


Vitamin A Deficiency and Its Association with Visceral Adiposity in Women

Abstract
1. Introduction
2. Materials and Methods
2.1. Sample Size
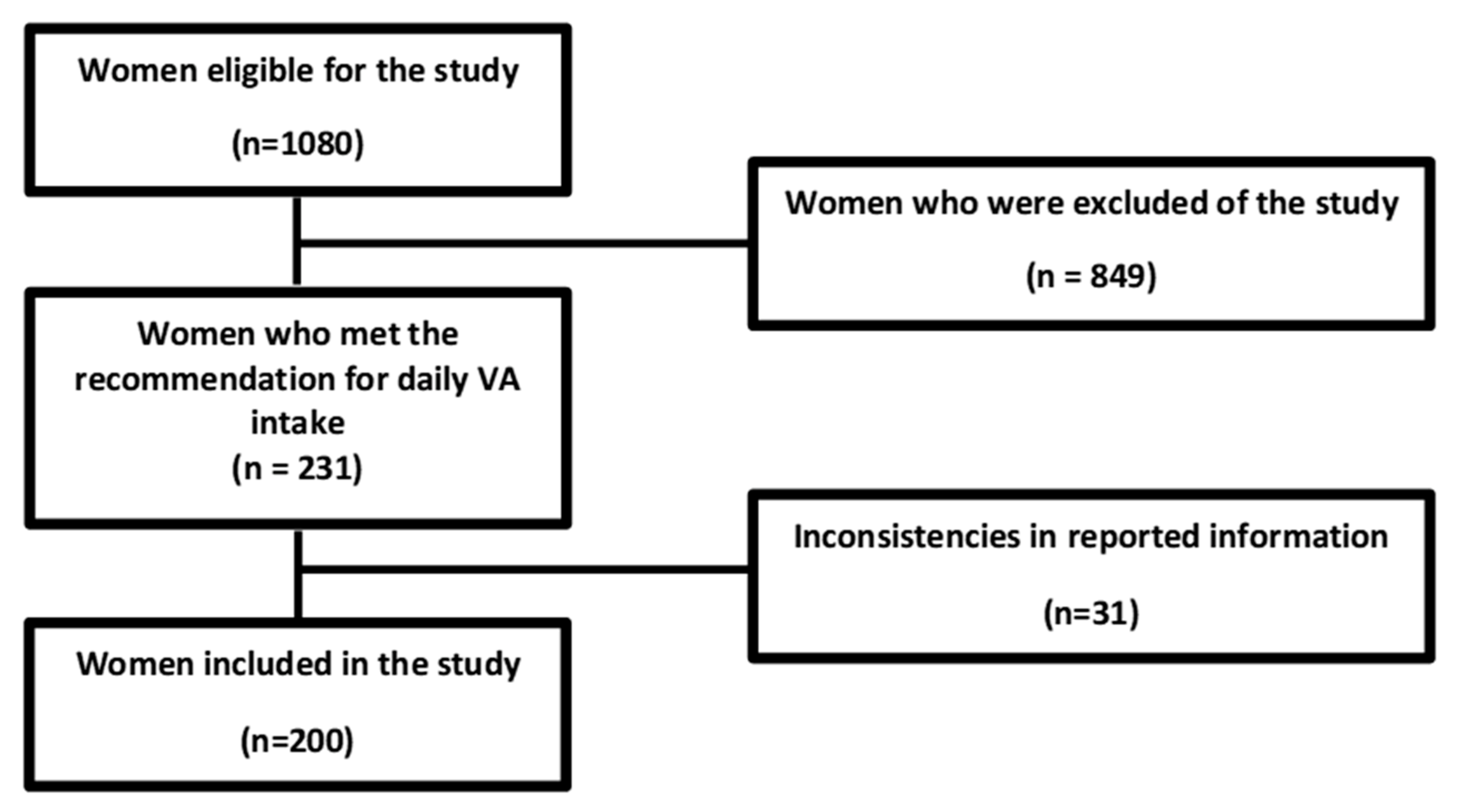
2.2. Selection of Study Participants
Assessment of Vitamin A Dietary
2.3. Assessment of Body Variables
- WC is a widely used anthropometric parameter to assess abdominal fat. It was considered high if >88 cm [1].
- WHtR is applied to diagnose abdominal obesity and plays an important role in assessing the risk of cardiovascular events. It was calculated using WC (in cm) divided by Height (in cm), with a cut-off point >0.5 [21].
- HW is a marker for the simultaneous presence of WC and elevated serum triglyceride levels. It is a simple and practical indicator that can be used as a predictor of metabolic disease. It is characterized by the simultaneous presence of increased WC (≥80 cm) and elevated serum triglyceride (TG) levels (≥1.7 mmol/L) [22].
- BAI evaluates the percentage of body fat in adults. It is a method used to estimate body adiposity and is considered an alternative predictor of body fat in the absence of more complex techniques or more expensive methods. According to the formula: (hip circumference (cm) ÷ height (m) 1.5) − 18; the cut-off point is >33 [23].
- VAI can estimate the distribution of fat and the dysfunction of the visceral adipose tissue, resulting from a specific mathematical formula for each gender. According to the formula: (WC (cm) ÷ (36.58 + (BMI * 1.89) * (TG ÷ 0.81) * (1.52 ÷ HDL-c) for women, where TG and high-density lipoprotein cholesterol (HDL-c) are expressed in mmol/L, with a cut-off point >1 [24].
- LAP can represent lipotoxicity and may be a marker of abdominal adiposity that correlates with central fat accumulation. This index was calculated: (WC (cm) − 58) × (TG (mmol/L)). The cut-off point used was 37.9 [25].
2.4. Biochemical Measurements of Vitamin A
2.5. Other Biochemical Measurements
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). Obesity and Overweight. Revised 18 February 2018. Available online: http://www.who.int/mediacentre/factsheets/fs311/en/ (accessed on 30 July 2022).
- Chooi, Y.C.; Ding, C.; Magkos, F. The epidemiology of obesity. Metabolism 2019, 92, 6–10. [Google Scholar] [CrossRef]
- González-Muniesa, P.; Mártinez-González, M.-A.; Hu, F.B.; Després, J.-P.; Matsuzawa, Y.; Loos, R.J.F.; Moreno, L.A.; Bray, G.A.; Martinez, J.A. Obesity. Nat. Rev. Dis. Prim. 2017, 3, 17034. [Google Scholar] [CrossRef] [PubMed]
- Singh, G.K.; Di Bari, J.N. Marked Disparities in Pre-Pregnancy Obesity and Overweight Prevalence among US Women by Race/Ethnicity, Nativity/Immigrant Status, and Sociodemographic Characteristics, 2012–2014. J. Obes. 2019, 2019, 2419263. [Google Scholar] [CrossRef]
- Kanter, R.; Caballero, B. Global Gender Disparities in Obesity: A Review. Adv Nutr. 2012, 3, 491–498. [Google Scholar] [CrossRef] [PubMed]
- Instituto Brasileiro de Geografia e Estatística-IBGE. Pesquisa Nacional de Saúde 2019 Atenção Primária à Saúde e Informações Antropométricas; Ministério da Saúde do Brazil: Brazilia, Brazil, 2020.
- Yao, N.; Yan, S.; Guo, Y.; Wang, H.; Li, X.; Wang, L.; Hu, W.; Li, B.; Cui, W. The association between carotenoids and subjects with overweight or obesity: A systematic review and meta-analysis. Food Funct. 2021, 12, 4768–4782. [Google Scholar] [CrossRef] [PubMed]
- Gurunathan, U.; Myles, P.S. Limitations of body mass index as an obesity measure of perioperative risk. BJA Br. J. Anaesth. 2016, 116, 319–321. [Google Scholar] [CrossRef]
- Herz, C.T.; Kiefer, F.W. The transcriptional role of vitamin A and the retinoid axis in brown fat function. Front. Endocrinol. 2020, 11, 608. [Google Scholar] [CrossRef] [PubMed]
- Blaner, W.S. Vitamin A signaling and homeostasis in obesity, diabetes, and metabolic disorders. Pharmacol. Ther. 2019, 197, 153–178. [Google Scholar] [CrossRef] [PubMed]
- Godala, M.M.; Materek-Kuśmierkiewicz, I.; Moczulski, D.; Rutkowski, M.; Szatko, F.; Gaszyńska, E.; Tokarski, S.; Kowalski, J. The risk of plasma vitamin A, C, E and D deficiency in patients with metabolic syndrome: A case-control study. Adv. Clin. Exp. Med. 2017, 26, 581–586. [Google Scholar] [CrossRef]
- Bonet, M.L.; Canas, J.A.; Ribot, J.; Palou, A. Carotenoids in Adipose Tissue Biology and Obesity. In Carotenoids in Nature. Subcellular Biochemistry; Stange, C., Ed.; Springer: Cham, Switzerland, 2016; Volume 79. [Google Scholar] [CrossRef]
- Bento, C.; Matos, A.; Cordeiro, A.; Ramalho, A. Serum concentration of vitamin A and its relationship with body adiposity, oxidative stress, and cardiovascular risk in women with recommended dietary intake of vitamin A. Nutr. Hosp. 2020, 37, 1135–1142. (In English) [Google Scholar] [CrossRef]
- Bento, C.; Matos, A.C.; Cordeiro, A.; Ramalho, A. Vitamin A deficiency is associated with body mass index and body adiposity in women with the recommended intake of vitamin A. Nutr. Hosp. 2018, 35, 1072–1078. [Google Scholar] [CrossRef] [PubMed]
- Araujo, M.C.; Verly Junior, E.; Junger, W.L.; Sichieri, R. Independent associations of income and education with nutrient intakes in Brazilian adults: 2008–2009 National Dietary Survey. Public Health Nutr. 2014, 17, 2740–2752. [Google Scholar] [CrossRef] [PubMed]
- Instituto Brasileiro de Geografia e Estatística (IBGE). Pesquisa de Orçamentos Familiares 2017–2018: Análise do Consumo Alimentar Pessoal no Brasil/IBGE, Coordenação deTrabalho e Rendimento; IBGE: Rio de Janeiro, Brazil, 2020.
- Institute of Medicine (IOM). Vitamin A. In Dietary Reference Intakes for Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc; National Academic Press: Washington, DC, USA, 2001; pp. 82–161. [Google Scholar]
- Tabela Brasileira de Composição de Alimentos (TBCA). Universidade de São Paulo (USP). Food Research Center (FoRC). Versão 7.2. São Paulo. 2022. Available online: http://www.fcf.usp.br/tbca (accessed on 6 November 2022).
- Pinheiro, A.B.V.; Lacerda, E.M.D.A.; Benzecry, E.H.; Gomes, M.C.D.S.; Costa, V.M.D. Tabela Para Avaliação de Consumo Alimentar em Medidas Caseiras; Ateneu: São Paulo, Brazil, 2001; Volume 5, p. 352. [Google Scholar]
- International Vitamin A Consultative Group (IVACG). The Annecy Accords to Assess and Control Vitamin A Deficiency: Summary of Recommendations and Clarifications; IVACG: Washington, DC, USA, 2003. [Google Scholar]
- Zeng, Q.; He, Y.; Dong, S.; Zhao, X.; Chen, Z.; Song, Z.; Chang, G.; Yang, F.; Wang, Y. Optimal cut-off values of BMI, waist circumference and waist: Height ratio for defining obesity in Chinese adults. Br. J. Nutr. 2014, 112, 1735–1744. [Google Scholar] [CrossRef] [PubMed]
- Freitas, R.S.; Fonseca, M.D.J.M.D.; Schmidt, M.I.; Molina, M.D.C.B.; Almeida, M.D.C.C.D. Fenótipo cintura hipertrigliceridêmica: Fatores associados e comparação com outros indicadores de risco cardiovascular e metabólico no ELSA-Brasil. Cad. De Saúde Pública 2018, 34, e00067617. [Google Scholar] [CrossRef]
- Bergman, R.N.; Stefanovski, D.; Buchanan, T.A.; Sumner, A.E.; Reynolds, J.C.; Sebring, N.G.; Xiang, A.; Watanabe, R.M. A Better Index of Body Adiposity. Obesity 2011, 19, 1083–1089. [Google Scholar] [CrossRef]
- Amato, M.C.; Giordano, C.; Galia, M.; Criscimanna, A.; Vitabile, S.; Midiri, M.; Galluzzo, A.; AlkaMeSy Study Group. Visceral Adiposity Index: A reliable indicator of visceral fat function associated with cardiometabolic risk. Diabetes Care 2010, 33, 920–922. [Google Scholar] [CrossRef]
- Vieira, J.N.; Braz, M.A.D.; Gomes, F.O.; Silva, P.R.D.; Santos, O.T.M.; Rocha, I.M.G.D.; Sousa, I.M.; Fayh, A.P.T. Cardiovascular risk assessment using the lipid accumulation product index among primary healthcare users: A cross-sectional study. Sao Paulo Med. J. 2019, 137, 126–131. [Google Scholar] [CrossRef]
- Mason, J. Vitamins, Trace Minerals, and other Micronutrients in Goldman’s Cecil Medicine, 24th ed.; Elsevier: Amsterdam, The Netherlands, 2012. [Google Scholar] [CrossRef]
- Wang, C.; Ling, C.-W.; Ding, D.; Li, Y.-H.; Cao, W.-T.; Tang, X.-Y.; Chen, Y.-M. Associations of Serum Carotenoids with DXA-Derived Body Fat and Fat Distribution in Chinese Adults: A Prospective Study. J. Acad. Nutr. 2020, 120, 985–1001. [Google Scholar] [CrossRef]
- Ide, J.; Gagnon, A.; Molgat, A.S.; Landry, A.; Foster, C.; Sorisky, A. Macrophage-conditioned medium inhibits the activation of cyclindependent kinase 2 by adipogenic inducers in 3T3-L1 preadipocytes. J. Cell Physiol. 2011, 226, 2297–2306. [Google Scholar] [CrossRef]
- Saini, R.K.; Prasad, P.; Lokesh, V.; Shang, X.; Shin, J.; Keum, Y.-S.; Lee, J.-H. Carotenoids: Dietary Sources, Extraction, Encapsulation, Bioavailability, and Health Benefits—A Review of Recent Advancements. Antioxidants 2022, 11, 795. [Google Scholar] [CrossRef]
- Mounien, L.; Tourniaire, F.; Landrier, J.-F. Anti-Obesity Effect of Carotenoids: Direct Impact on Adipose Tissue and Adipose Tissue-Driven Indirect Effects. Nutrients 2019, 11, 1562. [Google Scholar] [CrossRef] [PubMed]
- Da Cruz, B.; Cardozo, L.F.M.D.F.; Magliano, D.C.; Stockler-Pinto, M.B. Nutritional strategies to modulate inflammation pathways via regulation of peroxisome proliferator-activated receptor β/δ. Nutr. Rev. 2020, 78, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Bonet, M.L.; Ribot, J.; Galmés, S.; Serra, F.; Palou, A. Carotenoids and carotenoid conversion products in adipose tissue biology and obesity: Pre-clinical and human studies. Biochim. Biophys Acta Mol. Cell Biol. Lipids 2020, 1865, 158676. [Google Scholar] [CrossRef]
- Checa, J.; Aran, J.M. Reactive Oxygen Species: Drivers of Physiological and Pathological Processes. J. Inflamm. 2020, 13, 1057–1073. [Google Scholar] [CrossRef] [PubMed]
- Neeland, I.J.; Ross, R.; Després, J.-P.; Matsuzawa, Y.; Yamashita, S.; Shai, I.; Seidell, J.; Magni, P.; Santos, R.D.; Arsenault, B.; et al. Visceral and ectopic fat, atherosclerosis, and cardiometabolic disease: A position statement. Lancet Diabetes Endocrinol. 2019, 7, 715–725. [Google Scholar] [CrossRef]
- Ellulu, M.S.; Patimah, I.; Khaza’ai, H.; Rahmat, A.; Abed, Y. Obesity and inflammation: The linking mechanism and the complications. Arch. Med. Sci. 2017, 13, 851–863. [Google Scholar] [CrossRef]
- Haaker, M.W.; Vaandrager, A.B.; Helms, J.B. Retinoids in health and disease: A role for hepatic stellate cells in affecting retinoid levels. Biochim. Biophys Acta Mol. Cell Biol. Lipids 2020, 1865, 158674. [Google Scholar] [CrossRef]
- Elffers, T.W.; De Mutsert, R.; Lamb, H.J.; De Roos, A.; Van Dijk, K.W.; Rosendaal, F.R.; Jukema, J.W.; Trompet, S. Body fat distribution, in particular visceral fat, is associated with cardiometabolic risk factors in obese women. PLoS ONE 2017, 12, e0185403. [Google Scholar] [CrossRef]
- Stefan, N. Causes, consequences, and treatment of metabolically unhealthy fat distribution. Lancet Diabetes Endocrinol. 2020, 8, 616–627. [Google Scholar] [CrossRef]
- Schorr, M.; Dichtel, L.E.; Gerweck, A.V.; Valera, R.D.; Torriani, M.; Miller, K.K.; Bredella, M.A. Sex differences in body composition and association with cardiometabolic risk. Biol. Sex Differ. 2018, 9, 28. [Google Scholar] [CrossRef]
- De Mutsert, R.; Gast, K.; Widya, R.; de Koning, E.; Jazet, I.; Lamb, H.; le Cessie, S.; de Roos, A.; Smit, J.; Rosendaal, F.; et al. Associations of abdominal subcutaneous and visceral fat with insulin resistance and secretion differ between men and women: The Netherlands epidemiology of obesity study. Metab Syndr. Relat. Disord. 2018, 16, 54–63. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, B.; Sultana, R.; Greene, M.W. Adipose tissue and insulin resistance in obese. Biomed Pharm. 2021, 137, 111315. [Google Scholar] [CrossRef] [PubMed]
- Kabat, G.C.; Heo, M.; Ochs-Balcom, H.M.; LeBoff, M.S.; Mossavar-Rahmani, Y.; Adams-Campbell, L.L.; Nassir, R.; Ard, J.; Zaslavsky, O.; Rohan, T.E. Longitudinal association of measures of adiposity with serum antioxidant concentrations in postmenopausal women. Eur. J. Clin. Nutr. 2016, 70, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Thomas-Valdés, S.; das Graças, V.; Tostes, M.; Anunciação, P.C.; da Silva, B.P.; Sant’Ana, H.M.P. Association between vitamin deficiency and metabolic disorders related to obesity. Crit. Rev. Food Sci. Nutr. 2017, 57, 3332–3343. [Google Scholar] [CrossRef]
- Ribamar, A.; Cruz, S.; Bento, C.; Ramalho, A. Visceral and body adiposity are negatively associated with vitamin A nutritional status independently of Body Mass Index and recommended intake of vitamin A in Brazilian Women. J. Nutr. Biochem. 2022, 109, 109–120. [Google Scholar] [CrossRef]


{kind=link}
| Variables | NW (n = 80) | OW (n = 40) | OI (n = 68) | OII (n = 12) | p-value |
|---|---|---|---|---|---|
| BMI (kg/m2) | 22.8 ± 1.1 | 27.3 ± 1.2 | 33.1 ± 0.9 | 37.7 ± 0.9 | <0.001 |
| Age (years) | 48.2 ± 5.7 | 50.8 ± 5.6 | 50.8 ± 5.1 | 54.3 ± 3.7 | <0.001 |
| WC (cm) | 79.4 ± 6.1 | 112.4 ± 10.3 | 120.6 ± 10.2 | 121.1 ± 8.0 | <0.001 |
| WHtR | 0.5 ± 0.0 | 0.7 ± 0.1 | 0.7 ± 0.1 | 0.7 ± 0.0 | <0.001 |
| VAI | 3.4 ± 0.7 | 4.8 ± 0.7 | 5.1 ± 0.8 | 5.3 ± 0.4 | <0.001 |
| BAI | 22.4 ± 4.3 | 36.6 ± 6.3 | 37.3 ± 5.0 | 37.7 ± 3.6 | <0.001 |
| LAP | 33.8 ± 12.2 | 101.2 ± 22.2 | 137.2 ± 35.8 | 165.1 ± 30.4 | <0.001 |
| Retinol equivalent (μg/day) | 795.2 ± 49.9 | 781.5 ± 34.5 | 745.8 ± 72.8 | 740.1 ± 32.3 | 0.243 |
| BMI Groups | Retinol (μmol/L) | β-Carotene (μg/dL) |
|---|---|---|
| NW (n = 80) | 1.3 ± 0.2 | 61.2 ± 12.1 |
| OW (n = 40) | 1.0 ± 0.3 | 43.5 ± 5.9 |
| OI (n = 68) | 0.8 ± 0.3 | 35.9 ± 4.3 |
| OII (n = 12) | 0.7 ± 0.2 | 32.0 ± 0.9 |
| p-value | <0.001 | <0.001 |
| BMI Groups | WC (cm) | WHtR | VAI | BAI | LAP |
|---|---|---|---|---|---|
| NW (n = 80) | Retinol LConc 88.5 ± 14.5 Adq 78.6 ± 4.3 | Retinol LConc 0.6 ± 0.1 Adq 0.5 ± 0.0 | Retinol LConc 3.4 ± 0.9 Adq 3.4 ± 0.7 | Retinol LConc 27.4 ± 5.8 Adq 22.0 ± 3.9 | Retinol LConc 55.3 ± 31.0 Adq 32.1 ± 7.3 |
| β-carotene LConc 83.3 ± 11.1 Adq 78.7 ± 4.5 | β-carotene LConc 0.5 ± 0.1 Adq 0.5 ± 0.0 | β-carotene LConc 3.4 ± 0.8 Adq 3.4 ± 0.7 | β-carotene LConc 24.6 ± 5.4 Adq 22.0 ± 4.0 | β-carotene LConc 43.4 ± 24.3 Adq 32.1 ± 7.6 | |
| p-value < 0.001 | p-value < 0.001 | p-value < 0.001 | p-value < 0.001 | p-value < 0.001 | |
| Retinol LConc 111.2 ± 11.3 Adq 113.2 ± 9.6 | Retinol LConc 0.7 ± 0.1 Adq 0.7 ± 0.0 | Retinol LConc 5.1 ± 0.6 Adq 4.6 ± 0.7 | Retinol LConc 38.9 ± 7.8 Adq 34.8 ± 4.4 | Retinol LConc 104.3 ± 27.4 Adq 98.9 ± 17.6 | |
| OW (n = 40) | β-carotene LConc 111.0 ± 12.8 Adq 113.6 ± 7.4 p-value < 0.001 | β-carotene LConc 0.7 ± 0.1 Adq 0.7 ± 0.0 p-value < 0.001 | β-carotene LConc 5.1 ± 0.7 Adq 4.6 ± 0.7 p-value < 0.001 | β-carotene LConc 38.6 ± 8.1 Adq 34.7 ± 3.3 p-value < 0.001 | β-carotene LConc 102.8 ± 29.0 Adq 99.7 ± 14.0 p-value < 0.001 |
| OI (n = 68) | Retinol LConc 121.5 ± 11.2 Adq 117.8 ± 4.9 | Retinol LConc 0.7 ± 0.1 Adq 0.7 ± 0.0 | Retinol LConc 5.3 ± 0.8 Adq 4.4 ± 0.4 | Retinol LConc 37.7 ± 5.4 Adq 36.0 ± 3.4 | Retinol LConc 145.8 ± 36.6 Adq 109.4 ± 9.4 |
| β-carotene LConc 121.0 ± 10.9 Adq 118.5 ± 3.4 | β-carotene LConc 0.7 ± 0.1 Adq 0.7 ± 0.0 | β-carotene LConc 5.3 ± 0.8 Adq 4.4 ± 0.4 | β-carotene LConc 37.3 ± 5.3 Adq 37.2 ± 2.9 | β-carotene LConc 142.2 ± 36.5 Adq 108.4 ± 7.3 | |
| p-value < 0.001 | p-value < 0.001 | p-value < 0.001 | p-value < 0.001 | p-value < 0.001 | |
| OII (n = 12) | Retinol LConc 121.1 ± 8.0 | Retinol LConc 0.7 ± 0.0 | Retinol LConc 5.3 ± 0.4 | Retinol LConc 37.7 ± 3.6 | Retinol 165.1 ± 30.4 |
| β-carotene LConc 121.1 ± 8.1 | β-carotene LConc 0.7 ± 0.0 | β-carotene LConc 5.3 ± 0.4 | β-carotene LConc 37.7 ± 3.6 | β-carotene LConc 165.1 ± 30.4 | |
| p-value < 0.001 | p-value < 0.001 | p-value < 0.001 | p-value < 0.001 | p-value < 0.001 |
| Body Adiposity Parameters | Retinol (μmol/L) | β-Carotene (μg/dL) | ||
|---|---|---|---|---|
| r | p | r | p | |
| BMI (Kg/m2) | −0.65 | <0.001 | −0.76 | <0.001 |
| WC (cm) | −0.71 | <0.001 | −0.77 | <0.001 |
| WHtR | −0.72 | <0.001 | −0.73 | <0.001 |
| VAI | −0.73 | <0.001 | −0.68 | <0.001 |
| BAI | −0.70 | <0.001 | −0.71 | <0.001 |
| LAP | −0.81 | <0.001 | −0.78 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Góes, É.; Cordeiro, A.; Bento, C.; Ramalho, A. Vitamin A Deficiency and Its Association with Visceral Adiposity in Women. Biomedicines 2023, 11, 991. https://doi.org/10.3390/biomedicines11030991
Góes É, Cordeiro A, Bento C, Ramalho A. Vitamin A Deficiency and Its Association with Visceral Adiposity in Women. Biomedicines. 2023; 11(3):991. https://doi.org/10.3390/biomedicines11030991
Chicago/Turabian StyleGóes, Érica, Adryana Cordeiro, Claudia Bento, and Andrea Ramalho. 2023. "Vitamin A Deficiency and Its Association with Visceral Adiposity in Women" Biomedicines 11, no. 3: 991. https://doi.org/10.3390/biomedicines11030991
APA StyleGóes, É., Cordeiro, A., Bento, C., & Ramalho, A. (2023). Vitamin A Deficiency and Its Association with Visceral Adiposity in Women. Biomedicines, 11(3), 991. https://doi.org/10.3390/biomedicines11030991