
Psychological Effects of Motivational Aquatic Resistance Interval Training and Nutritional Education in Older Women

 ,
, 

Abstract
1. Introduction
2. Materials and Methods
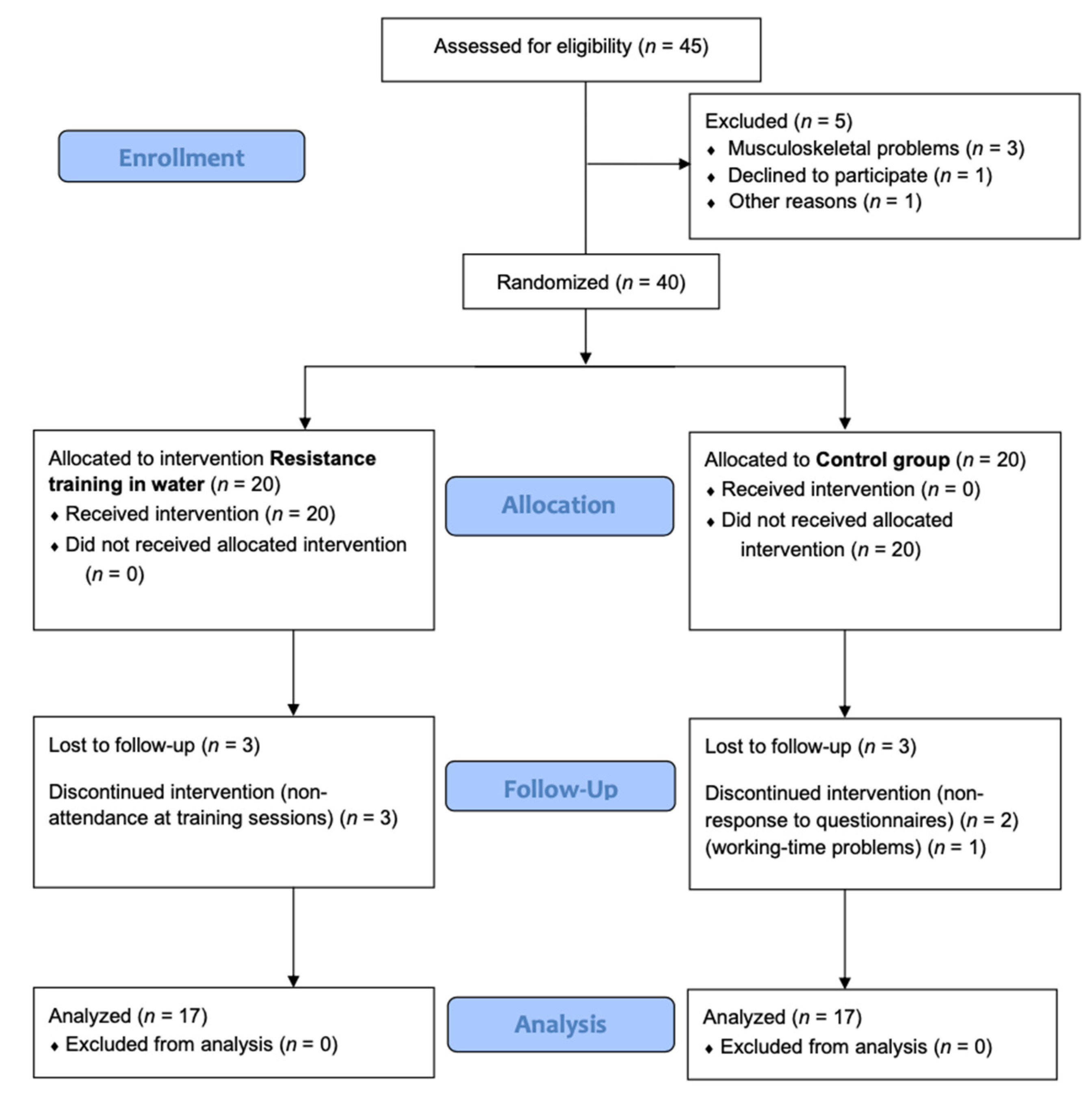
2.1. Design
2.2. Participants
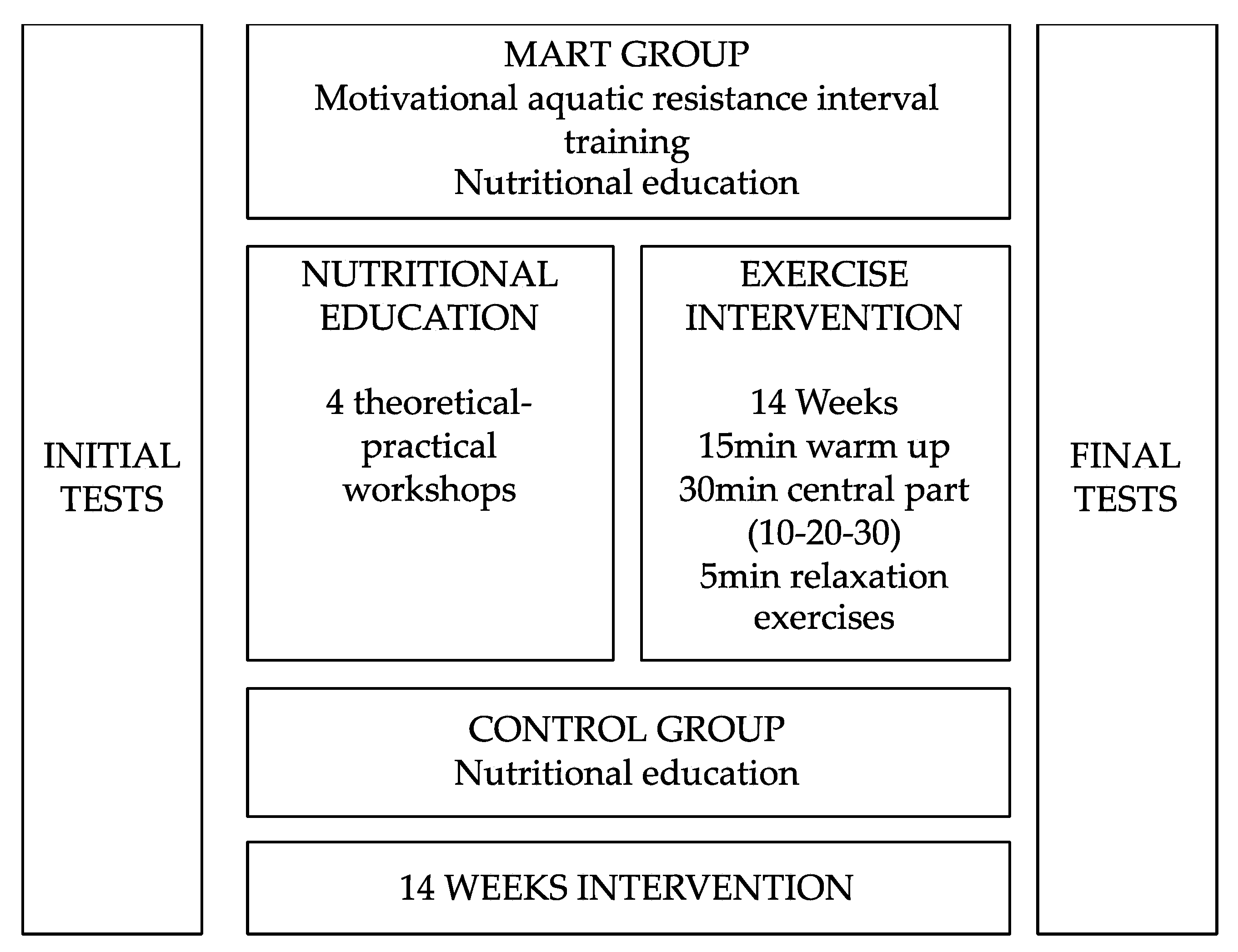
2.3. Intervention
- Educate older adults about the benefit of aquatic resistance training program;
- Explain the purpose of the aquatic resistance training program;
- 3.
- Encourage the perception of competence by the participant;
- 4.
- Establish moderately difficult objectives adapted to the biological individuality of each participant;
- 5.
- Take into account the information provided by the practitioner during aquatic resistance training program;
- 6.
- Convey an adequate task environment;
- 7.
- Encourage the participants by emphasizing that the activity can be improved through practice;
- 8.
- Offer clear feedbacks;
- 9.
- Encourage the relationship between participants;
- 10.
- Have the participants enjoy the activities in aquatic resistance training program.
2.4. Outcomes
2.4.1. Perception of Autonomy Support
2.4.2. Psychological Needs
2.4.3. Intrinsic Motivation to Exercise
2.4.4. Perception of Physical Activity
2.4.5. Anthropometric Measurements
2.5. Statistical Analysis
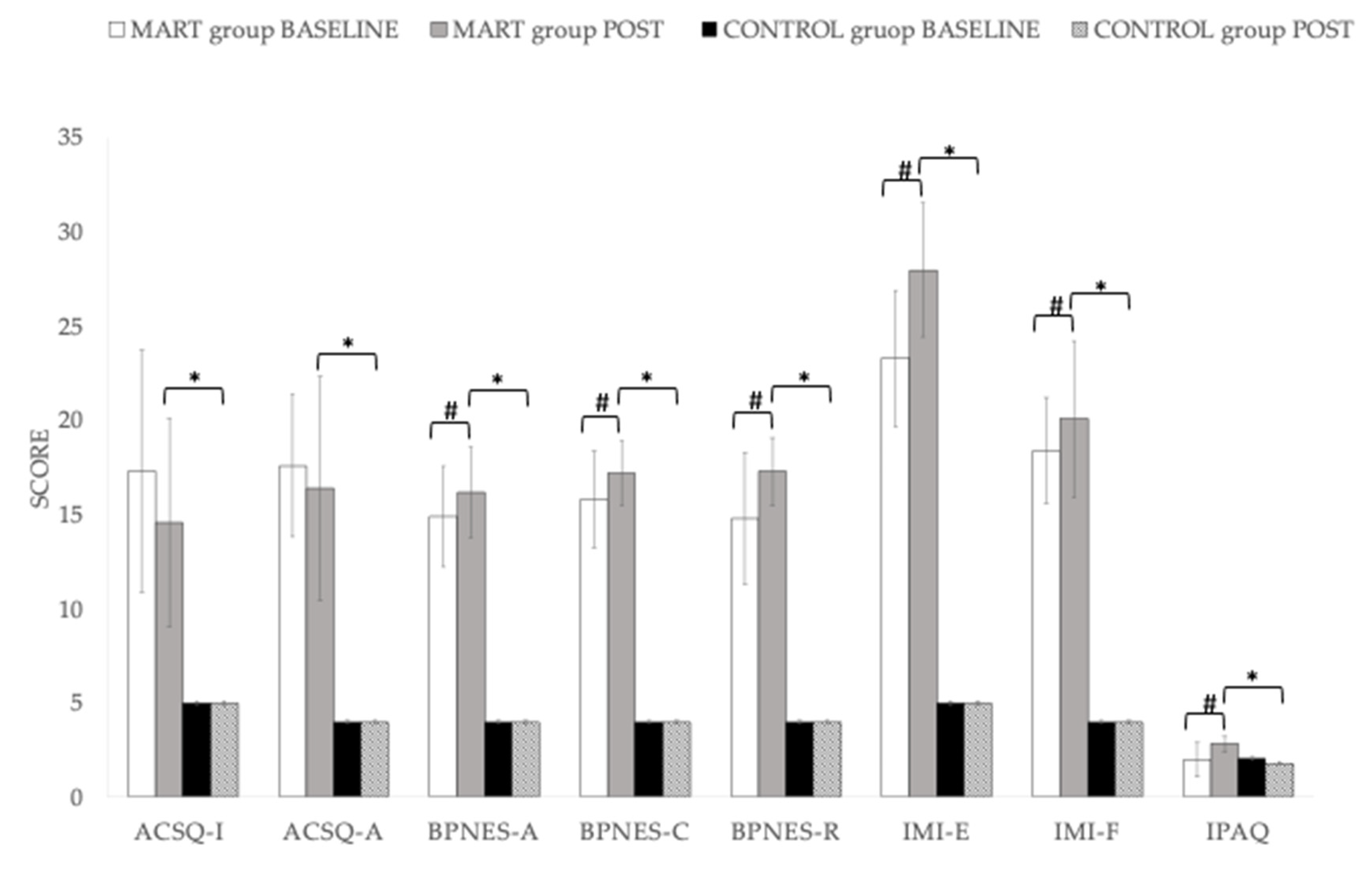
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tang, M.; Wang, D.; Guerrien, A. A systematic review and meta-analysis on basic psychological need satisfaction, motivation, and well-being in later life: Contributions of self-determination theory. PsyCh J. 2020, 9, 5–33. [Google Scholar] [CrossRef] [PubMed]
- Ryan, R.M.; Deci, E.L. On happiness and human potentials: A review of research on hedonic and eudaimonic well-being. Ann. Rev. Psychol. 2001, 52, 141–166. [Google Scholar] [CrossRef]
- Ryan, R.M.; Deci, E.L. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am. Psychol. 2000, 55, 68–78. [Google Scholar] [CrossRef] [PubMed]
- Ekelund, C.; Dahlin-Ivanoff, S.; Eklund, K. Self-determination and older people-A concept analysis. Scand. J. Occup. Ther. 2014, 21, 116–124. [Google Scholar] [CrossRef] [PubMed]
- Cardol, M.; De Jong, B.A.; Ward, C.D. On autonomy and participation in rehabilitation. Disabil. Rehabil. 2002, 24, 970–974. [Google Scholar] [CrossRef]
- Mackenzie, C.S.; Karaoylas, E.C.; Starzyk, K.B. Lifespan Differences in a self determination theory model of eudaimonia: A cross-sectional survey of younger, middle-aged, and older adults. J. Happiness Stud. 2018, 19, 2465–2487. [Google Scholar] [CrossRef]
- Souesme, G.; Martinent, G.; Ferrand, C. Perceived autonomy support, psychological needs satisfaction, depressive symptoms and apathy in French hospitalized older people. Arch. Gerontol. Geriatr. 2016, 65, 70–78. [Google Scholar] [CrossRef] [PubMed]
- Sandman, L. On the autonomy turf. Assessing the value of autonomy to patients. Med. Health Care Philos. 2005, 7, 261–268. [Google Scholar] [CrossRef]
- Deci, E.L.; Ryan, R.M. The “what” and “why” of goal pursuits: Human needs and the self-determination of behavior. Psychol. Inq. 2000, 11, 227–268. [Google Scholar] [CrossRef]
- Conroy, D.E.; Douglas Coatsworth, J. Assessing autonomy-supportive coaching strategies in youth sport. Psychol. Sport Exerc. 2007, 8, 671–684. [Google Scholar] [CrossRef] [PubMed]
- Lim, B.S.C.; Wang, C.K.J. Perceived autonomy support, behavioural regulations in physical education and physical activity intention. Psychol. Sport Exerc. 2009, 10, 52–60. [Google Scholar] [CrossRef]
- Pelletier, L.G.; Fortier, M.S.; Vallerand, R.J.; Brière, N.M. Associations among perceived autonomy support, forms of self-regulation, and persistence: A prospective study. Motiv. Emot. 2001, 25, 279–306. [Google Scholar] [CrossRef]
- Adie, J.W.; Duda, J.L.; Ntoumanis, N. Autonomy support, basic need satisfaction and the optimal functioning of adult male and female sport participants: A test of basic needs theory. Motiv. Emot. 2008, 32, 189–199. [Google Scholar] [CrossRef]
- Reinboth, M.; Duda, J.L.; Ntoumanis, N. Dimensions of coaching behavior, need satisfaction, and the psychological and physical welfare of young athletes. Motiv. Emot. 2004, 28, 297–313. [Google Scholar] [CrossRef]
- Ingledew, D.K.; Markland, D.; Medley, A.R. Exercise motives and stages of change. J. Health Psychol. 1998, 3, 477–489. [Google Scholar] [CrossRef] [PubMed]
- Landi, F.; Marzetti, E.; Martone, A.M.; Bernabei, R.; Onder, G. Exercise as a remedy for sarcopenia. Curr. Opin. Clin. Nutr. Metab. Care 2014, 17, 25–31. [Google Scholar] [CrossRef]
- Yates, L.B.; Djoussé, L.; Kurth, T.; Buring, J.E.; Gaziano, J.M. Exceptional longevity in men: Modifiable factors associated with survival and function to age 90 years. Arch. Intern. Med. 2008, 168, 284–290. [Google Scholar] [CrossRef] [PubMed]
- Sherrington, C.; Fairhall, N.; Kwok, W.; Wallbank, G.; Tiedemann, A.; Michaleff, Z.A.; Ng, C.A.C.M.; Bauman, A. Evidence on physical activity and falls prevention for people aged 65+ years: Systematic review to inform the WHO guidelines on physical activity and sedentary behaviour. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 144. [Google Scholar] [CrossRef]
- Kekäläinen, T.; Kokko, K.; Tammelin, T.; Sipilä, S.; Walker, S. Motivational characteristics and resistance training in older adults: A randomized controlled trial and 1-year follow-up. Scand. J. Med. Sci. Sport. 2018, 28, 2416–2426. [Google Scholar] [CrossRef]
- Ferrand, C.; Nasarre, S.; Hautier, C.; Bonnefoy, M. Aging and well-being in French older adults regularly practicing physical activity: A self-determination perspective. J. Aging Phys. Act. 2012, 20, 215–230. [Google Scholar] [CrossRef][Green Version]
- Delle Fave, A.; Bassi, M.; Boccaletti, E.S.; Roncaglione, C.; Bernardelli, G.; Mari, D. Promoting well-being in old age: The psychological benefits of two training programs of adapted physical activity. Front. Psychol. 2018, 9, 828. [Google Scholar] [CrossRef] [PubMed]
- Talar, K.; Hernández-Belmonte, A.; Vetrovsky, T.; Steffl, M.; Kałamacka, E.; Courel-Ibáñez, J. Benefits of resistance training in early and late stages of frailty and sarcopenia: A systematic review and meta-analysis of randomized controlled studies. J. Clin. Med. 2021, 10, 1630. [Google Scholar] [CrossRef] [PubMed]
- Fragala, M.S.; Cadore, E.L.; Dorgo, S.; Izquierdo, M.; Kraemer, W.J.; Peterson, M.D.; Ryan, E.D. Resistance training for older adults: Position statement from the national strength and conditioning association. J. Strength Cond. Res. 2019, 33, 2019–2052. [Google Scholar] [CrossRef] [PubMed]
- García-Pinillos, F.; Laredo-Aguilera, J.A.; Muñoz-Jiménez, M.; Latorre-Román, P.A. Effects of 12-week concurrent high-intensity interval strength and endurance training program on physical performance in healthy older people. J. Strength Cond. Res. 2019, 33, 1445–1452. [Google Scholar] [CrossRef] [PubMed]
- Bergamin, M.; Zanuso, S.; Alvar, B.A.; Ermolao, A.; Zaccaria, M. Is water-based exercise training sufficient to improve physical fitness in the elderly? A systematic review of the evidence. Eur. Rev. Aging Phys. Act. 2012, 9, 129–141. [Google Scholar] [CrossRef]
- Heyneman, C.A.; Premo, D.E. A “water walkers” exercise program for the elderly. Public Health Rep. 1992, 107, 213–217. [Google Scholar]
- Bento, P.C.B.; Pereira, G.; Ugrinowitsch, C.; Rodacki, A.L.F. The effects of a water-based exercise program on strength and functionality of older adults. J. Aging Phys. Act. 2012, 20, 469–483. [Google Scholar] [CrossRef]
- Waller, B.; Ogonowska-Słodownik, A.; Vitor, M.; Rodionova, K.; Lambeck, J.; Heinonen, A.; Daly, D. The effect of aquatic exercise on physical functioning in the older adult: A systematic review with meta-analysis. Age Ageing 2016, 45, 594–602. [Google Scholar] [CrossRef] [PubMed]
- Simas, V.; Hing, W.; Pope, R.; Climstein, M. Effects of water-based exercise on bone health of middle-aged and older adults: A systematic review and meta-analysis. Open Access J. Sports Med. 2017, 8, 39–60. [Google Scholar] [CrossRef]
- Marcos-Pardo, P.J.; Martínez-Rodríguez, A.; Gil-Arias, A. Impact of a motivational resistance-training programme on adherence and body composition in the elderly. Sci. Rep. 2018, 8, 1370. [Google Scholar] [CrossRef]
- Lübcke, A.; Martin, C.; Hellström, K. Older adults’ perceptions of exercising in a senior gym. Act. Adapt. Aging 2012, 36, 131–146. [Google Scholar] [CrossRef]
- Phillips, E.M.; Schneider, J.C.; Mercer, G.R. Motivating elders to initiate and maintain exercise. Arch. Phys. Med. Rehabil. 2004, 85, s52–s57. [Google Scholar] [CrossRef] [PubMed]
- Lachman, M.E.; Lipsitz, L.; Lubben, J.; Castaneda-Sceppa, C.; Jette, A.M. When adults don’t exercise: Behavioral strategies to increase physical activity in sedentary middle-aged and older adults. Innov. Aging 2018, 2, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Saghaei, M. An overview of randomization and minimization programs for randomized clinical trials. J. Med. Signals Sens. 2011, 1, 55–61. [Google Scholar]
- Gunnarsson, T.P.; Bangsbo, J. The 10-20-30 training concept improves performance and health profile in moderately trained runners. J. Appl. Physiol. 2012, 113, 16–24. [Google Scholar] [CrossRef]
- Andrade, L.S.; Kanitz, A.C.; Häfele, M.S.; Schaun, G.Z.; Pinto, S.S.; Alberton, C.L. Relationship between oxygen uptake, heart rate, and perceived effort in an aquatic incremental test in older women. Int. J. Environ. Res. Public Health 2020, 17, 8324. [Google Scholar] [CrossRef]
- Borg, G. Psychophysical scaling with applications in physical work and the perception of exertion. Scand. J. Work Environ. Health 1990, 16, 55–58. [Google Scholar] [CrossRef]
- Moreno-Murcia, J.A.; Marcos Pardo, P.J. Estrategias Motivacionales Para Programas de Ejercicio Físico Acuático; Wanceulen: Sevilla, Spain, 2010. [Google Scholar]
- Moreno-Murcia, J.A.; Martínez-Galindo, C.; Moreno-Pérez, V.; Marcos, P.J.; Borges, F. Confirmation of the basic psychological needs in exercise scale (BPNES) with a sample of people who do healthy exercise. J. Sport. Sci. Med. 2012, 11, 141–146. [Google Scholar]
- Vlachopoulos, S.P.; Michailidou, S. Development and initial validation of a measure of autonomy, competence, and relatedness in exercise: The Basic Psychological Needs in Exercise Scale. Meas. Phys. Educ. Exerc. Sci. 2006, 10, 179–201. [Google Scholar] [CrossRef]
- Deci, E.L.; Ryan, R.M. Intrinsic Motivation and Self-Determination in Human Behavior; Plenum: New York, NY, USA, 1985. [Google Scholar]
- Markland, D.; Hardy, L. On the factorial and construct validity of the intrinsic motivation inventory: Conceptual and operational concerns. Res. Q. Exerc. Sport 1997, 68, 20–32. [Google Scholar] [CrossRef] [PubMed]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-Country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef]
- Hallal, P.C.; Victora, C.G. Reliability and validity of the international physical activity questionnaire (IPAQ). Med. Sci. Sports Exerc. 2004, 36, 556. [Google Scholar]
- Gignac, G.E.; Szodorai, E.T. Effect size guidelines for individual differences researchers. Personal. Individ. Differ. 2016, 102, 74–78. [Google Scholar] [CrossRef]
- Barriopedro, M.I.; Lledó Mallol, I.E. Relación entre la actividad física con la depresión y la satisfacción con la vida en la tercera edad. Rev. Psicol. Deport. 2001, 10, 239–246. [Google Scholar]
- Faulkner, G.; Biddle, S. Mental health nursing and the promotion of physical activity. J. Psychiatr. Ment. Health Nurs. 2002, 9, 659–665. [Google Scholar] [CrossRef]
- Moral-García, J.E.; García, D.O.; García, S.L.; Jiménez, M.A.; Dios, R.M. Influencia de la actividad física en la autoestima y riesgo de dependencia en personas mayores activas y sedentarias. Anal. Psicol. 2018, 34, 162–166. [Google Scholar] [CrossRef]
- Battaglia, G.; Bellafiore, M.; Alesi, M.; Paoli, A.; Bianco, A.; Palma, A. Effects of an adapted physical activity program on psychophysical health in elderly women. Clin. Interv. Aging 2016, 11, 1009–1015. [Google Scholar] [CrossRef] [PubMed]
- Netz, Y.; Wu, M.J.; Becker, B.J.; Tenenbaum, G. Physical activity and psychological well-being in advanced age: A meta-analysis of intervention studies. Psychol. Aging 2005, 20, 272–284. [Google Scholar] [CrossRef] [PubMed]
- Ferrand, C.; Martinent, G.; Durmaz, N. Psychological need satisfaction and well-being in adults aged 80years and older living in residential homes: Using a self-determination theory perspective. J. Aging Stud. 2014, 30, 104–111. [Google Scholar] [CrossRef] [PubMed]
- Ruuskanen, J.M.; Ruoppila, I. Physical activity and psychological well-being among people aged 65 to 84 years. Age Ageing 1995, 24, 292–296. [Google Scholar] [CrossRef]
- Katayama, O.; Lee, S.; Bae, S.; Makino, K.; Chiba, I.; Harada, K.; Shinkai, Y.; Shimada, H. Participation in social activities and relationship between walking habits and disability incidence. J. Clin. Med. 2021, 10, 1895. [Google Scholar] [CrossRef] [PubMed]
- Pernambuco, C.S.; Borba-Pinheiro, C.J.; Vale, R.G. de S.; Di Masi, F.; Monteiro, P.K.P.; Dantas, E.H.M. Functional autonomy, bone mineral density (BMD) and serum osteocalcin levels in older female participants of an aquatic exercise program (AAG). Arch. Gerontol. Geriatr. 2013, 56, 466–471. [Google Scholar] [CrossRef] [PubMed]
- D’Angelo, M.E.S.; Pelletier, L.G.; Reid, R.D.; Huta, V. The roles of self-efficacy and motivation in the prediction of short- and long-term adherence to exercise among patients with coronary heart disease. Health Psychol. 2014, 33, 1344–1353. [Google Scholar]
- Collado-Mateo, D.; Lavín-Pérez, A.M.; Peñacoba, C.; Del Coso, J.; Leyton-Román, M.; Luque-Casado, A.; Gasque, P.; Fernández-Del-Olmo, M.Á.; Amado-Alonso, D. Key factors associated with adherence to physical exercise in patients with chronic diseases and older adults: An umbrella review. Int. J. Environ. Res. Public Health 2021, 18, 2023. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| MART Group (n = 17) | Control Group (n = 17) | Baseline Differences | ||||||
|---|---|---|---|---|---|---|---|---|
| Baseline | Baseline | |||||||
| Mean | SD | Mean | SD | t | p | |||
| Age (Years) | 69.6 | ± | 5.01 | 67.7 | ± | 3.60 | 1.257 | 0.218 |
| Height (cm) | 162 | ± | 7.88 | 154 | ± | 5.47 | 3.347 | 0.002 * |
| Weight (kg) | 75.3 | ± | 12.8 | 66.9 | ± | 10.2 | 2.122 | 0.042 * |
| Effect Time | Effect Time × Group | |||||||
|---|---|---|---|---|---|---|---|---|
| MD | SE | t | p | MD | SE | t | p | |
| ACSQ Interest in the athlete’s opinion | 1.43 | 0.75 | 1.90 | 0.066 | 9.36 | 1.38 | 6.76 | < 0.001 |
| ACSQ Assessment of autonomous behaviour | 0.63 | 0.74 | 0.85 | 0.403 | 12.26 | 1.22 | 60.4 | < 0.001 |
| BPNES Autonomy | −0.63 | 0.34 | −1.87 | 0.070 | 12.15 | 0.62 | 19.55 | < 0.001 |
| BPNES Competence | −0.74 | 0.33 | −2.24 | 0.032 | 13.22 | 0.53 | 24.89 | < 0.001 |
| BPNES Relationship with others | −1.29 | 0.47 | −2.73 | 0.010 | 13.31 | 0.69 | 19.39 | < 0.001 |
| IMI Enjoyment | −2.40 | 0.69 | −3.47 | 0.001 | 23.15 | 0.86 | 26.96 | < 0.001 |
| IMI Effort | −0.83 | 0.46 | −1.80 | 0.080 | 16.32 | 0.80 | 20.29 | < 0.001 |
| IPAQ | −0.31 | 0.15 | −2.05 | 0.049 | 1.01 | 0.25 | 50.70 | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martínez-Rodríguez, A.; Cuestas-Calero, B.J.; García-De Frutos, J.M.; Marcos-Pardo, P.J. Psychological Effects of Motivational Aquatic Resistance Interval Training and Nutritional Education in Older Women. Healthcare 2021, 9, 1665. https://doi.org/10.3390/healthcare9121665
Martínez-Rodríguez A, Cuestas-Calero BJ, García-De Frutos JM, Marcos-Pardo PJ. Psychological Effects of Motivational Aquatic Resistance Interval Training and Nutritional Education in Older Women. Healthcare. 2021; 9(12):1665. https://doi.org/10.3390/healthcare9121665
Chicago/Turabian StyleMartínez-Rodríguez, Alejandro, Bernardo José Cuestas-Calero, José Manuel García-De Frutos, and Pablo Jorge Marcos-Pardo. 2021. "Psychological Effects of Motivational Aquatic Resistance Interval Training and Nutritional Education in Older Women" Healthcare 9, no. 12: 1665. https://doi.org/10.3390/healthcare9121665
APA StyleMartínez-Rodríguez, A., Cuestas-Calero, B. J., García-De Frutos, J. M., & Marcos-Pardo, P. J. (2021). Psychological Effects of Motivational Aquatic Resistance Interval Training and Nutritional Education in Older Women. Healthcare, 9(12), 1665. https://doi.org/10.3390/healthcare9121665