
Familial and Parental Predictors of Physical Activity in Late Adolescence: Prospective Analysis over a Two-Year Period

 ,
, 
 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Design and Participants
2.2. Instruments
2.3. Procedures
2.4. Data Analysis
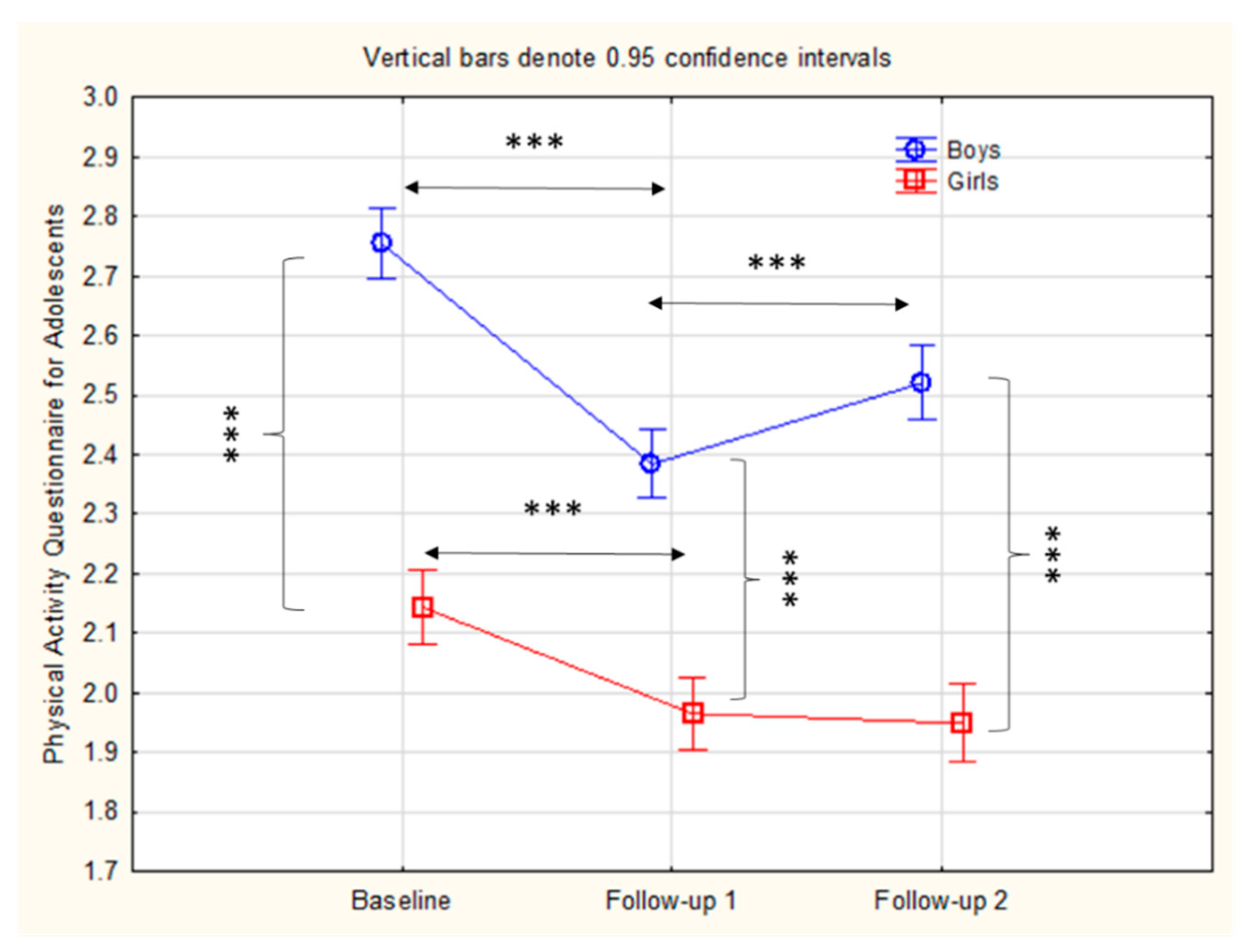
3. Results
4. Discussion
4.1. Gender and Changes in PALs
4.2. Parental Education and PALs
4.3. Parental Conflict and PALs
4.4. Limitations and Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Action Plan on Physical Activity 2018–2030: More Active People for a Healthier World; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Global trends in insufficient physical activity among adolescents: A pooled analysis of 298 population-based surveys with 1.6 million participants. Lancet Child Adolesc. Health 2020, 4, 23–35. [Google Scholar] [CrossRef]
- Maric, D.; Kvesic, I.; Lujan, I.K.; Bianco, A.; Zenic, N.; Separovic, V.; Terzic, A.; Versic, S.; Sekulic, D. Parental and Familial Factors Influencing Physical Activity Levels in Early Adolescence: A Prospective Study. Healthcare 2020, 8, 532. [Google Scholar] [CrossRef] [PubMed]
- Miljanovic Damjanovic, V.; Obradovic Salcin, L.; Zenic, N.; Foretic, N.; Liposek, S. Identifying Predictors of changes in physical activity level in adolescence: A prospective analysis in Bosnia and Herzegovina. Int. J. Environ. Res. Public Health 2019, 16, 2573. [Google Scholar] [CrossRef] [PubMed]
- Sekulic, D.; Rodek, J.; Sattler, T. Factors associated with physical activity levels in late adolescence: A prospective study. Med. Pr. 2020, 71, 637–647. [Google Scholar] [CrossRef] [PubMed]
- Štefan, L.; Sorić, M.; Devrnja, A.; Petrić, V.; Mišigoj-Duraković, M. One-year changes in physical activity and sedentary behavior among adolescents: The Croatian Physical Activity in Adolescence Longitudinal Study (CRO-PALS). Int. J. Adolesc. Med. Health 2018, 32. [Google Scholar] [CrossRef]
- Alotaibi, T.; Almuhanna, R.; Alhassan, J.; Alqadhib, E.; Mortada, E.; Alwhaibi, R. The relationship between technology use and physical activity among typically-developing children. Healthcare 2020, 8, 488. [Google Scholar] [CrossRef] [PubMed]
- Faigenbaum, A.D.; Rebullido, T.R.; Chulvi-Medrano, I. Youth physical activity is all about the “F-Words”. Strength Cond. J. 2020, 42, 2–6. [Google Scholar] [CrossRef]
- Trost, S.G.; Loprinzi, P.D. Parental influences on physical activity behavior in children and adolescents: A brief review. Am. J. Lifestyle Med. 2011, 5, 171–181. [Google Scholar] [CrossRef]
- Park, H.; Kim, N. Predicting factors of physical activity in adolescents: A systematic review. Asian Nurs. Res. 2008, 2, 113–128. [Google Scholar] [CrossRef]
- Hallal, P.C.; Victora, C.G.; Azevedo, M.R.; Wells, J.C. Adolescent physical activity and health: A systematic review. Sports Med. 2006, 36, 1019–1030. [Google Scholar] [CrossRef]
- Sallis, J.F.; Prochaska, J.J.; Taylor, W.C. A review of correlates of physical activity of children and adolescents. Med. Sci. Sports Exerc. 2000, 32, 963–975. [Google Scholar] [CrossRef] [PubMed]
- Koçak, S.; Harris, M.B.; Işler, A.K.; Çiçek, Ş. Physical activity level, sport participation, and parental education level in Turkish junior high school students. Pediatr. Exerc. Sci. 2002, 14, 147–154. [Google Scholar] [CrossRef]
- Patnode, C.D.; Lytle, L.A.; Erickson, D.J.; Sirard, J.R.; Barr-Anderson, D.; Story, M. The relative influence of demographic, individual, social, and environmental factors on physical activity among boys and girls. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 79. [Google Scholar] [CrossRef] [PubMed]
- Ornelas, I.J.; Perreira, K.M.; Ayala, G.X. Parental influences on adolescent physical activity: A longitudinal study. Int. J. Behav. Nutr. Phys. Act. 2007, 4, 3. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Trost, S.G.; Sallis, J.F.; Pate, R.R.; Freedson, P.S.; Taylor, W.C.; Dowda, M. Evaluating a model of parental influence on youth physical activity. Am. J. Prev. Med. 2003, 25, 277–282. [Google Scholar] [CrossRef]
- Beets, M.W.; Cardinal, B.J.; Alderman, B.L. Parental social support and the physical activity-related behaviors of youth: A review. Health Educ. Behav. 2010, 37, 621–644. [Google Scholar] [CrossRef]
- Brustad, R.J. Who will go out and play? Parental and psychological influences on children’s attraction to physical activity. Pediatr. Exerc. Sci. 1993, 5, 210–223. [Google Scholar] [CrossRef]
- Kohl, H.W.; Hobbs, K.E. Development of physical activity behaviors among children and adolescents. Pediatrics 1998, 101, 549–554. [Google Scholar]
- Goldscheider, F.; Thornton, A.; Young-DeMarco, L. A portrait of the nest-leaving process in early adulthood. Demography 1993, 30, 683–699. [Google Scholar] [CrossRef]
- Office of the Surgeon General (US); Office of Disease Prevention and Health Promotion (US); Centers for Disease Control and Prevention (US); National Institutes of Health (US). The Surgeon General’s Call to Action to Prevent and Decrease Overweight and Obesity; US Government Printing Office: Washington, DC, USA, 2001.
- Mattoo, K.; Shubayr, M.; Moaleem, M.A.; Halboub, E. Influence of parental physical activity and screen time on the BMI of adult offspring in a Saudi population. Healthcare 2020, 8, 110. [Google Scholar] [CrossRef]
- Gustafson, S.L.; Rhodes, R.E. Parental correlates of physical activity in children and early adolescents. Sports Med. 2006, 36, 79–97. [Google Scholar] [CrossRef] [PubMed]
- Jaeschke, L.; Steinbrecher, A.; Luzak, A.; Puggina, A.; Aleksovska, K.; Buck, C.; Burns, C.; Cardon, G.; Carlin, A.; Chantal, S.; et al. Socio-cultural determinants of physical activity across the life course: A ‘Determinants of Diet and Physical Activity’ (DEDIPAC) umbrella systematic literature review. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 173. [Google Scholar] [CrossRef] [PubMed]
- Lau, R.R.; Quadrel, M.J.; Hartman, K.A. Development and change of young adults’ preventive health beliefs and behavior: Influence from parents and peers. J. Health Soc. Behav. 1990, 31, 240–259. [Google Scholar] [CrossRef] [PubMed]
- Sallis, J.F.; Prochaska, J.J.; Taylor, W.C.; Hill, J.O.; Geraci, J.C. Correlates of physical activity in a national sample of girls and boys in grades 4 through 12. Health Psychol. 1999, 18, 410–415. [Google Scholar] [CrossRef] [PubMed]
- Sekulic, D.; Sisic, N.; Terzic, A.; Jasarevic, I.; Ostojic, L.; Pojskic, H.; Zenic, N. Sport and scholastic factors in relation to smoking and smoking initiation in older adolescents: A prospective cohort study in Bosnia and Herzegovina. BMJ Open 2017, 7, e014066. [Google Scholar] [CrossRef]
- Sasayama, K.; Adachi, M. Tracking of objective physical activity and physical fitness in Japanese children. BMC Res. Notes 2019, 12, 252. [Google Scholar] [CrossRef]
- Wyszyńska, J.; Matłosz, P.; Podgórska-Bednarz, J.; Herbert, J.; Przednowek, K.; Baran, J.; Dereń, K.; Mazur, A. Adaptation and validation of the Physical Activity Questionnaire for Adolescents (PAQ-A) among Polish adolescents: Cross-sectional study. BMJ Open 2019, 9, e030567. [Google Scholar] [CrossRef]
- Zubak, Z.; Zenic, N.; Ostojic, L.; Zubak, I.; Pojskic, H. A prospective study on the influence of scholastic factors on the prevalence and initiation of illicit drug misuse in adolescence. Int. J. Environ. Res. Public Health 2018, 15, 874. [Google Scholar] [CrossRef]
- Eime, R.M.; Casey, M.M.; Harvey, J.T.; Sawyer, N.A.; Symons, C.M.; Payne, W.R. Socioecological factors potentially associated with participation in physical activity and sport: A longitudinal study of adolescent girls. J. Sci. Med. Sport 2015, 18, 684–690. [Google Scholar] [CrossRef]
- Wheeler, S. The significance of family culture for sports participation. Int. Rev. Sociol. Sport 2012, 47, 235–252. [Google Scholar] [CrossRef]
- Sajber, D.; Tahiraj, E.; Zenic, N.; Peric, M.; Sekulic, D. Alcohol drinking among kosovar adolescents: An examination of gender-Specific sociodemographic, sport and familial factors associated with harmful drinking. Subst. Use Misuse 2016, 51, 533–539. [Google Scholar] [CrossRef] [PubMed]
- Zenic, N.; Ban, D.; Jurisic, S.; Cubela, M.; Rodek, J.; Ostojic, L.; Jelicic, M.; Bianco, A.; Sekulic, D. Prospective analysis of the influence of sport and educational factors on the prevalence and initiation of smoking in older adolescents from Croatia. Int. J. Environ. Res. Public Health 2017, 14, 446. [Google Scholar] [CrossRef] [PubMed]
- Tahiraj, E.; Cubela, M.; Ostojic, L.; Rodek, J.; Zenic, N.; Sekulic, D.; Lesnik, B. Prevalence and factors associated with substance use and misuse among Kosovar adolescents; cross sectional study of scholastic, familial- and sports-related factors of influence. Int. J. Environ. Res. Public Health 2016, 13, 502. [Google Scholar] [CrossRef] [PubMed]
- Bjelica, D.; Idrizovic, K.; Popovic, S.; Sisic, N.; Sekulic, D.; Ostojic, L.; Spasic, M.; Zenic, N. An examination of the ethnicity-specific prevalence of and factors associated with substance use and misuse: Cross-sectional analysis of Croatian and Bosniak adolescents in Bosnia and Herzegovina. Int. J. Environ. Res. Public Health 2016, 13, 968. [Google Scholar] [CrossRef]
- Trost, S.G.; Pate, R.R.; Sallis, J.F.; Freedson, P.S.; Taylor, W.C.; Dowda, M.; Sirard, J. Age and gender differences in objectively measured physical activity in youth. Med. Sci. Sports Exerc. 2002, 34, 350–355. [Google Scholar] [CrossRef]
- WHO. Physical Activity. Available online: https://www.who.int/news-room/fact-sheets/detail/physical-activity (accessed on 17 August 2020).
- Archer, J.; McDonald, M. Gender roles and sports in adolescent girls. Leis. Stud. 1990, 9, 225–240. [Google Scholar] [CrossRef]
- Sallis, J.F.; Patterson, T.L.; Buono, M.J.; Atkins, C.J.; Nader, P.R. Aggregation of physical activity habits in Mexican-American and Anglo families. J. Behav. Med. 1988, 11, 31–41. [Google Scholar] [CrossRef]
- Eime, R.M.; Harvey, J.T.; Sawyer, N.A.; Craike, M.J.; Symons, C.M.; Payne, W.R. Changes in sport and physical activity participation for adolescent females: A longitudinal study. BMC Public Health 2016, 16, 533. [Google Scholar] [CrossRef]
- Raudsepp, L. The relationship between socio-economic status, parental support and adolescent physical activity. Acta Paediatr. 2006, 95, 93–98. [Google Scholar] [CrossRef]
- Vilhjalmsson, R.; Kristjansdottir, G. Gender differences in physical activity in older children and adolescents: The central role of organized sport. Soc. Sci. Med. 2003, 56, 363–374. [Google Scholar] [CrossRef]
- Casey, M.M.; Eime, R.M.; Payne, W.R.; Harvey, J.T. Using a socioecological approach to examine participation in sport and physical activity among rural adolescent girls. Qual. Health Res. 2009, 19, 881–893. [Google Scholar] [CrossRef]
- Finkenberg, M. Sex and ethnicity as factors for participation in physical activity. Int. J. Phys. Educ. 1991, 28, 23–26. [Google Scholar]
- Lantz, C.D.; Schroeder, P.J. Endorsement of masculine and feminine gender roles: Differences between participation in and…. J. Sport Behav. 1999, 22, 545. [Google Scholar]
- Telford, R.M.; Telford, R.D.; Olive, L.S.; Cochrane, T.; Davey, R. Why are girls less physically active than boys? Findings from the LOOK longitudinal study. PLoS ONE 2016, 11, e0150041. [Google Scholar] [CrossRef] [PubMed]
- Park, E.; Park, H.R.; Choi, E.S. Barriers to and facilitators of physical activity among korean female adults with knee osteoarthritis and comorbidity: A qualitative study. Healthcare 2020, 8, 226. [Google Scholar] [CrossRef]
- Dowda, M.; Dishman, R.K.; Pfeiffer, K.A.; Pate, R.R. Family support for physical activity in girls from 8th to 12th grade in South Carolina. Prev. Med. 2007, 44, 153–159. [Google Scholar] [CrossRef]
- Greendorfer, S.L.; Lewko, J.H. Role of family members in sport socialization of children. Res. Q. Am. Alliance Health Phy. Educ. Recreat. 1978, 49, 146–152. [Google Scholar] [CrossRef]
- Rossow, I.; Rise, J. Concordance of parental and adolescent health behaviors. Soc. Sci. Med. 1994, 38, 1299–1305. [Google Scholar] [CrossRef]
- Martin, L.; Bruner, M.; Eys, M.; Spink, K. The social environment in sport: Selected topics. Int. Rev. Sport Exerc. Psychol. 2014, 7, 87–105. [Google Scholar] [CrossRef]
- Larson, R.; Richards, M.H. Daily companionship in late childhood and early adolescence: Changing developmental contexts. Child. Dev. 1991, 62, 284–300. [Google Scholar] [CrossRef]
- Larson, R.W.; Richards, M.H.; Moneta, G.; Holmbeck, G.; Duckett, E. Changes in adolescents’ daily interactions with their families from ages 10 to 18: Disengagement and transformation. Dev. Psychol. 1996, 32, 744. [Google Scholar] [CrossRef]
- Blakemore, S.-J.; Mills, K.L. Is adolescence a sensitive period for sociocultural processing? Annu. Rev. Psychol. 2014, 65, 187–207. [Google Scholar] [CrossRef] [PubMed]
- Bauman, A.; Phongsavan, P. Epidemiology of substance use in adolescence: Prevalence, trends and policy implications. Drug Alcohol Depend. 1999, 55, 187–207. [Google Scholar] [CrossRef]
- Wing, E.K.; Belanger, M.; Brunet, J. Linking parental influences and youth participation in physical activity in- and out-of-school: The mediating role of self-efficacy and enjoyment. Am. J. Health Behav. 2016, 40, 31–37. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Main Effects | Interaction | ||||
|---|---|---|---|---|---|---|
| Gender | Measurement | Gender × Measurement | ||||
| F-test | p-level | F-test | p | F-test | p-level | |
| PAQ-A | 94.17 | 0.001 | 83.05 | 0.001 | 6.61 | 0.001 |
| Variables | PAL Baseline | PAL Follow-Up 1 | PAL Follow-Up 2 | |||
|---|---|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | OR | 95% CI | |
| Socioeconomic status | 0.79 | 0.44–1.41 | 0.89 | 0.48–1.67 | 0.65 | 0.35–1.21 |
| Paternal education | 1.42 | 1.17–1.84 | 1.16 | 0.98–1.49 | 1.23 | 0.97–1.56 |
| Maternal education | 1.16 | 0.95–1.43 | 1.18 | 0.88–1.41 | 0.90 | 0.71–1.13 |
| Parental/familial conflict | 0.72 | 0.58–0.88 | 0.83 | 0.63–0.98 | 0.75 | 0.60–0.94 |
| Parental absence | 1.13 | 0.97–1.32 | 1.06 | 0.88–1.28 | 1.14 | 0.96–1.36 |
| Parental care | 0.80 | 0.62–1.04 | 1.09 | 0.81–1.47 | 1.01 | 0.76–1.33 |
| Parental questioning | 1.16 | 0.93–1.44 | 1.09 | 0.87–1.38 | 1.20 | 0.98–1.47 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sekulic, D.; Maric, D.; Versic, S.; Zevrnja, A.; Terzic, A.; Zenic, N. Familial and Parental Predictors of Physical Activity in Late Adolescence: Prospective Analysis over a Two-Year Period. Healthcare 2021, 9, 132. https://doi.org/10.3390/healthcare9020132
Sekulic D, Maric D, Versic S, Zevrnja A, Terzic A, Zenic N. Familial and Parental Predictors of Physical Activity in Late Adolescence: Prospective Analysis over a Two-Year Period. Healthcare. 2021; 9(2):132. https://doi.org/10.3390/healthcare9020132
Chicago/Turabian StyleSekulic, Damir, Dora Maric, Sime Versic, Ante Zevrnja, Admir Terzic, and Natasa Zenic. 2021. "Familial and Parental Predictors of Physical Activity in Late Adolescence: Prospective Analysis over a Two-Year Period" Healthcare 9, no. 2: 132. https://doi.org/10.3390/healthcare9020132
APA StyleSekulic, D., Maric, D., Versic, S., Zevrnja, A., Terzic, A., & Zenic, N. (2021). Familial and Parental Predictors of Physical Activity in Late Adolescence: Prospective Analysis over a Two-Year Period. Healthcare, 9(2), 132. https://doi.org/10.3390/healthcare9020132