
Perceived Barriers of Physical Activity Participation in Individuals with Intellectual Disability—A Systematic Review

 ,
,  , ,
, ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Information Sources and Search Strategy
2.2. Eligility Criteria
2.3. Selection and Data Collection Process
2.4. Evaluation of the Quality of the Studies
3. Results
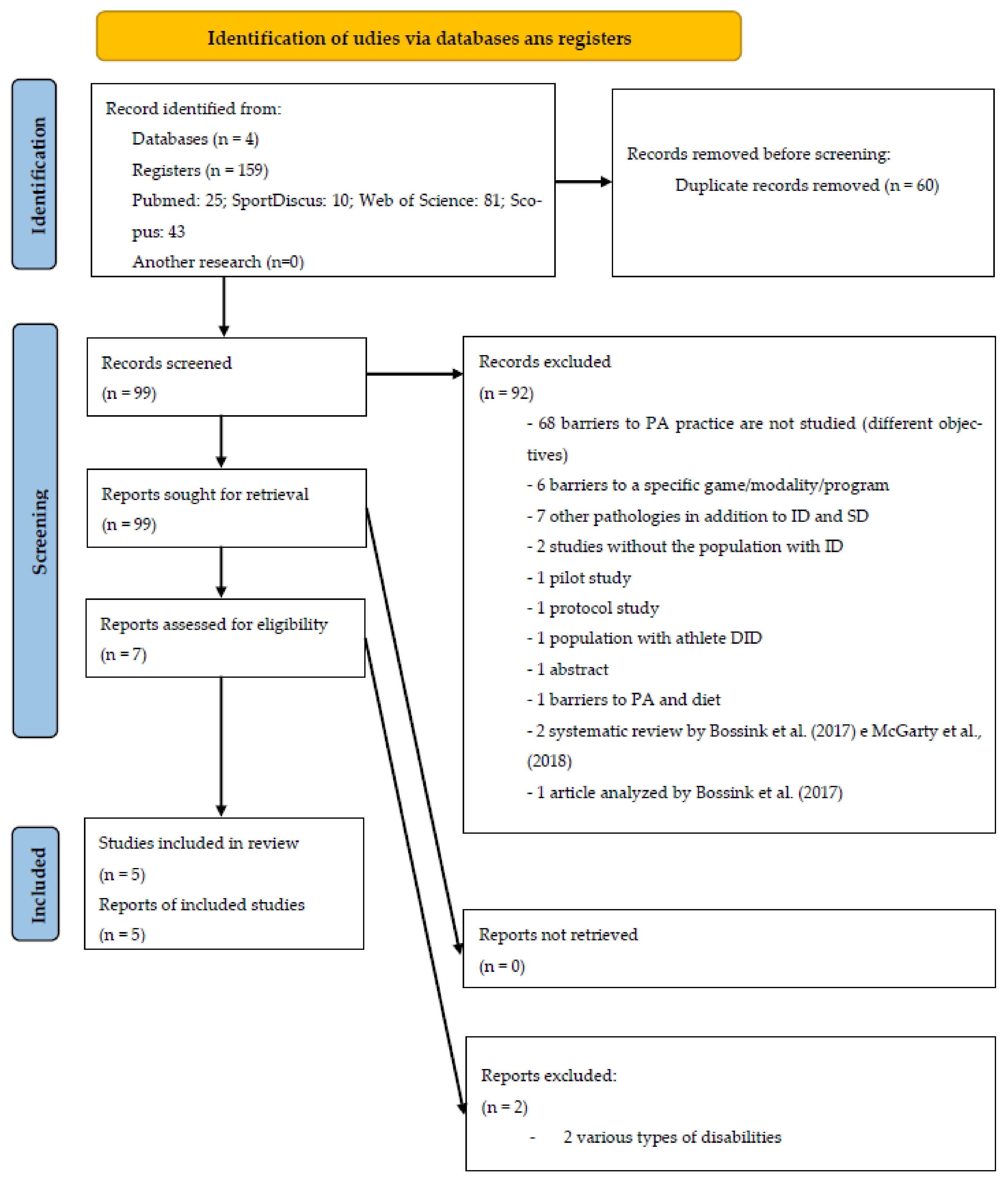
3.1. Selection of Studies
3.2. Methodological Quality
3.3. Characteristics of the Studies
3.4. Origin
3.5. Type of Studies
3.6. Participants
3.7. Evaluation Techniques
3.8. Barriers to PA Pratice
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Personal | Interpersonal | Organizational | Community | Public Policy | Author | |
|---|---|---|---|---|---|---|
| Greater participation by families | X | Alesi [20]; McGarty et al. [22]; Stanish et al. [24] | ||||
| Creating more adapted sports offerings | X | X | Alesi [20] | |||
| Organize environments that aim to stimulate sports participation | X | X | X | Alesi [20] | ||
| Organizational change, in the sense of giving greater importance to PA in the lives of people with ID | X | Cartwright et al. [21] | ||||
| Local authorities or organizations to increase the offer of adapted PA and finance services | X | X | X | Cartwright et al. [21]; Stanish et al. [24] | ||
| Pay more attention to the sporting preferences of individuals | X | X | X | X | Cartwright et al. [21] | |
| Greater cooperation between all parties in order to promote PA | X | X | X | X | X | Cartwright et al. [21] |
| More and better support and information | X | X | X | X | McGarty et al. [22] | |
| Personal training | X | X | Stanish et al. [24] | |||
| PA instruction carried out carefully and with quality; | X | Stanish et al. [24] | ||||
| Development of group activities | X | X | X | X | Stanish et al. [24] |
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM–5); American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Dairo, Y.M.; Collett, J.; Dawes, H.; Oskrochi, G.R. Physical activity levels in adults with intellectual disabilities: A systematic review. Prev. Med. Rep. 2016, 4, 209–219. [Google Scholar] [CrossRef]
- Hsieh, K.; Hilgenkamp, T.I.M.; Murthy, S.; Heller, T.; Rimmer, J.H. Low levels of physical activity and sedentary behavior in adults with intellectual disabilities. Int. J. Environ. Res. Public Health 2017, 14, 1503. [Google Scholar] [CrossRef]
- World Health Organization. Guidelines on Physical Activity and Sedentary Behaviour; World Health Organization WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Borji, R.; Zghal, F.; Zarrouk, N.; Sahli, S.; Rebai, H. Individuals with intellectual disability have lower voluntary muscle activation level. Res. Dev. Disabil. 2014, 35, 3574–3581. [Google Scholar] [CrossRef]
- Chow, B.C.; Choi, P.H.N.; Huang, W.Y.J. Physical Activity and Physical Fitness of Adults with Intellectual Disabilities in Group Homes in Hong Kong. Int. J. Environ. Res. Public Health 2018, 15, 1370. [Google Scholar] [CrossRef] [PubMed]
- Gawlik, K.; Zwierzchowska, A.; Manowska, B.; Celebańska, D. Aerobic capacity of adults with intellectual disabilities. Ann. Agric. Environ. Med. 2016, 24, 117–120. [Google Scholar] [CrossRef] [PubMed]
- De Winter, C.F.; Bastiaanse, L.P.; Hilgenkamp, T.I.M.; Evenhuis, H.M.; Echteld, M.A. Cardiovascular risk factors (diabetes, hypertension, hypercholesterolemia and metabolic syndrome) in older people with intellectual disability: Results of the HA-ID study. Res. Dev. Disabil. 2012, 33, 1722–1731. [Google Scholar] [CrossRef] [PubMed]
- Bartlo, P.; Klein, P.J. Physical activity benefits and needs in adults with intellectual disabilities: Systematic review of the literature. Am. J. Intellect. Dev. Disabil. 2011, 116, 220–232. [Google Scholar] [CrossRef] [PubMed]
- Pestana, M.B.; Barbieri, F.A.; Vitório, R.; Figueiredo, G.A.; Mauerberg de Castro, E. Efeitos do Exercício Físico para Adultos com Deficiência Intelectual: Uma revisão sistemática. J. Phys. Educ. 2018, 29, e2920. [Google Scholar] [CrossRef][Green Version]
- Ptomey, L.T.; Szabo, A.N.; Willis, E.A.; Gorczyca, A.M.; Greene, J.L.; Danon, J.C.; Donnelly, J.E. Changes in cognitive function after a 12-week exercise intervention in adults with Down syndrome. Disabil. Health J. 2018, 11, 486–490. [Google Scholar] [CrossRef] [PubMed]
- Calders, P.; Elmahgoub, S.; Roman de Mettelinge, T.; Vandenbroeck, C.; Dewandele, I.; Rombaut, L.; Vandevelde, A.; Cambier, D. Effect of combined exercise training on physical and metabolic fitness in adults with intellectual disability: A controlled trial. Clin. Rehabil. 2011, 25, 1097–1108. [Google Scholar] [CrossRef]
- Bossink, L.W.M.; van der Putten, A.A.; Vlaskamp, C. Understanding low levels of physical activity in people with intellectual disabilities: A systematic review to identify barriers and facilitators. Res. Dev. Disabil. 2017, 68, 95–110. [Google Scholar] [CrossRef]
- McGarty, A.M.; Melville, C.A. Parental perceptions of facilitators and barriers to physical activity for children with intellectual disabilities: A mixed methods systematic review. Res. Dev. Disabil. 2018, 73, 40–57. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Steward, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Bento, T. Revisões sistemáticas em desporto e saúde: Orientações para o planeamento, elaboração, redação e avaliação. Motricidade 2014, 10, 107–123. [Google Scholar] [CrossRef]
- Methley, A.M.; Campbell, S.; Chew-Graham, C.; McNally, R.; Cheraghi-Sohi, S. PICO, PICOS and SPIDER: A comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv. Res. 2014, 14, 579. [Google Scholar] [CrossRef]
- Nang, C.; Piano, B.; Lewis, A.; Lycett, K.; Woodhouse, M. Using The PICOS Model to Design and Conduct a Systematic Search: A Speech Pathology Case Study. In Proceedings of the ECU Research Week, Perth, Australia, 14–18 September 2015; p. 51. [Google Scholar]
- Alesi, M. Investigating Parental Beliefs Concerning Facilitators and Barriers to the Physical Activity in Down Syndrome and Typical Development. SAGE Open 2017, 7, 215824401668779. [Google Scholar] [CrossRef]
- Cartwright, L.; Reid, M.; Hammersley, R.; Walley, R.M. Barriers to increasing the physical activity of people with intellectual disabilities. Br. J. Learn. Disabil. 2017, 45, 47–55. [Google Scholar] [CrossRef]
- McGarty, A.M.; Westrop, S.C.; Melville, C.A. Exploring parents’ experiences of promoting physical activity for their child with intellectual disabilities. J. Appl. Res. Intellect. Disabil. 2021, 34, 140–148. [Google Scholar] [CrossRef]
- Salomon, C.; Whittle, E.; Bellamy, J.; Evans, E.; Teasdale, S.; Samaras, K.; Ward, P.B.; Hsu, M.; Trollor, J. A qualitative exploration of barriers and enablers of healthy lifestyle engagement for older Australians with intellectual disabilities. Res. Pract. Intellect. Dev. Disabil. 2019, 6, 182–191. [Google Scholar] [CrossRef]
- Stanish, H.I.; Curtin, C.; Must, A.; Phillips, S.; Maslin, M.; Bandini, L.G. Physical Activity Enjoyment, Perceived Barriers, and Beliefs Among Adolescents with and Without Intellectual Disabilities. J. Phys. Act. Health 2016, 13, 102–110. [Google Scholar] [CrossRef]
- Downs, S.H.; Black, N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J. Epidemiol. Community Health 1998, 52, 377–384. [Google Scholar] [CrossRef]
- Abellán, J.; Januário, N. Barreras, facilitadores y motivos de la práctica deportiva de deportistas con discapacidad intelectual. Psychol. Soc. Educ. 2017, 9, 419–431. [Google Scholar] [CrossRef]
- Bossink, L.W.M.; van der Putten, A.A.J.; Vlaskamp, C. Physical-activity support for people with intellectual disabilities: A theory-informed qualitative study exploring the direct support professionals’ perspective. Disabil. Rehabil. 2020, 42, 3614–3620. [Google Scholar] [CrossRef] [PubMed]
- Chow, B.C.; Choi, P.H.N.; Huang, W.Y.; Pan, C.-Y. Promoting Physical Activity in Group Home Settings: Staff Perspectives through a SWOT Analysis. Int. J. Environ. Res. Public Health 2020, 17, 5805. [Google Scholar] [CrossRef]
- Hartman, E.; Smith, J.; Westendorp, M.; Visscher, C. Development of physical fitness in children with intellectual disabilities. J. Intellect. Disabil. Res. 2015, 59, 439–449. [Google Scholar] [CrossRef] [PubMed]
- Telama, R.; Yang, X.; Viikari, J.; Välimäki, I.; Wanne, O.; Raitakari, O. Physical activity from childhood to adulthood: A 21-year tracking study. Am. J. Prev. Med. 2005, 28, 267–273. [Google Scholar] [CrossRef]
- Temple, V.A.; Stanish, H.I. The feasibility of using a peer-guided model to enhance participation in community-based physical activity for youth with intellectual disability. J. Intellect. Disabil. 2011, 15, 209–217. [Google Scholar] [CrossRef]
- Trost, S.G.; Kerr, L.M.; Ward, D.S.; Pate, R.R. Physical activity and determinants of physical activity in obese and non-obese children. Int. J. Obes. Relat. Metab. Disord. 2001, 25, 822–829. [Google Scholar] [CrossRef]
- Jaarsma, E.A.; Dijkstra, P.U.; Geertzen, J.H.B.; Dekker, R. Barriers to and facilitators of sports participation for people with physical disabilities: A systematic review. Scand. J. Med. Sci. Sports 2014, 24, 871–881. [Google Scholar] [CrossRef]
- Marmeleira, J.; Fernandes, J.; Ribeiro, N.; Teixeira, J.; Gutierres Filho, P. Barreiras para a prática de atividade física em pessoas com deficiência visual. Rev. Bras. Ciênc. Esporte 2018, 40, 197–204. [Google Scholar] [CrossRef]
- Tsai, E.; Fung, L. Perceived constraints to leisure time physical activity participation of students with hearing impairment. Ther. Recreat. J. 2005, 39, 192–206. [Google Scholar]
- Messent, P.R.; Cooke, C.B.; Long, J. Physical Activity, Exercise and Health of Adults with Mild and Moderate Learning Disabilities. Br. J. Learn. Disabil. 1998, 26, 17–22. [Google Scholar] [CrossRef]
- McLeroy, K.R.; Bibeau, D.; Steckler, A.; Glanz, K. An ecological perspective on health promotion programs. Health Educ. Q. 1988, 15, 351–377. [Google Scholar] [CrossRef] [PubMed]

| Author, Reference, Country | Aims | Participants | Type of Study | Evaluation Techniques | Barriers to PA Practice | Quality Score |
|---|---|---|---|---|---|---|
| Alesi [20] Italy | Compare the perceptions about the practice of PA between parents of children with and without DS. | 19 families of individuals with DS (children: 10 boys and 9 girls, 20.94Y); Recruitment: support institutions for people with DS. | Exploratory study. | Semi-structured interview with family members; Maximum duration of 25 min. | Lack of technical specialists in adapted PA; Lack of adapted PA programs; Lack of inclusive programs; Characteristics of the disability itself (physical, physiological and psychological); Parent’s preoccupation; Lack of time for parents to engage in PA with their children; Transport difficulties (high costs, lack of transport); Limitation on economic resources. | Poor |
| Cartwright et al. [21] United Kingdom | Analyze the perspectives of individuals with ID and their caregivers about PA. | N = 42 (12 individuals who were part of the project, 10 family members, 10 technical caregivers and 10 individuals with ID); Recruitment: day centres in Scotland. | Qualitative study. | Semi-structured interviews, with different questions for the 4 groups. | Acceptance of the inactive lifestyle of people with ID—technical caregivers, family members and individuals with ID; Limitation of human resources—technical caregivers and project leaders;Other preferences of intitution-techical caregivers; Communication problems between caregivers and family members regarding the dynamization of PA—technical caregivers, family members and project leaders. | Poor |
| McGarty et al. [22] United Kingdom | Explore parents’ experience in promoting PA to their children with ID. | N = 8 family members (4 mothers, 3 fathers and a stepfather—a recruited couple, who responded separately); Age of children: 10 to 18 years old (6 male; 1 female) Recruitment: support schools and clubs for people with ID in Glasgow. | Exploratory study. | Semi-structured interviews with family members; Duration: 20 to 55 min. | Lack of information about adequate and inclusive PA; Social exclusion; Fear of parents in relation to bullying; Other preoccupation of parents; Lack of support; Lack of inclusive opportunities; Stigma and lack of understanding about disability; Barriers related to disability itself. | Poor |
| Salomon et al. [23] Australia | Perception of barriers and facilitators to the practice of PA and healthy eating (separately). | N = 14; 6 renumbered workers and 8 people with ID; ˃60Y; Recruitment: support service for people with ID. | Qualitative study. | Semi-structured interviews. | Both groups: (i) aging; (ii) health problems; (iii) lack of adapted spaces; (iv) lack of inclusion; ID group: (i) chronic diseases; (ii) climatic conditions; Group of workers (i) low concentration; (ii) challenging behaviors; iii) social stigma; (iv) lack of adapted places; (v) sensory issues (example: loud music in spaces; (vi) limitation of financial resources; (vii) limitation of human resources. | Poor |
| Stanish et al. [24] USA | Compare pleasure with PA, perceived barriers, beliefs and self-efficacy between ID and the general population. | N = 98; ID group (N = 38, 3–21 years, AA:16.8y); general population group (N = 60, 13–18y, AA: 15.3y); Recruitment: agencies, organizations and schools to support individuals with ID. | Cross-sectional study. | Structured interview of 33 closed-response items; Duration: 15 to 20 min. | ID group: (i) PA is difficult to learn; (ii) lack of places to practice PA. | Poor |
| Personal | Characteristics of the disability itself (physical, physiological and psychological); acceptance of inactive lifestyles; aging; health problems; lack of concentration; challenging behaviors. |
| Family members | Parents’ concerns (bullying, among others); acceptance of inactive lifestyles; communication problems with technical caregivers; lack of time to engage in PA with their children. |
| Social | Acceptance of inactive lifestyles; lack of information on adapted PA; lack of adapted PA programs; lack of inclusive opportunities; lack of technicians specialized in adapted PA; lack of places to practice PA; limitation of human resources; other preferences of the institution providing support services; communication problems between family members and caregivers; social exclusion (stigma and lack of understanding in relation to disability); lack of support; sensory issues (music too loud in training places); difficulties in transportation (high costs, lack of transport). |
| Financial | Limited financial resources. |
| Environmental | Climate. |
| Personal | (i) Preference for inactive lifestyles [21]; (ii) Aging [23]; (iii) Health problems [23]. |
| Social | (i) Lack of adapted spaces [23]; (ii) Lack of inclusion [23]; (iii) Lack of places to practice PA [24]; (iv) Lack of adapted PA [24]. |
| Environmental | (i) Adverse weather conditions [23]. |
| Personal | (i) Characteristics of the disability itself [20,22]. |
| Social | (i) Lack of specialists in adapted PA [20]; (ii) Lack of adapted PA programs [20]; (iii) Lack of inclusive programs [20,22]; (iv) Difficulties in transportation [20]; (v) Lack of information about adequate and inclusive PA [22]; (vi) Social exclusion [22]; (vii) Lack of support [22]; (viii) Stigma and lack of understanding of disability [22]. |
| Family members | (i) Parents’ concerns [20,22]; (ii) Lack of time for parents to engage in PA with their children [20]; (iii) Acceptance of children’s inactive lifestyles [21]; (iv) Communication problems between family members and caregivers [21]. |
| Financial | (i) Limitation of economic resources [20]. |
| Personal | (i) Aging [23]; (ii) Health problems [23]; (iii) Low concentration capacity [23]; (iv) Challenging behaviors [23]. |
| Social | (i) Lack of adapted spaces [23]; (ii) Lack of inclusion [23]; (iii) Stigma [23]; (iv) Sensory issues [23]; (v) Lack of human resources in institutions; (vi) Acceptance of inactive lifestyles [21,23]; (vii) Other preferences of technical caregivers and institutions [21]; (viii) Communication problems between family members and caregivers [21]. |
| Financial | (i) Limitation of financial resources [23]. |
| Social | (i) Limitation of human resources; (ii) Communication problems between family members and caregivers. |
| Greater participation by families | Alesi [20]; McGarty et al. [22]; Stanish et al. [25] |
| Creating more adapted sports offerings | Alesi [20] |
| Organize environments that aim to stimulate sports participation | Alesi [20] |
| Organizational change, in the sense of giving greater importance to PA in the lives of people with ID | Cartwright et al. [21] |
| Local authorities or organizations to increase the offer of adapted PA and finance services | Cartwright et al. [21]; Stanish et al. [25] |
| Pay more attention to the sporting preferences of individuals | Cartwright et al. [21] |
| Greater cooperation between all parties in order to promote PA | Cartwright et al. [21] |
| More and better support and information | McGarty et al. [22] |
| Personal training | Stanish et al. [24] |
| PA instruction carried out carefully and with quality | Stanish et al. [24] |
| Development of group activities | Stanish et al. [24] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jacinto, M.; Vitorino, A.S.; Palmeira, D.; Antunes, R.; Matos, R.; Ferreira, J.P.; Bento, T. Perceived Barriers of Physical Activity Participation in Individuals with Intellectual Disability—A Systematic Review. Healthcare 2021, 9, 1521. https://doi.org/10.3390/healthcare9111521
Jacinto M, Vitorino AS, Palmeira D, Antunes R, Matos R, Ferreira JP, Bento T. Perceived Barriers of Physical Activity Participation in Individuals with Intellectual Disability—A Systematic Review. Healthcare. 2021; 9(11):1521. https://doi.org/10.3390/healthcare9111521
Chicago/Turabian StyleJacinto, Miguel, Anabela Sousa Vitorino, Diogo Palmeira, Raul Antunes, Rui Matos, José Pedro Ferreira, and Teresa Bento. 2021. "Perceived Barriers of Physical Activity Participation in Individuals with Intellectual Disability—A Systematic Review" Healthcare 9, no. 11: 1521. https://doi.org/10.3390/healthcare9111521
APA StyleJacinto, M., Vitorino, A. S., Palmeira, D., Antunes, R., Matos, R., Ferreira, J. P., & Bento, T. (2021). Perceived Barriers of Physical Activity Participation in Individuals with Intellectual Disability—A Systematic Review. Healthcare, 9(11), 1521. https://doi.org/10.3390/healthcare9111521