Abstract
Background: Sevoflurane is a polyfluorinated compound extensively used as an inhalation anesthetic in patients undergoing surgery. If administered outside the operating room, sevoflurane is dangerous and potentially lethal, and toxicologists may be asked to investigate its presence in biological matrices for forensic purposes. The aim of the present study is to develop and validate a method for the detection and the quantification of sevoflurane in biological fluids and organs through gas chromatography coupled to flame ionization detection (GC–FID). Methods: The method was optimized based on the maximization of the signal-to-noise ratio. The GC–FID instrument was equipped with a Zebron capillary column ZB-624 (30 m, 0.32 mm ID, 1.80 µm film thickness). Results: The method was validated over a concentration range of 1.0–304.0 µg/mL (blood and urine) and µg/g (brain, lungs). The lower limit of quantitation was 1.0 µg/mL or µg/g. Both the intra- and interassay imprecision and inaccuracy were ≤15% at all quality control concentrations in all the matrices. The method was successfully applied to measure the sevoflurane concentrations for 20 negative controls and for a real forensic case. Conclusions: The present method is suitable for the identification and quantification of sevoflurane in fluids and organs and can be a reliable tool in forensic casework.
1. Introduction
Sevoflurane (1,1,1,3,3,3-Hexafluoro-2-(fluoromethoxy)propane, Figure 1) is a polyfluorinated methyl-isopropanol compound. Due to of its inherent stability, low flammability, pleasant odor, lack of airway irritation and low solubility in blood, sevoflurane is extensively used as an inhalation anesthetic in patients undergoing surgery. Moreover, it is the one of most volatile anesthetics with the fastest onset [1,2,3].
Figure 1.
Chemical structure of sevoflurane.
Epidemiological studies show that volatile substances are frequently abused worldwide, especially by children and adolescents, making inhalant abuse a serious public health problem [4]. Unlike other inhalants, particularly mixtures containing toluene [5], the abuse of general anesthetics is rare because they are accessible only to medical personnel [6]. However, the increasing frequency of anesthesia has increased the storage of anesthetics and muscle relaxants, making diversion easier [7,8,9]. Inhalation anesthetics rank among potentially dangerous drugs. The controlled conditions during anesthesia minimize the danger of overdose caused by the anesthetic [10], but inhalation without controlled conditions can be fatal. A few cases of sevoflurane-induced death are reported in the forensic literature [6,11,12], all with suicidal intent, and toxicological analyses have not been performed in all cases [13]. Consequently, there are a few analytical methods developed for the determination of sevoflurane in post-mortem samples, which are limited to the matrices commonly sampled during an autopsy, such as blood and urine [14]. For this reason, the study of the sevoflurane distribution in sevoflurane-induced fatalities is not well documented [6]. Nevertheless, inhalant use is not limited to abuse and suicide. Instead, the use of muscle relaxants and anesthetics with homicidal intentions frequently involves anesthesiologists or other professional figures who know the dosage and effects of these drugs [9].
Analysis for the volatile organic compounds is usually performed using gas chromatography (GC). The headspace (HS) techniques prevent the contamination of the chromatographic system by non-volatile substances from the matrix [15]. The HS procedure is simple and minimizes the number of artifacts, while mass spectrometry (MS), electron capture detection (ECD) and flame ionization detection (FID) are usually used for quantification [4]. The analyses are normally performed on blood, urine and other organs, such as the liver, kidney, adipose tissue, lungs and brain, due to their suitability for determining volatile organic compounds in post-mortem sampling [4].
The HS–GC–FID is undoubtedly one of the most used techniques to determine ethanol and other volatiles with forensic interest. Since an extractive procedure is not necessary, the analysis with this technique is quick and easy to prepare, with enormous advantages to laboratories that routinely perform ethanol determination. However, the retention times of the other volatiles should be known to the laboratory in order avoid interferences.
The aim of the present study is to develop and validate a new method for the determination of sevoflurane in the blood, urine, brain and lungs using HS–GC–FID. The present method was then applied to the negative controls and a real case, where a toxicological analysis was performed for forensic purposes.
2. Materials and Methods
2.1. Chemicals and Reagents
Multiple chemicals and reagents, including 2-butanol, 2-propanol, n-butanol, n-hexane, acetone, dimethyl sulfoxide (DMSO), ethanol, methanol and toluene at the LC-MS grade, were obtained from Sigma Aldrich® (Steinheim, Germany). The sevoflurane was supplied by Merck KGaA (Darmstadt, Germany). The ultra-pure water was obtained from PURELAB® Chorus 1, Elga Veolia.
2.2. Stock Solutions, Standards and Quality Controls
The sevoflurane stock solution was prepared in DMSO at a concentration of 15,200 µg/mL. The appropriate dilutions (at a concentration of 7600 µg/mL; 2500 µg/mL; 1000 µg/mL; 250 µg/mL; 50 µg/mL) with DMSO were made to prepare the calibration curves and QC samples.
All the sevoflurane solutions were stored at room temperature (25 °C). A solution of n-butanol in ultra-pure water was used as an internal standard (IS) at a concentration of 500 µg/mL, stored ad 4 °C. The blank matrices were obtained from autoptic cases were the presence of any volatiles, psychoactive drugs and drugs of abuse were excluded by routine analysis [16,17,18].
The blank matrices (blood, urine, brain and lungs) were spiked with sevoflurane working solutions to obtain a six-point calibration curve (1.0, 5.1, 20.3, 50.7, 152.0, 304.0 µg/mL for blood and urine or µg/g for the brain and lungs). The organ samples (approximately 6 g of brain and lungs) were previously homogenized using an IKA® ULTRA URRAX® Tube Drive.
For the method validation, the QC samples at four concentrations were likewise prepared from the blank matrices (lower limit of the quantification-LLOQ 1.0, low 3.0, medium 152.0, high 304.0 μg/mL or µg/g). To obtain the independent quality control (QC) samples, the commercial sevoflurane, namely Sevoflurane from Baxter S.p.A., was used.
2.3. Instrumentation and Method Optimization
A Shimadzu GC-2010 gas chromatography system equipped with FID was used for the separation and quantitation of the compounds analyzed. The GC–FID instrument was equipped with a Zebron capillary column ZB-624 (30 m, 0.32 mm ID, 1.80 µm film thickness) purchased from Phenomenex (Torrance, CA, USA). The system was run with helium 5.0 as the carrier gas with a flow rate of 21.5 mL/min. The split mode was used at a split rate of 1:10 (liner 3.5 mm × 5.0 × 95, Restek Superchrom, Milano). The optimization of the sevoflurane determination in all the matrices was performed by evaluating the following parameters: the split ratio (1:10, 1:20, 1:30), injector temperature (100 °C, 150 °C, 200 °C), column flow (1.32 mL/min, 1.52 mL/min), oven temperature (isothermal or with a gradient), detector temperature (100 °C, 150 °C, 200 °C) and runtime.
The choice of the conditions to be adopted was based on maximizing the signal-to-noise ratio, separating the peaks with the other volatiles under investigation—especially ethanol, which is the most frequently encountered volatile in forensic cases—simplifying the analysis and reducing the execution time.
Figure 2 reports four examples of the chromatograms obtained during the method optimization, where the first peak is sevoflurane and the second peak is ethanol.
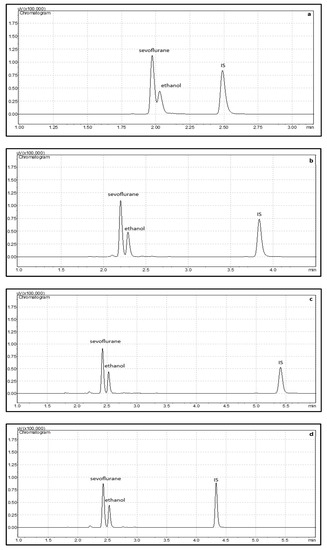
Figure 2.
Chromatograms of sevoflurane, ethanol and IS during optimization: (a) oven T = 150 °C; (b) oven T = 100 °C; (c) oven T = 80 °C; (d) oven T ramp from T = 80 °C to 120 °C at a rate of 40 °C/min to 120 °C. The optimized method is reported in d, where a good separation between the sevoflurane and ethanol peaks was obtained.
Figure 2a represents the injection with the method currently in use in the laboratory for the ethanol analysis: a split ratio of 1:10, injection temperature of 200 °C, column flow of 1.32 mL/min, oven temperature of 150 °C, detector temperature of 200 °C and runtime of 3.5 min. In Figure 2b, the sevoflurane and ethanol peaks show a better separation with the following parameters: a split ratio of 1:10, injection temperature of 150 °C, column flow of 1.46 mL/min, oven temperature of 100 °C, detector temperature of 150 °C and runtime of 4.5 min. Figure 2c shows a further optimization, with a good separation between the sevoflurane and ethanol peaks with the following parameters: a split ratio of 1:10, injection temperature of 150 °C, column flow of 1.52 mL/min, oven temperature of 80 °C, detector temperature of 150 °C and runtime of 6.0 min. A ramp was used to reduce the runtime, as the n-butanol IS showed a retention time of more than 5 min.
The optimized conditions were as follows and resulted in the chromatography shown in Figure 2d. The injector temperature was set at 150 °C and the detector was set at 150 °C. The injection mode was split, with a split ratio of 1:10. The flow rate of the helium carrier gas was 1.52 mL/min. The temperature program started with the oven at 80 °C for 2.5 min. The temperature was then ramped up at a rate of 40 °C/min to 120 °C and held for 2 min.
2.4. Headspace Procedure
A 0.5 mL (blood, urine) or 0.5 g (homogenized brain and lungs for 10 s, in order to reduce the evaporation as much as possible) of sevoflurane-free samples were added with 1 g of NaCl and 0.5 mL of the IS solution were pooled in a 10 mL headspace vial (22.5 × 46 mm). The spiking procedure was performed by adding a 10 µL aliquot of the single working solution directly into the cuvette. The vial was immediately sealed with a rubber stopper and an aluminum crimp seal, shaken for 30 s and kept for 50 min at 40 °C in the heater. A 0.5 mL aliquot of headspace was withdrawn with a gas-tight syringe for analysis and injected onto the GC–FID.
2.5. Validation Plan
The validation was planned according to the Guidelines of the Scientific Working Group for Forensic Toxicology (SWGTOX) [19].
2.5.1. Interferences Studies
Ten blank sources of each matrix (n = 40 samples) were extracted without the IS and analyzed to test the co-elution of the endogenous substances. Two randomly selected samples for each matrix (n = 8) were added with the exogenous volatiles, namely sevoflurane, acetone, isobutanol, hexane, ethanol, methanol, toluene and formaldehyde, to test whether the volatiles commonly searched for forensic purposes interfere with the retention times of the molecules tested.
2.5.2. Linearity and Carryover
It was decided that the calibration model should be linear, in the same calibration range for all the matrices (1.0–5.1–20.3–50.7–152.0–304.0 µg/mL for blood and urine and µg/g for the brain and lungs). The calibration range was defined according to the concentrations detected in the post-mortem samples of the available studies [14]. The linearity was assessed by a simple linear regression, accepting a correlation coefficient (r2) ≥ 0.990 and by a residue plot analysis. Two extracted blank matrices were analyzed after the highest calibrator to evaluate the carryover. The carryover was considered negligible if the signal in the blank was lower than 10% of the method’s LLOQ.
2.5.3. Limit of Detection and Limit of Quantification
The LLOQ was identified as the lowest non-zero calibrator that meets a signal-to-noise ratio of at least 10 and can reproducibly replicate within a 20% bias and 20% CV% in three samples per run over three runs. To assess the LOD, another spiked calibrator was obtained by diluting (1:3; v/v) the LLOQ. Three separated samples were analyzed in duplicate for at least three runs. The LOD was identified as the lowest point that (1) yields a reproducible instrument response greater than or equal to three times the noise level of the background signal from the negative samples and (2) achieves an acceptable retention time and peak shape.
2.5.4. Precision and Accuracy
The precision was evaluated by determining the relative standard deviation (RSD) at the four sevoflurane concentrations of the QCs corresponding to the LLOQ (1.0 μg/mL) and the low (3.0 μg/mL), medium (152.0 μg/mL) and high concentrations (304.0 μg/mL) (µg/g for long and brain) within the same analysis (n = 6, intraday precision) and in triplicate over a series of five analyses (n = 15, interday precision). Each QC was prepared according to the procedure described for the calibrator preparation, using commercial sevoflurane (Baxter) as the standard in order to obtain the independent controls. The accuracy (bias) of the method was determined by comparing the means of the calculated concentrations of the QCs with the nominal concentrations. The intraday accuracy (n = 6) and interday accuracy (n = 15, in triplicate over a series of five analysis) were calculated. The acceptance criteria for the intra- and interday precision and accuracy were ±15% for the low, medium and high QCs and ±20% for the LLOQ.
2.5.5. Stability Studies
The short-term stability was evaluated by reanalyzing the QC blood samples (low and high) in triplicate after 4 h in the heather after extraction. To assess the long-term stability, the QCs were prepared and stored at −20 °C and analyzed 30 days later. The processed QCs were considered stable if their mean concentrations were within ±15% of the nominal concentration for the low and high QCs.
2.5.6. Method Application
The validated method was applied on the blood taken during anesthesia in a driver who underwent surgery after a car crash. Analysis was requested by a judicial authority for the assessment of driving under the influence of alcohol and drugs. The method was also applied to the blood, urine, brain and lungs of 20 cases of traumatic deaths where circumstantial, autoptic and toxicological data excluded sevoflurane exposure as the negative controls. As recommended in forensic cases to confirm the presence of sevoflurane, a GC–MS analysis was performed on the real sample. For a qualitative analysis, a Shimadzu GC-2010 Plus coupled with a GC–MS–QP 2010 Ultra autosampler AOC 6000 (Shimadzu, Milano) was used. The system was equipped with a RXi-5sil MSN 13 capillary column (30 m × 0.25 mm id, 0.25 µm film thickness). The GC–MS conditions included an injection temperature of 200 °C, column flow of 0.94 mL/min, ion source temperature of 220 °C and interface temperature of 200 °C. The split mode was used at a split rate of 1:30. The flow rate of the helium 6.0 carrier gas was 32.2 mL/min. The temperature gradient of the GC oven started at 40 °C for 4 min, then increased to 200 °C at a rate of 60 °C/min and was held at 200 °C for 15 min. An electron impact (EI) ionization mode was used. The ions of m/z 131, 69 and 181 were selected for identification.
3. Results
3.1. Interferences Studies
The method showed no interference from the endogenous substances, the other exogenous substances tested co-eluting within the time frame of the method, or between the analyte and the internal standard. The retention times of sevoflurane and the volatiles tested were (min,s) methanol 2.27; sevoflurane 2.43; ethanol 2.53; acetone 2.77; hexane 3.19; isobutanol 3.90 and n-butanol 4.34 (IS). The retention times of toluene and formaldehyde were out of the runtime. The peak of sevoflurane was well distinguishable from the other volatiles’ peaks (Figure 3).
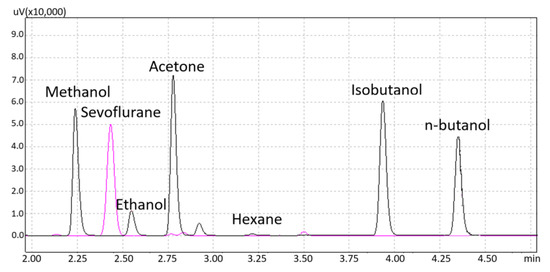
Figure 3.
Chromatograms of sevoflurane and the other volatiles tested.
3.2. Linearity and Carryover
The calibration curve appeared to provide a better fit of the data using an unweighted linear model, passing through the zero, as confirmed by the residual plot, which showed a random distribution around the zero line. The mean equations of the resulting curves are reported in Table 1. The calibration curve obtained in the blood matrix is reported in Figure 4.

Table 1.
Equations and correlation coefficients (r2) for all the matrices tested are reported. Mean and standard deviation (SD) are calculated over five calibration curves.
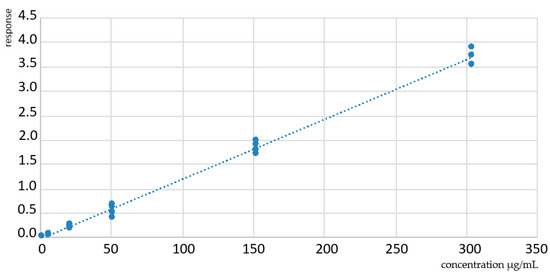
Figure 4.
Calibration curve obtained in the blood shows a good linearity in the calibration range (1.0–304.0 μg/mL). The equation and correlation coefficients are reported in Table 1. X axis: concentration in µg/mL. Y-axis: response.
The carryover was not present for all the drugs or the internal standard in any of the extracted blank matrices that followed the highest calibrator and were deemed acceptable.
3.3. Limit of Detection and Limit of Quantification
The LLOQ was set at 1.0 µg/mL for blood and urine or µg/g for the brain and lungs within and between the run precision and the biases are shown in Table 2. The LOD respected all the pre-defined criteria and was set at 0.3 µg/mL or µg/g (1/3 of the LLOQ) in all the matrices.
Table 2.
Precision and accuracy of the sevoflurane assay.
3.4. Precision and Accuracy
The results of the precision and accuracy are reported in Table 2. Both the intra- and interassay imprecision and inaccuracy were ≤20% for the whole concentrations range. The representative chromatograms of a QC sample for all the matrices are reported in Figure 5a–d.
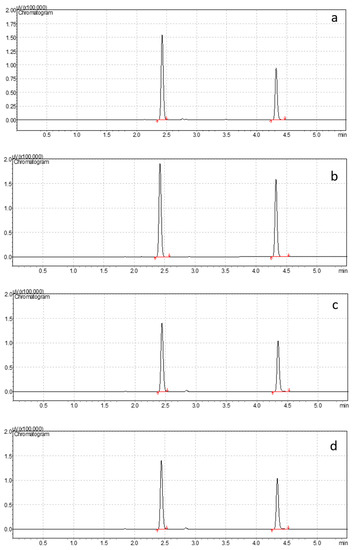
Figure 5.
Chromatograms of the medium QC in the blood (a), urine (b), brain (c), lung (d). Retention times: sevoflurane 2.43; IS 4.34.
3.5. Stability Studies
The short-term stability in all matrices showed mean sevoflurane calculated concentration within 10% of the nominal concentrations for both QC levels. Similarly, sevoflurane in the processed QCs was stable after 30 days at −20 °C, with an mean concentration in the matrix of the analyte at less than 10% of nominal concentrations.
3.6. Method Application
Analysis performed on the controls (n = 20) was negative on all the matrices tested (<LLOQ). The method was applied to measure the blood concentrations of a real forensic case, which tested negative for alcohol, drugs and other psychoactive substances. As the patient underwent anesthesia after the trauma, the toxicological analysis detected the presence of sevoflurane at a concentration of 23.3 µg/mL, a value within the concentration ranges found in patients undergoing surgical anesthesia with sevoflurane [14]. The chromatogram of the real case obtained by HS–GC–FID is reported in Figure 6a. The full scan mass spectrum of sevoflurane obtained by GC–MS to be interpreted as a qualitative confirmation is reported in Figure 6b.
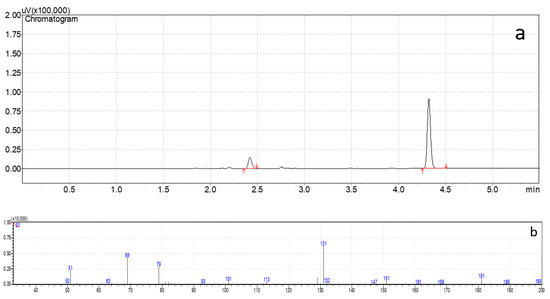
Figure 6.
Chromatogram of the real case (a) obtained with the validated method in GC–FID (b). Mass spectrum of sevoflurane. The ions of m/z 131, 69 and 181 were selected.
4. Discussion
The analytical methods to detect the volatile substance in post-mortem samples, such as peripheral or central blood, kidney, brain, liver and urine, have long been studied in forensic literature [4]. Analyses of the samples can be based on direct detection of the compound itself in the blood or tissue, but, for some volatiles, also through the detection of metabolites [20]. Blood is the most used matrix, but due to their lipophilic nature, volatile compounds can be easily detected in other organs such as brain tissue. In fact, due to its high fat content, the brain is a reliable source of sampling, and it is more resistant to post-mortem decomposition [21]. Lungs tissue is also frequently sampled and analyzed during autopsy procedures [22,23], and a previous study demonstrated that volatile compounds can be retained in many tissues, including the lungs, and could be more informative in cases with a burned body [24].
An overview of the most cited papers that report the detection and quantification of sevoflurane, alone or with other volatiles, in the biological matrices is shown in Table 3. The table also shows the methods applied in the three cases reported in the forensic literature, all reporting sevoflurane-induced suicidal deaths [6,11,12].
Table 3.
An overview of the published methods for the detection of sevoflurane in biological samples.
The table shows that most of the developed methods, including those applied in the case reports, were based on the direct detection of sevoflurane. In fact, only 5% of sevoflurane is metabolized into hexafluroisopropanol (HFIP) by the hepatic cytochrome isoenzyme family. HFIP is conjugated and eliminated in the urine. No other metabolic pathway has been identified. Moreover, the volatile metabolites analysis was important both in occupational and environmental exposure and in the monitoring of abuse [29,30]. In post-mortem cases, the metabolites in urine seemed less relevant, as the detection of the volatile that exerts the toxicity in blood or tissues can provide a direct toxicological link between exposure and death or the state of acute intoxication. Therefore, the direct identification of sevoflurane has been recognized as the preferred method to assess the presence of the volatile compound. Many other methods have been validated on exhaled air, and they cannot be obviously applied in a post-mortem setting [31,32]. The analysis of sevoflurane in urine is commonly used for the biomonitoring of exposed workers for clinical purposes on living subjects [33,34].
The literature review demonstrated that, in forensic cases, organ analysis provides insight into the post-mortem distribution of sevoflurane to better understand the cause of death. To date, most published methods for the detection and quantification of sevoflurane and other volatile compounds have been validated on blood samples [25,26,27,28] and rarely on urine or plasma samples [14]. Plasma is not a valid matrix for post-mortem samples since post-mortem blood is characterized by a variable degree of hemolysis, which prevents the separation of the serum or plasma [35]. In addition, blood and urine cannot always be taken during an autopsy, as in the case of burned bodies or after a long PMI, and organ analysis is the only method available in some cases. Analysis of the other organs may be useful to study the distribution of the compounds in the organs, to reduce the hypothesis of external contamination and to confirm the results obtained in the other matrices. The comparison with the pre-existing methods also shows that, to the best of our knowledge, this is the first validated method for the detection and quantification of sevoflurane on brain and lungs tissue. Moreover, the low sample volume (0.5 mL of blood and urine and 0.5 g for brain and lungs) allows for the repeatability of the analysis, which is a major issue in case of analyses performed for forensic purposes. The present method also respects the minimum standards of practice for validating the analytical methods in forensic toxicology, which are not always respected for the methods designed for clinical application or for the method published in the past. The validation of a method is fundamental in forensics to determine if a method is suitable to be used in court, as stated by the Daubert criteria for the admissibility of an expert testimony in a trial [36].
Regarding the technique of the analysis chosen, gas-chromatography coupled with flamed ionizing detection (GC–FID) is a well-established method for the detection and quantification of volatiles for forensic purposes. In fact, the “Guidelines for the Forensic analysis of drugs facilitating sexual assault and other criminal acts” of the United Nations Office on Drugs and Crime (UNODC) [37] reports that the analysis for volatile substances can be achieved by HS–GC with either FID or with MS detection. According the UNODC guidelines, the identification and confirmation of the volatiles present in the samples is considered positive when the gas chromatogram reveals the presence of a signal whose retention time is identical to the positive control analyzed simultaneously under the same conditions. For this reason, the anesthetics not tested during the method interference studies may hinder the ethanol analysis and vice versa. In forensic cases, a qualitative confirmation by GC–MS is recommended.
The method presented was suitable for the identification and quantification of sevoflurane in the fluids and organs inasmuch as the LOD and LLOQ of the method, as well as the calibration range, encompass the concentrations described in the three cases of sevoflurane-induced death reported in the literature. When toxicological investigations require lower LOQ, the HS procedure could be optimized, for example, by increasing the sample volume, the injection volume, or the temperature of the heater. In 2004, Burrows et al. [6] were the first to report a death caused by sevoflurane inhalation involving a 44-year-old anesthetist lying in a bed with an oxygen mask secured to his face, with numerous bottles of sevoflurane found near the body. The toxicological analysis detected sevoflurane concentrations of 26.2 μg/mL in the blood, 105 μg/mL in the urine, 31.9 μg/mL in the tracheal aspirate, 86.7 μg/mL in the vitreous humor, 30.8 μg/g in the liver and 12.8 μg/g in the kidney. The remaining two cases were described in 2007. Lavine et al. [12] reported the death of a 47-year-old nurse found lying in a bed with a container of sevoflurane found in proximity to the body. The sevoflurane concentrations were 16 μg/mL and 8.0 μg/mL in the central and peripheral blood, 9.9 μg/mL in the bile, 29 μg/g in the kidney, 269 μg/g in the liver and 1.1 μg/mL in the urine. Rosales et al. [11] reported the death of a 31-year-old anesthetist found dead in the surgery area, holding an uncapped empty bottle of sevoflurane. The sevoflurane concentrations were 15 μg/mL in the blood and 130 μg/g in the brain and lungs.
In two of the presented cases, sevoflurane analysis was carried out using GC–FID [6,11]. In one case [12], the analysis was performed using GC–MS. The authors report that the MS acquisition was run in SIM mode, measuring 131, 69 and 181 mass ions for sevoflurane and 117 and 198 mass ions for the internal standard (halothane). In all these reports, apart from the blood and urine, concentrations of tissue samples were reported. However, the validation plans, especially for the organs, were not extensively reported, thus not allowing the repeatability of the analytical technique.
All the cases reported involved healthcare professionals and that sevoflurane, identified as the sole cause of death, was found in the range 16–26.2 μg/mL in the blood and at higher values in the organs. However, a “threshold” cannot be defined as the data are currently very scarce to define a distribution pattern in the fluids and organs in sevoflurane-induced fatalities. Moreover, other circumstances, such as the time and post-mortem redistribution of the volatile agents, are not always available in forensic casework. More data are needed in order to define the distribution pattern of sevoflurane in fatalities.
The main limit of the present method is that, since it is based on FID, the identification of the compound only relies on the exact retention time of the sevoflurane compared to a known standard and on the absence of interreferences with the other tested volatiles, those mainly encountered in forensic casework, including ethanol. In the absence of clinical, circumstantial or forensic data that can be used to support the hypothesis of sevoflurane intoxication, the present method should be supplemented with an MS-based technique, the technique of choice for qualitative analysis in forensics that allows the library to be used as a reference [38]. In fact, mass spectrometry is widely used in forensics because of its enormous advantages, namely the high sensitivity and precision of the qualitative and quantitative analysis and the small amount of the sample required. As an instrumental analytical technique, MS is more reliable for identification and quantification purposes, allowing the determination of the mass-to-charge ratio (m/z) of the charged and fragmented molecules in the gas phase [39]. Therefore, in the real casework of suspected sevoflurane intoxication, this method could be used to rule out or confirm sevoflurane exposure and to evaluate the resulting concentrations in order to establish the cause of death through multidisciplinary forensic analysis. In the case of isolated findings with no suspicious history, the positive result could be supplemented with a qualitative GC–MS analysis or, if possible, the identification/quantification of the major metabolite.
Recent forensic literature highlights that the crimes related to the use of inhalants and/or anesthetics should not be underestimated. The present method could be profitably applied in forensic casework and aid investigators to better understand the diffusion of sevoflurane for non-medical use. Future research will focus on the extensive application of this method to test its sensitivity and selectivity on a larger number of cases and to verify the interfaces with the other types of volatiles.
5. Conclusions
Apart from clinical and occupational monitoring, toxicologists may be asked to investigate the presence of fluorinated anesthetics in biological matrices, also for forensic purposes. The availability of a validated method on organs could prove useful in case of an absence of “classic” biological matrices, such as blood and urine, as often occurs when sampling is performed after longer post-mortem intervals. The proposed method, validated following forensic guidelines and characterized by excellent linearity, precision, accuracy and limit of detection/quantification, will find its application in the deaths that occur during anesthesia, deaths from anesthetic abuse and other inhalant-induced deaths.
Author Contributions
Conceptualization, G.P.; methodology, R.B. and S.M.; software, M.G.; validation, R.B.; formal analysis, F.R.; data curation, P.F.; writing—original draft preparation, G.P. and S.M.; writing—review and editing, A.G.; supervision, S.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Our investigations were carried out following the rules of the Declaration of Helsinki of 1975, revised in 2013. According to Italian legislation, ethical approval for a single case is not required, as long as the data are kept anonymous, and the investigations performed do not imply genetic results.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to privacy concerns.
Conflicts of Interest
The authors declare no conflict of interest.
References
- O’Keeffe, N.J.; Healy, T.E. The role of new anesthetic agents. Pharm. Ther. 1999, 84, 233–248. [Google Scholar] [CrossRef]
- Behne, M.; Wilke, H.J.; Harder, S. Clinical pharmacokinetics of sevoflurane. Clin. Pharmacokinet. 1999, 36, 13–26. [Google Scholar] [CrossRef]
- Delgado-Herrera, L.; Ostroff, R.D.; Rogers, S.A. Sevoflurance: Approaching the ideal inhalational anesthetic. a pharmacologic, pharmacoeconomic, and clinical review. CNS Drug Rev. 2001, 7, 48–120. [Google Scholar] [CrossRef]
- Wille, S.M.; Lambert, W.E. Volatile substance abuse--post-mortem diagnosis. Forensic Sci. Int. 2004, 142, 135–156. [Google Scholar] [CrossRef] [PubMed]
- Pelletti, G.; Rossi, F.; Garagnani, M.; Barone, R.; Roffi, R.; Pelotti, S. Medico-legal implications of toluene abuse and toxicity. Review of cases along with blood concentrations. Leg Med. 2018, 34, 48–57. [Google Scholar] [CrossRef]
- Burrows, D.L.; Nicolaides, A.; Stephens, G.C.; Ferslew, K.E. The distribution of sevoflurane in a sevoflurane induced death. J. Forensic Sci. 2004, 49, 394–397. [Google Scholar]
- Epstein, R.H.; Gratch, D.M.; Grunwald, Z. Development of a scheduled drug diversion surveillance system based on an analysis of atypical drug transactions. Anesth. Analg. 2007, 105, 1053–1060. [Google Scholar] [CrossRef]
- Hayashi, T.; Buschmann, C.; Riesselmann, B.; Roscher, S.; Tsokos, M. Circumstantial and toxicological features of deaths from self-administered intravenous anesthetic/narcotic agents. Forensic Sci. Med. Pathol. 2013, 9, 138–144. [Google Scholar] [CrossRef]
- Johnstone, R.E.; Katz, R.L.; Stanley, T.H. Homicides using muscle relaxants, opioids, and anesthetic drugs: Anesthesiologist assistance in their investigation and prosecution. Anesthesiology 2011, 114, 713–716. [Google Scholar] [CrossRef]
- Derrington, M.C.; Smith, G. A review of studies of anaesthetic risk, morbidity and mortality. Br. J. Anaesth. 1987, 59, 815–833. [Google Scholar] [CrossRef] [PubMed]
- Rosales, C.M.; Young, T.; Laster, M.J.; Eger, E.I., 2nd; Garg, U. Sevoflurane concentrations in blood, brain, and lung after sevoflurane-induced death. J. Forensic Sci. 2007, 52, 1408–1410. [Google Scholar] [CrossRef]
- Levine, B.; Cox, D.; Jufer-Phipps, R.A.; Li, L.; Jacobs, A.; Fowler, D. A fatality from sevoflurane abuse. J. Anal. Toxicol. 2007, 31, 534–536. [Google Scholar] [CrossRef]
- Cantrell, F.L. A fatal case of sevoflurane abuse. Clin. Toxicol. 2008, 46, 918–919. [Google Scholar] [CrossRef]
- Kovatsi, L.; Giannakis, D.; Arzoglou, V.; Samanidou, V. Development and validation of a direct headspace GC-FID method for the determination of sevoflurane, desflurane and other volatile compounds of forensic interest in biological fluids: Application on clinical and post-mortem samples. J. Sep. Sci. 2011, 34, 1004–1010. [Google Scholar] [CrossRef]
- Pihlainen, K.; Ojanperä, I. Analytical toxicology of fluorinated inhalation anaesthetics. Forensic Sci. Int. 1998, 97, 117–133. [Google Scholar] [CrossRef]
- Pelletti, G.; Rossi, F.; Garagnani, M.; Barone, R.; Roffi, R.; Fais, P.; Pelotti, S. Optimization of cloned enzyme donor immunoassay cut-offs for drugs of abuse in post-mortem whole blood. Forensic Sci. Int. 2020, 312, 110291. [Google Scholar] [CrossRef]
- Giorgetti, A.; Barone, R.; Pelletti, G.; Garagnani, M.; Pascali, J.; Haschimi, B.; Auwärter, V. Development and validation of a rapid LC-MS/MS method for the detection of 182 novel psychoactive substances in whole blood. Drug Test. Anal. 2022, 14, 202–223. [Google Scholar] [CrossRef]
- Pelletti, G.; Verstraete, A.G.; Reyns, T.; Barone, R.; Rossi, F.; Garagnani, M.; Pelotti, S. Prevalence of therapeutic drugs in blood of drivers involved in traffic crashes in the area of Bologna, Italy. Forensic Sci. Int. 2019, 302, 109914. [Google Scholar] [CrossRef]
- Scientific Working Group for Forensic Toxicology. Scientific Working Group for Forensic Toxicology (SWGTOX) standard practices for method validation in forensic toxicology. J. Anal. Toxicol. 2013, 37, 452–474. [Google Scholar] [CrossRef]
- Larry, B. (Ed.) Principles of Forensic Toxicology; American Association for Clinical Chemistry: Washington, DC, USA, 1999; ISBN 1-890883-07-7. [Google Scholar]
- Pelletti, G.; Garagnani, M.; Barone, R.; Boscolo-Berto, R.; Rossi, F.; Morotti, A.; Roffi, R.; Fais, P.; Pelotti, S. Validation and preliminary application of a GC-MS method for the determination of putrescine and cadaverine in the human brain: A promising technique for PMI estimation. Forensic Sci. Int. 2019, 297, 221–227. [Google Scholar] [CrossRef]
- Romolo, F.S.; di Luca, N.M.; Ciallella, C.; Bottoni, E.; Fiore, P.A.; Cappelletti, S.; Giuliani, N.; Augsburger, M.; Varlet, V. Volatile lipophilic substances management in case of fatal sniffing. J. Forensic Leg. Med. 2017, 52, 35–39. [Google Scholar] [CrossRef]
- Soejima, M.; Tanaka, N.; Oshima, T.; Kinoshita, H.; Koda, Y. Detection of helium in a fire victim: A case report. Forensic Sci. Int. 2021, 318, 110613. [Google Scholar] [CrossRef]
- Pahor, K.; Olson, G.; Forbes, S.L. Post-mortem detection of gasoline residues in lung tissue and heart blood of fire victims. Int. J. Leg. Med. 2013, 127, 923–930. [Google Scholar] [CrossRef]
- Saito, K.; Takayasu, T.; Nishigami, J.; Kondo, T.; Ohtsuji, M.; Lin, Z.; Ohshima, T. Determination of the volatile anesthetics halothane, enflurane, isoflurane, and sevoflurane in biological specimens by pulse-heating GC-MS. J. Anal. Toxicol. 1995, 19, 115–119. [Google Scholar] [CrossRef] [PubMed]
- Yang, N.C.; Hwang, K.L.; Shen, C.H.; Wang, H.F.; Ho, W.M. Simultaneous determination of fluorinated inhalation anesthetics in blood by gas chromatography-mass spectrometry combined with a headspace autosampler. J. Chromatogr. B Biomed. Sci. Appl. 2001, 759, 307–318. [Google Scholar] [CrossRef]
- Kojima, T.; Ishii, A.; Watanabe-Suzuki, K.; Kurihara, R.; Seno, H.; Kumazawa, T.; Suzuki, O.; Katsumata, Y. Sensitive determination of four general anaesthetics in human whole blood by capillary gas chromatography with cryogenic oven trapping. J. Chromatogr. B Biomed. Sci. Appl. 2001, 762, 103–108. [Google Scholar] [CrossRef]
- Bourdeaux, D.; Sautou-Miranda, V.; Montagner, A.; Perbet, S.; Constantin, J.M.; Bazin, J.E.; Chopineau, J. Simple assay of plasma sevoflurane and its metabolite hexafluoroisopropanol by headspace GC-MS. J. Chromatogr. B Anal. Technol. Biomed. Life Sci. 2010, 878, 45–50. [Google Scholar] [CrossRef]
- Accorsi, A.; Morrone, B.; Domenichini, I.; Valenti, S.; Raffi, G.B.; Violante, F.S. Urinary sevoflurane and hexafluoro-isopropanol as biomarkers of low-level occupational exposure to sevoflurane. Int. Arch. Occup. Environ. Health. 2005, 78, 369–378. [Google Scholar] [CrossRef]
- Astier, A. Chromatographic determination of volatile solvents and their metabolites in urine for monitoring occupational exposure. J. Chromatogr. 1993, 643, 389–398. [Google Scholar] [CrossRef]
- Ghimenti, S.; Tabucchi, S.; Bellagambi, F.G.; Lomonaco, T.; Onor, M.; Trivella, M.G.; Fuoco, R.; Di Francesco, F. Determination of sevoflurane and isopropyl alcohol in exhaled breath by thermal desorption gas chromatography-mass spectrometry for exposure assessment of hospital staff. J. Pharm. Biomed. Anal. 2015, 106, 218–223. [Google Scholar] [CrossRef]
- Dong, H.; Zhang, F.J.; Wang, F.Y.; Wang, Y.Y.; Guo, J.; Kanhar, G.M.; Chen, J.; Liu, J.; Zhou, C.; Yan, M.; et al. Simultaneous on-line monitoring of propofol and sevoflurane in balanced anesthesia by direct resistive heating gas chromatography. J. Chromatogr. A 2017, 1506, 93–100. [Google Scholar] [CrossRef]
- Accorsi, A.; Barbieri, A.; Raffi, G.B.; Violante, F.S. Biomonitoring of exposure to nitrous oxide, sevoflurane, isoflurane and halothane by automated GC/MS headspace urinalysis. Int. Arch. Occup. Environ. Health. 2001, 74, 541–548. [Google Scholar] [CrossRef]
- Jafari, A.; Bargeshadi, R.; Jafari, F.; Mohebbi, I.; Hajaghazadeh, M. Environmental and biological measurements of isoflurane and sevoflurane in operating room personnel. Int. Arch. Occup. Environ. Health. 2018, 91, 349–359. [Google Scholar] [CrossRef] [PubMed]
- Woydt, L.; Bernhard, M.; Kirsten, H.; Burkhardt, R.; Hammer, N.; Gries, A.; Dreßler, J.; Ondruschka, B. Intra-individual alterations of serum markers routinely used in forensic pathology depending on increasing post-mortem interval. Sci. Rep. 2018, 8, 12811. [Google Scholar] [CrossRef]
- Pelletti, G.; Cecchetto, G.; Viero, A.; Fais, P.; Weber, M.; Miotto, D.; Montisci, M.; Viel, G.; Giraudo, C. Accuracy, precision and inter-rater reliability of micro-CT analysis of false starts on bones. A preliminary validation study. Leg Med. 2017, 29, 38–43. [Google Scholar] [CrossRef]
- United Nations Office on Drugs and Crime (UNDC). Laboratory and Scientific Section United Nations Office on Drugs and Crime. Guidelines for the Forensic Analysis of Drugs Facilitating Sexual Assault and Other Criminal Acts. United Nations. December 2011. Available online: https://www.unodc.org/documents/scientific/forensic_analys_of_drugs_facilitating_sexual_assault_and_other_criminal_acts.pdf (accessed on 24 November 2022).
- Grocholska, P.; Popiel, D.; Walter, M.; Biernat, M.; Cebrat, M.; Kuczer, M.; Modzel, M.; Bachor, R.; Kluczyk, A. Citius, Altius, Fortius—Advanced Mass Spectrometry in Service of Forensic Analysis. Chemosensors 2022, 10, 324. [Google Scholar] [CrossRef]
- Barea-Sepúlveda, M.; Duarte, H.; Aliaño-González, M.J.; Romano, A.; Medronho, B. Total Ion Chromatogram and Total Ion Mass Spectrum as Alternative Tools for Detection and Discrimination (A Review). Chemosensors 2022, 10, 465. [Google Scholar] [CrossRef]






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).