
Differences in Mortality and Sepsis-Associated Organ Dysfunction between Surgical and Non-Surgical Sepsis Patients

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Enrollment
- -
- Age below 18 years;
- -
- Pregnancy or breastfeeding;
- -
- Immunosuppressive drugs and/or chemotherapy within six months prior to enrollment;
- -
- History of myocardial infarction within six weeks before recruitment;
- -
- New York Heart Association stage IV chronic heart failure;
- -
- Human immunodeficiency virus (HIV) infection and/or hepatitis B/C infection;
- -
- End-stage incurable disease;
- -
- Persistent vegetative state (apallic syndrome);
- -
- “Do Not Treat” or “Do Not Resuscitate” order;
- -
- Participation in interventional studies;
- -
- Family member of a study-site employee.
2.2. Data Collection
2.3. Statistical Analysis
3. Results
3.1. Demographics and Patient Baseline Characteristics
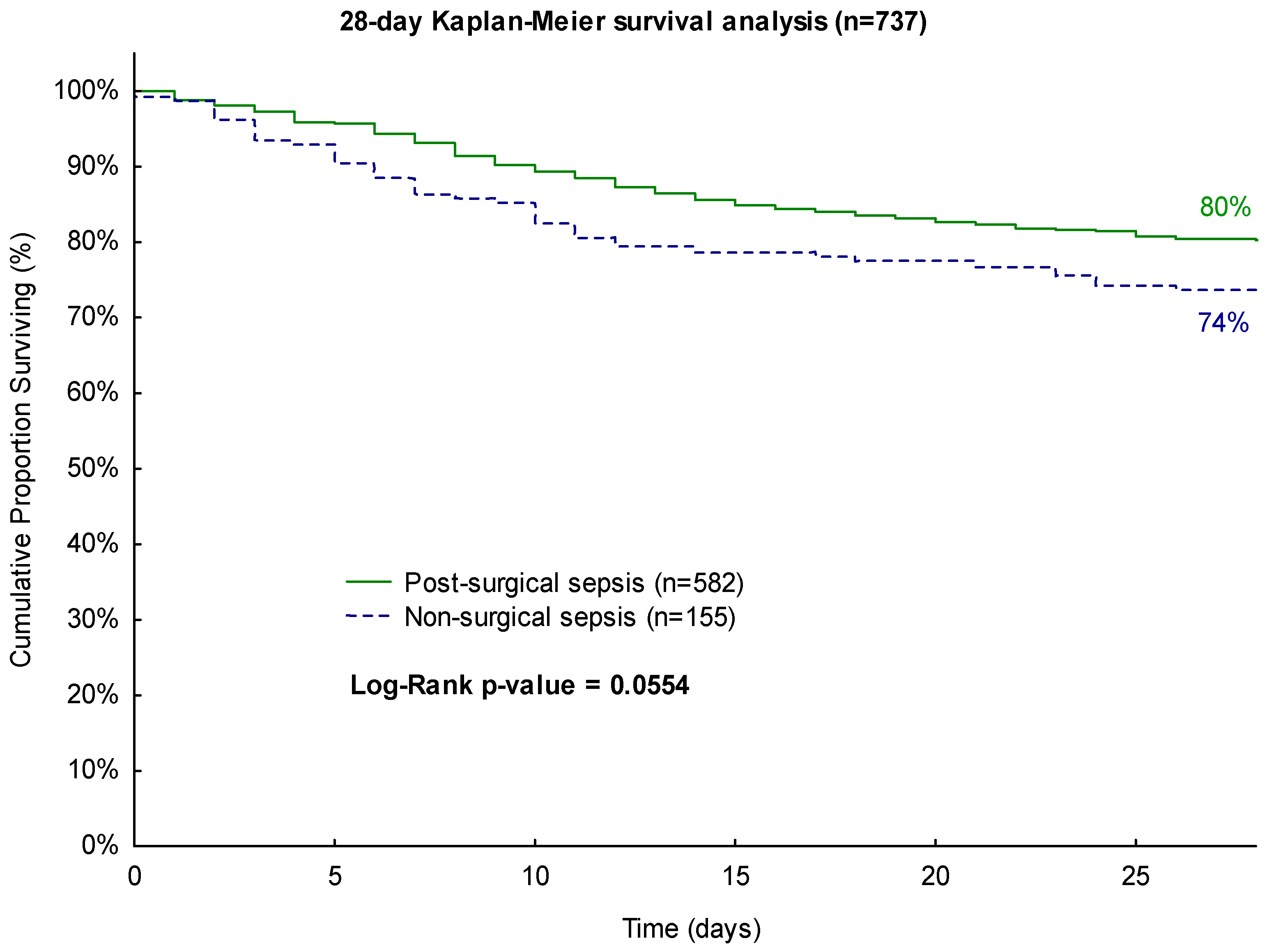
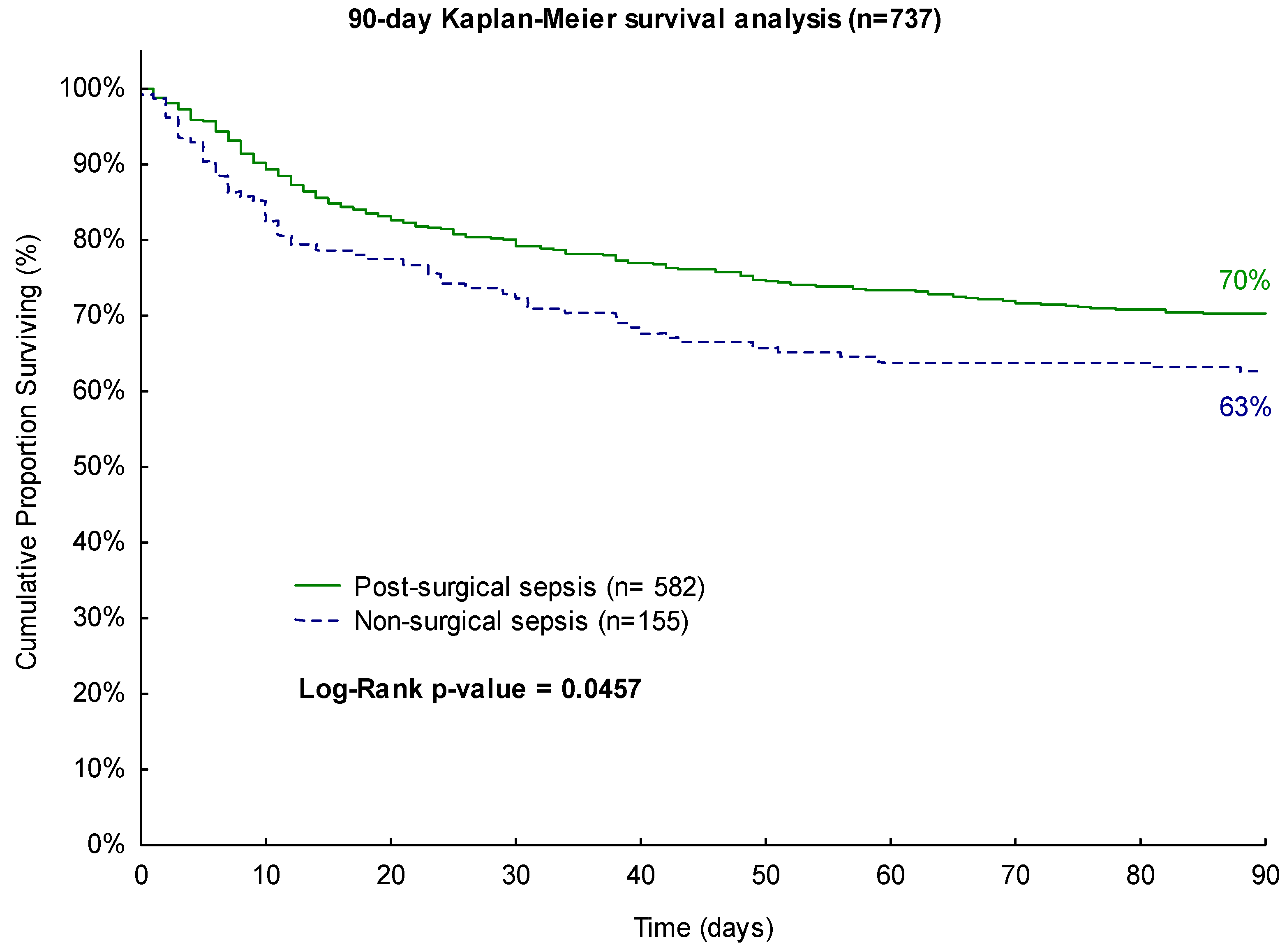
3.2. Survival Analysis
3.3. Disease Severity Analysis
3.4. Multivariate Cox Proportional Hazards Regression Analysis
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Markwart, R.; Saito, H.; Harder, T.; Tomczyk, S.; Cassini, A.; Fleischmann-Struzek, C.; Reichert, F.; Eckmanns, T.; Allegranzi, B. Epidemiology and Burden of Sepsis Acquired in Hospitals and Intensive Care Units: A Systematic Review and Meta-Analysis. Intensive Care Med. 2020, 46, 1536–1551. [Google Scholar] [CrossRef]
- Fleischmann-Struzek, C.; Rose, N.; Freytag, A.; Spoden, M.; Prescott, H.C.; Schettler, A.; Wedekind, L.; Ditscheid, B.; Storch, J.; Born, S.; et al. Epidemiology and Costs of Postsepsis Morbidity, Nursing Care Dependency, and Mortality in Germany, 2013 to 2017. JAMA Netw. Open 2021, 4, e2134290. [Google Scholar] [CrossRef]
- Gaieski, D.F.; Edwards, J.M.; Kallan, M.J.; Carr, B.G. Benchmarking the Incidence and Mortality of Severe Sepsis in the United States. Crit. Care Med. 2013, 41, 1167–1174. [Google Scholar] [CrossRef] [PubMed]
- Levy, M.M.; Evans, L.E.; Rhodes, A. The Surviving Sepsis Campaign Bundle: 2018 Update. Intensive Care Med. 2018, 44, 925–928. [Google Scholar] [CrossRef] [PubMed]
- Varon, J.; Baron, R.M. Sepsis Endotypes: The Early Bird Still Gets the Worm. eBioMedicine 2022, 76, 103832. [Google Scholar] [CrossRef] [PubMed]
- Cohen, N.S.; Bock, J.M.; May, A.K. Sepsis and Postoperative Surgical Site Infections. Surgery 2023, 174, 403–405. [Google Scholar] [CrossRef]
- Vogel, T.R.; Dombrovskiy, V.Y.; Lowry, S.F. Trends in Postoperative Sepsis: Are We Improving Outcomes? Surg. Infect 2009, 10, 71–78. [Google Scholar] [CrossRef]
- Chen, P.-Y.; Luo, C.-W.; Chen, M.-H.; Yang, M.-L.; Kuan, Y.-H. Epidemiological Characteristics of Postoperative Sepsis. Open Med. 2019, 14, 928–938. [Google Scholar] [CrossRef]
- Rhee, C.; Dantes, R.; Epstein, L.; Murphy, D.J.; Seymour, C.W.; Iwashyna, T.J.; Kadri, S.S.; Angus, D.C.; Danner, R.L.; Fiore, A.E.; et al. Incidence and Trends of Sepsis in US Hospitals Using Clinical vs Claims Data, 2009–2014. JAMA 2017, 318, 1241–1249. [Google Scholar] [CrossRef]
- Sinapidis, D.; Kosmas, V.; Vittoros, V.; Koutelidakis, I.M.; Pantazi, A.; Stefos, A.; Katsaros, K.E.; Akinosoglou, K.; Bristianou, M.; Toutouzas, K.; et al. Progression into Sepsis: An Individualized Process Varying by the Interaction of Comorbidities with the Underlying Infection. BMC Infect. Dis. 2018, 18, 242. [Google Scholar] [CrossRef] [PubMed]
- Spoden, M.; Hartog, C.S.; Schlattmann, P.; Freytag, A.; Ostermann, M.; Wedekind, L.; Storch, J.; Reinhart, K.; Günster, C.; Fleischmann-Struzek, C. Occurrence and Risk Factors for New Dependency on Chronic Care, Respiratory Support, Dialysis and Mortality in the First Year After Sepsis. Front. Med. 2022, 9, 878337. [Google Scholar] [CrossRef] [PubMed]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef] [PubMed]
- Levy, M.M.; Fink, M.P.; Marshall, J.C.; Abraham, E.; Angus, D.; Cook, D.; Cohen, J.; Opal, S.M.; Vincent, J.-L.; Ramsay, G.; et al. 2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference. Crit. Care Med. 2003, 31, 1250–1256. [Google Scholar] [CrossRef]
- Mewes, C.; Runzheimer, J.; Böhnke, C.; Büttner, B.; Hinz, J.; Quintel, M.; Mansur, A. Association of Sex Differences with Mortality and Organ Dysfunction in Patients with Sepsis and Septic Shock. J. Pers. Med. 2023, 13, 836. [Google Scholar] [CrossRef] [PubMed]
- Hinz, J.; Büttner, B.; Kriesel, F.; Steinau, M.; Popov, A.F.; Ghadimi, M.; Beissbarth, T.; Tzvetkov, M.; Bergmann, I.; Mansur, A. The FER Rs4957796 TT Genotype Is Associated with Unfavorable 90-Day Survival in Caucasian Patients with Severe ARDS Due to Pneumonia. Sci. Rep. 2017, 7, 9887. [Google Scholar] [CrossRef] [PubMed]
- Kristof, K.; Büttner, B.; Grimm, A.; Mewes, C.; Schmack, B.; Popov, A.F.; Ghadimi, M.; Beissbarth, T.; Hinz, J.; Bergmann, I.; et al. Anaemia Requiring Red Blood Cell Transfusion Is Associated with Unfavourable 90-Day Survival in Surgical Patients with Sepsis. BMC Res. Notes 2018, 11, 879. [Google Scholar] [CrossRef]
- Mewes, C.; Böhnke, C.; Alexander, T.; Büttner, B.; Hinz, J.; Popov, A.-F.; Ghadimi, M.; Beißbarth, T.; Raddatz, D.; Meissner, K.; et al. Favorable 90-Day Mortality in Obese Caucasian Patients with Septic Shock According to the Sepsis-3 Definition. J. Clin. Med. 2019, 9, 46. [Google Scholar] [CrossRef]
- Mewes, C.; Büttner, B.; Hinz, J.; Alpert, A.; Popov, A.F.; Ghadimi, M.; Beissbarth, T.; Tzvetkov, M.; Shen-Orr, S.; Bergmann, I.; et al. The CTLA-4 Rs231775 GG Genotype Is Associated with Favorable 90-Day Survival in Caucasian Patients with Sepsis. Sci. Rep. 2018, 8, 15140. [Google Scholar] [CrossRef]
- Mewes, C.; Alexander, T.; Büttner, B.; Hinz, J.; Alpert, A.; Popov, A.-F.; Ghadimi, M.; Beißbarth, T.; Tzvetkov, M.; Grade, M.; et al. TIM-3 Genetic Variants Are Associated with Altered Clinical Outcome and Susceptibility to Gram-Positive Infections in Patients with Sepsis. Int. J. Mol. Sci. 2020, 21, 8318. [Google Scholar] [CrossRef]
- Mewes, C.; Alexander, T.; Büttner, B.; Hinz, J.; Alpert, A.; Popov, A.-F.; Beißbarth, T.; Tzvetkov, M.; Grade, M.; Quintel, M.; et al. Effect of the Lymphocyte Activation Gene 3 Polymorphism Rs951818 on Mortality and Disease Progression in Patients with Sepsis-A Prospective Genetic Association Study. J. Clin. Med. 2021, 10, 5302. [Google Scholar] [CrossRef] [PubMed]
- Runzheimer, J.; Mewes, C.; Büttner, B.; Hinz, J.; Popov, A.-F.; Ghadimi, M.; Kristof, K.; Beissbarth, T.; Schamroth, J.; Tzvetkov, M.; et al. Lack of an Association between the Functional Polymorphism TREM-1 Rs2234237 and the Clinical Course of Sepsis among Critically Ill Caucasian Patients–A Monocentric Prospective Genetic Association Study. J. Clin. Med. 2019, 8, 301. [Google Scholar] [CrossRef] [PubMed]
- Brakenridge, S.C.; Efron, P.A.; Cox, M.C.; Stortz, J.A.; Hawkins, R.B.; Ghita, G.; Gardner, A.; Mohr, A.M.; Anton, S.D.; Moldawer, L.L.; et al. Current Epidemiology of Surgical Sepsis: Discordance Between Inpatient Mortality and 1-Year Outcomes. Ann. Surg. 2019, 270, 502–510. [Google Scholar] [CrossRef] [PubMed]
- Finks, J.F.; Osborne, N.H.; Birkmeyer, J.D. Trends in Hospital Volume and Operative Mortality for High-Risk Surgery. N. Engl. J. Med. 2011, 364, 2128–2137. [Google Scholar] [CrossRef]
- Motzkus, C.A.; Luckmann, R. Does Infection Site Matter? A Systematic Review of Infection Site Mortality in Sepsis. J. Intensive Care Med. 2017, 32, 473–479. [Google Scholar] [CrossRef] [PubMed]
- Leligdowicz, A.; Dodek, P.M.; Norena, M.; Wong, H.; Kumar, A.; Kumar, A.; Co-operative Antimicrobial Therapy of Septic Shock Database Research Group. Association between Source of Infection and Hospital Mortality in Patients Who Have Septic Shock. Am. J. Respir. Crit. Care Med. 2014, 189, 1204–1213. [Google Scholar] [CrossRef]
- Stortz, J.A.; Cox, M.C.; Hawkins, R.B.; Ghita, G.L.; Brumback, B.A.; Mohr, A.M.; Moldawer, L.L.; Efron, P.A.; Brakenridge, S.C.; Moore, F.A. Phenotypic Heterogeneity by Site of Infection in Surgical Sepsis: A Prospective Longitudinal Study. Crit. Care 2020, 24, 203. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | All (n = 737) | Surgical (n = 582) | Non-Surgical (n = 155) | p-Value |
|---|---|---|---|---|
| Basic Conditions | ||||
| Age (years) | 63 ± 15 | 64 ± 15 | 62 ± 15 | 0.2778 |
| Gender (% male) | 66 | 65 | 66 | 0.8180 |
| Body mass index (kg/m2) | 28 ± 7 | 27 ± 6 | 30 ± 10 | 0.0354 |
| Septic Shock (%) | 51 | 49 | 57 | 0.0841 |
| Severity on Sepsis Onset (Day 1) | ||||
| SOFA score | 10 ± 4 | 9 ± 4 | 11 ± 4 | <0.001 |
| APACHE II score | 22 ± 7 | 21 ± 7 | 23 ± 7 | <0.001 |
| Use of vasopressor (%) | 70 | 69 | 75 | 0.1024 |
| Mechanical ventilation (%) | 87 | 86 | 87 | 0.8278 |
| Renal replacement therapy (%) | 10 | 10 | 12 | 0.4636 |
| Comorbidities (%) | ||||
| Arterial hypertension | 53 | 53 | 53 | 0.9969 |
| COPD | 15 | 13 | 21 | 0.0208 |
| Bronchial asthma | 2 | 2 | 5 | 0.0136 |
| Renal dysfunction | 10 | 9 | 13 | 0.1597 |
| NIDDM | 8 | 9 | 8 | 0.7350 |
| IDDM | 10 | 10 | 10 | 0.9460 |
| Chronic liver disease | 6 | 6 | 6 | 0.6491 |
| History of myocardial infarction | 6 | 6 | 4 | 0.3010 |
| History of stroke | 5 | 5 | 6 | 0.5265 |
| History of cancer | 14 | 16 | 7 | 0.0062 |
| Medication on Sepsis Onset (%) | ||||
| Statins | 23 | 25 | 17 | 0.0268 |
| Beta-blocker | 37 | 38 | 31 | 0.1075 |
| ACE-inhibitor | 29 | 30 | 25 | 0.2478 |
| Bronchodilator | 10 | 9 | 14 | 0.0627 |
| Diuretics | 33 | 33 | 32 | 0.8004 |
| Anticoagulation during the last 6 months | 26 | 26 | 25 | 0.8094 |
| Site of Infection (%) | ||||
| Lung | 63 | 61 | 72 | <0.001 |
| Abdomen | 19 | 22 | 5 | |
| Bone or soft tissue | 4 | 3 | 5 | |
| Surgical wound | 2 | 2 | 0 | |
| Urogenital | 2 | 2 | 4 | |
| Primary bacteremia | 6 | 5 | 10 | |
| Other | 4 | 5 | 4 |
| Characteristics | All (n = 737) | Surgical (n = 582) | Non-Surgical (n = 155) | p-Value |
|---|---|---|---|---|
| Sepsis Severity | ||||
| SOFA score | 7.2 ± 3.7 | 6.9 ± 3.5 | 8.5 ± 4 | <0.001 |
| Days in septic shock | 1 (0, 2) | 0 (0, 2) | 1 (0, 3) | 0.0285 |
| ICU length of stay | 21 ± 16 | 21 ± 15 | 20 ± 19 | 0.1361 |
| Hospital length of stay | 39 ± 29 | 41 ± 30 | 32 ± 23 | <0.001 |
| Inflammatory Values | ||||
| Leukocytes (1000/µL) | 13.2 ± 5 | 13.2 ± 5 | 13.3 ± 5 | 0.9717 |
| C-reactive Protein (mg/L) (n = 380) | 150.9 ± 85.7 | 151.5 ± 82.7 | 148.4 ± 97.7 | 0.3567 |
| Procalcitonin (ng/dL) (n = 657) | 1 (0.3, 3.4) | 0.9 (0.3, 2.9) | 1.2 (0.4, 5.1) | 0.0102 |
| Respiratory Values | ||||
| SOFA respiratory subscore | 2.0 ± 0.8 | 1.9 ± 0.8 | 2.2 ± 0.8 | <0.001 |
| Patients with mechanical ventilation (%) | 94 | 93 | 97 | 0.0807 |
| Ventilation days/observation days (%) | 68 ± 32 | 66 ± 32 | 77 ± 29 | <0.001 |
| Coagulation | ||||
| SOFA coagulation subscore | 0 (0, 0.5) | 0 (0, 0.54) | 0.1 (0, 0.9) | 0.0335 |
| Thrombocytes (1000/µL) | 292 ± 150 | 304 ± 153 | 246 ± 129 | <0.001 |
| Liver Values | ||||
| SOFA hepatic subscore | 0 (0, 0.4) | 0 (0, 0.4) | 0 (0, 0.5) | 0.3188 |
| Bilirubin (mg/dL) | 0.6 (0.4, 1.1) | 0.6 (0.4, 1.1) | 0.7 (0.4, 1.3) | 0.3229 |
| AST (IU/L) (n = 483) | 57 (35, 112) | 57 (35, 110) | 54 (34, 133) | 0.7879 |
| ALT (IU/L) (n = 713) | 46 (23, 92) | 46 (22, 93) | 43 (21, 88) | 0.6174 |
| Cardiovascular Values | ||||
| SOFA cardiovascular subscore | 1.6 ± 1 | 1.6 ± 1 | 1.9 ± 1.1 | <0.001 |
| Patients with vasopressor treatment (%) | 81 | 80 | 87 | 0.0406 |
| Vasopressor days/observation days (%) | 29 (11, 57) | 28 (10, 54) | 39 (18, 71) | <0.001 |
| Central Nervous System | ||||
| SOFA central nervous system | 2.1 ± 1.1 | 2 ± 1.1 | 2.2 ± 1 | 0.0206 |
| Glasgow Coma Scale (GCS) | 10 ± 3 | 10 ± 3 | 9 ± 3 | 0.0093 |
| Renal Values | ||||
| SOFA renal subscore | 0.2 (0, 1.2) | 0.1 (0, 1) | 0.4 (0, 2) | <0.001 |
| Creatinine (mg/dL) | 1.2 ± 0.9 | 1.2 ± 0.9 | 1.5 ± 1.1 | <0.001 |
| Urine output (mL/d) | 2904 ± 1341 | 3027 ± 1332 | 2444 ± 1279 | <0.001 |
| Urine output (mL/kg/h) | 1.5 ± 0.8 | 1.5 ± 0.8 | 1.2 ± 0.7 | <0.001 |
| Patients with renal replacement therapy (%) | 22 | 20 | 31 | 0.0039 |
| Dialysis days/observation days (%) | 0 (0, 0) | 0 (0, 0) | 0 (0, 1) | 0.0364 |
| 90-Day Mortality | 28-Day Mortality | |||||
|---|---|---|---|---|---|---|
| Variables | HR | 95%-CI | p-Value | HR | 95%-CI | p-Value |
| Age | 1.03 | 1.02–1.04 | <0.001 | 1.03 | 1.02–1.05 | <0.001 |
| Male sex | 1.04 | 0.79–1.37 | 0.7802 | 1.17 | 0.83–1.65 | 0.3683 |
| BMI | 0.99 | 0.97–1.01 | 0.2042 | 0.97 | 0.94–1 | 0.0243 |
| SOFA Day 1 | 1.09 | 1.04–1.13 | <0.001 | 1.09 | 1.04–1.15 | <0.001 |
| APACHE II | 1.03 | 1–1.05 | 0.0629 | 1.03 | 1–1.06 | 0.0762 |
| COPD | 1.08 | 0.77–1.53 | 0.6544 | 1.06 | 0.69–1.62 | 0.7883 |
| Bronchial asthma | 0.41 | 0.13–1.30 | 0.1322 | 0.22 | 0.03–1.55 | 0.1271 |
| History of cancer | 1.44 | 1.01–2.03 | 0.0418 | 1.18 | 0.76–1.85 | 0.4622 |
| Statin therapy | 0.93 | 0.68–1.27 | 0.6435 | 0.79 | 0.54–1.16 | 0.2284 |
| Surgical intervention | 0.73 | 0.53–0.99 | 0.0428 | 0.7 | 0.49–1.01 | 0.0561 |
| 90-Day Mortality | 28-Day Mortality | |||||
|---|---|---|---|---|---|---|
| Variables | HR | 95%-CI | p-Value | HR | 95%-CI | p-Value |
| Age | 1.03 | 1.02–1.04 | <0.001 | 1.03 | 1.02–1.05 | <0.001 |
| Male sex | 0.94 | 0.7–1.27 | 0.7055 | 0.96 | 0.65–1.4 | 0.8238 |
| BMI | 0.98 | 0.96–1 | 0.0965 | 0.97 | 0.94–1 | 0.0421 |
| SOFA Day 1 | 0.86 | 0.81–0.92 | <0.001 | 0.83 | 0.77–0.9 | <0.001 |
| APACHE II | 0.99 | 0.97–1.02 | 0.729 | 1 | 0.96–1.04 | 0.9119 |
| COPD | 1.05 | 0.72–1.54 | 0.7922 | 0.90 | 0.56–1.46 | 0.6702 |
| Bronchial asthma | 0.59 | 018–1.87 | 0.3658 | 0.61 | 0.08–4.49 | 0.625 |
| History of cancer | 2.17 | 1.45–3.25 | <0.001 | 1.91 | 1.09–3.33 | 0.0229 |
| Statin therapy | 1.09 | 0.77–1.53 | 0.6170 | 0.86 | 0.55–1.33 | 0.4863 |
| SOFA score | 1.06 | 0.85–1.31 | 0.6112 | 1.04 | 0.79–1.37 | 0.7644 |
| Days in septic shock | 0.96 | 0.92–1.01 | 0.1231 | 0.94 | 0.88–1 | 0.0494 |
| Hospital length of stay | 0.97 | 0.97–0.98 | <0.001 | 0.93 | 0.92–0.95 | <0.001 |
| Procalcitonin | 1.01 | 1–1.02 | 0.2075 | 1.01 | 1–1.02 | 0.1798 |
| SOFA respiratory subscore | 1.5 | 1.06–2.11 | 0.022 | 1.31 | 0.88–1.94 | 0.1869 |
| Ventilation days/observation days | 0.6 | 0.24–1.46 | 0.2595 | 0.88 | 0.28–2.76 | 0.8316 |
| SOFA coagulation subscore | 1.21 | 0.84–1.74 | 0.296 | 1.13 | 0.72–1.77 | 0.5837 |
| SOFA cardiovascular subscore | 3.31 | 1.71–6.39 | <0.001 | 2.95 | 1.31–6.64 | 0.0092 |
| Vasopressor days/observation days | 0.18 | 0.03–1.22 | 0.0791 | 0.38 | 0.04–3.96 | 0.4199 |
| SOFA central nervous system | 2.36 | 1.65–3.38 | <0.001 | 2.49 | 1.55–4.02 | <0.001 |
| SOFA renal subscore | 1.7 | 1.19–2.41 | 0.0032 | 1.72 | 1.1–2.7 | 0.018 |
| Urine output | 0.87 | 0.63–1.2 | 0.3842 | 0.94 | 0.63–1.39 | 0.75 |
| Dialysis days/observation days | 0.21 | 0.09–0.49 | <0.001 | 0.27 | 0.1–0.77 | 0.0143 |
| Surgical intervention | 1.08 | 0.78–1.5 | 0.6321 | 0.98 | 0.64–1.47 | 0.9052 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mewes, C.; Runzheimer, J.; Böhnke, C.; Büttner, B.; Nemeth, M.; Hinz, J.; Quintel, M.; Mansur, A. Differences in Mortality and Sepsis-Associated Organ Dysfunction between Surgical and Non-Surgical Sepsis Patients. Biomedicines 2023, 11, 2233. https://doi.org/10.3390/biomedicines11082233
Mewes C, Runzheimer J, Böhnke C, Büttner B, Nemeth M, Hinz J, Quintel M, Mansur A. Differences in Mortality and Sepsis-Associated Organ Dysfunction between Surgical and Non-Surgical Sepsis Patients. Biomedicines. 2023; 11(8):2233. https://doi.org/10.3390/biomedicines11082233
Chicago/Turabian StyleMewes, Caspar, Julius Runzheimer, Carolin Böhnke, Benedikt Büttner, Marcus Nemeth, José Hinz, Michael Quintel, and Ashham Mansur. 2023. "Differences in Mortality and Sepsis-Associated Organ Dysfunction between Surgical and Non-Surgical Sepsis Patients" Biomedicines 11, no. 8: 2233. https://doi.org/10.3390/biomedicines11082233
APA StyleMewes, C., Runzheimer, J., Böhnke, C., Büttner, B., Nemeth, M., Hinz, J., Quintel, M., & Mansur, A. (2023). Differences in Mortality and Sepsis-Associated Organ Dysfunction between Surgical and Non-Surgical Sepsis Patients. Biomedicines, 11(8), 2233. https://doi.org/10.3390/biomedicines11082233