
Systematic Literature Review of Capitation and Fee-for-Service Payment Models for Oral Health Services: An Australian Perspective

 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy and Eligibility Criteria
2.2. Data Extraction
2.3. Quality Assessment
3. Results
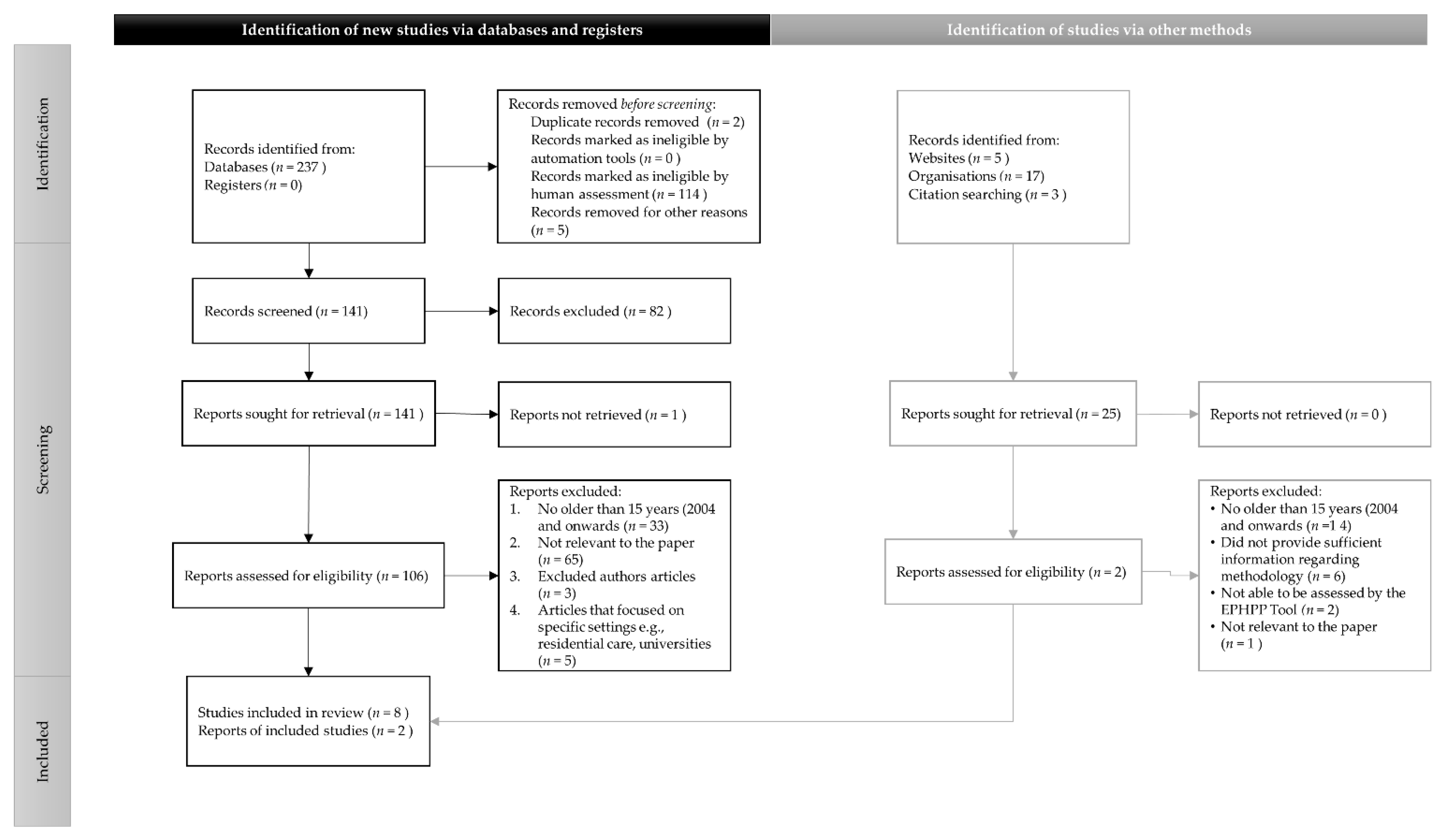
3.1. Reference Selection
3.2. Study Design
3.3. Quality Assessment
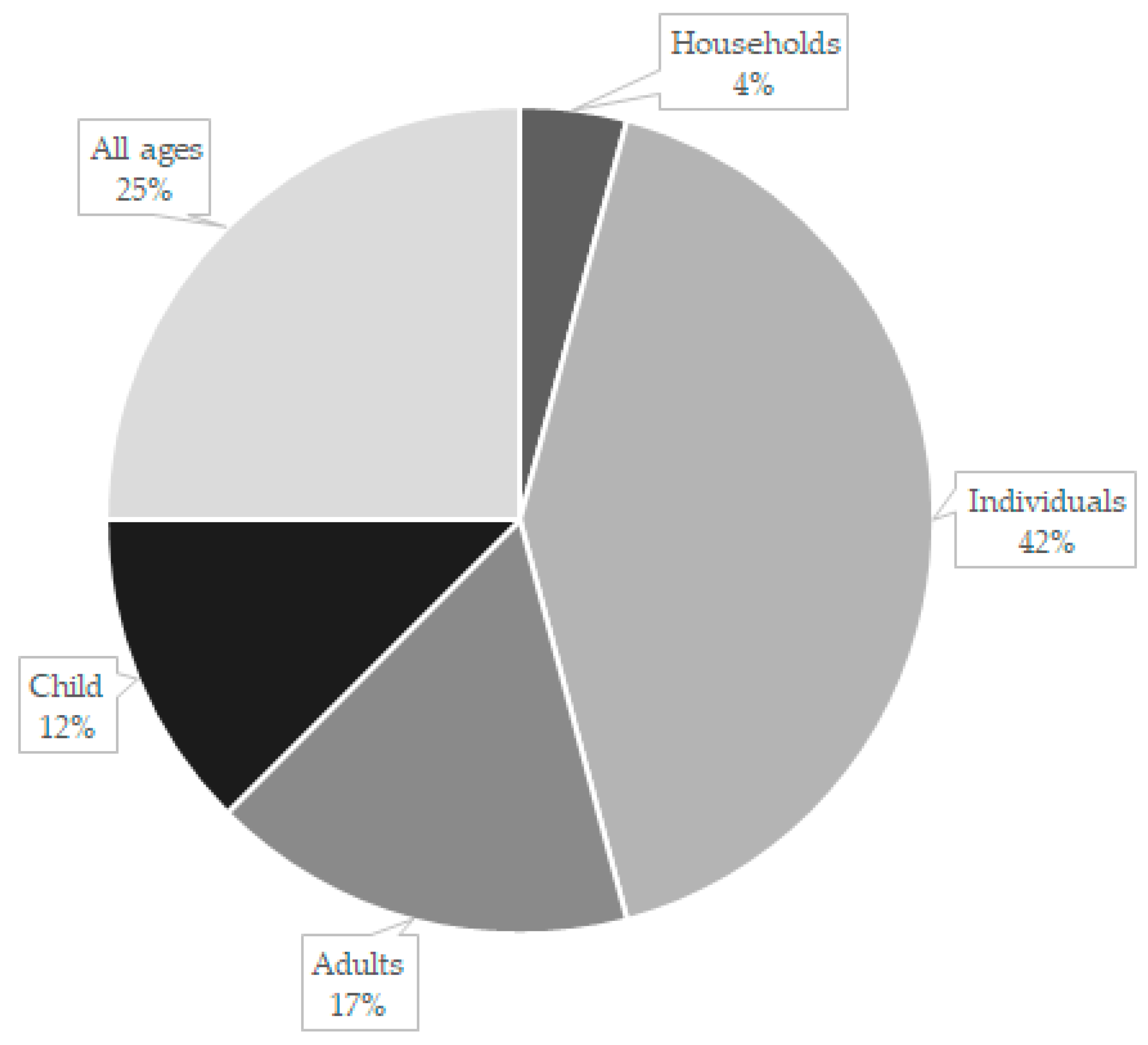
3.4. Study Population
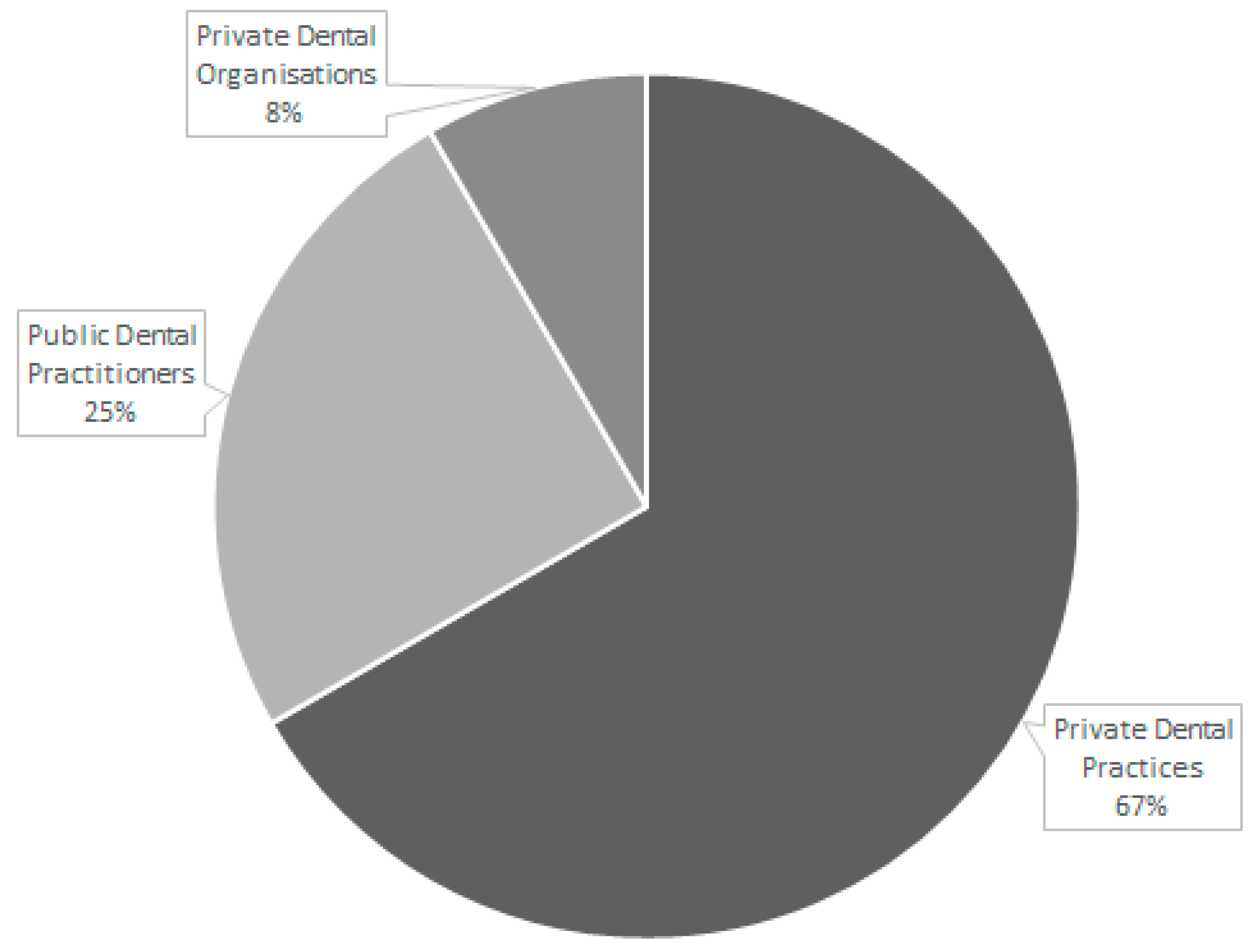
3.5. Dental Provider
3.6. Interventions
3.7. Outcomes
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Park, M.; Braun, T.; Carrin, G.; Evans, D.B. Technical Briefs for Policy Makers No 2: Provider Payments and Cost-Containment Lessons from OECD Countries; World Health Organisation: Geneva, Switzerland, 2007; Available online: https://apps.who.int/iris/handle/10665/340521 (accessed on 3 February 2021).
- Jessep, A. Health Cost Containment and Medical Innovation; U.S. Department of Health and Human Services: Washington, DC, USA, 2012. Available online: https://aspe.hhs.gov/basic-report/health-care-cost-containment-and-medical-innovation (accessed on 16 February 2021).
- Mooney, G.; Newberry, G. Priority setting in dentistry: Putting teeth into the process. NSW Public Health Bull. 1999, 10, 42–43. Available online: https://www.phrp.com.au/wp-content/uploads/2014/10/NB99019.pdf (accessed on 31 January 2021). [CrossRef]
- World Health Organisation. Decisions and Resolutions: Prevention and Control of Noncommunicable Diseases; Fifty-Third World Health Assembly: Geneva, Switzerland, 2000; Available online: https://apps.who.int/gb/ebwha/pdf_files/WHA53-REC1/WHA53-2000-REC1-eng.pdf (accessed on 12 January 2021).
- Blinkhorn, A.S.; Hassell, D.C.; Holloway, P.J.; Mellor, A.C.; Worthington, H.V. An Assessment of capitation in the new general dental service contract. Community Dent. Health 1996, 13, 3–20. Available online: https://europepmc.org/article/MED/8689497 (accessed on 16 February 2021).
- Kassebaum, N.J.; Smith, A.G.C.; Bernabé, E.; Fleming, T.D.; Reynolds, A.E.; Vos, T.; Murray, C.J.L.; Marcenes, W.; GBD 2015 Oral Health Collaborators. Global, regional, and national prevalence, incidence, and disability adjusted life years for oral conditions for 195 countries, 1990–2015: A systematic analysis for the global burden of diseases, injuries, and risk factors. J. Dent. Res. 2017, 96, 380–387. [Google Scholar] [CrossRef] [PubMed]
- Gusmano, M.K.; Laugesen, M.; Rodwin, V.G.; Brown, L.D. Getting the price right: How Some countries control spending in a fee-for-service system. Health Aff. 2020, 39, 1867–1874. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffman, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 1–9. [Google Scholar] [CrossRef]
- Thomas, B.H.; Ciliska, D.; Dobbins, M.; Micucci, S. A process for systematically reviewing the literature: Providing the research evidence for public health nursing interventions. Worldviews Evid. Based Nurs. 2004, 1, 76–184. [Google Scholar] [CrossRef] [PubMed]
- Chillón, P.; Evenson, K.R.; Vaughn, A.; Ward, D.S. A systematic review of interventions for promoting active transportation to school. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 1–17. Available online: http://www.ijbnpa.org/content/8/1/10 (accessed on 8 April 2021). [CrossRef] [PubMed]
- Schardt, C.; Adams, M.B.; Owens, T.; Keitz, S.; Fontelo, P. Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Med. Inform. Decis. Mak. 2007, 7, 16. [Google Scholar] [CrossRef] [PubMed]
- Andås, C.A.; Hakeberg, M. Who chooses prepaid dental care? A baseline report of a prospective observational study. BMC Oral Health 2014, 14, 146. [Google Scholar] [CrossRef] [PubMed]
- Andås, C.A.; Hakeberg, M. Payment systems and oral health in Swedish dental care: Observations over six years. Community Dent. Health 2016, 33, 257–261. [Google Scholar] [CrossRef] [PubMed]
- Brocklehurst, P.; Tickle, M.; Birch, S.; McDonald, R.; Walsh, T.; Goodwin, T.L.; Hill, H.; Howarth, E.; Donaldson, M.; O’Carolan, D.; et al. Impact of changing provider remuneration on NHS general dental practitioner services in Northern Ireland: A mixed-methods study. Health Serv. Deliv. Res. 2020, 8, 1–168. [Google Scholar] [CrossRef] [PubMed]
- Woods, N. The role of payments systems in influencing oral health care provision. OA Dent. 2013, 1, 1–4. [Google Scholar] [CrossRef][Green Version]
- Voinea-Griffin, A.; Fellows, J.L.; Rindal, D.B.; Barasch, A.; Gilbert, G.H.; Safford, M.M. Pay for performance: Will dentistry follow? BMC Oral Health 2010, 10, 9. [Google Scholar] [CrossRef] [PubMed]
- Hill, H.; Howarth, E.; Walsh, T.; Tickle, M.; Birch, S.; Brocklehurst, P. The impact of changing provider remuneration on clinical activity and quality of care: Evaluation of a pilot NHS contract in Northern Ireland. Community Dent Oral Epidemiol. 2020, 48, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Strand, J.; Andås, C.A.; Boman, U.W.; Hakeberg, M.; Tidefors, I. A new capitation system in dentistry: The patients’ perspective. Community Dent. Health 2015, 32, 83–88. Available online: https://pubmed.ncbi.nlm.nih.gov/26263600/ (accessed on 30 October 2020).
- Voinea-Griffin, A.; Rindal, B.; Fellows, J.L.; Barasch, A.; Gilbert, G.H.; Safford, M.M.; DPBRN Collaborative Group. Pay for performance in dentistry: What we know. J. Healthc. Qual. 2010, 32, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Tickle, M. Revolution in the provision of dental services in the UK. Community Dent. Oral Epidemiol. 2012, 40, 110–116. [Google Scholar] [CrossRef] [PubMed]
- Whittaker, W.; Birch, S. Provider incentives and access to dental care: Evaluating NHS reforms in England. Soc. Sci. Med. 2012, 75, 2515–2521. [Google Scholar] [CrossRef] [PubMed]
- Schneider, E.C.; Sarnak, D.O.; Squires, D.; Shah, A.; Dory, M.M. Mirror, Mirror 2017: International Comparison Reflects Flaws and Opportunities for Better, U.S. Health Care; The Commonwealth Fund: Washington, DC, USA, 2017; Available online: https://interactives.commonwealthfund.org/2017/july/mirror-mirror/ (accessed on 30 October 2020).
- Centre for Oral Health Strategy. Oral Health 2020: A Strategic Framework for Dental Health in NSW; NSW Ministry of Health, Nth: Sydney, NSW, Australia, 2013. [Google Scholar]
- Dawda, P. Bundled Payments: Their Role in Australian Primary Health Care; Australian Healthcare & Hospitals Association: Canberra, ACT, Australia, 2015. Available online: https://www.health.nsw.gov.au/oralhealth/Publications/oral-health-2020.pdf (accessed on 3 August 2021).
- Daly, B.; Batchelor, P.; Treasure, E.T.; Watt, R.G. Essential Dental Public Health, 2nd ed.; Oxford University Press: Hampshire, UK, 2013; ISBN 978-0-19-967937-9. [Google Scholar]
- Watt, R.G.; Steele, G.; Treasure, E.T.; White, D.A.; Pitts, N.B.; Murray, J.J. Adult Dental Health Survey 2009: Implications of findings for clinical practice and oral health policy. Br. Dent. J. 2013, 214, 71–75. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Study (n = 10) | Title | Objective | Study Design | Selection Bias and Cohort, Population | Outcome(s) | EPHPP Global Rating |
|---|---|---|---|---|---|---|
| Andäs C A., Hakeberg M (2014) Sweden [12] | Who chooses prepaid dental care? A baseline report of a prospective observational study | Describes potential differences regarding socioeconomic and lifestyle factors, perceived oral health and attitudes towards oral health between patients in the two payment systems (Swedish capitation system and the FFS within the Public Dental Service). | Moderate quasi-experimental design | Strong 13,719 patients enrolled from 20 PDS clinics selected through a stratified, random procedure. Participants who were ≥20 years (male and female) chose their service type. Participants had education levels. | Patients who chose to prepay differed statistically significantly (e.g., BMI, sex, and age) than those who chose to pay traditionally. | Strong |
| Andäs C A., Hakeberg M (2016) Sweden [13] | Payment Systems and oral health in Swedish dental care: observations over 6 years | The aim of this study was patients in regular dental care compare to the findings of manifest caries and fillings after a 6-year period of care. Either through FFS or capped-fee, e.g., Dental Care for Health (DCH). | Weak longitudinal study | Moderate The target population was 485,000 number of adults ≥20 years (male and female) was 6229. There was 100% participation rate. | The incidence rate ratio of manifest caries lesions after six years in FFS was 1.5 times higher than capped-fee (DCH). | Moderate |
| Brocklehurst P, et al., (2020) Northern Ireland [14] | Impact of changing provider remuneration on NHS general dental practitioner services in Northern Ireland: a mixed-methods study | Study looked at the levels of care between capped-fee and FFS back to capped-fee. | Strong systematic review | Weak Control practices, practices varied in practice size. Behaviours of equity-owning practice principles and non-equity-owning associate dentists. Age groups were that of children and ≥24 to 60 years of age. The participants were not representative of the target population. | A move from FFS to capped-fee had little impact on access but produced large reductions in clinical activity and patient charge income. Patients noticed little difference in the service that they received. | Moderate |
| Woods, N. (2013) United Kingdom, Norway, and Ireland [15] | The role of payments systems in influencing oral health care provision | Among the leading strategies to reform health care is the development and implementation of new payment models. The goal is to change the way physicians, dentists, hospitals, and other care providers are paid to emphasise value for money. | Strong systematic review | Weak Participants were children and adults (aged 16 years). Unable to determine participant rate. | The optimal dental contract may be a ‘blended’ payment system whereby dentists receive a proportion of their income through capped-fee, a proportion from allowances and proportion from FFS. | Moderate |
| Voinea-Griffith A, et al., (2010b) United Kingdom and United States of America [16] | Pay for performance: will dentistry follow? | This article explored factors that would influence the adoption of value-based purchasing programs in dentistry. | Strong systematic review | Weak Analysis covers such aspects as variation in dental care, evidence-based dentistry, outcome indicators, diagnostic codes. Cohort covers all ages; age groups and sex not identified. Unable to determine participant rate. | Discussion on dentists’ performance under FSS and who work in the community and/or dental organisations. | Moderate |
| Hill H, et al., (2020) Northern Ireland [17] | The impact of changing provider remuneration a clinical activity and quality of care: Evaluation of a pilot NHS contract in Northern Ireland | This study was a pilot to introduce NHS general dental practitioner contractual system in Northern Ireland (2015 and 2016). | Moderate difference-in-difference (DiD) evaluation | Weak Participants were a mix of socioeconomic status, both child and adult and no sex or age groups identified. There was less than 60% of the cohort agreed to participate. | Overall, the move to a capped-fee from FFS suppressed clinical activity, including prevention. | Moderate |
| Strand J, et al., (2015) Sweden [18] | A new capitation payment system in dentistry: the patients’ perspective | Explore patients’ experiences and attitudes to a new dental payment system regarding the contract, risk assessment, dental care content and economy, as well as the advantages and disadvantages of the payment system. | Weak qualitative research | Weak 20 interviews with 12 women and 8 men between the ages of 24 to 60 years. 77% of the cohort agreed to participate. | Patients were generally in favour of the capped-fee. | Weak |
| Voinea-Griffith A et al., (2010a) United Kingdom and United States of America [19] | Pay for performance in dentistry: what we know | Current experience of Pay for Performance system (P4P-FFS) in primary medical care that has relevance to dentistry and discuss the dental performance-based programs to date. | Strong qualitative analysis | Weak Cohort covers all ages; age groups and sex not identified. Unable to determine participant rate. | FFS could be successful if there is: (i) explanation of knowledge; (ii) increase in evidence-based clinical guidelines; and (iii) evidence-based performance measures tied to existing clinical practice guidelines. | Moderate |
| Tickle M. (2012) United Kingdom [20] | Revolution in the provision of dental services in the UK | This paper provides a historical overview of NHS dental services and some personal reflections on the main challenges over the next five years. | Moderate study on narrative literature review (not systematic) and some subjective comments included | Weak Article is based on other articles analysing pilots of capped-fee and FFS that is paid for NHS budget. Participants (child and adult) and age or sex were not identified. Unable to determine participant rate. | Article discusses the history of payment (capped-fee and FFS) transitions of the NHS between 2205 and 2010 as well as historical dental services (1948). It concludes that the NHS will be in financial trouble in years to come because of the inability to control its finances. | Moderate |
| Whittaker W., Birch S. (2012) United Kingdom [21] | Provider incentives and access to dental care: Evaluating NHS reforms in England | England aimed at improving access to populations with low use. This included: (i) commissioning of NHS dental services by primary care trusts (ii) replacing FFS patient charges by capped-fees and (iii) changing the remuneration of dentists providing dental care. | Strong longitudinal study | Strong 5000 households, and approximately 10,000 individuals (≥16 years and sex not identified). | Evidence shows a decrease in NHS use, driven by those who had previously good access to care. This trend had positive effects on the consumer’s transitions from NHS to private practice. This transition relied upon the ability of the private sector to absorb the demand. | Strong |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Conquest, J.H.; Gill, N.; Sivanujan, P.; Skinner, J.; Kruger, E.; Tennant, M. Systematic Literature Review of Capitation and Fee-for-Service Payment Models for Oral Health Services: An Australian Perspective. Healthcare 2021, 9, 1129. https://doi.org/10.3390/healthcare9091129
Conquest JH, Gill N, Sivanujan P, Skinner J, Kruger E, Tennant M. Systematic Literature Review of Capitation and Fee-for-Service Payment Models for Oral Health Services: An Australian Perspective. Healthcare. 2021; 9(9):1129. https://doi.org/10.3390/healthcare9091129
Chicago/Turabian StyleConquest, Jennifer H., Nirjgot Gill, Praveena Sivanujan, John Skinner, Estie Kruger, and Marc Tennant. 2021. "Systematic Literature Review of Capitation and Fee-for-Service Payment Models for Oral Health Services: An Australian Perspective" Healthcare 9, no. 9: 1129. https://doi.org/10.3390/healthcare9091129
APA StyleConquest, J. H., Gill, N., Sivanujan, P., Skinner, J., Kruger, E., & Tennant, M. (2021). Systematic Literature Review of Capitation and Fee-for-Service Payment Models for Oral Health Services: An Australian Perspective. Healthcare, 9(9), 1129. https://doi.org/10.3390/healthcare9091129