
Blended Learning on Blood Pressure Measurement: Investigating Two In-Class Strategies in a Flipped Classroom-Like Setting to Teach Pharmacy Students Blood Pressure Measurement Skills

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Objectives
2.2. Study Design and Procedure
2.3. Flipped Classroom Approach
2.3.1. Out-of-Class Activity
2.3.2. In-Class Session
Group with Brief In-Class Session (Group A)
Group with Extended In-Class Session (Group B)
2.4. Data Collection
2.4.1. Objective Structured Clinical Examination
2.4.2. OSCE Checklist
2.4.3. Self-Assessment Survey
2.4.4. Perception and Satisfaction Survey
2.5. Statistical Analysis
3. Results
3.1. Effect of the Two Flipped Classroom-Like Approaches
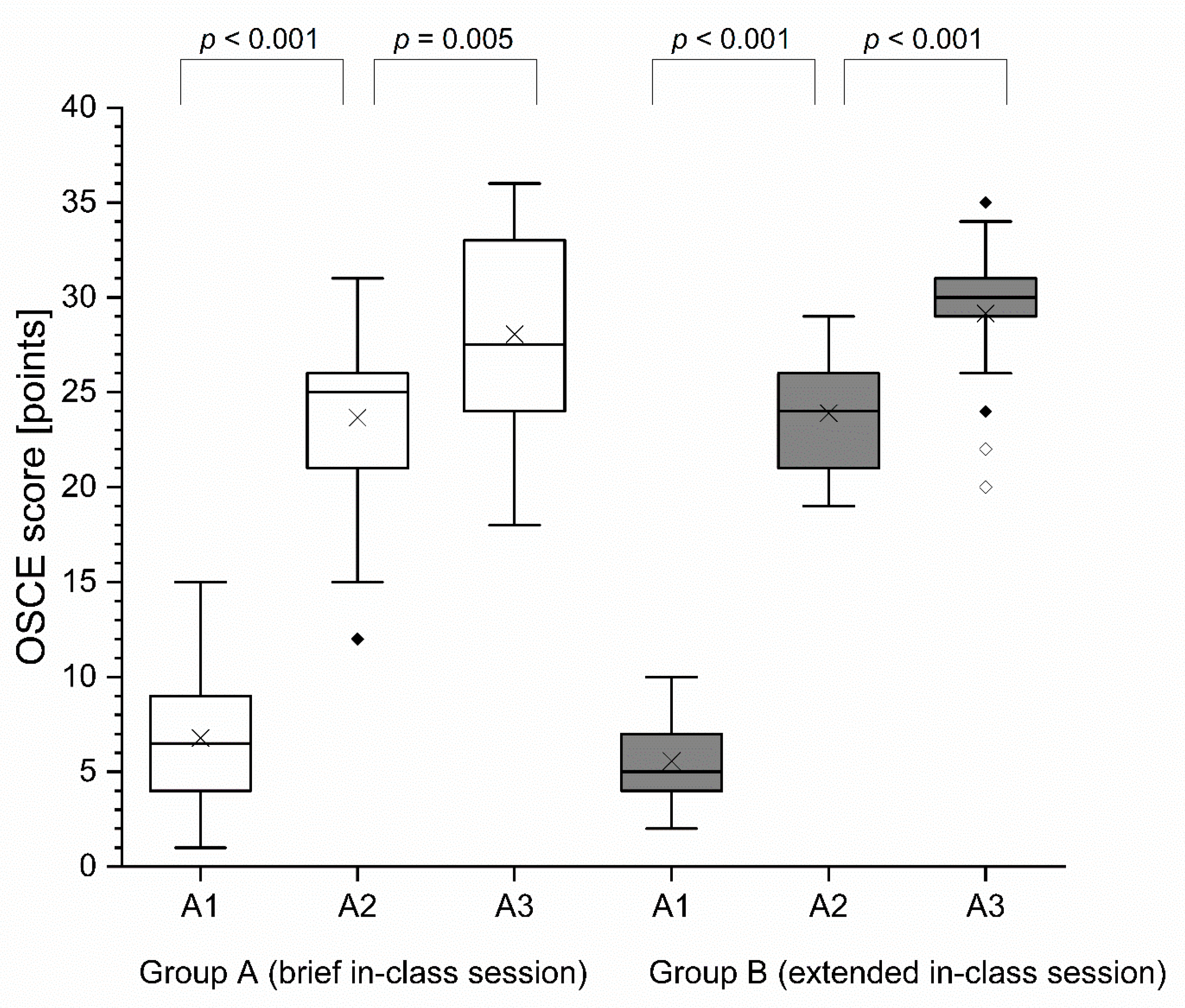
3.1.1. OSCE Score
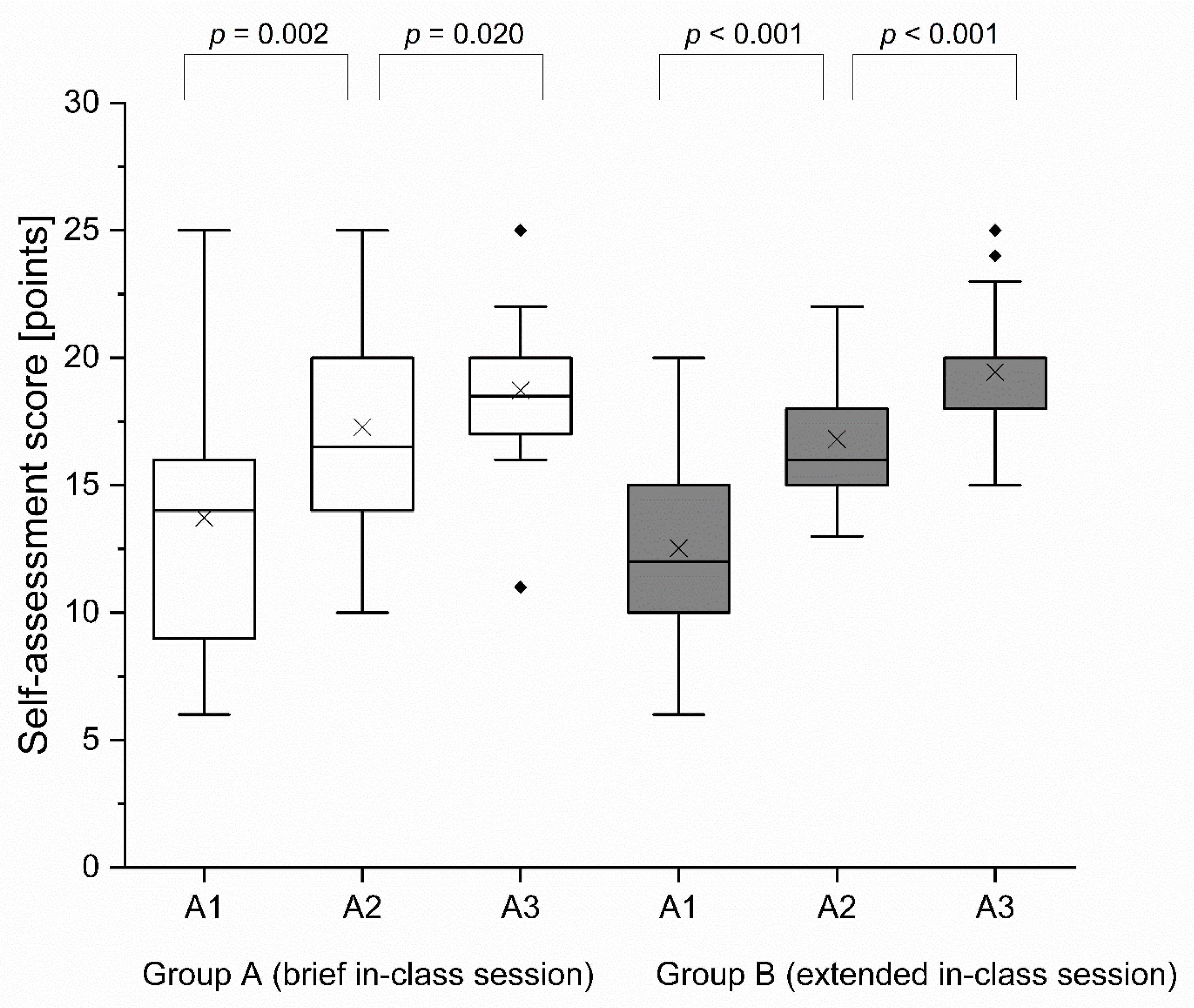
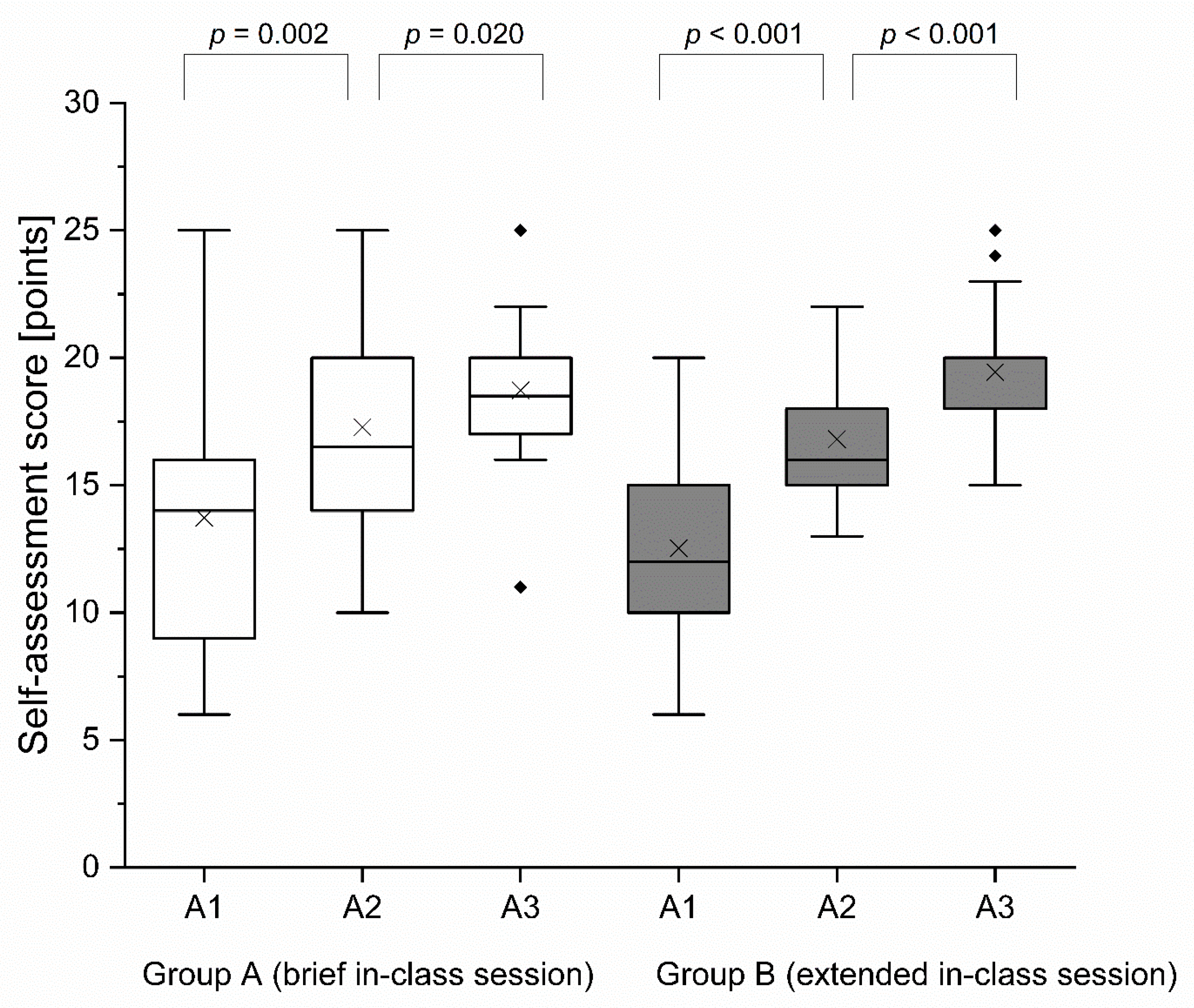
3.1.2. Self-Assessment Score
3.1.3. Perception and Satisfaction Survey
3.1.4. Video Access
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- GBD 2017 Risk Factor Collaborators. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1923–1994. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. A Global Brief on Hypertension: Silent Killer, Global Public Health Crisis: World Health Day 2013. Available online: https://apps.who.int/iris/handle/10665/79059 (accessed on 25 June 2021).
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.F.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104, corrected in Eur. Heart J. 2019, 40, 475. [Google Scholar] [CrossRef]
- Kehrer, J.P.; Eberhart, G.; Wing, M.; Horon, K. Pharmacy’s role in a modern health continuum. Can. Pharm. J. 2013, 146, 321–324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santschi, V.; Chiolero, A.; Colosimo, A.L.; Platt, R.W.; Taffé, P.; Burnier, M.; Burnand, B.; Paradis, G. Improving blood pressure control through pharmacist interventions: A meta-analysis of randomized controlled trials. J. Am. Heart Assoc. 2014, 3, e000718. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reeves, L.; Robinson, K.; McClelland, T.; Adedoyin, C.A.; Broeseker, A.; Adunlin, G. Pharmacist Interventions in the Management of Blood Pressure Control and Adherence to Antihypertensive Medications: A Systematic Review of Randomized Controlled Trials. J. Pharm. Pract. 2021, 34, 480–492. [Google Scholar] [CrossRef] [PubMed]
- Cheema, E.; Sutcliffe, P.; Singer, D.R.J. The impact of interventions by pharmacists in community pharmacies on control of hypertension: A systematic review and meta-analysis of randomized controlled trials. Br. J. Clin. Pharmacol. 2014, 78, 1238–1247. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization; Regional Office for Europe. Pharmacy-Based Hypertension Management Model: Protocol and Guidelines: A Joint CINDI/EuroPharm Forum Project; WHO Regional Office for Europe: Copenhagen, Denmark, 2005; Available online: https://apps.who.int/iris/handle/10665/107638 (accessed on 25 June 2021).
- Padwal, R.; Campbell, N.R.C.; Schutte, A.E.; Olsen, M.H.; Delles, C.; Etyang, A.; Cruickshank, J.K.; Stergiou, G.; Rakotz, M.K.; Wozniak, G.; et al. Optimizing observer performance of clinic blood pressure measurement: A position statement from the Lancet Commission on Hypertension Group. J. Hypertens. 2019, 37, 1737–1745. [Google Scholar] [CrossRef]
- Kallioinen, N.; Hill, A.; Horswill, M.S.; Ward, H.E.; Watson, M.O. Sources of inaccuracy in the measurement of adult patients’ resting blood pressure in clinical settings: A systematic review. J. Hypertens. 2017, 35, 421–441. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. WHO Technical Specifications for Automated Non-Invasive Blood Pressure Measuring Devices with Cuff; World Health Organization (WHO): Geneva, Switzerland, 2020; Available online: https://apps.who.int/iris/handle/10665/331749 (accessed on 25 June 2021).
- ABDA—Bundesvereinigung Deutscher Apothekerverbände e.V.; Geschäftsbereich Arzneimittel. Blutdruckmessung in der Apotheke: Standardarbeitsanweisung (SOP). 2020. Available online: https://www.abda.de/fileadmin/user_upload/assets/Praktische_Hilfen/Leitlinien/Blutdruckmessung/SOP_Blutdruckmessung_in_der_Apotheke.pdf (accessed on 14 June 2021).
- Garrison, D.; Kanuka, H. Blended learning: Uncovering its transformative potential in higher education. Internet High Educ. 2004, 7, 95–105. [Google Scholar] [CrossRef]
- Hess, R.; Hagemeier, N.E.; Blackwelder, R.; Rose, D.; Ansari, N.; Branham, T. Teaching Communication Skills to Medical and Pharmacy Students Through a Blended Learning Course. Am. J. Pharm. Educ. 2016, 80, 64. [Google Scholar] [CrossRef] [Green Version]
- McCutcheon, K.; O’Halloran, P.; Lohan, M. Online learning versus blended learning of clinical supervisee skills with pre-registration nursing students: A randomised controlled trial. Int. J. Nurs. Stud. 2018, 82, 30–39. [Google Scholar] [CrossRef]
- Qutieshat, A.S.; Abusamak, M.O.; Maragha, T.N. Impact of Blended Learning on Dental Students’ Performance and Satisfaction in Clinical Education. J. Dent. Educ. 2020, 84, 135–142. [Google Scholar] [CrossRef]
- Makhdoom, N.; Khoshhal, K.I.; Algaidi, S.; Heissam, K.; Zolaly, M.A. ‘Blended learning’ as an effective teaching and learning strategy in clinical medicine: A comparative cross-sectional university-based study. J. Taibah Univ. Med. Sci 2013, 8, 12–17. [Google Scholar] [CrossRef] [Green Version]
- Viljoen, C.A.; Millar, R.S.; Manning, K.; Burch, V.C. Effectiveness of blended learning versus lectures alone on ECG analysis and interpretation by medical students. BMC Med. Educ. 2020, 20, 488. [Google Scholar] [CrossRef] [PubMed]
- Farahani, I.; Laeer, S.; Farahani, S.; Schwender, H.; Laven, A. Blended learning: Improving the diabetes mellitus counseling skills of German pharmacy students. Curr. Pharm. Teach. Learn. 2020, 12, 963–974. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; He, J.; Yuan, C.; Chen, B.; Sun, Z. The effects of blended learning on knowledge, skills, and satisfaction in nursing students: A meta-analysis. Nurse Educ. Today 2019, 82, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Berga, K.-A.; Vadnais, E.; Nelson, J.; Johnston, S.; Buro, K.; Hu, R.; Olaiya, B. Blended learning versus face-to-face learning in an undergraduate nursing health assessment course: A quasi-experimental study. Nurse Educ. Today 2021, 96, 104622. [Google Scholar] [CrossRef] [PubMed]
- Ghirardini, B. E-Learning Methodologies: A Guide for Designing and Developing E-Learning Courses; Food and Agriculture Organization of the United Nations: Rome, Italy, 2011; ISBN 9789251070970. [Google Scholar]
- Staker, H.C.; Horn, M.B. Classifying-K-12-Blended-Learning. Innosight Institute. 2012. Available online: https://www.christenseninstitute.org/wp-content/uploads/2013/04/Classifying-K-12-blended-learning.pdf (accessed on 7 June 2021).
- Hege, I.; Tolks, D.; Adler, M.; Härtl, A. Blended learning: Ten tips on how to implement it into a curriculum in healthcare education. GMS J. Med. Educ. 2020, 37, Doc45. [Google Scholar] [CrossRef]
- Le Roux, I.; Nagel, L. Seeking the best blend for deep learning in a flipped classroom—viewing student perceptions through the Community of Inquiry lens. Int. J. Educ. Technol. High. Educ. 2018, 15, 16. [Google Scholar] [CrossRef] [Green Version]
- Baker, J.W. The “Classroom Flip”: Using Web Course Management Tools to Become the Guide by the Side. In Proceedings of the 11th International Conference on College Teaching and Learning, Jacksonville, FL, USA, 12–15 April 2000. [Google Scholar]
- Lage, M.J.; Platt, G.J.; Treglia, M. Inverting the Classroom: A Gateway to Creating an Inclusive Learning Environment. J. Econ. Educ. 2000, 31, 30–43. [Google Scholar] [CrossRef]
- Bergmann, J.; Sams, A. Flip Your Classroom: Reach Every Student in Every Class. Every Day; ISTE: Washington, DC, USA, 2012; ISBN 9781564843159. [Google Scholar]
- Brame, C. Flipping the Classroom; Vanderbilt University Center for Teaching. 2013. Available online: https://cft.vanderbilt.edu/guides-sub-pages/flipping-the-classroom/ (accessed on 12 June 2021).
- Abeysekera, L.; Dawson, P. Motivation and cognitive load in the flipped classroom: Definition, rationale and a call for research. High. Educ. Res. Dev. 2015, 34, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Milman, N.B. The flipped classroom strategy: What is it and how can it best be used? Distance Learn. 2014, 11, 9–11. [Google Scholar]
- Bergmann, J.; Overmyer, J.; Wilie, B. The Flipped Class: What it is and What it is Not. Available online: https://kmtrosclair.files.wordpress.com/2015/06/the-flipped-class-myths-vs-reality-the-daily-riff-be-smarter-about-education.pdf (accessed on 25 June 2021).
- Jensen, J.L.; Kummer, T.A.; Godoy, P.D.D.M. Improvements from a Flipped Classroom May Simply Be the Fruits of Active Learning. CBE—Life Sci. Educ. 2015, 14, ar5. [Google Scholar] [CrossRef] [PubMed]
- Bishop, J.; Verleger, M. The Flipped Classroom: A Survey of the Research. In Proceedings of the ASEE Annual Conference & Exposition, Atlanta, Georgia, 23–26 June 2013. [Google Scholar]
- He, Y.; Lu, J.; Huang, H.; He, S.; Ma, N.; Sha, Z.; Sun, Y.; Li, X. The effects of flipped classrooms on undergraduate pharmaceutical marketing learning: A clustered randomized controlled study. PLoS ONE 2019, 14, e0214624. [Google Scholar] [CrossRef] [PubMed]
- Akçayır, G.; Akçayır, M. The flipped classroom: A review of its advantages and challenges. Comput. Educ. 2018, 126, 334–345. [Google Scholar] [CrossRef]
- Sharma, N.; Lau, C.S.; Doherty, I.; Harbutt, D. How we flipped the medical classroom. Med. Teach. 2015, 37, 327–330. [Google Scholar] [CrossRef] [PubMed]
- Giuliano, C.A.; Moser, L.R. Evaluation of a Flipped Drug Literature Evaluation Course. Am. J. Pharm. Educ. 2016, 80, 66. [Google Scholar] [CrossRef] [Green Version]
- Cotta, K.I.; Shah, S.; Almgren, M.M.; Macías-Moriarity, L.Z.; Mody, V. Effectiveness of flipped classroom instructional model in teaching pharmaceutical calculations. Curr. Pharm. Teach. Learn. 2016, 8, 646–653. [Google Scholar] [CrossRef]
- Smith, J.D. Student attitudes toward flipping the general chemistry classroom. Chem. Educ. Res. Pract. 2013, 14, 607–614. [Google Scholar] [CrossRef]
- Prescott, W.A.; Woodruff, A.; Prescott, G.M.; Albanese, N.; Bernhardi, C.; Doloresco, F. Introduction and Assessment of a Blended-Learning Model to Teach Patient Assessment in a Doctor of Pharmacy Program. Am. J. Pharm. Educ. 2016, 80, 176. [Google Scholar] [CrossRef]
- Bachur, C.K.; Bachur, J.A.; Da Candido, S.S.; Machado, J.P.; Daniel, A.C.Q.G.; da Silva e Silva, C.M.; Veiga, E.V. The use of active methodologies as teaching strategies of measuring blood pressure. O uso das metodologias ativas como estratégias de ensino da medida da pressão arterial. J. Hum. Growth Dev. 2020, 30, 443–450. [Google Scholar] [CrossRef]
- Gross, D.; Pietri, E.S.; Anderson, G.; Moyano-Camihort, K.; Graham, M.J. Increased Preclass Preparation Underlies Student Outcome Improvement in the Flipped Classroom. CBE Life Sci. Educ. 2015, 14, ar36. [Google Scholar] [CrossRef] [Green Version]
- Strelan, P.; Osborn, A.; Palmer, E. The flipped classroom: A meta-analysis of effects on student performance across disciplines and education levels. Educ. Res. Rev. 2020, 30, 100314. [Google Scholar] [CrossRef]
- Anderson, H.G.; Frazier, L.; Anderson, S.L.; Stanton, R.; Gillette, C.; Broedel-Zaugg, K.; Yingling, K. Comparison of Pharmaceutical Calculations Learning Outcomes Achieved Within a Traditional Lecture or Flipped Classroom Andragogy. Am. J. Pharm. Educ. 2017, 81, 70. [Google Scholar] [CrossRef]
- O’Flaherty, J.; Phillips, C. The use of flipped classrooms in higher education: A scoping review. Internet High. Educ. 2015, 25, 85–95. [Google Scholar] [CrossRef]
- Rawas, H.; Bano, N.; Alaidarous, S. Comparing the Effects of Individual Versus Group Face-to-Face Class Activities in Flipped Classroom on Student’s Test Performances. Health Prof. Educ. 2020, 6, 153–161. [Google Scholar] [CrossRef]
- Schwarzenberg, P.; Navon, J.; Nussbaum, M.; Pérez-Sanagustín, M.; Caballero, D. Learning experience assessment of flipped courses. J. Comput. High. Educ. 2018, 30, 237–258. [Google Scholar] [CrossRef]
- Eryilmaz, M.; Cigdemoglu, C. Individual flipped learning and cooperative flipped learning: Their effects on students’ performance, social, and computer anxiety. Interact. Learn. Environ. 2019, 27, 432–442. [Google Scholar] [CrossRef]
- Farahani, S.; Farahani, I.; Burckhardt, B.B.; Monser, K.; Laeer, S. The development of an educational video on blood pressure measurement for pharmacy students. Adv. Med. Educ. Pract. 2021, 12, 655–663. [Google Scholar] [CrossRef] [PubMed]
- Lyman, F.T. The Responsive Classroom Discussion: The Inclusion of All Students. In Mainstreaming Digest; Anderson, A.S., Ed.; College of Education, University of Maryland: College Park, MD, USA, 1981; pp. 109–113. [Google Scholar]
- Farahani, S.; Farahani, I.; Burckhardt, B.B.; Schwender, H.; Laeer, S. Self-Instruction Video Versus Face-to-Face Instruction of Pharmacy Students’ Skills in Blood Pressure Measurement. Pharmacy 2020, 8, 217. [Google Scholar] [CrossRef]
- ABDA—Bundesvereinigung Deutscher Apothekerverbände e.V.; Geschäftsbereich Arzneimittel. Blutdruckmessung in der Apotheke: Standardarbeitsanweisung (SOP) für die Apotheke. 2017. Available online: https://www.abda.de/fuer-apotheker/qualitaetssicherung/leitlinien/leitlinien-und-arbeitshilfen/ (accessed on 17 February 2019).
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E.; Collins, K.J.; Dennison Himmelfarb, C.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2018, 15, 2275–2279, corrected in J. Am. Coll. Cardiol. 2018, 71, e127–e248. [Google Scholar] [CrossRef]
- Microsoft Corporation. Microsoft Excel 2019 (for Windows); Microsoft Corporation: Redmond, WA, USA, 2019. [Google Scholar]
- OriginLab Corporation. OriginPro 2019; OriginLab Corporation: Northampton, MA, USA, 2019. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2019. [Google Scholar]
- Clynes, M.P.; Raftery, S.E.C. Feedback: An essential element of student learning in clinical practice. Nurse Educ. Pract. 2008, 8, 405–411. [Google Scholar] [CrossRef]
- Ende, J. Feedback in Clinical Medical Education. JAMA 1983, 250, 777–781. [Google Scholar] [CrossRef] [PubMed]
- Hardavella, G.; Aamli-Gaagnat, A.; Saad, N.; Rousalova, I.; Sreter, K.B. How to give and receive feedback effectively. Breathe 2017, 13, 327–333. [Google Scholar] [CrossRef] [PubMed]
- Hill, F. Feedback to enhance student learning: Facilitating interactive feedback on clinical skills. Int. J. Clin. Ski. 2007, 1, 21–24. [Google Scholar]
- Schüler, I.M.; Heinrich-Weltzien, R.; Eiselt, M. Effect of individual structured and qualified feedback on improving clinical performance of dental students in clinical courses-randomised controlled study. Eur J. Dent. Educ. 2018, 22, e458–e467. [Google Scholar] [CrossRef]
- van de Ridder, J.M.M.; Peters, C.M.M.; Stokking, K.M.; de Ru, J.A.; Ten Cate, O.T.J. Framing of feedback impacts student’s satisfaction, self-efficacy and performance. Adv. Health Sci. Educ. Theory Pract. 2015, 20, 803–816. [Google Scholar] [CrossRef]
- Gillette, C.; Rudolph, M.; Kimble, C.; Rockich-Winston, N.; Smith, L.; Broedel-Zaugg, K. A Meta-Analysis of Outcomes Comparing Flipped Classroom and Lecture. Am. J. Pharm. Educ. 2018, 82, 6898. [Google Scholar] [CrossRef]
- Han, E.; Klein, K.C. Pre-Class Learning Methods for Flipped Classrooms. Am. J. Pharm. Educ. 2019, 83, 6922. [Google Scholar] [CrossRef]
- Bassett, K.; Olbricht, G.R.; Shannon, K.B. Student Preclass Preparation by Both Reading the Textbook and Watching Videos Online Improves Exam Performance in a Partially Flipped Course. CBE Life Sci. Educ. 2020, 19, ar32. [Google Scholar] [CrossRef]
- Tune, J.D.; Sturek, M.; Basile, D.P. Flipped classroom model improves graduate student performance in cardiovascular, respiratory, and renal physiology. Adv. Physiol. Educ. 2013, 37, 316–320. [Google Scholar] [CrossRef] [Green Version]
- Hew, K.F.; Lo, C.K. Flipped classroom improves student learning in health professions education: A meta-analysis. BMC Med. Educ. 2018, 18, 38. [Google Scholar] [CrossRef] [Green Version]
- Liu, K.J.; Tkachenko, E.; Waldman, A.; Boskovski, M.T.; Hartman, R.I.; Levin, A.A.; Nguyen, B.M.; Ruiz, E.S.; Sharon, V.R.; Sowerby, L.; et al. A video-based, flipped classroom, simulation curriculum for dermatologic surgery: A prospective, multi-institution study. J. Am. Acad. Dermatol. 2019, 81, 1271–1276. [Google Scholar] [CrossRef]
- Gloudeman, M.W.; Shah-Manek, B.; Wong, T.H.; Vo, C.; Ip, E.J. Use of condensed videos in a flipped classroom for pharmaceutical calculations: Student perceptions and academic performance. Curr. Pharm. Teach. Learn. 2018, 10, 206–210. [Google Scholar] [CrossRef] [PubMed]
- Wong, T.H.; Ip, E.J.; Lopes, I.; Rajagopalan, V. Pharmacy students’ performance and perceptions in a flipped teaching pilot on cardiac arrhythmias. Am. J. Pharm. Educ. 2014, 78, 185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hotle, S.L.; Garrow, L.A. Effects of the Traditional and Flipped Classrooms on Undergraduate Student Opinions and Success. J. Prof. Issues Eng. Educ. Pract. 2016, 142, 5015005. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Group A (Brief In-Class Session) (n = 18) | Group B (Extended In-Class Session) (n = 21) | |
|---|---|---|
| OSCE 1 | ||
| 1.1 Age in years a | ||
| Median (IQR) | 24 (4) | 23 (3) |
| Mean (SD) | 25.72 (4.53) | 24.4 (3.19) |
| 1.2. Gender | ||
| Female, n (%) | 12 (66.67) | 16 (76.19) |
| Male, n (%) | 6 (33.33) | 5 (23.81) |
| 1.3. Training as a pharmaceutical technical assistant | ||
| Yes, n (%) | 3 (16.67) | 2 (9.52) |
| No, n (%) | 15 (83.33) | 19 (90.48) |
| 1.4. Currently or formerly worked in a community pharmacy b | ||
| Yes, n (%) | 8 (44.44) | 4 (19.05) |
| No, n (%) | 10 (55.56) | 17 (80.95) |
| 1.5. Have measured BP by myself for the first time in my life | ||
| Yes, n (%) | 3 (16.67) | 6 (28.57) |
| No, n (%) | 15 (83.33) | 15 (71.43) |
| 1.6. If answered item 1.5 with no: What kind of blood pressure measurement device/s have you already used to measure the BP? c | ||
| Upper arm blood pressure monitor | 11 (73.33) | 13 (92.86) |
| Wrist blood pressure monitor | 10 (66.67) | 8 (57.14) |
| Blood pressure measurement device with stethoscope | 5 (33.33) | 3 (21.43) |
| 1.7. Preparation for BP measurement task d | ||
| Yes, n (%) | 0 (0) | 0 (0) |
| No, n (%) | 18 (100) | 20 (100) |
| OSCE 2 | ||
| 2.1. Preparation for BP measurement task | ||
| Yes, n (%) | 18 (100) | 21 (100) |
| No, n (%) | 0 (0) | 0 (0) |
| 2.2. If item 2.1 was answered yes: Did you prepare yourself with the self-instruction video from the university’s video platform? | ||
| Yes, n (%) | 18 (100) | 21 (100) |
| No, n (%) | 0 (0) | 0 (0) |
| 2.3. If item 2.1 was answered yes: Did you use other materials for preparation in addition to the video? e | ||
| Yes, n (%) | 0 (0) | 0 (0) |
| No, n (%) | 18 (100) | 21 (100) |
| OSCE 3 | ||
| 3.1. Preparation for BP measurement task f | ||
| Yes, n (%) | 15 (83.33) | 19 (90.48) |
| No, n (%) | 3 (16.67) | 2 (9.52) |
| 3.2. If item 3.1 was answered yes: Did you prepare yourself with the self-instruction video from the university’s video platform? | ||
| Yes, n (%) | 15 (100) | 18 (94.74) |
| No, n (%) | 0 (0) | 1 (5.26) |
| 3.3. If item 3.1 was answered yes: Did you use other materials for preparation in addition to the video? e,g | ||
| Yes, n (%) | 0 (0) | 0 (0) |
| No, n (%) | 15 (100) | 19 (100) |
| Instrument | Group | Change in Score between A1 and A2 in Points | p-Value a | Change in Score between A2 and A3 in Points | p-Value b | ||
|---|---|---|---|---|---|---|---|
| Mean (SD) | Median (IQR) | Mean (SD) | Median (IQR) | ||||
| OSCE checklist | Group A (n = 18) | 16.89 (3.88) | 16.5 (5) | 0.213 | 4.39 (5.74) | 2 (7) | 0.202 |
| Group B (n = 21) | 18.33 (4.27) | 19 (5) | 5.24 (4.07) | 5 (6) | |||
| Self-assessment survey | Group A (n = 18) | 3.56 (4.93) | 3 (6) | 0.178 | 1.44 (2.64) | 1 (4) | 0.113 |
| Group B (n = 21) | 4.29 (3.26) | 5 (3) | 2.62 (2.50) | 2 (3) | |||
| Proportion of Responses, n (%) | ||||||
|---|---|---|---|---|---|---|
| Strongly Disagree | Disagree | Rather Disagree | Rather Agree | Agree | Strongly Agree | |
| I found the seminar series on BP measurement interesting. | ||||||
| Group A; n = 21 | 0 (0) | 1 (4.76) | 2 (9.52) | 6 (28.57) | 7 (33.33) | 5 (23.81) |
| Group B; n = 16 | 0 (0) | 0 (0) | 2 (12.5) | 5 (31.25) | 6 (37.5) | 3 (18.75) |
| During the OSCEs/simulations, I was able to determine my strengths and weaknesses in BP measurement. | ||||||
| Group A; n = 21 | 0 (0) | 0 (0) | 1 (4.76) | 3 (14.29) | 6 (28.57) | 11 (52.38) |
| Group B; n = 16 | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 9 (56.25) | 7 (43.75) |
| The OSCEs/simulations enabled me to apply the knowledge and skills I gained during the instruction video and the in-class phase. | ||||||
| Group A; n = 21 | 0 (0) | 0 (0) | 0 (0) | 2 (9.52) | 13 (61.90) | 6 (28.57) |
| Group B; n = 16 | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 10 (62.5) | 6 (37.5) |
| After this seminar series, I feel better prepared for the correct BP measurement in the community pharmacy on real patients. | ||||||
| Group A; n = 21 | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 11 (52.38) | 10 (47.62) |
| Group B; n = 16 | 0 (0) | 0 (0) | 0 (0) | 3 (18.75) | 5 (31.25) | 8 (50) |
| The instruction video was helpful in conveying knowledge about measuring BP. | ||||||
| Group A; n = 21 | 0 (0) | 0 (0) | 1 (4.76) | 3 (14.29) | 8 (38.10) | 9 (42.86) |
| Group B; n = 16 | 0 (0) | 0 (0) | 0 (0) | 2 (12.5) | 7 (43.75) | 7 (43.75) |
| The instruction video was helpful in improving my practical BP measurement skills. | ||||||
| Group A; n = 21 | 0 (0) | 0 (0) | 0 (0) | 6 (28.57) | 5 (23.81) | 10 (47.62) |
| Group B; n = 16 | 0 (0) | 0 (0) | 0 (0) | 4 (25) | 6 (37.5) | 6 (37.5) |
| I had technical problems accessing or playing the instruction video. | ||||||
| Group A; n = 20 | 17 (85) | 1 (5) | 0 (0) | 1 (5) | 1 (5) | 0 (0) |
| Group B; n = 16 | 14 (87.5) | 2 (12.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| The in-class phase was helpful to improve my understanding of BP measurement. | ||||||
| Group A; n = 20 | 0 (0) | 0 (0) | 1 (5) | 3 (15) | 10 (50) | 6 (30) |
| Group B; n = 16 | 0 (0) | 2 (12.5) | 1 (6.25) | 5 (31.25) | 6 (37.5) | 2 (12.5) |
| The in-class phase was helpful in improving my practical BP measurement skills. | ||||||
| Group A; n = 21 | 0 (0) | 0 (0) | 1 (4.76) | 3 (14.29) | 8 (38.10) | 9 (42.86) |
| Group B; n = 16 | 0 (0) | 3 (18.75) | 1 (6.25) | 3 (18.75) | 6 (37.5) | 3 (18.75) |
| I prefer the instruction video on its own to train the competence of BP measurement. | ||||||
| Group A; n = 21 | 3 (14.29) | 6 (28.57) | 4 (19.05) | 4 (19.05) | 2 (9.52) | 2 (9.52) |
| Group B; n = 16 | 1 (6.25) | 2 (12.5) | 6 (37.5) | 2 (12.5) | 3 (18.75) | 2 (12.5) |
| I prefer the active in-class phase on its own to train the competence of BP measurement. | ||||||
| Group A; n = 21 | 3 (14.29) | 6 (28.57) | 4 (19.05) | 6 (28.57) | 2 (9.52) | 0 (0) |
| Group B; n = 16 | 2 (12.5) | 4 (25) | 6 (37.5) | 3 (18.75) | 1 (6.25) | 0 (0) |
| I prefer the combination of instruction video with the active in-class phase undertaken in this study to train the competence of measuring BP. | ||||||
| Group A; n = 21 | 0 (0) | 1 (4.76) | 2 (9.52) | 3 (14.29) | 10 (47.62) | 5 (23.81) |
| Group B; n = 16 | 0 (0) | 1 (6.25) | 1 (6.25) | 5 (31.25) | 4 (25) | 5 (31.25) |
| In the future, instruction videos should be included in pharmacy teaching. | ||||||
| Group A; n = 21 | 0 (0) | 1 (4.76) | 1 (4.76) | 2 (9.52) | 9 (42.86) | 8 (38.10) |
| Group B; n = 16 | 0 (0) | 0 (0) | 0 (0) | 2 (12.5) | 9 (56.25) | 5 (31.25) |
| OSCEs/simulations about BP measurement are superfluous because one can do nothing wrong with the BP measurement. | ||||||
| Group A; n = 21 | 13 (61.90) | 5 (23.81) | 3 (14.29) | 0 (0) | 0 (0) | 0 (0) |
| Group B; n = 16 | 13 (81.25) | 3 (18.75) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| In the future, OSCEs/simulations should be included as a regular part of the clinical pharmacy course to train practical skills (such as BP measurement). | ||||||
| Group A; n = 21 | 0 (0) | 1 (4.76) | 1 (4.76) | 4 (19.05) | 11 (52.38) | 4 (19.05) |
| Group B; n = 16 | 0 (0) | 0 (0) | 0 (0) | 5 (31.25) | 4 (25) | 7 (43.75) |
| In the future, the “flipped classroom model” should be included in pharmacy teaching. | ||||||
| Group A; n = 21 | 1 (4.76) | 2 (9.52) | 3 (14.29) | 9 (42.86) | 5 (23.81) | 1 (4.76) |
| Group B; n = 15 | 0 (0) | 0 (0) | 3 (20) | 5 (33.33) | 4 (26.67) | 3 (20) |
| Free-Text Item | Group | Topics |
|---|---|---|
| What did you particularly like about the series of seminars in the “flipped classroom model”? | Group A (brief in-class session) |
|
| ||
| ||
| Group B (extended in-class session) |
| |
| ||
| ||
| I would change the following on the on the seminar series in the format of “flipped classroom model” | Group A (brief in-class session |
|
| ||
| ||
| Group B (extended in-class session) |
| |
| ||
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Farahani, S.; Farahani, I.; Deters, M.A.; Schwender, H.; Burckhardt, B.B.; Laeer, S. Blended Learning on Blood Pressure Measurement: Investigating Two In-Class Strategies in a Flipped Classroom-Like Setting to Teach Pharmacy Students Blood Pressure Measurement Skills. Healthcare 2021, 9, 822. https://doi.org/10.3390/healthcare9070822
Farahani S, Farahani I, Deters MA, Schwender H, Burckhardt BB, Laeer S. Blended Learning on Blood Pressure Measurement: Investigating Two In-Class Strategies in a Flipped Classroom-Like Setting to Teach Pharmacy Students Blood Pressure Measurement Skills. Healthcare. 2021; 9(7):822. https://doi.org/10.3390/healthcare9070822
Chicago/Turabian StyleFarahani, Samieh, Imaneh Farahani, Maira Anna Deters, Holger Schwender, Bjoern Bengt Burckhardt, and Stephanie Laeer. 2021. "Blended Learning on Blood Pressure Measurement: Investigating Two In-Class Strategies in a Flipped Classroom-Like Setting to Teach Pharmacy Students Blood Pressure Measurement Skills" Healthcare 9, no. 7: 822. https://doi.org/10.3390/healthcare9070822
APA StyleFarahani, S., Farahani, I., Deters, M. A., Schwender, H., Burckhardt, B. B., & Laeer, S. (2021). Blended Learning on Blood Pressure Measurement: Investigating Two In-Class Strategies in a Flipped Classroom-Like Setting to Teach Pharmacy Students Blood Pressure Measurement Skills. Healthcare, 9(7), 822. https://doi.org/10.3390/healthcare9070822