

Prognostic Factors of Long-Term Outcomes after Primary Chemo-Radiotherapy in Non-Metastatic Anal Squamous Cell Carcinoma: An International Bicentric Cohort

 , , ,
, , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Anal Cancer Cohort
2.2. Treatment and Follow-Up
2.3. HPV Detection and Genotyping
2.4. Statistical Analysis
3. Results
3.1. Patients
3.2. Treatment and Response
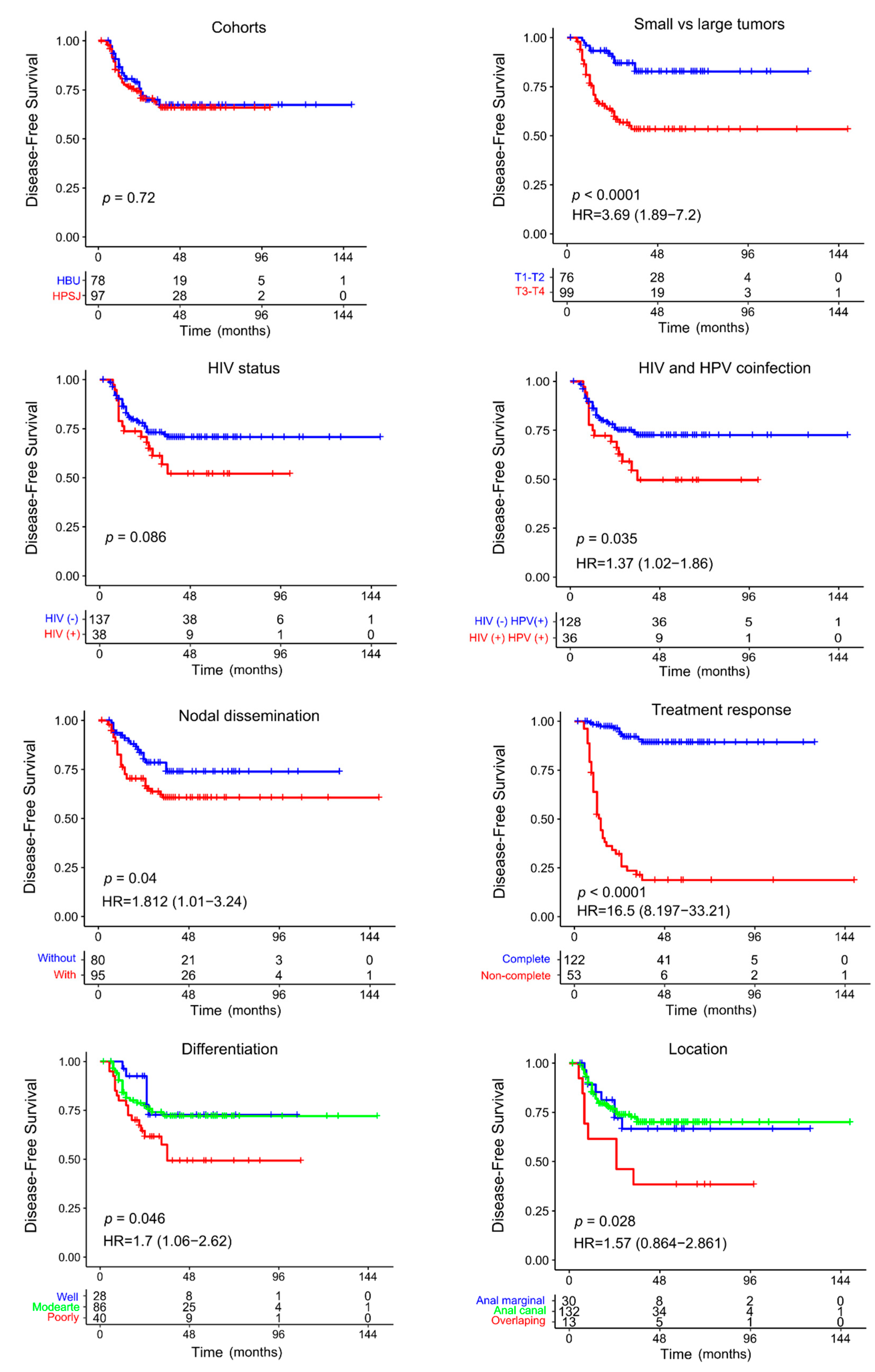
3.3. Outcomes during Follow-Up
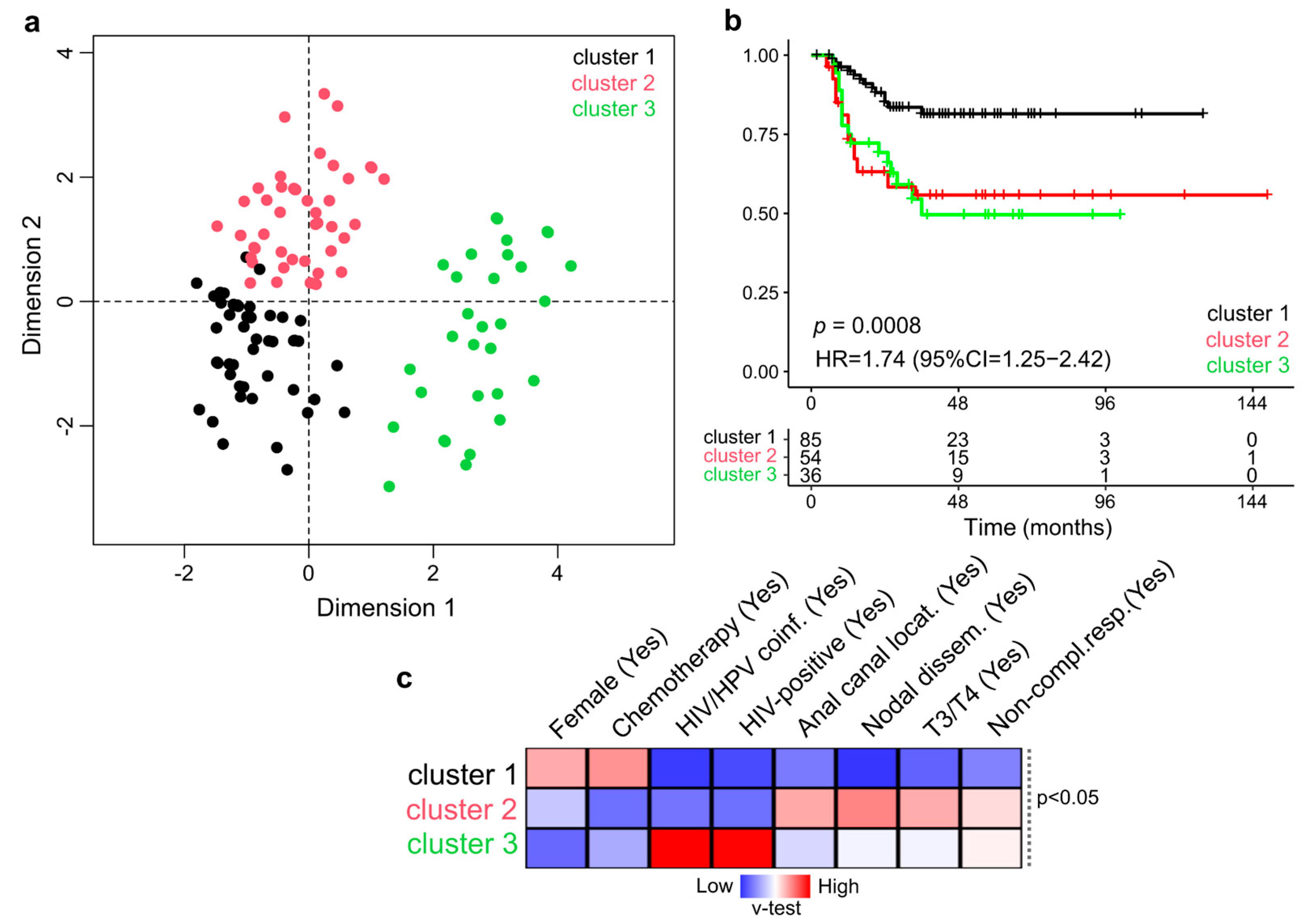
3.4. Multivariate Analysis of NM-ASCC Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Islami, F.; Ferlay, J.; Lortet-Tieulent, J.; Bray, F.; Jemal, A. International trends in anal cancer incidence rates. Int. J. Epidemiol. 2017, 46, 924–938. [Google Scholar] [CrossRef] [PubMed]
- Nelson, V.M.; Benson, A.B. Epidemiology of Anal Canal Cancer. Surg. Oncol. Clin. N. Am. 2017, 26, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Grave, A.; Blanc, J.; De Bari, B.; Pernot, M.; Boulbair, F.; Noirclerc, M.; Vienot, A.; Kim, S.; Borg, C.; Boustani, J. Long-Term Disease Control After locoregional Pelvic Chemoradiation in Patients with Advanced Anal Squamous Cell Carcinoma. Front. Oncol. 2022, 12, 918271. [Google Scholar] [CrossRef] [PubMed]
- Eng, C.; Messick, C.; Glynne-Jones, R. The Management and Prevention of Anal Squamous Cell Carcinoma. Am. Soc. Clin. Oncol. Educ. Book 2019, 39, 216–225. [Google Scholar] [CrossRef]
- Kang, Y.-J.; Smith, M.; Canfell, K. Anal cancer in high-income countries: Increasing burden of disease. PLoS ONE 2018, 13, e0205105. [Google Scholar] [CrossRef]
- Clifford, G.M.; Georges, D.; Shiels, M.S.; Engels, E.A.; Albuquerque, A.; Poynten, I.M.; De Pokomandy, A.; Easson, A.M.; Stier, E.A. A meta-analysis of anal cancer incidence by risk group: Toward a unified anal cancer risk scale. Int. J. Cancer 2021, 148, 38–47. [Google Scholar] [CrossRef]
- De Martel, C.; Plummer, M.; Vignat, J.; Franceschi, S. Worldwide burden of cancer attributable to HPV by site, country and HPV type. Int. J. Cancer 2017, 141, 664–670. [Google Scholar] [CrossRef]
- Machalek, D.A.; Poynten, M.; Jin, F.; Fairley, C.K.; Farnsworth, A.; Garland, S.M.; Hillman, R.J.; Petoumenos, K.; Roberts, J.; Tabrizi, S.N.; et al. Anal human papillomavirus infection and associated neoplastic lesions in men who have sex with men: A systematic review and meta-analysis. Lancet Oncol. 2012, 13, 487–500. [Google Scholar] [CrossRef]
- Rao, S.; Guren, M.; Khan, K.; Brown, G.; Renehan, A.; Steigen, S.; Deutsch, E.; Martinelli, E.; Arnold, D. Anal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2021, 32, 1087–1100. [Google Scholar] [CrossRef]
- Cancer of the Anus, Anal Canal, and Anorectum—Cancer Stat Facts. SEER. Available online: https://seer.cancer.gov/statfacts/html/anus.html (accessed on 6 October 2022).
- Deshmukh, A.A.; Suk, R.; Shiels, M.S.; Sonawane, K.; Nyitray, A.G.; Liu, Y.; Gaisa, M.M.; Palefsky, J.M.; Sigel, K. Recent Trends in Squamous Cell Carcinoma of the Anus Incidence and Mortality in the United States, 2001–2015. JNCI J. Natl. Cancer Inst. 2020, 112, 829–838. [Google Scholar] [CrossRef]
- Spehner, L.; Boustani, J.; Cabel, L.; Doyen, J.; Vienot, A.; Borg, C.; Kim, S. Present and Future Research on Anal Squamous Cell Carcinoma. Cancers 2021, 13, 3895. [Google Scholar] [CrossRef] [PubMed]
- Epidermoid anal cancer: Results from the UKCCCR randomised trial of radiotherapy alone versus radiotherapy, 5-fluorouracil, and mitomycin. UKCCCR Anal Cancer Trial Working Party. UK Co-ordinating Committee on Cancer Research. Lancet 1996, 348, 1049–1054. [CrossRef]
- Bartelink, H.; Roelofsen, F.; Eschwege, F.; Rougier, P.; Bosset, J.F.; Gonzalez, D.G.; Peiffert, D.; Van Glabbeke, M.; Pierart, M. Concomitant radiotherapy and chemotherapy is superior to radiotherapy alone in the treatment of locally advanced anal cancer: Results of a phase III randomized trial of the European Organization for Research and Treatment of Cancer Radiotherapy and Gastrointestinal Cooperative Groups. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 1997, 15, 2040–2049. [Google Scholar]
- Ajani, J.A.; Winter, K.A.; Gunderson, L.L.; Pedersen, J.; Benson, A.B., III; Thomas, C.R., Jr.; Mayer, R.J.; Haddock, M.G.; Rich, D.A.; Willett, C.G. Prognostic factors derived from a prospective database dictate clinical biology of anal cancer: The intergroup trial (RTOG 98-11). Cancer 2010, 116, 4007-13. [Google Scholar] [CrossRef] [PubMed]
- Gunderson, L.L.; Winter, K.A.; Ajani, J.A.; Pedersen, J.E.; Moughan, J.; Benson, A.B.; Thomas, C.R., Jr.; Mayer, R.J.; Haddock, M.G.; Rich, T.A.; et al. Long-term update of US GI intergroup RTOG 98-11 phase III trial for anal carcinoma: Survival, relapse, and colostomy failure with concurrent chemoradiation involving fluorouracil/mitomycin versus fluorouracil/cisplatin. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2012, 30, 4344–4351. [Google Scholar] [CrossRef] [PubMed]
- Peiffert, D.; Tournier-Rangeard, L.; Gérard, J.-P.; Lemanski, C.; François, E.; Giovannini, M.; Cvitkovic, F.; Mirabel, X.; Bouché, O.; Luporsi, E.; et al. Induction chemotherapy and dose intensification of the radiation boost in locally advanced anal canal carcinoma: Final analysis of the randomized UNICANCER ACCORD 03 trial. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2012, 30, 1941–1948. [Google Scholar] [CrossRef]
- Garg, M.K.; Zhao, F.; Sparano, J.A.; Palefsky, J.; Whittington, R.; Mitchell, E.P.; Mulcahy, M.F.; Armstrong, K.I.; Nabbout, N.H.; Kalnicki, S.; et al. Cetuximab Plus Chemoradiotherapy in Immunocompetent Patients with Anal Carcinoma: A Phase II Eastern Cooperative Oncology Group–American College of Radiology Imaging Network Cancer Research Group Trial (E3205). J. Clin. Oncol. 2017, 35, 718–726. [Google Scholar] [CrossRef]
- James, R.D.; Glynne-Jones, R.; Meadows, H.M.; Cunningham, D.; Myint, A.S.; Saunders, M.P.; Maughan, T.; McDonald, A.; Essapen, S.; Leslie, M.; et al. Mitomycin or cisplatin chemoradiation with or without maintenance chemotherapy for treatment of squamous-cell carcinoma of the anus (ACT II): A randomised, phase 3, open-label, 2×2 factorial trial. Lancet Oncol. 2013, 14, 516–524. [Google Scholar] [CrossRef]
- Osborne, M.C.; Maykel, J.; Johnson, E.K.; Steele, S.R. Anal squamous cell carcinoma: An evolution in disease and management. World J. Gastroenterol. 2014, 20, 13052–13059. [Google Scholar] [CrossRef]
- Nilsson, M.P.; Nilsson, E.D.; Johnsson, A.; Leon, O.; Gunnlaugsson, A.; Scherman, J. Patterns of recurrence in anal cancer: A detailed analysis. Radiat Oncol. 2020, 15, 125. [Google Scholar] [CrossRef]
- Iseas, S.; Golubicki, M.; Robbio, J.; Ruiz, G.; Guerra, F.; Mariani, J.; Salanova, R.; Cabanne, A.; Eleta, M.; Gonzalez, J.V.; et al. A clinical and molecular portrait of non-metastatic anal squamous cell carcinoma. Transl. Oncol. 2021, 14, 101084. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, S.A.; Malley, R.; Wang, H.; Lenz, H.-J.; Arguello, D.; El-Deiry, W.S.; Xiu, J.; Gatalica, Z.; Philip, P.A.; Shields, A.F.; et al. Molecular characterization of squamous cell carcinoma of the anal canal. J. Gastrointest. Oncol. 2021, 12, 2423–2437. Available online: https://jgo.amegroups.com/article/view/56717 (accessed on 6 October 2022). [CrossRef] [PubMed]
- Eklund, C.; Forslund, O.; Wallin, K.L.; Dillner, J. Continuing global improvement in human papillomavirus DNA genotyping services: The 2013 and 2014 HPV LabNet international proficiency studies. J. Clin. Virol. Off. Publ. Pan. Am. Soc. Clin. Virol. 2018, 101, 74–85. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, M.; Dondog, B.; Waterboer, T.; Pawlita, M. Homogeneous amplification of genital human alpha papillomaviruses by PCR using novel broad-spectrum GP5+ and GP6+ primers. J. Clin. Microbiol. 2008, 46, 1050–1059. [Google Scholar] [CrossRef]
- FactoMineR: Exploratory Multivariate Data Analysis with R. Available online: http://factominer.free.fr/ (accessed on 6 October 2022).
- Hosni, A.; Han, K.; Le, L.W.; Ringash, J.; Brierley, J.; Wong, R.; Dinniwell, R.; Brade, A.; Dawson, L.A.; Cummings, B.J.; et al. The ongoing challenge of large anal cancers: Prospective long term outcomes of intensity-modulated radiation therapy with concurrent chemotherapy. Oncotarget 2018, 9, 20439–20450. [Google Scholar] [CrossRef] [PubMed]
- Balermpas, P.; Martin, D.; Wieland, U.; Rave-Fränk, M.; Strebhardt, K.; Rödel, C.; Fokas, E.; Rödel, F. Human papilloma virus load and PD-1/PD-L1, CD8+ and FOXP3 in anal cancer patients treated with chemoradiotherapy: Rationale for immunotherapy. Oncoimmunology 2017, 6, e1288331. [Google Scholar] [CrossRef]
- Grimminger, P.P.; Danenberg, P.; Dellas, K.; Arnold, D.; Rödel, C.; Machiels, J.-P.; Haustermans, K.; Debucquoy, A.; Velenik, V.; Sempoux, C.; et al. Biomarkers for Cetuximab-Based Neoadjuvant Radiochemotherapy in Locally Advanced Rectal Cancer. Clin. Cancer Res. 2011, 17, 3469–3477. [Google Scholar] [CrossRef]
- Schernberg, A.; Huguet, F.; Moureau-Zabotto, L.; Chargari, C.; Del Campo, E.R.; Schlienger, M.; Escande, A.; Touboul, E.; Deutsch, E. External validation of leukocytosis and neutrophilia as a prognostic marker in anal carcinoma treated with definitive chemoradiation. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2017, 124, 110–117. [Google Scholar] [CrossRef]
- Shakir, R.; Adams, R.; Cooper, R.; Downing, A.; Geh, I.; Gilbert, D.; Jacobs, C.; Jones, C.; Lorimer, C.; Namelo, W.C.; et al. Patterns and Predictors of Relapse Following Radical Chemoradiation Therapy Delivered Using Intensity Modulated Radiation Therapy with a Simultaneous Integrated Boost in Anal Squamous Cell Carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 2020, 106, 329–339. [Google Scholar] [CrossRef]
- Glynne-Jones, R.; Sebag-Montefiore, D.; Adams, R.; Gollins, S.; Harrison, M.; Meadows, H.M.; for the United Kingdom Coordinating Committee on Cancer Research Anal Cancer Trial Working Party. Prognostic factors for recurrence and survival in anal cancer: Generating hypotheses from the mature outcomes of the first United Kingdom Coordinating Committee on Cancer Research Anal Cancer Trial (ACT I). Cancer 2013, 119, 748–755. [Google Scholar] [CrossRef]
- Available online: https://seer.cancer.gov/statisticsnetwork/explorer/application.html?site=34&data_type=1&graph_type=10&compareBy=age_range&chk_age_range_1=1&chk_age_range_9=9&chk_age_range_141=141&chk_age_range_157=157&series=9&sex=1&race=1&stage=101&advopt_precision=1&advopt_show_ci=on&hdn_view=0#graphArea (accessed on 6 October 2022).
- Wei, F.; Gaisa, M.M.; D’Souza, G.; Xia, N.; Giuliano, A.R.; Hawes, S.E.; Gao, L.; Cheng, S.-H.; Donà, M.G.; Goldstone, S.E.; et al. Epidemiology of anal human papillomavirus infection and high-grade squamous intraepithelial lesions in 29 900 men according to HIV status, sexuality, and age: A collaborative pooled analysis of 64 studies. Lancet HIV 2021, 8, e531–e543. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.-S.; Lee, J.-H.; Choo, J.-Y.; Byun, H.-J.; Jun, J.-H.; Lee, J.-Y. Immunohistochemistry and Polymerase Chain Reaction for Detection Human Papilloma Virus in Warts: A Comparative Study. Ann. Dermatol. 2016, 28, 479–485. [Google Scholar] [CrossRef]
- Parwaiz, I.; MacCabe, T.A.; Thomas, M.G.; Messenger, D.E. A Systematic Review and Meta-Analysis of Prognostic Biomarkers in Anal Squamous Cell Carcinoma Treated with Primary Chemoradiotherapy. Clin. Oncol. R. Coll. Radiol. 2019, 31, e1–e13. [Google Scholar] [CrossRef]
- Moniz, C.M.V.; Riechelmann, R.P.; Oliveira, S.C.R.; Bariani, G.M.; Rivelli, T.G.; Ortega, C.; Pereira, A.A.L.; Meireles, S.I.; Franco, R.; Chen, A.; et al. A Prospective Cohort Study of Biomarkers in Squamous Cell Carcinoma of the Anal Canal (SCCAC) and their Influence on Treatment Outcomes. J. Cancer 2021, 12, 7018–7025. [Google Scholar] [CrossRef]
- Fraunholz, I.; Rabeneck, D.; Gerstein, J.; Jäck, K.; Haberl, A.; Weiss, C.; Rödel, C. Concurrent chemoradiotherapy with 5-fluorouracil and mitomycin C for anal carcinoma: Are there differences between HIV-positive and HIV-negative patients in the era of highly active antiretroviral therapy? Radiother Oncol. 2011, 98, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Martin, D.; Balermpas, P.; Fokas, E.; Rödel, C.; Yildirim, M. Are there HIV-specific Differences for Anal Cancer Patients Treated with Standard Chemoradiotherapy in the Era of Combined Antiretroviral Therapy? Clin. Oncol. 2017, 29, 248–255. [Google Scholar] [CrossRef] [PubMed]
- Susko, M.; Wang, C.-C.J.; Lazar, A.A.; Kim, S.; Laffan, A.; Feng, M.; Ko, A.; Venook, A.P.; Atreya, C.E.; Van Loon, K.; et al. Factors Impacting Differential Outcomes in the Definitive Radiation Treatment of Anal Cancer Between HIV-Positive and HIV-Negative Patients. Oncologist 2020, 25, 772–779. [Google Scholar] [CrossRef]
- Grew, D.; Bitterman, D.; Leichman, C.G.; Leichman, L.; Sanfilippo, N.; Moore, H.G.; Du, K. HIV Infection Is Associated with Poor Outcomes for Patients With Anal Cancer in the Highly Active Antiretroviral Therapy Era. Dis. Colon Rectum 2015, 58, 1130–1136. [Google Scholar] [CrossRef] [PubMed]
- Wieghard, N.; Hart, K.D.; Kelley, K.; Lu, K.C.; Herzig, D.O.; Mitin, T.; Thomas, C.R.; Tsikitis, V.L. HIV positivity and anal cancer outcomes: A single-center experience. Am. J. Surg. 2016, 211, 886–893. [Google Scholar] [CrossRef]
- Camandaroba, M.P.G.; Iseas, S.; Oliveira, C.; Taboada, R.G.; Xerfan, M.P.; Mauro, C.C.; Silva, V.S.; Barros, M.; de Jesus, V.H.F.; Felismino, T.; et al. Disease-Free Survival and Time to Complete Response After Definitive Chemoradiotherapy for Squamous-Cell Carcinoma of the Anus According to HIV Infection. Clin. Color. Cancer 2020, 19, e129–e136. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Total n = 176 (%) | HPSJ n = 97 (%) | HBU n = 79 (%) | p-Value |
|---|---|---|---|---|
| Sex | 0.137 | |||
| Female | 119 (68) | 61 (63) | 58 (73) | |
| Male | 57 (32) | 36 (37) | 21 (27) | |
| Median age at diagnosis (range) in years | 61 (26–89) | 62 (46–89) | 59 (26–87) | 0.013 |
| Location | 0.006 | |||
| Anal margin | 30 (17) | 6 (6) | 24 (30) | |
| Anal canal | 133 (76) | 78 (81) | 55 (70) | |
| Overlapping | 13 (7) | 13 (13) | 0 (0) | |
| Extent of disease | 0.499 | |||
| cT1-T2-N0 | 43 (24) | 20 (21) | 23 (29) | |
| cT3-T4-N0 | 38 (22) | 14 (14) | 25 (30) | |
| TxcN+ | 95 (54) | 63 (65) | 32 (41) | |
| Differentiation | 0.109 | |||
| Well | 29 (16) | 10 (10) | 19 (24) | |
| Medium | 86 (49) | 44 (45) | 42 (53) | |
| Poorly | 40 (23) | 24 (25) | 16 (20) | |
| Unknown | 21 (12) | 19 (20) | 2 (3) | |
| HPV | 0.006 | |||
| Positive | 164 (93) | 95 (98) | 69 (87) | |
| Negative | 12 (7) | 2 (2) | 10 (13) | |
| HIV | 0.028 | |||
| Positive | 38 (22) | 27 (28) | 11 (14) | |
| Negative | 138 (78) | 70 (72) | 68 (86) | |
| CRT treatment response | 0.689 | |||
| Complete | 123 (70) | 69 (71) | 54 (68) | |
| Non-complete | 53 (30) | 28 (29) | 25 (32) | |
| Disease progression at follow-up | 0.86 | |||
| Local | 37 (72) | 21 (70) | 16 (76) | |
| Distant | 9 (18) | 6 (20) | 3 (14) | |
| Both | 5 (10) | 3 (10) | 2 (10) |
| Characteristic | Total n = 175 (%) | Non-Disease Progression n = 124 (%) | Disease Progression n = 51 (%) | p-Value |
|---|---|---|---|---|
| Sex | 0.229 | |||
| Female | 118 (67) | 87 (70) | 31 (61) | |
| Male | 57 (33) | 37 (30) | 20 (39) | |
| Tumor | 0.0002 | |||
| T1-T2 | 76 (43) | 59 (48) | 11 (22) | |
| T3-T4 | 99 (57) | 65 (52) | 40 (78) | |
| Nodes | 0.035 | |||
| Negative | 80 (46) | 63 (51) | 17 (33) | |
| Positive | 95 (54) | 61 (49) | 34 (67) | |
| Differentiation | 0.037 | |||
| Well | 28 (16) | 22 (18) | 6 (12) | |
| Moderate | 86 (49) | 65 (52) | 21 (41) | |
| Poorly | 40 (23) | 22 (18) | 18 (35) | |
| Unknown | 21 (12) | 15 (12) | 6 (12) | |
| HPV | 0.586 | |||
| Positive | 164 (94) | 117 (94) | 47 (92) | |
| Negative | 11 (6) | 7 (6) | 4 (8) | |
| HIV | 0.047 | |||
| Negative | 137 (78) | 102 (82) | 35 (69) | |
| Positive | 38 (22) | 22 (18) | 16 (31) | |
| HIV-HPV infection | 0.018 * | |||
| HIV- and HPV- | 9 (5) | 5 (4) | 4 (8) | |
| * HIV- and HPV+ | 128 (73) | 97 (78) | 31 (61) | |
| HIV+ and HPV- | 2 (1) | 2 (2) | 0 | |
| * HIV+ and HPV+ | 36 (21) | 20 (16) | 16 (31) | |
| CRT treatment regimen | 0.001 | |||
| Standard | 133 (76) | 103 (83) | 30 (59) | |
| Induction + CRT | 42 (24) | 21 (17) | 21 (41) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iseas, S.; Prost, D.; Bouchereau, S.; Golubicki, M.; Robbio, J.; Oviedo, A.; Coraglio, M.; Kujaruk, M.; Méndez, G.; Carballido, M.; et al. Prognostic Factors of Long-Term Outcomes after Primary Chemo-Radiotherapy in Non-Metastatic Anal Squamous Cell Carcinoma: An International Bicentric Cohort. Biomedicines 2023, 11, 791. https://doi.org/10.3390/biomedicines11030791
Iseas S, Prost D, Bouchereau S, Golubicki M, Robbio J, Oviedo A, Coraglio M, Kujaruk M, Méndez G, Carballido M, et al. Prognostic Factors of Long-Term Outcomes after Primary Chemo-Radiotherapy in Non-Metastatic Anal Squamous Cell Carcinoma: An International Bicentric Cohort. Biomedicines. 2023; 11(3):791. https://doi.org/10.3390/biomedicines11030791
Chicago/Turabian StyleIseas, Soledad, Diego Prost, Sarah Bouchereau, Mariano Golubicki, Juan Robbio, Ana Oviedo, Mariana Coraglio, Mirta Kujaruk, Guillermo Méndez, Marcela Carballido, and et al. 2023. "Prognostic Factors of Long-Term Outcomes after Primary Chemo-Radiotherapy in Non-Metastatic Anal Squamous Cell Carcinoma: An International Bicentric Cohort" Biomedicines 11, no. 3: 791. https://doi.org/10.3390/biomedicines11030791
APA StyleIseas, S., Prost, D., Bouchereau, S., Golubicki, M., Robbio, J., Oviedo, A., Coraglio, M., Kujaruk, M., Méndez, G., Carballido, M., Roca, E., Gros, L., De Parades, V., Baba-Hamed, N., Adam, J., Abba, M. C., & Raymond, E. (2023). Prognostic Factors of Long-Term Outcomes after Primary Chemo-Radiotherapy in Non-Metastatic Anal Squamous Cell Carcinoma: An International Bicentric Cohort. Biomedicines, 11(3), 791. https://doi.org/10.3390/biomedicines11030791