
Effect of Ranitidine Intake on the Risk of Gastric Cancer Development

 , and
, and
Abstract
:1. Introduction
2. Experimental Section
2.1. Korea National Health Insurance Service
2.2. Study Population
2.3. Predictor and Outcome Variables
2.4. Statistical Analysis
3. Results
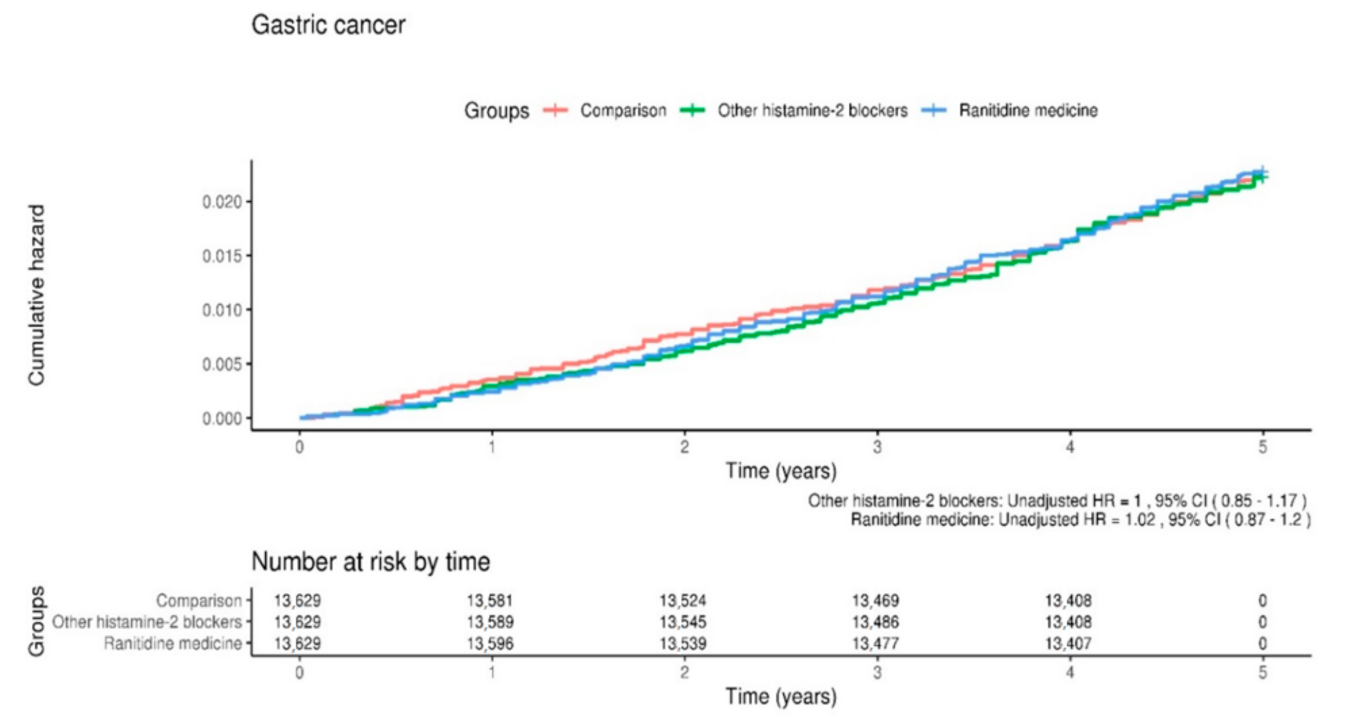
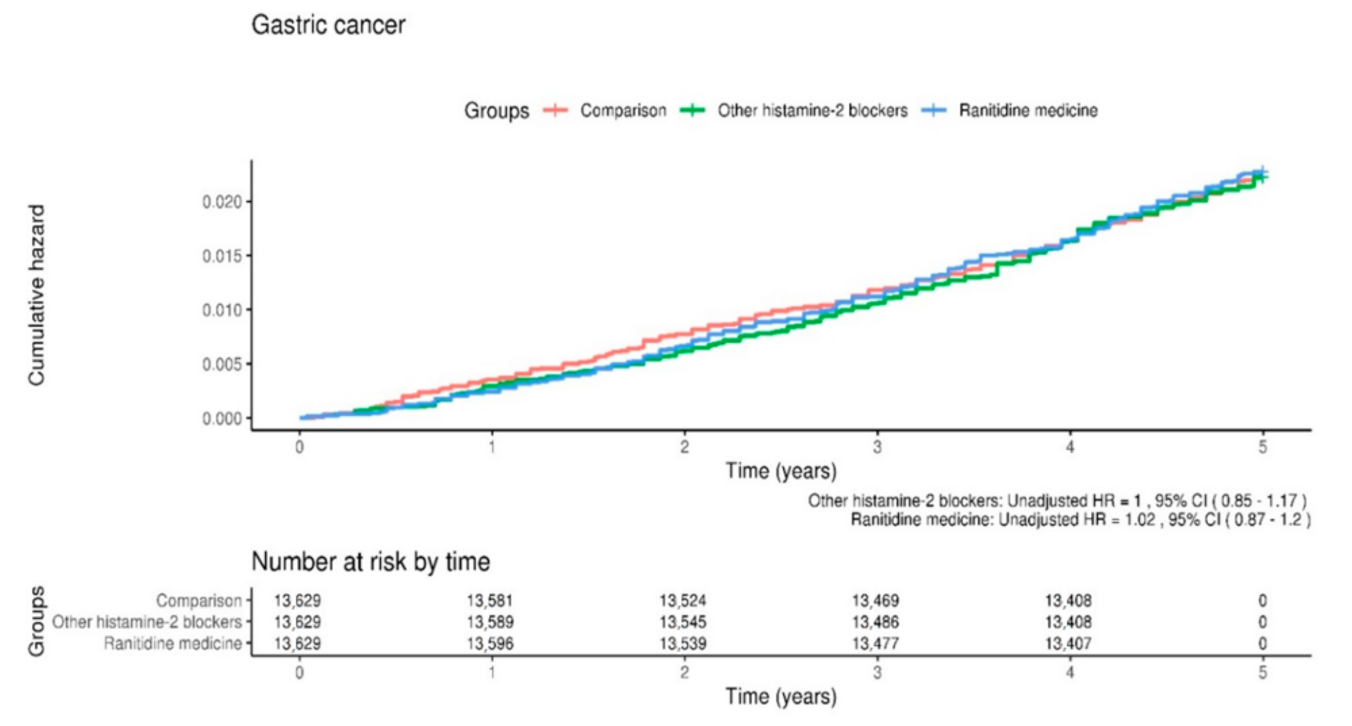
3.1. Incidence of Gastric Cancer
3.2. Hazard Ratio
3.3. Predictor and Outcome Variables
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global Cancer Statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Rawla, P.; Barsouk, A. Epidemiology of gastric cancer: Global trends, risk factors and prevention. Gastroenterol. Rev. 2019, 14, 26–38. [Google Scholar] [CrossRef] [PubMed]
- Balakrishnan, M.; George, R.; Sharma, A.; Graham, D.Y. Changing trends in stomach cancer throughout the world. Curr. Gastroenterol. Rep. 2017, 19, 36. [Google Scholar] [CrossRef] [PubMed]
- Noto, J.M.; Peek, R.M. The gastric microbiome, its interaction with Helicobacter pylori, and its potential role in the progression to stomach cancer. PLoS Pathog. 2017, 13, e1006573. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Take, S.; Mizuno, M.; Ishiki, K.; Nagahara, Y.; Yoshida, T.; Yokota, K.; Oguma, K. Baseline gastric mucosal atrophy is a risk factor associated with the development of gastric cancer after Helicobacter pylori eradication therapy in patients with peptic ulcer diseases. J. Gastroenterol. 2007, 42, 21–27. [Google Scholar] [CrossRef]
- Ladeiras-Lopes, R.; Pereira, A.K.; Nogueira, A.; Pinheiro-Torres, T.; Pinto, I.; Santos-Pereira, R.; Lunet, N. Smoking and gastric cancer: Systematic review and meta-analysis of cohort studies. Cancer Causes Control. 2008, 19, 689–701. [Google Scholar] [CrossRef]
- Tramacere, I.; Negri, E.; Pelucchi, C.; Bagnardi, V.; Rota, M.; Scotti, L.; Islami, F.; Corrao, G.; La Vecchia, C.; Boffetta, P. A meta-analysis on alcohol drinking and gastric cancer risk. Ann. Oncol. 2012, 23, 28–36. [Google Scholar] [CrossRef]
- Fortunato, L.; Rushton, L. Stomach cancer and occupational exposure to asbestos: A meta-analysis of occupational cohort studies. Br. J. Cancer 2015, 112, 1805–1815. [Google Scholar] [CrossRef] [Green Version]
- Weisburger, J.H.; Reddy, B.S.; Hill, P.; Cohen, L.A.; Wynder, E.L.; Spingarn, N.E. Nutrition and cancer—On the mechanisms bearing on causes of cancer of the colon, breast, prostate, and stomach. Bull. NY Acad. Med. 1980, 56, 673–696. [Google Scholar]
- Eichholzer, M.; Gutzwiller, F. Dietary nitrates, nitrites, and n-nitroso compounds and cancer risk: A review of the epidemiologic evidence. Nutr. Rev. 1998, 56, 95–105. [Google Scholar] [CrossRef] [Green Version]
- Tsugane, S.; Sasazuki, S. Diet and the risk of gastric cancer: Review of epidemiological evidence. Gastric Cancer 2007, 10, 75–83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knekt, P.; Dich, J.; Hakulinen, T. Risk of colorectal and other gastro-intestinal cancers after exposure to nitrate, nitrite andN-nitroso compounds: A follow-up study. Int. J. Cancer 1999, 80, 852–856. [Google Scholar] [CrossRef]
- Song, P.; Wu, L.; Guan, W. Dietary nitrates, nitrites, and nitrosamines intake and the risk of gastric cancer: A meta-analysis. Nutr. 2015, 7, 9872–9895. [Google Scholar] [CrossRef]
- Tricker, A.; Pfundstein, B.; Theobald, E.; Preussmann, R.; Spiegelhalder, B. Mean daily intake of volatile N-nitrosamines from foods and beverages in West Germany in 1989–1990. Food Chem. Toxicol. 1991, 29, 729–732. [Google Scholar] [CrossRef]
- Jakszyn, P.; Agudo, A.; Berenguer-Llergo, A.; Ibáñez, R.; Amiano, P.; Pera, G.; Ardanaz, E.; Barricarte, A.; Chirlaque, M.D.; Dorronsoro, M.; et al. Intake and food sources of nitrites and N-nitrosodimethylamine in Spain. Public Heal. Nutr. 2006, 9, 785–791. [Google Scholar] [CrossRef] [Green Version]
- Tricker, A.R.; Preussmann, R. Carcinogenic N-nitrosamines in the diet: Occurrence, formation, mechanisms and carcinogenic potential. Mutat. Res. Toxicol. 1991, 259, 277–289. [Google Scholar] [CrossRef]
- Anderson, L.M.; Souliotis, V.L.; Chhabra, S.K.; Moskal, T.J.; Harbaugh, S.D.; Kyrtopoulos, S.A. N-nitrosodimethylamine-derived O(6)-methylguanine in DNA of monkey gastrointestinal and urogenital organs and enhancement by ethanol. Int. J. Cancer 1996, 66, 130–134. [Google Scholar] [CrossRef]
- Mahase, E. FDA recalls ranitidine medicines over potential cancer causing impurity. BMJ 2019, 367, l5832. [Google Scholar] [CrossRef] [PubMed]
- Mahase, E. Ranitidine: Patients taking certain batches should “immediately discontinue use,” says FDA. BMJ 2019, 367, l7053. [Google Scholar] [CrossRef]
- Kim, Y.D.; Wang, J.; Shibli, F.; Poels, K.E.; Ganocy, S.J.; Fass, R. No association between chronic use of ranitidine, compared with omeprazole or famotidine, and gastrointestinal malignancies. Aliment. Pharmacol. Ther. 2021, 12, 606–615. [Google Scholar] [CrossRef]
- Kumar, S.; Goldberg, D.S.; Kaplan, D.E. Ranitidine use and gastric cancer among persons with Helicobacter pylori. Dig. Dis. Sci. 2021, 15, 1–9. [Google Scholar] [CrossRef]
- Iwagami, M.; Kumazawa, R.; Miyamoto, Y.; Ito, Y.; Ishimaru, M.; Morita, K.; Hamada, S.; Tamiya, N.; Yasunaga, H. Risk of cancer in association with ranitidine and nizatidine vs. other H2 blockers: Analysis of the Japan medical data center claims database 2005–2018. Drug Saf. 2021, 44, 361–371. [Google Scholar] [CrossRef] [PubMed]
- McGwin, G. The association between ranitidine use and gastrointestinal cancers. Cancers 2020, 13, 24. [Google Scholar] [CrossRef]
- Cardwell, C.R.; McDowell, R.D.; Hughes, C.M.; Hicks, B.; Murchie, P. Exposure to ranitidine and risk of bladder cancer. Am. J. Gastroenterol. 2021, 116, 1612–1619. [Google Scholar] [CrossRef]
- Relevance of N-nitroso compounds to human cancer: Exposures and mechanisms. In Proceedings of the IXth International Symposium on N-Nitroso Compounds, Baden, Austria, 1–5 September 1986; IARC Scientific Publications: Lyon, France, 1987; pp. 1–663.
- Kim, J.-Y.; Ko, I.; Kim, M.S.; Yu, M.S.; Cho, B.-J.; Kim, D.-K. Association of chronic rhinosinusitis with depression and anxiety in a nationwide insurance population. JAMA Otolaryngol. Neck Surg. 2019, 145, 313–319. [Google Scholar] [CrossRef]
- Kim, J.-Y.; Ko, I.; Cho, B.-J.; Kim, D.-K. Association of obstructive sleep apnea with the risk of Ménière’s disease and sudden sensorineural hearing loss: A study using data from the Korean National Health Insurance Service. J. Clin. Sleep Med. 2019, 15, 1293–1301. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.-Y.; Ko, I.; Kim, M.S.; Kim, D.W.; Cho, B.-J.; Kim, D.-K. Relationship of chronic rhinosinusitis with asthma, myocardial infarction, stroke, anxiety, and depression. J. Allergy Clin. Immunol. Pract. 2020, 8, 721–727.e3. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.-Y.; Ko, I.; Kim, D.-K. Association of obstructive sleep apnea with the risk of affective disorders. JAMA Otolaryngol. Neck Surg. 2019, 145, 1020–1026. [Google Scholar] [CrossRef]
- Cheung, K.-S.; Chan, E.W.Y.; Wong, A.Y.S.; Chen, L.; Wong, I.C.K.; Leung, W.K. Long-term proton pump inhibitors and risk of gastric cancer development after treatment for Helicobacter pylori: A population-based study. Gut 2017, 67, 28–35. [Google Scholar] [CrossRef] [Green Version]
- Wan, Q.-Y.; Wu, X.-T.; Li, N.; Du, L.; Zhou, Y. Long-term proton pump inhibitors use and risk of gastric cancer: A meta-analysis of 926 386 participants. Gut 2018, 68, 762–764. [Google Scholar] [CrossRef]
- Cheung, K.S.; Leung, W.K. Long-term use of proton-pump inhibitors and risk of gastric cancer: A review of the current evidence. Ther. Adv. Gastroenterol. 2019, 12, 1756284819834511. [Google Scholar] [CrossRef] [PubMed]
- Archimandritis, A.; Bitsikas, J.; Tjivras, M.; Anastasakou, E.; Tsavaris, N.; Kalogeras, D.; Davaris, P.; Fertakis, A. Non-cardia gastric adenocarcinoma and Helicobacter pylori infection. Ital. J. Gastroenterol. 1993, 25, 368–371. [Google Scholar] [PubMed]
- Nguyen, T.H.; Mallepally, N.; Hammad, T.; Liu, Y.; Thrift, A.P.; El-Serag, H.B.; Tan, M.C. Prevalence of Helicobacter pylori positive non-cardia gastric adenocarcinoma is low and decreasing in a US population. Dig. Dis. Sci. 2019, 65, 2403–2411. [Google Scholar] [CrossRef] [PubMed]
- Ye, W.; Held, M.; Lagergren, J.; Engstrand, L.; Blot, W.J.; McLaughlin, J.K.; Nyrén, O. Helicobacter pylori infection and gastric atrophy: Risk of adenocarcinoma and squamous-cell carcinoma of the esophagus and adenocarcinoma of the gastric cardia. J. Natl. Cancer Inst. 2004, 96, 388–396. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| Variable | Comparison (n = 13,629) | Other Histamine-2 Blockers (n = 13,629) | Ranitidine Medicine (n = 132,629) | p Value |
|---|---|---|---|---|
| Sex | 0.976 | |||
| Female | 5848 (42.9%) | 5830 (42.8%) | 5838 (42.8%) | |
| Male | 7781 (57.1%) | 7799 (57.2%) | 7791 (57.2%) | |
| Age (years) | >0.999 | |||
| 20–44 | 9204 (67.5%) | 9207 (67.6%) | 9211 (67.6%) | |
| 45–64 | 3740 (27.4%) | 3741 (27.4%) | 3739 (27.4%) | |
| ≥65 | 685 (5.0%) | 681 (5.0%) | 679 (5.0%) | |
| Residence | >0.999 | |||
| Seoul (metropolitan) | 2884 (21.2%) | 2880 (21.1%) | 2891 (21.2%) | |
| Second area (other metropolitan) | 3513 (25.8%) | 3517 (25.8%) | 3518 (25.8%) | |
| Third area | 7232 (53.1%) | 7232 (53.1%) | 7220 (53.0%) | |
| Household income | 0.999 | |||
| Low (0–30%) | 3213 (23.6%) | 3209 (23.5%) | 3221 (23.6%) | |
| Middle (31–70%) | 5395 (39.6%) | 5379 (39.5%) | 5377 (39.5%) | |
| High (71–100%) | 5021 (36.8%) | 5041 (37.0%) | 5031 (36.9%) | |
| Disability | 0.539 | |||
| No | 13,238 (97.1%) | 13,219 (97.0%) | 13,207 (96.9%) | |
| Yes | 391 (2.9%) | 410 (3.0%) | 422 (3.1%) | |
| NSAID | >0.999 | |||
| No | 1700 (12.5%) | 1697 (12.5%) | 1700 (12.5%) | |
| <60 days | 8082 (59.3%) | 8088 (59.3%) | 8080 (59.3%) | |
| 60–120 days | 1883 (13.8%) | 1872 (13.7%) | 1872 (13.7%) | |
| 120–180 days | 546 (4.0%) | 559 (4.1%) | 561 (4.1%) | |
| >180 days | 1418 (10.4%) | 1413 (10.4%) | 1416 (10.4%) | |
| Smoking | >0.999 | |||
| Never | 8671 (63.6%) | 8664 (63.6%) | 8661 (63.5%) | |
| Former | 1491 (10.9%) | 1502 (11.0%) | 1500 (11.0%) | |
| Current | 3467 (25.4%) | 3463 (25.4%) | 3468 (25.4%) | |
| Alcohol Drinking habit | >0.999 | |||
| Rare | 7258 (53.3%) | 7252 (53.2%) | 7240 (53.1%) | |
| Intermediate | 5222 (38.3%) | 5228 (38.4%) | 5235 (38.4%) | |
| Heavy | 1149 (8.4%) | 1149 (8.4%) | 1154 (8.5%) |
| Variable | Case | Person Year | Incidence |
|---|---|---|---|
| Group | |||
| Control | 300 | 67,422 | 4.40 |
| Other histamine-2 blockers | 300 | 67,470 | 4.40 |
| Ranitidine medicine | 306 | 67,444 | 4.50 |
| Sex | |||
| Female | 291 | 86,930 | 3.30 |
| Male | 615 | 115,406 | 5.30 |
| Age (years) | |||
| 20–44 | 151 | 137,703 | 1.10 |
| 45–64 | 365 | 55,254 | 6.60 |
| ≥65 | 390 | 9380 | 41.60 |
| Residence | |||
| Seoul (metropolitan) | 128 | 42,954 | 3.00 |
| Second area (other metropolitan) | 192 | 52,312 | 3.70 |
| Third area | 586 | 107,070 | 5.50 |
| Household income | |||
| Low (0–30%) | 275 | 47,602 | 5.80 |
| Middle (31–70%) | 330 | 80,003 | 4.10 |
| High (71–100%) | 301 | 74,731 | 4.00 |
| Disability | |||
| No | 826 | 196,401 | 4.20 |
| Yes | 80 | 5935 | 13.50 |
| NSAID | |||
| No | 78 | 25,310 | 3.10 |
| <60 days | 369 | 120,330 | 3.10 |
| 60–120 days | 122 | 27,853 | 4.40 |
| 121–180 days | 77 | 8169 | 9.40 |
| >180 days | 260 | 20,673 | 12.60 |
| Smoking | |||
| Never | 576 | 128,655 | 4.50 |
| Former | 94 | 22,240 | 4.20 |
| Current | 236 | 51,441 | 4.60 |
| Alcohol drinking habit | |||
| Rare | 578 | 107,445.2 | 5.40 |
| Intermediate | 245 | 77,839.9 | 3.10 |
| Heavy | 83 | 17,050.6 | 4.90 |
| Variable | Unadjusted HR 1 (95% CI) | p Value | Adjusted HR 1 (95% CI) | p Value |
|---|---|---|---|---|
| Group | ||||
| Control | 1 (ref) | 1 (ref) | ||
| Other histamine-2 blockers | 1 (0.85–1.17) | 0.99 | 0.98 (0.84–1.15) | 0.83 |
| Ranitidine medicine | 1.02 (0.87–1.2) | 0.81 | 1.01 (0.86–1.18) | 0.94 |
| Sex | ||||
| Female | 1 (ref) | 1 (ref) | ||
| Male | 1.59 (1.39–1.83) | 0.00 | 1.88 (1.6–2.22) | 0.00 |
| Age (years) | ||||
| 20–44 | 1 (ref) | 1 (ref) | ||
| 45–64 | 6.04 (4.99–7.3) | 0.00 | 5.94 (4.88–7.23) | 0.00 |
| ≥65 | 38.5 (31.9–46.45) | 0.00 | 39.05 (31.64–48.19) | 0.00 |
| Residence | ||||
| Seoul (metropolitan) | 1 (ref) | 1 (ref) | ||
| Second area (other metropolitan) | 1.23 (0.98–1.54) | 0.07 | 1.1 (0.88–1.38) | 0.39 |
| Third area | 1.84 (1.52–2.23) | 0.00 | 1.33 (1.09–1.61) | 0.00 |
| Household income | ||||
| Low (0–30%) | 1 (ref) | 1 (ref) | ||
| Middle (31–70%) | 0.71 (0.61–0.84) | 0.00 | 1.01 (0.86–1.19) | 0.90 |
| High (71–100%) | 0.7 (0.59–0.82) | 0.00 | 0.75 (0.63–0.88) | 0.00 |
| Disability | ||||
| No | 1 (ref) | 1 (ref) | ||
| Yes | 3.22 (2.56–4.05) | 0.00 | 1.93 (1.53–2.44) | 0.00 |
| NSAID | ||||
| No | 1 (ref) | 1 (ref) | ||
| <60 days | 1 (0.78–1.27) | 0.97 | 1.02 (0.8–1.31) | 0.86 |
| 60–120 days | 1.42 (1.07–1.89) | 0.02 | 1.04 (0.78–1.38) | 0.81 |
| 121–180 days | 3.07 (2.24–4.2) | 0.00 | 1.64 (1.19–2.25) | 0.00 |
| >180 days | 4.09 (3.18–5.27) | 0.00 | 1.24 (0.96–1.62) | 0.10 |
| Smoking | ||||
| Never | 1 (ref) | 1 (ref) | ||
| Former | 0.94 (0.76–1.17) | 0.61 | 0.99 (0.78–1.25) | 0.92 |
| Current | 1.02 (0.88–1.19) | 0.75 | 1.39 (1.17–1.67) | 0.00 |
| Alcohol drinking habit | ||||
| Rare | 1 (ref) | 1 (ref) | ||
| Intermediate | 0.58 (0.50–0.68) | 0.00 | 0.84 (0.72–1.00) | 0.05 |
| Heavy | 0.9 (0.72–1.14) | 0.39 | 1.18 (0.92–1.52) | 0.19 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, S.; Lee, S.; Hong, J.; Ko, I.; Kim, J.-Y.; Kim, D.-K. Effect of Ranitidine Intake on the Risk of Gastric Cancer Development. Healthcare 2021, 9, 1071. https://doi.org/10.3390/healthcare9081071
Kim S, Lee S, Hong J, Ko I, Kim J-Y, Kim D-K. Effect of Ranitidine Intake on the Risk of Gastric Cancer Development. Healthcare. 2021; 9(8):1071. https://doi.org/10.3390/healthcare9081071
Chicago/Turabian StyleKim, SunMoon, Suehyun Lee, JeeYoung Hong, Inseok Ko, Jong-Yeup Kim, and Dong-Kyu Kim. 2021. "Effect of Ranitidine Intake on the Risk of Gastric Cancer Development" Healthcare 9, no. 8: 1071. https://doi.org/10.3390/healthcare9081071
APA StyleKim, S., Lee, S., Hong, J., Ko, I., Kim, J.-Y., & Kim, D.-K. (2021). Effect of Ranitidine Intake on the Risk of Gastric Cancer Development. Healthcare, 9(8), 1071. https://doi.org/10.3390/healthcare9081071