practice (the EVALUAS study). Health Qual. Life Outcomes 2019, 17, 23. [Google Scholar] [CrossRef]
- Mlynek, A.; Zalewska-Janowska, A.; Martus, P.; Staubach, P.; Zuberbier, T.; Maurer, M. How to assess disease activity in patients with chronic urticaria? Allergy 2008, 63, 777–780. [Google Scholar] [CrossRef]
- Plavsic, A.; Tomic-Spiric, V.; Arandjelovic, S.; Miskovic, R.; Dimitrijevic, M.; Peric-Popadic, A. Biomarkers of disease activity in patients with chronic spontaneous urticaria. Postep. Dermatol. Alergol. 2021, 38, 1017–1022. [Google Scholar] [CrossRef]
- de Montjoye, L.; Darrigade, A.S.; Giménez-Arnau, A.; Herman, A.; Dumoutier, L.; Baeck, M. Correlations between disease activity, autoimmunity and biological parameters in patients with chronic spontaneous urticaria. Eur. Ann. Allergy Clin. Immunol. 2021, 53, 55–66. [Google Scholar] [CrossRef]
- Kolkhir, P.; Altrichter, S.; Hawro, T.; Maurer, M. C-reactive protein is linked to disease activity, impact, and response to treatment in patients with chronic spontaneous urticaria. Allergy 2018, 73, 940–948. [Google Scholar] [CrossRef]
- Brzoza, Z.; Badura-Brzoza, K.; Maurer, M.; Hawro, T.; Weller, K. Chronic spontaneous urticaria activity, impact and control as well as their changes are strongly linked, and these links are not affected by angioedema or comorbid inducible urticaria—Results from the validation of the Polish Urticaria Control Test. World Allergy Organ. J. 2022, 15, 100635. [Google Scholar] [CrossRef]
- Kocatürk, E.; Kızıltaç, U.; Can, P.; Öztaş Kara, R.; Erdem, T.; Kızıltaç, K.; Sahillioğlu, N.; Gelincik, A.; Maurer, M.; Weller, K. Validation of the Turkish version of the Urticaria Control Test: Correlation with other tools and comparison between spontaneous and inducible chronic urticaria. World Allergy Organ. J. 2019, 12, 100009. [Google Scholar] [CrossRef] [PubMed]
- Khoshkhui, M.; Weller, K.; Fadaee, J.; Maurer, M.; Jabbari Azad, F.; Emadzadeh, M. Evaluation of the Reliability and Validity of the Persian Version of Urticaria Control Test (UCT). Iran. J. Allergy Asthma Immunol. 2021, 20, 423–431. [Google Scholar] [CrossRef] [PubMed]
- Dortas Junior, S.D.; Valle, S.O.R.; Weller, K.; Maurer, M.; Lupi, O. Validity, reliability, and interpretability of the Brazilian urticaria control test. Allergy Asthma Proc. 2020, 41, e61–e66. [Google Scholar] [CrossRef] [PubMed]
- Sánchez, J.; Zakzuk, J.; Cardona, R. Evaluation of a Guidelines-Based Approach to the Treatment of Chronic Spontaneous Urticaria. J. Allergy Clin. Immunol. Pract. 2018, 6, 177–182.e1. [Google Scholar] [CrossRef]
- Maurer, M.; Raap, U.; Staubach, P.; Richter-Huhn, G.; Bauer, A.; Oppel, E.M.; Hillen, U.; Baeumer, D.; Reinhardt, M.; Chapman-Rothe, N. Antihistamine-resistant chronic spontaneous urticaria: 1-year data from the AWARE study. Clin. Exp. Allergy 2019, 49, 655–662. [Google Scholar] [CrossRef]
- Grzanka, A.; Machura, E.; Misiolek, M.; Polaniak, R.; Kasperski, J.; Kasperska-Zajac, A. Systemic inflammatory response and calcification markers in patients with long lasting moderate-severe chronic spontaneous urticaria. Eur. J. Dermatol. 2015, 25, 26–28. [Google Scholar] [CrossRef]
- Grieco, T.; Porzia, A.; Paolino, G.; Chello, C.; Sernicola, A.; Faina, V.; Carnicelli, G.; Moliterni, E.; Mainiero, F. IFN-γ/IL-6 and related cytokines in chronic spontaneous urticaria: Evaluation of their pathogenetic role and changes during omalizumab therapy. Int. J. Dermatol. 2020, 59, 590–594. [Google Scholar] [CrossRef]
- Maheshwari, A.; Garg, T.; Chander, R.; Debnath, E. Chronic Spontaneous Urticaria: An Etiopathogenic Study. Indian J. Dermatol. 2022, 67, 92. [Google Scholar] [CrossRef]
- Yanase, Y.; Matsubara, D.; Takahagi, S.; Tanaka, A.; Ozawa, K.; Hide, M. Basophil characteristics as a marker of the pathogenesis of chronic spontaneous urticaria in relation to the coagulation and complement systems. Int. J. Mol. Sci. 2023, 24, 10320. [Google Scholar] [CrossRef]
- Poddighe, D.; Vangelista, L. Effects of omalizumab on basophils: Potential biomarkers in asthma and chronic spontaneous urticaria. Cell. Immunol. 2020, 358, 104215. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Median | Interquartile Range | Minimum | Maximum |
|---|---|---|---|---|
| IL-6 serum | 2.9 | 2.0–4.4 | 1.5 | 12.6 |
| CRP | 1.3 | 0.5–3.0 | 0.2 | 14 |
| ESR | 6 | 4–12.3 | 2 | 28 |
| Once-daily UAS | 2 | 0.3–2 | 0 | 6 |
| UAS 7 | 13.5 | 9–22 | 3 | 30 |
| DLQI | 4 | 2.3–8.8 | 0 | 19 |
| UCT | 9 | 8–10 | 5 | 13 |
| Once-Daily UAS | UAS7 | DLQI | UCT | IL-6 Serum | CRP | ESR | ||
|---|---|---|---|---|---|---|---|---|
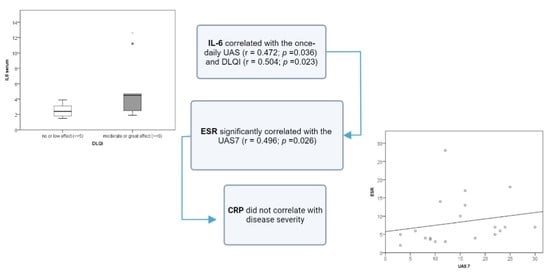
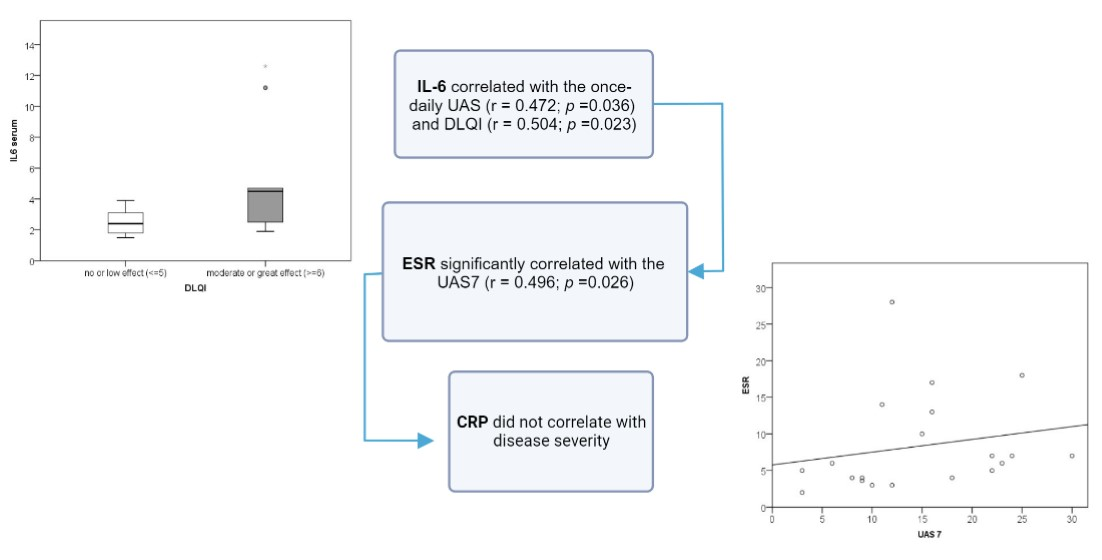
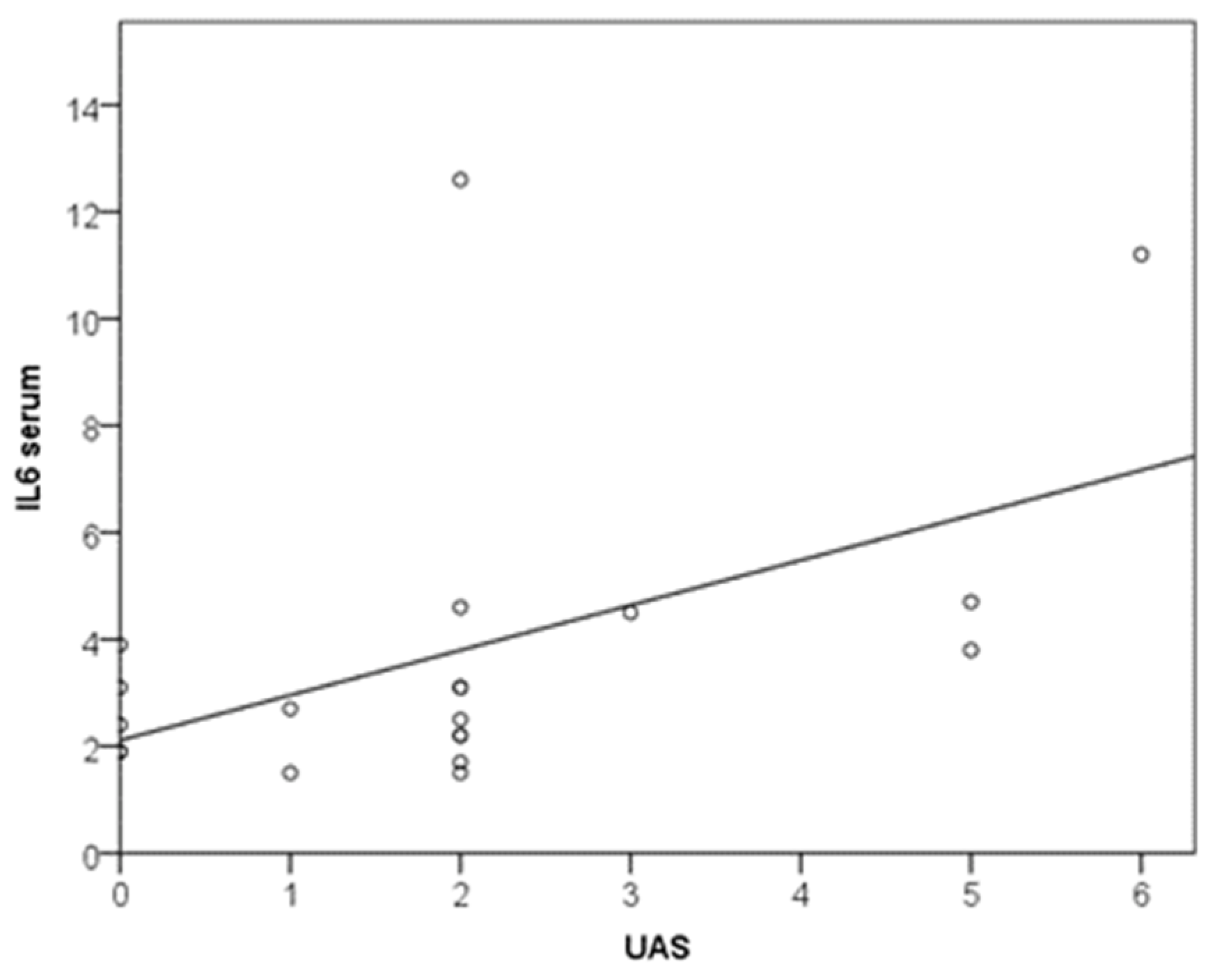
| Once-daily UAS | R | 1 | 0.271 | 0.383 | 0.040 | 0.472 | 0.022 | 0.050 |
| P | 0.247 | 0.096 | 0.866 | 0.036 | 0.927 | 0.833 | ||
| UAS7 | R | 0.271 | 1 | 0.784 | −0.445 | 0.332 | 0.373 | 0.496 |
| P | 0.247 | <0.001 | 0.049 | 0.153 | 0.105 | 0.026 | ||
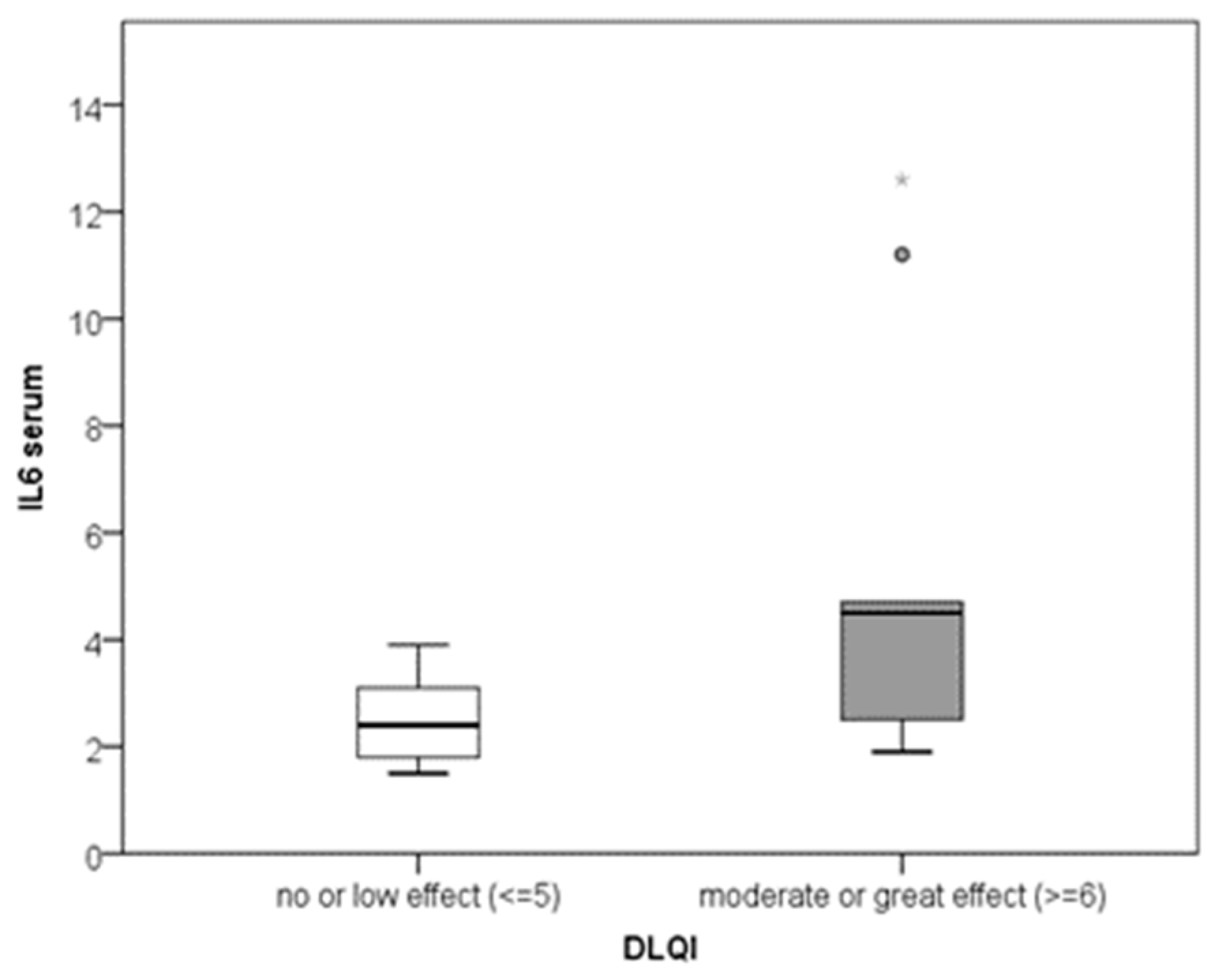
| DLQI | R | 0.383 | 0.784 | 1 | −0.419 | 0.504 | 0.403 | 0.438 |
| P | 0.096 | <0.001 | 0.066 | 0.023 | 0.078 | 0.054 | ||
| UCT | R | 0.04 | −0.445 | −0.419 | 1 | −0.126 | −0.148 | −0.107 |
| P | 0.866 | 0.049 | 0.066 | 0.597 | 0.534 | 0.652 | ||
| IL-6 serum | R | 0.472 | 0.332 | 0.504 | −0.126 | 1 | 0.214 | 0.148 |
| P | 0.036 | 0.153 | 0.023 | 0.597 | 0.364 | 0.532 | ||
| CRP | R | 0.022 | 0.373 | 0.403 | −0.148 | 0.214 | 1 | 0.369 |
| P | 0.927 | 0.105 | 0.078 | 0.534 | 0.364 | 0.110 | ||
| ESR | R | 0.050 | 0.496 | 0.438 | −0.107 | 0.148 | 0.369 | 1 |
| P | 0.833 | 0.026 | 0.054 | 0.652 | 0.532 | 0.110 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuna, M.; Štefanović, M.; Ladika Davidović, B.; Mandušić, N.; Birkić Belanović, I.; Lugović-Mihić, L. Chronic Urticaria Biomarkers IL-6, ESR and CRP in Correlation with Disease Severity and Patient Quality of Life—A Pilot Study. Biomedicines 2023, 11, 2232. https://doi.org/10.3390/biomedicines11082232
Kuna M, Štefanović M, Ladika Davidović B, Mandušić N, Birkić Belanović I, Lugović-Mihić L. Chronic Urticaria Biomarkers IL-6, ESR and CRP in Correlation with Disease Severity and Patient Quality of Life—A Pilot Study. Biomedicines. 2023; 11(8):2232. https://doi.org/10.3390/biomedicines11082232
Chicago/Turabian StyleKuna, Matea, Mario Štefanović, Blaženka Ladika Davidović, Nikolina Mandušić, Ines Birkić Belanović, and Liborija Lugović-Mihić. 2023. "Chronic Urticaria Biomarkers IL-6, ESR and CRP in Correlation with Disease Severity and Patient Quality of Life—A Pilot Study" Biomedicines 11, no. 8: 2232. https://doi.org/10.3390/biomedicines11082232
APA StyleKuna, M., Štefanović, M., Ladika Davidović, B., Mandušić, N., Birkić Belanović, I., & Lugović-Mihić, L. (2023). Chronic Urticaria Biomarkers IL-6, ESR and CRP in Correlation with Disease Severity and Patient Quality of Life—A Pilot Study. Biomedicines, 11(8), 2232. https://doi.org/10.3390/biomedicines11082232