In order to suggest or encourage future lines of research, to determine which areas are sufficiently investigated and which require greater penetration, it is necessary to investigate the scientific production of the researchers. It can also be helpful to study each line of research based on a country, an author, or even a specific institution.
3.1. Descriptive Analysis
3.1.1. Evolution of Scientific Production
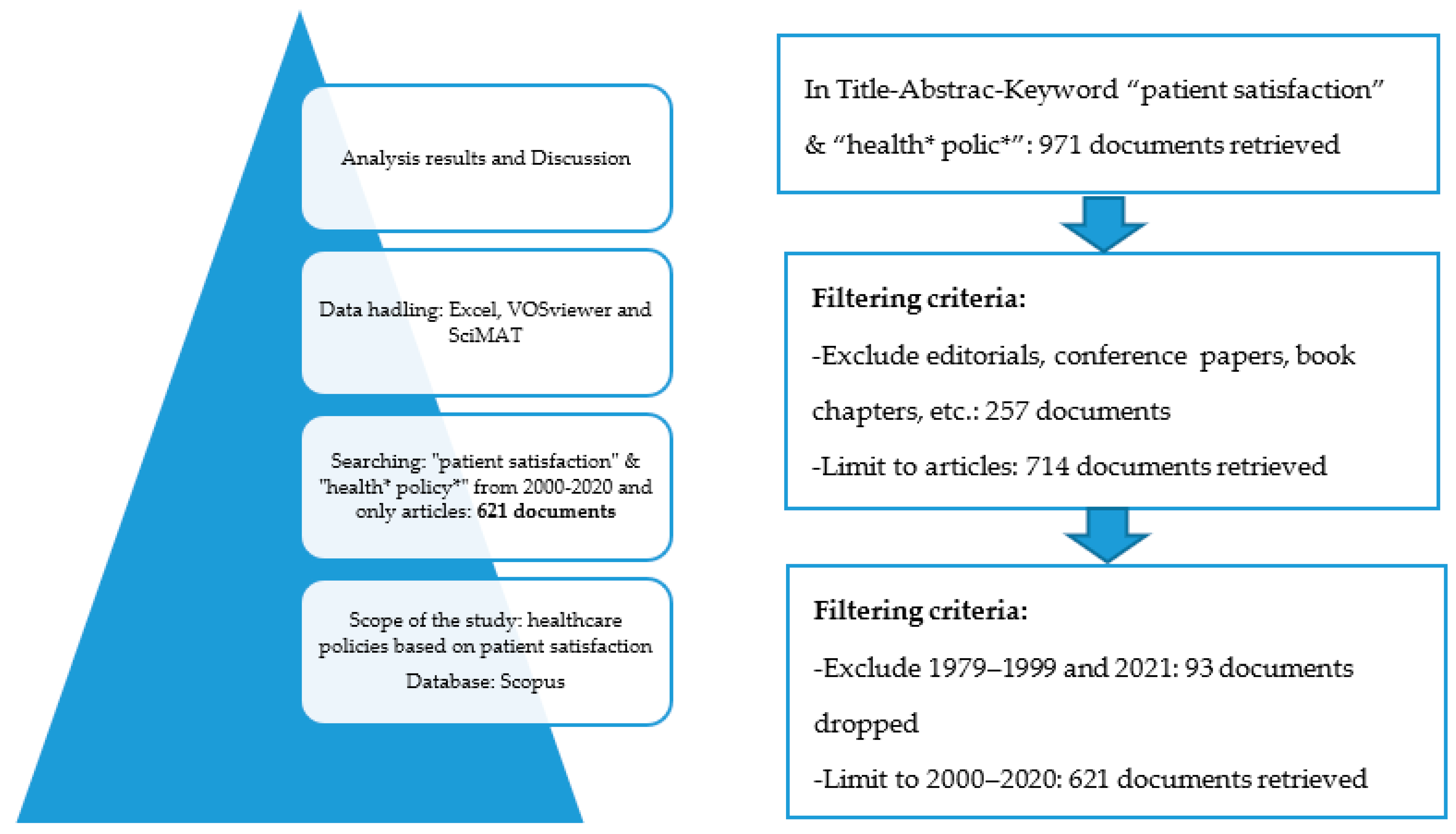
The 621 articles that make up the sample selected were published between 2000 and 2020.
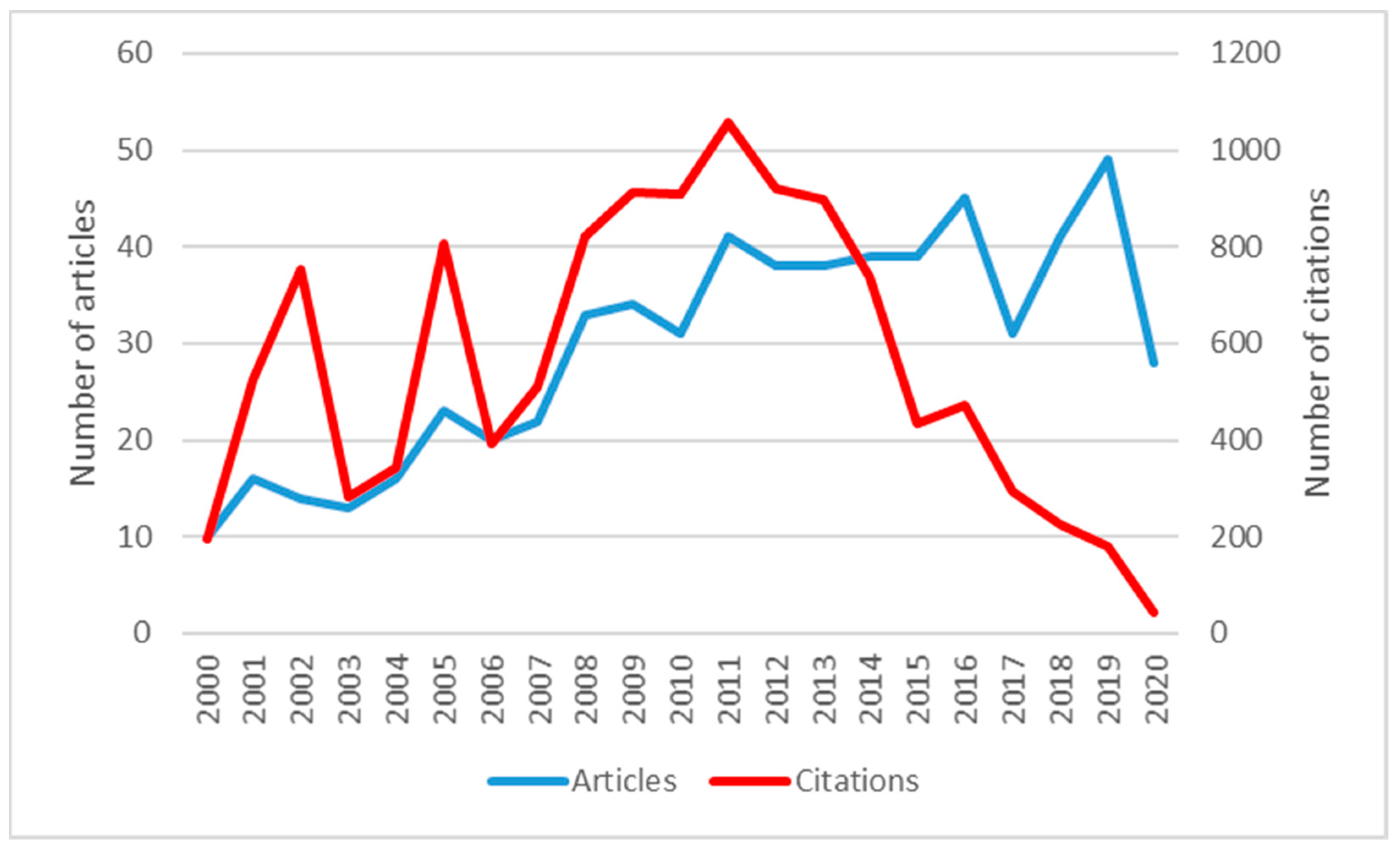
Figure 2 shows that Patient Satisfaction and Health Policy (PS and HP) has had an increasing global trend of scientific production.
Despite the growing trend, two very pronounced decreases can be observed in 2017 and 2020. This latest decrease occurs immediately after the number of publications climbs to its peak in 2019. Therefore, the decline may be caused by the COVID 19 Health Crisis, and it is likely to be an isolated event.
A total of 2672 authors wrote all the articles included in the sample. We can see that 62.64% of the total has been published during the last ten years, so it can be deduced that it is an emerging issue. The citations reached their peak in 2011 with 1059.
With respect to the number of citations, it can be observed that those years with the highest number of citations correspond to those with the highest scientific production. In the articles corresponding to the last six years, the number of citations decreases ostensibly. It should be considered that not enough time has elapsed since their publication for their influence to be effective in subsequent research.
3.1.2. Distribution of Scientific Production
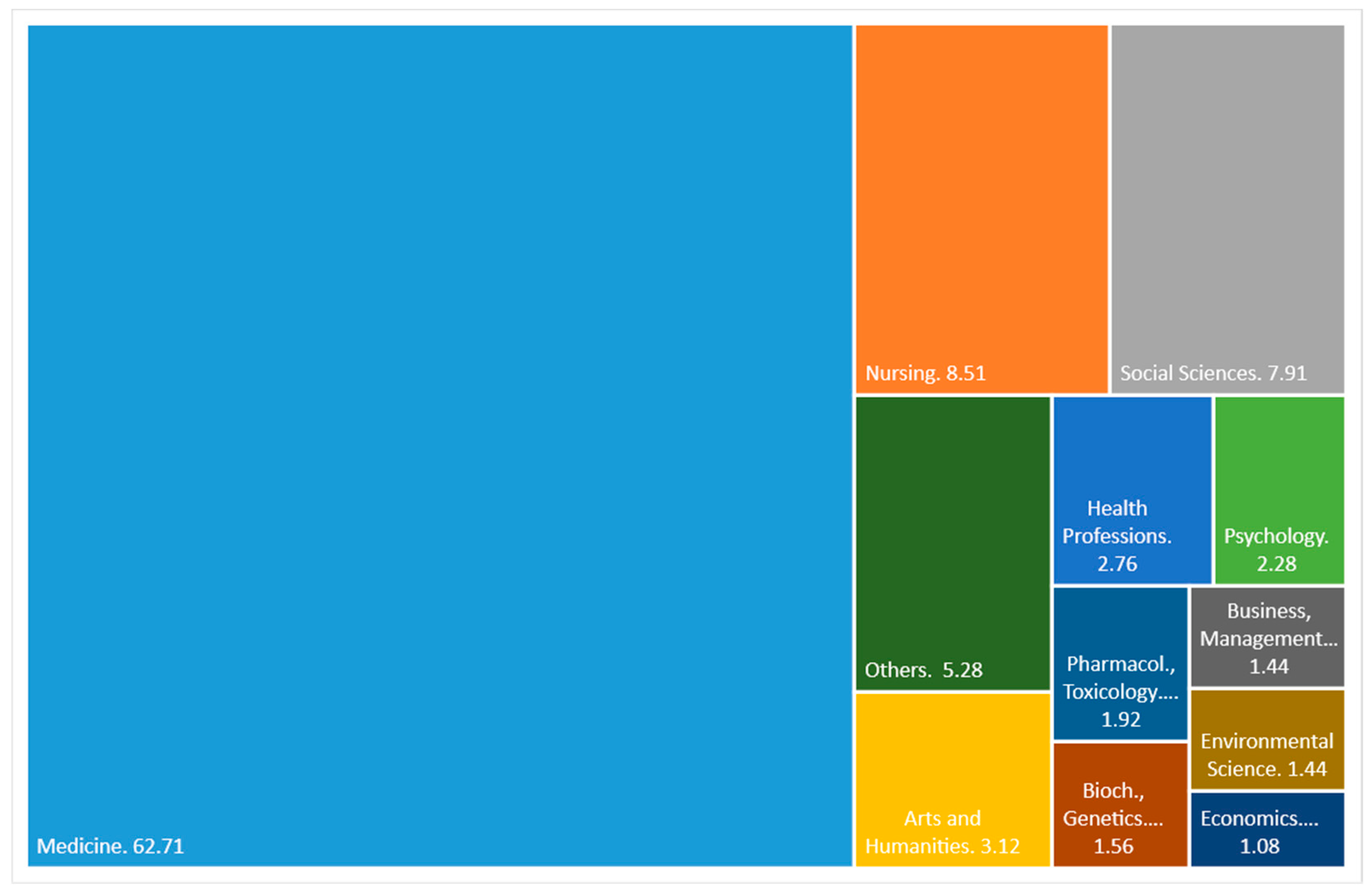
Figure 3 shows the main areas on which Scopus classifies scientific production on PS and HP. The medicine theme prevails widely over the rest with 62.71%. Far behind, with 8.51% and 7.91%, are nursing and social sciences, respectively. The rest of the defined themes have less than 4% each. As we can see, the subject is mainly approached with merely medical criteria and not from an economic or investment management point of view, areas that, as a whole, do not reach 3%.
Table 2 displays the 11 most productive PS and HP journals. These journals published 20.13% (125 of 621) of the total number of articles included in this study, which shows that scientific activity in PS and HP is distributed in a large number of journals. The first four journals produced 55.2% of the top 11, and these journals were Social Science and Medicine, BMC Health Services Research, Health Policy, and BMJ Open, in order of productivity.
Table 2 exhibits other bibliometric indicators such as the average number of citations per year since the 1st published article, the average citation by paper, the year corresponding to the first published article, the year corresponding to the last published article, the Scimago Journal Rank (Quartile in 2019), and the h-index.
It is worth noting that the first journal in the ranking, with 19 articles, generated 644 citations, while the second in the ranking with only one fewer article generated 228 fewer citations than the first. The journal with the most citations is Social Science and Medicine. However, concerning the average number of citations per article, Health Affairs leads with 53 citations per article. Far behind is the leader in scientific productivity, with 33.89 citations per article.
An important point to highlight is that none of the journals included in the top 11 has scientific activity in this area in all the years analysed, the average being 15.54 years. To reduce the effect of the number of years of publication, the average citation per year was calculated from the first year of publication, where Social Science and Medicine maintain the lead with 40.25 citations per year, followed by BMC Health Services Research with 29.71, and in third place is Health Affairs with 21.20.
Regarding the h-index, Social Science and Medicine stands out widely from the rest with an h-index of 15. BMC Health Services Research follows it with 11 and Health Policy with 9. The fourth place is shared by Health Affairs and the International Journal of Healthcare Quality Assurance with an h-index of 8. Regarding the quartile of the SJR indicator, 8 of the 11 journals are in quartile 1, which means that patient satisfaction as the basis for decision-making is an appealing topic for high-impact journals.
A noteworthy fact is that 8 of the 11 journals included in the top 11 are from the United Kingdom, which means that this country is interested in researching patient satisfaction to formulate health policies. The rests are two European (one of Irish origin and one of Swiss origin) and one American.
3.1.3. Countries, Institutions, Authors, and Papers
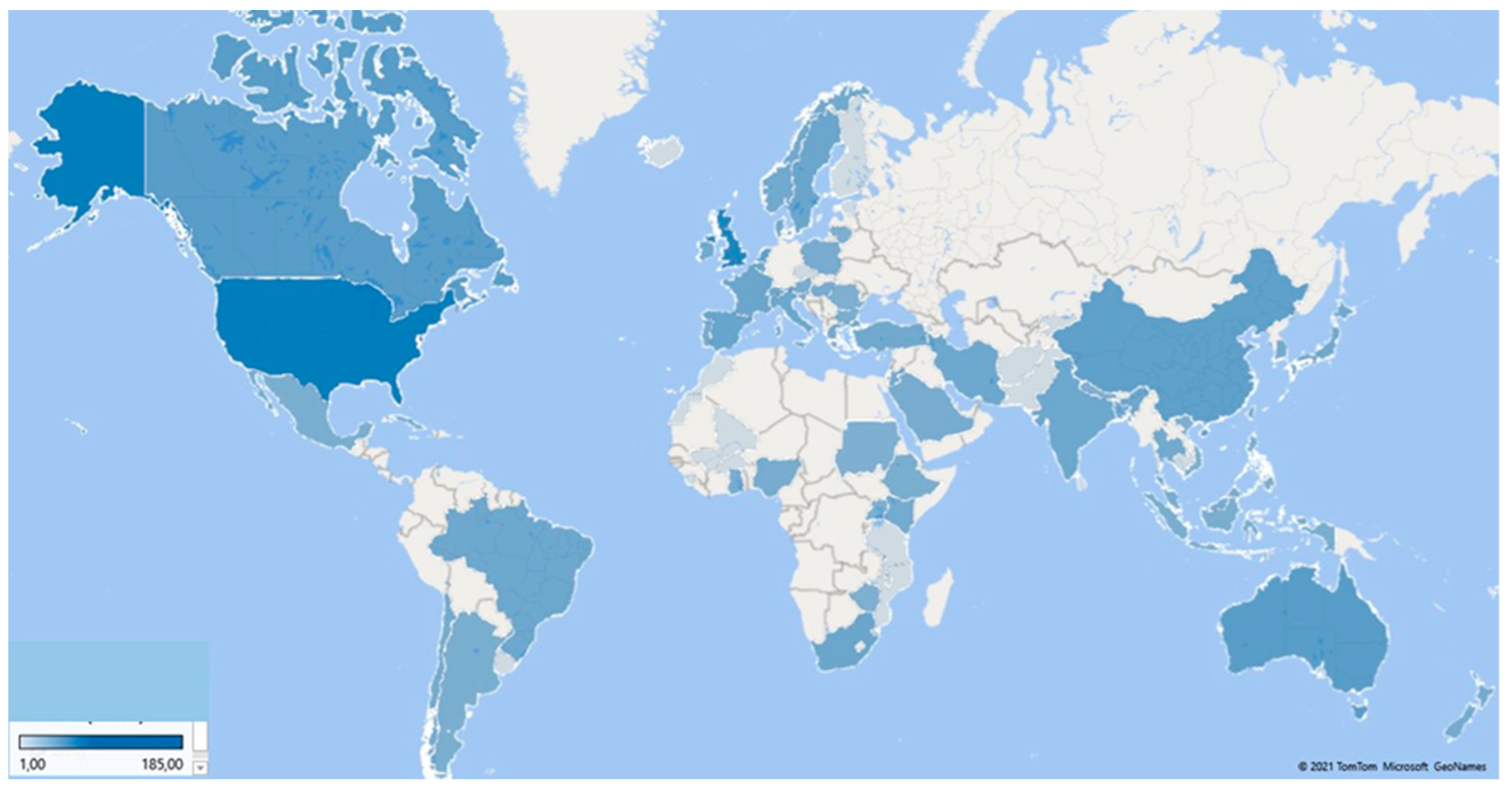
Figure 4 illustrates a map of the countries that produce PS and HP articles, and
Table 3 shows the data of the 11 most productive countries. It can be seen that most of the published articles are concentrated in the United States and the United Kingdom, with 185 and 144 published articles, respectively, which implies that authors from these two countries published 52.97% of PS and HP articles. It should be remembered that, in this analysis, a publication may represent more than one country because the authors’ affiliation institutions represent the publishing countries.
The next most productive are English-speaking countries or countries with a very high English proficiency according to the EF English Proficiency Index 2020 [
79]: Canada with 43 articles, Australia with 42, and Germany with 40. This fact is not surprising because the report above indicates that English proficiency is related to the Global Talent Competitiveness Index, which measures a country’s ability to attract, develop, and retain talented people and invest in research and development. The importance of the English language in the scientific field dates back to the Industrial Revolution because those who promoted this movement used this language as it was their mother tongue (British and American). Consequently, those who wanted to learn about the advances had to learn the Anglo-Saxon language [
80]. According to the United Nations report [
81], the United States, the United Kingdom, and Germany are among the ten countries with the highest investment in research and development.
Analysing the total number of citations, the United States is ahead, followed by the United Kingdom and Canada. On the other hand, if the analysis is based on the number of citations per article, Canada is the first, followed by the Netherlands, the United Kingdom, and Germany. The number of citations evaluates the scientific quality for which these countries are considered most useful for science. A point to highlight is that countries such as Spain and China began scientific production on this subject 9 and 8 years, respectively, later than the countries that lead the ranking, so it is expected that the number of citations will grow in the future. By considering the h-index, the names of the leading countries are the same. In first place is the United Kingdom, second place the United States, third place the Netherlands, and Canada and Germany share fourth place.
In the ranking of the 11 most productive countries, only five were productive during the 20 years studied. A relevant piece of information that can signify the diversity and growth of research on PS and HP is that the countries are on all of the continents. The United States and Canada represent America; Europe is represented by the United Kingdom, Germany, the Netherlands, Spain, France, and Sweden; Oceania accounts for Australia; China for Asia; and South Africa for Africa.
On the other hand,
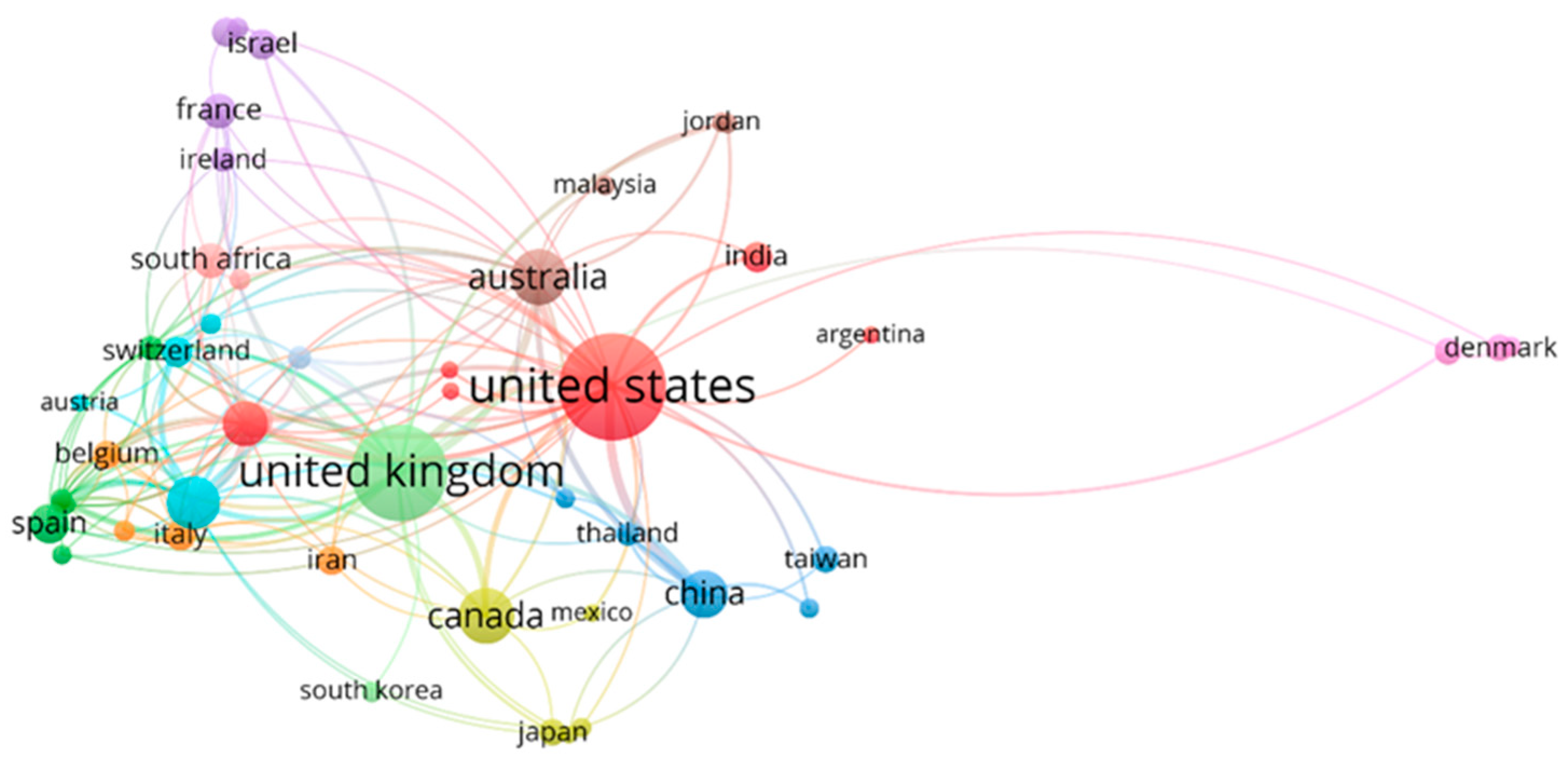
Figure 5 represents a co-authorship network based on international collaboration between countries with at least three articles published on PS and HP. The volume of the circles varies depending on the number of articles published. The colour corresponds to a cluster that encompasses each of the groups of countries. Twelve different groups can be observed.
The United States led the red cluster, representing a robust collaborative link with Argentina, Ethiopia, India, the Netherlands, and the Philippines. Spain heads the dark green group, and its major collaborating countries are all from the European continent (Bulgaria, Greece, Hungary, Norway, and Poland). China fronted the blue cluster, whose collaborators are from the same continent: Bangladesh, Hong Kong, Taiwan, and Thailand. For its part, the yellow cluster has representatives from the American continent (Canada and Mexico), Asia (Indonesia and Japan) and Africa (Nigeria). The dark purple group represents co-authorship from Brazil, France, Ireland, Israel, and Portugal.
On the other hand, the light blue comprises Austria, Chile, Germany, and Switzerland. Likewise, Belgium, Iran, Italy, and Slovenia are grouped in orange. In addition, the brown group is led by Australia, Joran, Malaysia, and Saudi Arabia. The light purple cluster, headed by Denmark, also includes Ghana and Turkey. The countries associated with the salmon colour are Kenya, South Africa, and Sweden. The light blue, orange, and brown groups are composed of co-authors representing four countries each; the light purple and salmon cluster by three countries, the light green by two countries, and the last set only by New Zealand.
Table 4 shows the ten countries that have contributed the most to scientific production through collaboration with other countries. The United States leads the ranking with 89 collaborations. China, the United Kingdom, Australia, and Canada are the countries that have collaborated the most with the United States in scientific production. Moreover, the country closest to the United States regarding the number of collaborators is the United Kingdom (85). The rest of the countries have much smaller collaborations: Germany (58), Australia (47), the Netherlands (38), and China (34). The last four positions in the top 10 have between 23 and 21 collaborators each. The United Kingdom is listed as a contributor to all countries in the top 10, as is the United States, though there is no colaboration with Belgium. The latter has a considerable number of citations, 373 for only nine published papers.
3.1.4. Productivity of the Most Prolific Authors
Table 5 shows the 17 most relevant authors in the scientific literature on PS and HP. These authors represent thirteen academic institutions. The main characteristics include the number of articles, total citations, total citations by article, the year corresponding to the first published article, the year corresponding to the last published article, the average number of citations per year since the first published article, and the h-index, all of which are displayed in the table.
Considering the number of articles published and the h-index, we can divide the authors into two groups. The first comprising the two authors with six published articles and an h-index of 6. The second group, consisting of the remaining 15 authors, with three published articles each and an h-index of 3. Of the 17 authors, ten are of European origin, and six are from the United Kingdom. There are five authors of Israeli origin who participate in this ranking. These authors have three articles published in the period analysed, with 28 citations by authorship, which is possible because they are co-authors in the three scientific productions. Only two authors represent the American continent.
None of the authors of this ranking published during 2020, while 6 of the 17 published the last paper in 2019. In 2016, six of the 17 authors listed in
Table 5 published their first article on PS and HP, and 15 of these authors published in the second part of the period analysed (2010–2020), which indicates that this line of research is booming.
The two most prolific authors are Bower, P. and Roland, M., affiliated with the Universities of Manchester and Cambridge, respectively. Both authors are from the United Kingdom. They have six published articles, an h-index of 6, their first publication in 2006 and their last in 2014. Bower, P. surpasses Roland, M. in the number of citations. The most popular work of both was “The GP patient survey for use in primary care in the national health service in the UK- development and psychometric characteristics”, published in 2009 and cited 94 times. This paper is one of the five articles that share authorship. These authors are also ranked first and second if we analyse the average number of citations per year since the first publication and the total number of citations.
The ranking is primarily led by Blendon, R.J. (86) regarding the number of citations per article with only three published papers. Far behind are Mead, N. (59.67), Cheraghi-Sohi, S. (53.33), and Kringos, D.S. (52.33), the latter also with only three articles published.
Authors with more than 100 citations began publishing on PS and HP in the first half of the period under review, except for Kringos D.S., who began publishing in 2011 and has 157 citations.
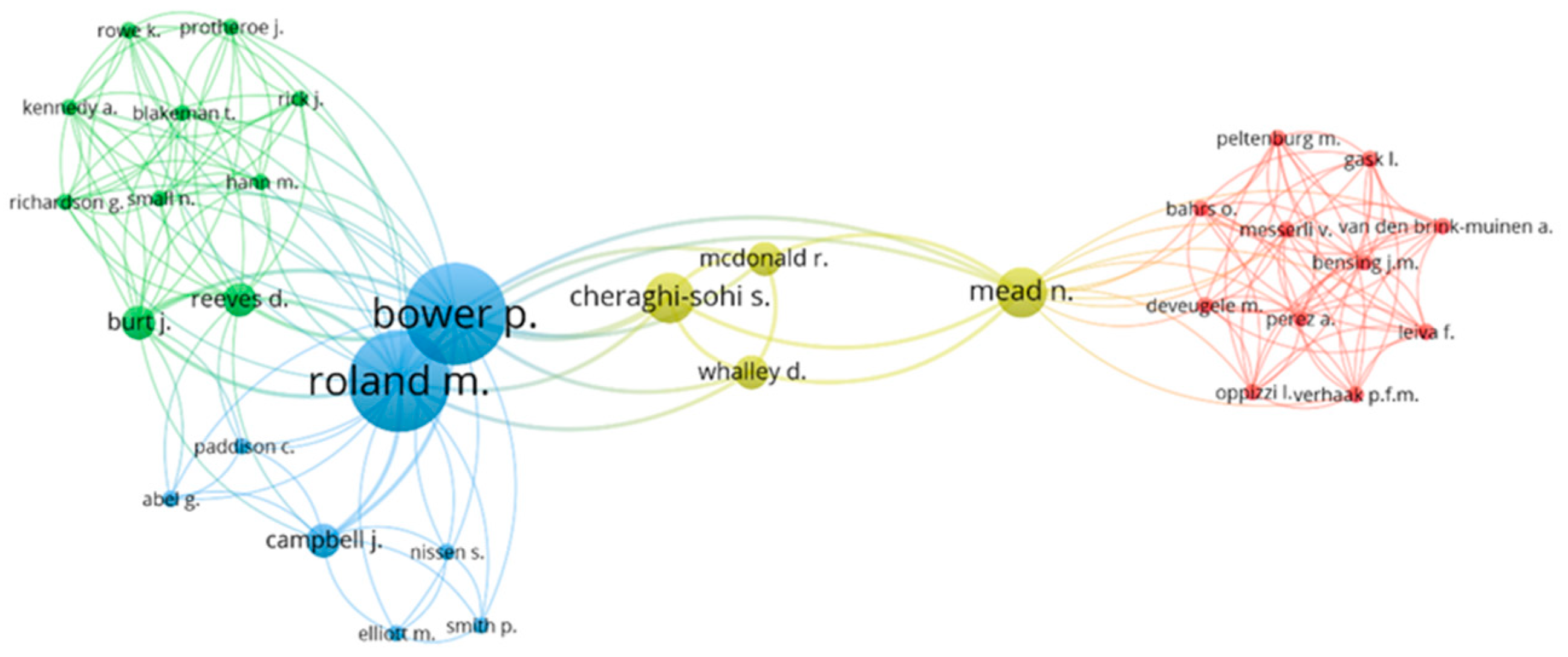
Figure 6, made with the VOSviewer tool, represents the collaboration network among the principal authors. Close authors within the diagram are particularly collaborative, and the bubble size indicates the author’s relevance within the collaboration network. Only authors with works cited at least ten times have been taken into account. Four main collaborative groups have been found. The blue group is the only one with authors considered the most productive in this study (Bower, P. and Roland, M.). The country of the affiliate institution seems to determine the collaboration. The red cluster is made up of 11 authors belonging to institutions in the Netherlands. In the other three groups, all authors were affiliated with institutions of British origin.
The red circle comprises Bahrs, O., Bensing, J.M., Deveugele, M., Gask, L., Leiva, F., Messerli, V., Oppizzi, I., Peltenburg, M., Perez A., Van den Brink-Muinen, A., and Verhaak, P.F.M. The green circle includes ten authors: Burt, J., Blakeman, T., Hann, M. Kennedy, A., Protheroe, J., Reeves, D., Richardson, G., Rick, J., Rowe, K., and Small, N. On the other hand, the blue cluster comprises Abel, G. together with Bower, P., Campbell, J., Elliott, M., Nissen, S., Paddison, C., Roland, M., and Smith, P. Finally, the fourth cluster, in yellow, is formed by Mcdonals, R., Mead, N., and Whalley, D.
3.1.5. Identification of the Main Research Institutions
Table 6 displays the 13 most productive PS and HP research institutions from 2000 to 2020, concentrated in 4 countries. It is worth noting that 61.54% are British. The United States and Canada have 15.385% each, and Israel has 7.69%. The table shows the data related to the citations and the first and last years of publication for each institution.
The University of Manchester is the institution that leads the ranking, with 14 articles and an h-index of 11. Three of the authors we previously named the most prolific belong to this University, accounting for 6 of the 14 articles published by this institution. Although it has a better h-index, it shares the number of articles with the London School of Hygiene and Tropical Medicine. It does not have better values than the other institutions concerning the rest of the parameters. The number of citations per article is 38.71, and the number of citations from the first year of publication is 27.10.
By considering the number of citations or the number of citations since the first year of publication, the leader in the ranking is the London School of Hygiene and Tropical Medicine. On the other hand, if the analysis is carried out from the number of citations per article, the leader is Imperial College London, with 62.58; this is also the institution to which the eighth-most prolific author belongs (see
Table 5).
Except for Harvard Medical School, which first published in 2012, the institutions included in the ranking published in both analysis periods. Moreover, it is accurate to announce that 7 of the 13 published their last article on PS and HP in 2019. The University of Oxford and Harvard T.H. Chan School of Public Health are the institutions with the most extended history of research on public politics based on patient satisfaction.
London School of Hygiene and Tropical Medicine and Harvard T.H. Chan School of Public Health share second place in the h-index with a value of 9.
3.1.6. Identification of the Most Cited Articles
Table 7 shows the 11 most cited titles during the analysed period, which is a relevant analysis as it reflects the most influential and popular titles in the scientific community. The year of publication, its authors, the total number of citations, and the average number of citations per year since its publication are indicated for each of them.
The success of the article “Systematic review of involving patients in the planning and development of healthcare” [
23] is resounding, whether we analyse it from the point of view of the total number of citations (600) or if we analyse it as citations per year (31.58). It is followed in the ranking by “European patients” [
82] views on the responsiveness of health systems and healthcare providers”, although with a 65% lower number approximately (214 citations).
It should be noted that Blendon, R.J, identified in
Table 5 as one of the most prolific authors, is the author of one of the articles included in
Table 7 within the ranking of the most cited. Its title is “Public trust in physicians—US medicine in international perspective” [
83], and it corresponds to a publication from 2014 that has the highest number of citations per year (20.43) after the leading article. The rest of the articles in this Top 11 are not by authors considered more prolific.
An important fact that reveals the quality of the articles written by the author Coulter, A. is that his only two articles published on PS and HP during the study period are among the most cited. One of these was the one previously identified as the second most cited. The other is in tenth place with 122 citations [
84].
3.2. Content Analysis
As indicated above, we divided the analysis period into two subgroups of 10 years each. The objective is to carry out a better analysis of the research evolution [
65,
85]. Considering it logical that research can change its study objectives over a period of 20 years and show an evolution, dividing the time horizon considered can give us a perspective of the researchers’ interest. The first period includes a total of 232 articles, while the second comprises 389.
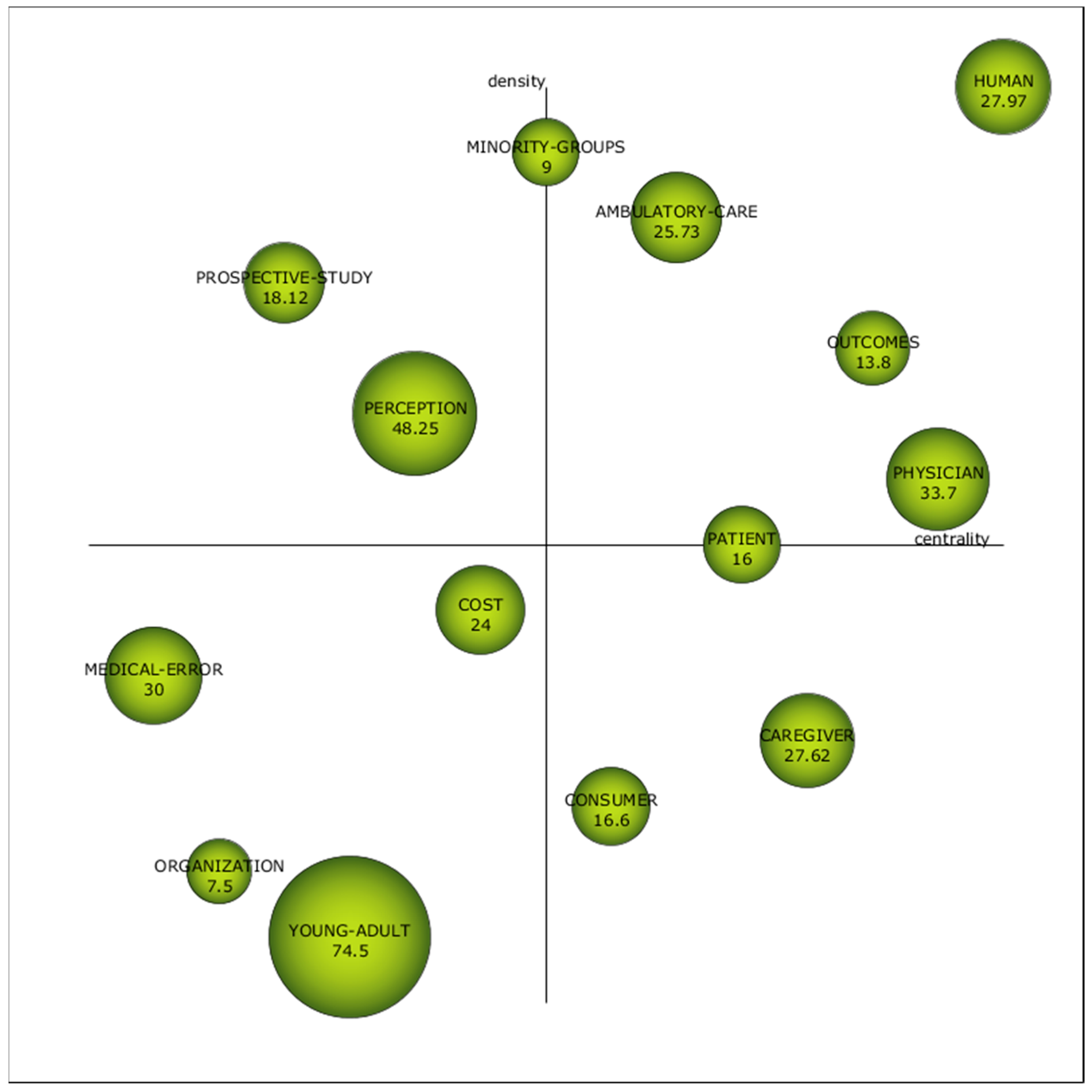
Figure 7 exhibits the strategic diagram of the first sub-period (2000–2010). It illustrates four clearly defined motor keywords: “Human”, “Outcomes”, “Physician”, and “Ambulatory Care”, which, during this first period, were well developed and, therefore, were relevant in the research on PS and HP. Besides, two keywords are at the limit of being considered a motor keyword: “Patients”, whose density is not enough, and “Minority Groups” have a lower centrality than necessary to be regarded as proper motor keywords. These, also called driving themes, are in the upper-right quadrant, and they represent themes extensively developed and essential to shaping the scientific field [
70].
The position of “Physician” is not surprising because most studies analyse patient satisfaction from a medical or nursing perspective, such as clinical preventive services [
86], the communication skills of doctors [
87], and technical quality [
88,
89], among others. In turn, all these aspects significantly influence the “Outcomes” obtained [
90].
For its part, “Human” has total density and centrality, so we could affirm that it is a mature topic broadly connected with the rest of the keywords [
91]. Another topic considered motor is “Ambulatory Care”, which has received particular attention from various authors [
89,
92,
93,
94].
In the reverse sector of the diagram, we find emerging or decaying keywords: “Medical Error”, “Organization”, ”Young-Adult”, and “Cost”, which are not the focus of current research, nor are they mature [
95]. The subdivision of the period will allow us to observe if these issues acquire a better position or, on the contrary, end up disappearing.
Moreover, two basic themes, “Consumer” and “Caregiver”, and two peripheral themes, “Prospective Study” and “Perception”, were also identified. Words located in the upper left quadrant are not currently receiving attention but are potential research areas [
96].
We can highlight the role of “Perception”, which is not yet sufficiently linked to the other research topics on PS and HP, although it is a highly developed topic.
The sphere’s size represents the number of citations per article, which is also indicated on each label.
Table 8 complements
Figure 7, showing the h-index, density, and centrality of the keywords.
The h-index of these keywords is led by two motor themes: “Human”, with 39, and “Physician”, with 17. The third place is shared, with an h-index of 7, a motor keyword (“Ambulatory-care”), and a basic one (“Caregiver”), which is logical because it deals with general or cross-cutting issues in the scientific field.
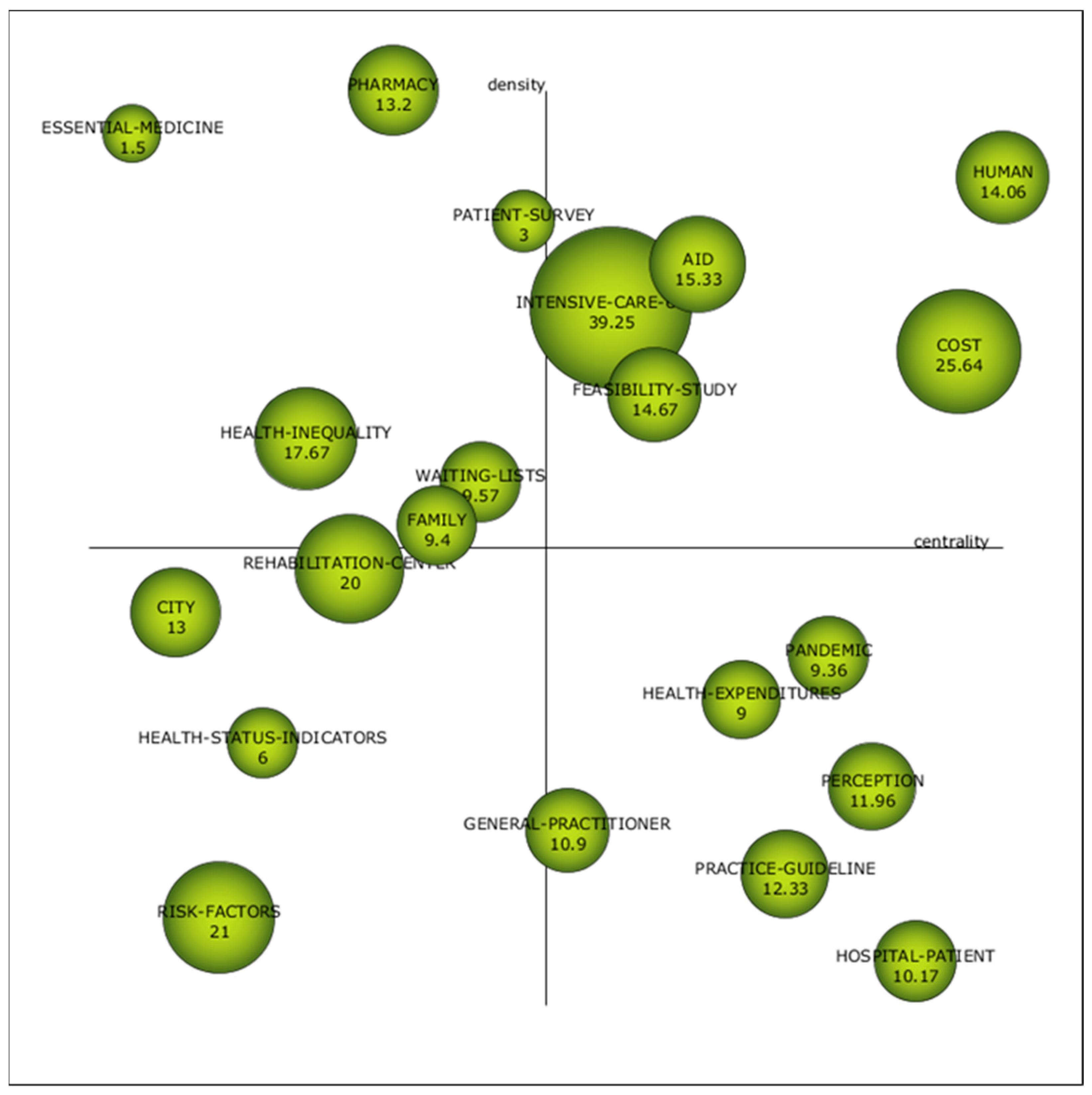
Figure 8 shows the strategic diagram of the second sub-period (2010–2020). It can be seen that the number of keywords has multiplied. Newly appeared are “Intensive Care”, “Feasibility Study”, and “Aid”. The authors identify points for improvement of public policies in different aspects of intensive care. On the one hand, Kasparian, N.A. seeks to develop better practices in paediatric intensive care [
97]. On the other hand, Gunchan, P. studied the relationship between discharges against medical advice and the quality of public policies [
98].
We can also find numerous feasibility studies within the bibliography that find relevant data for public policymakers [
99,
100,
101,
102].
“Human” continues to be a motor keyword with total centrality and 10% less density compared to the first period. “Cost” goes from being an emergent keyword to a motor keyword.
For its part, “Perception” went from being a topic with high density and low centrality to becoming a basic topic, a keyword with high centrality and low density. Although clients’ perception has been studied since the 1950s [
6,
7], the economic crisis of 2008 [
29,
51,
103,
104] may have been a turning point in research on the perception of patients linked to the cost of healthcare.
For the other three topics in the emerging or declining quadrant in the first period, we can confirm they were declining keywords because they disappeared in the second period.
Table 9 complements
Figure 8 by indicating the degree of density and centrality, h-index, and the number of documents and citations for each keyword. In this second period, the keyword with the best h-index continues to be “Human”, with 30. It is followed by the keyword “Perception”, which denotes the importance given to the evaluation of the patients’ opinion. Another keyword that emerges and reveals this to us is “Patient Survey” (keyword that goes hand in hand with “Perception” because it is a method to know it), which is in the peripheral quadrant at the limit with the quadrant of motor keywords.
Table 9 shows relevant data for these terms; for example, “Perception” occurred in 25 papers and had 299 citations.
Besides “Perception”, we also observe the entry of the word “Pandemic” to the quadrant of basic keywords, a product of the health crisis caused by COVID-19. Some investigations are related to the advance in telemedicine that the COVID-19 forced [
105,
106].
The rest of the keywords in the lower right quadrant are compound words. “Health-Patient”, “Practice-Guideline”, and “Health-Expenditures” have a high centrality, which reveals the importance of these issues in the general development of public health policies based on patient satisfaction. Finally, “General-Practitioner” has a medium centrality, to the limit of becoming an emerging theme.
We found four emerging themes, that is, themes with low centrality and low density. They are “Risk-Factors”, “Health-Status-Indicators”, “City”, and “Rehabilitation-Centre”. None of them was found in the first period.
Finally, we highlight keywords with a high density that were highly developed independently in the scientific field analysed. They are ”Pharmacy”, “Essential-Medicine”, “Health Inequality”, “Waiting-List”, “Family”, and, the one already named, “Patient-Survey”.
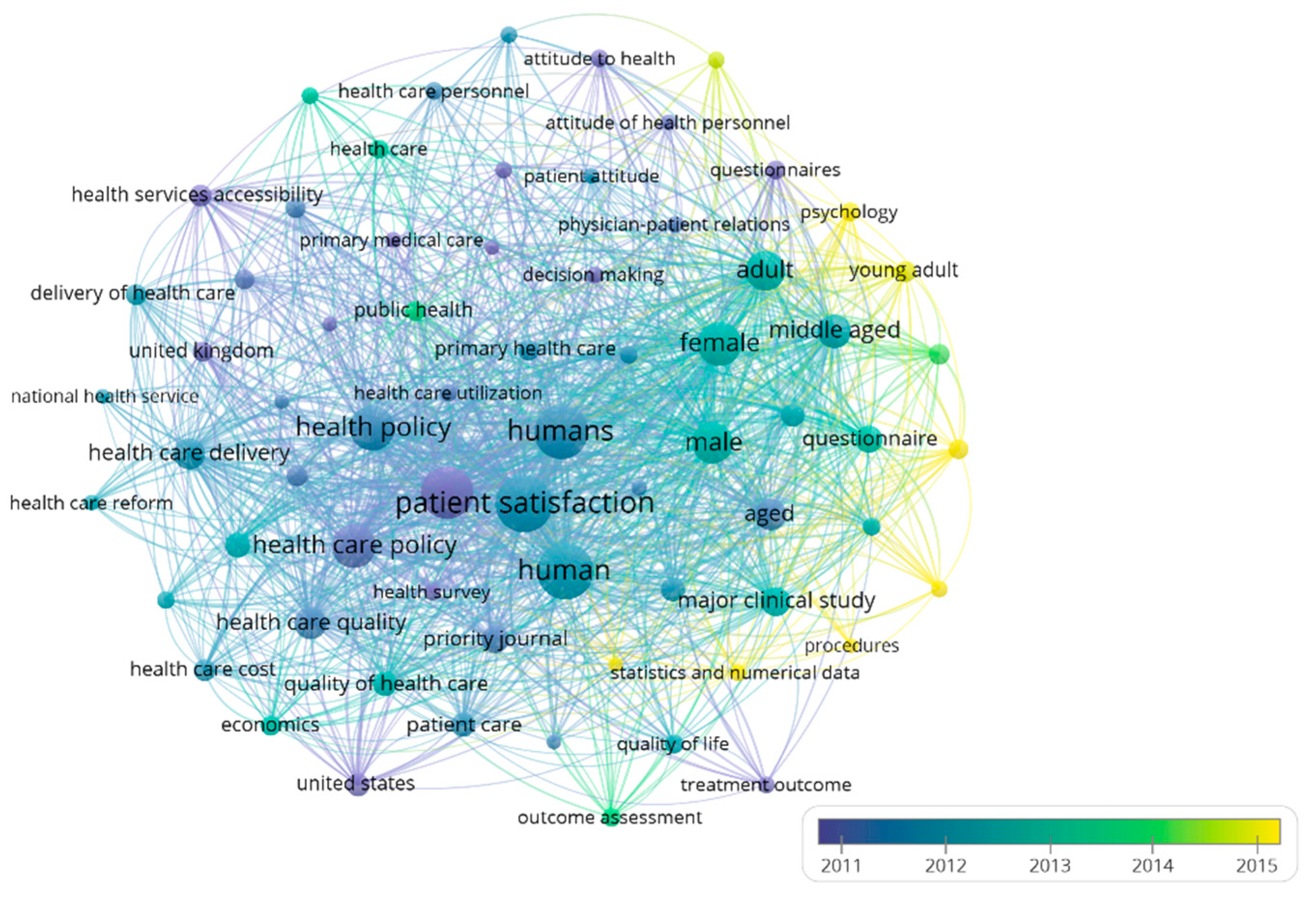
Figure 9 shows the evolution of keywords within the PS and HP research field, complementing the study of trends. For the analysis, only those words that appeared at least 40 times were taken. Blue indicates older terms used in the literature. Instead, the yellow colour represents terms that appeared more recently in the field of research under analysis.
During 2011, the articles were more related to patient satisfaction, healthcare quality, healthcare policy, and health services accessibility. During 2012, many keywords coincided with the previous year, such as the healthcare quality and public health policies. These words constitute a cluster that includes other keywords such as “National Health Service” or “Healthcare reform”.
In 2013, cross-sectional studies appeared as well as studies with gender distinction and outcomes assessment. In 2014, psychological aspects were incorporated into the evaluation of patient satisfaction to formulate public policies. In addition, the studies began to appear with statistical methodologies and numerical data.















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}