
Methoxyflurane in Non-Life-Threatening Traumatic Pain—A Retrospective Observational Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
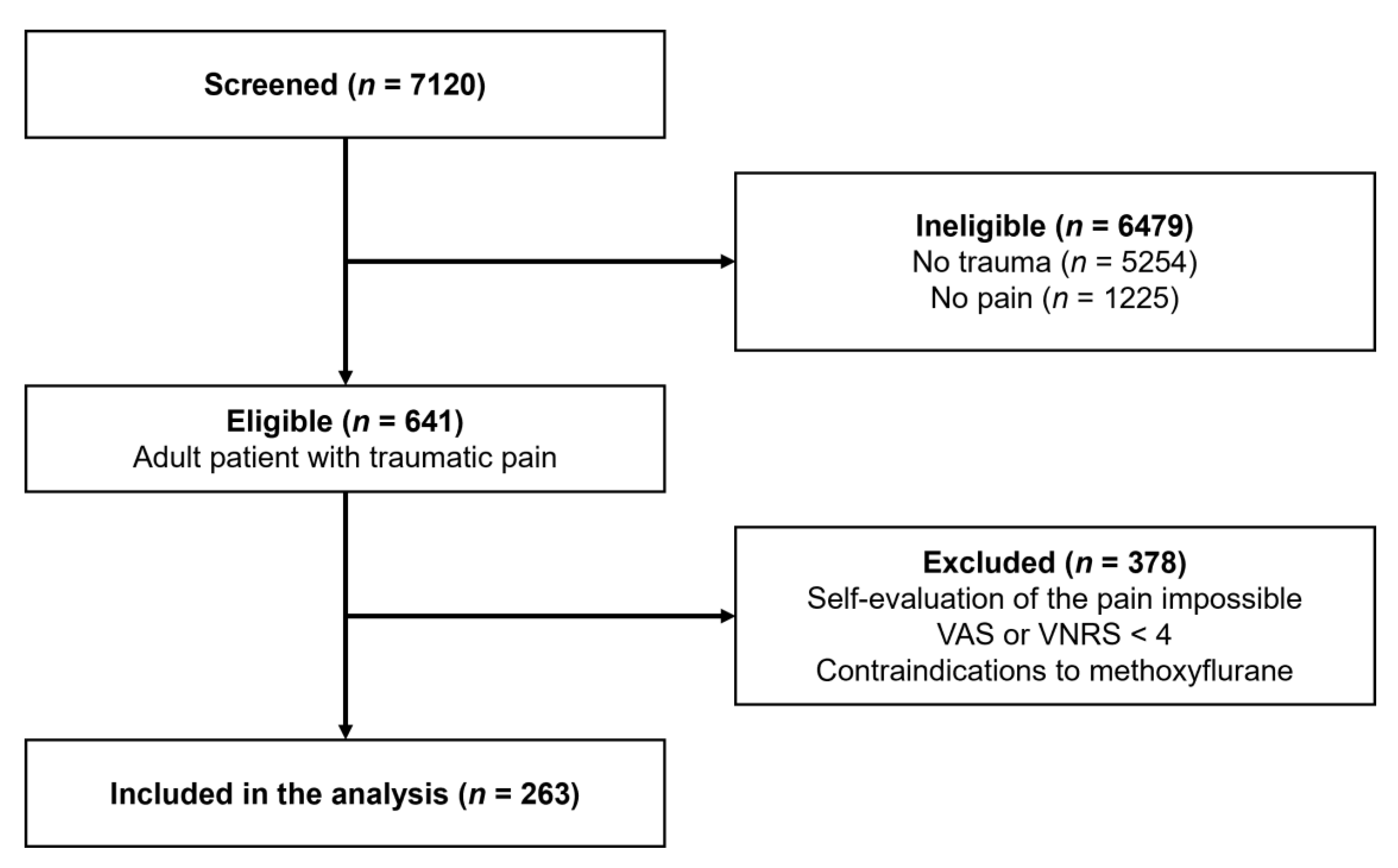
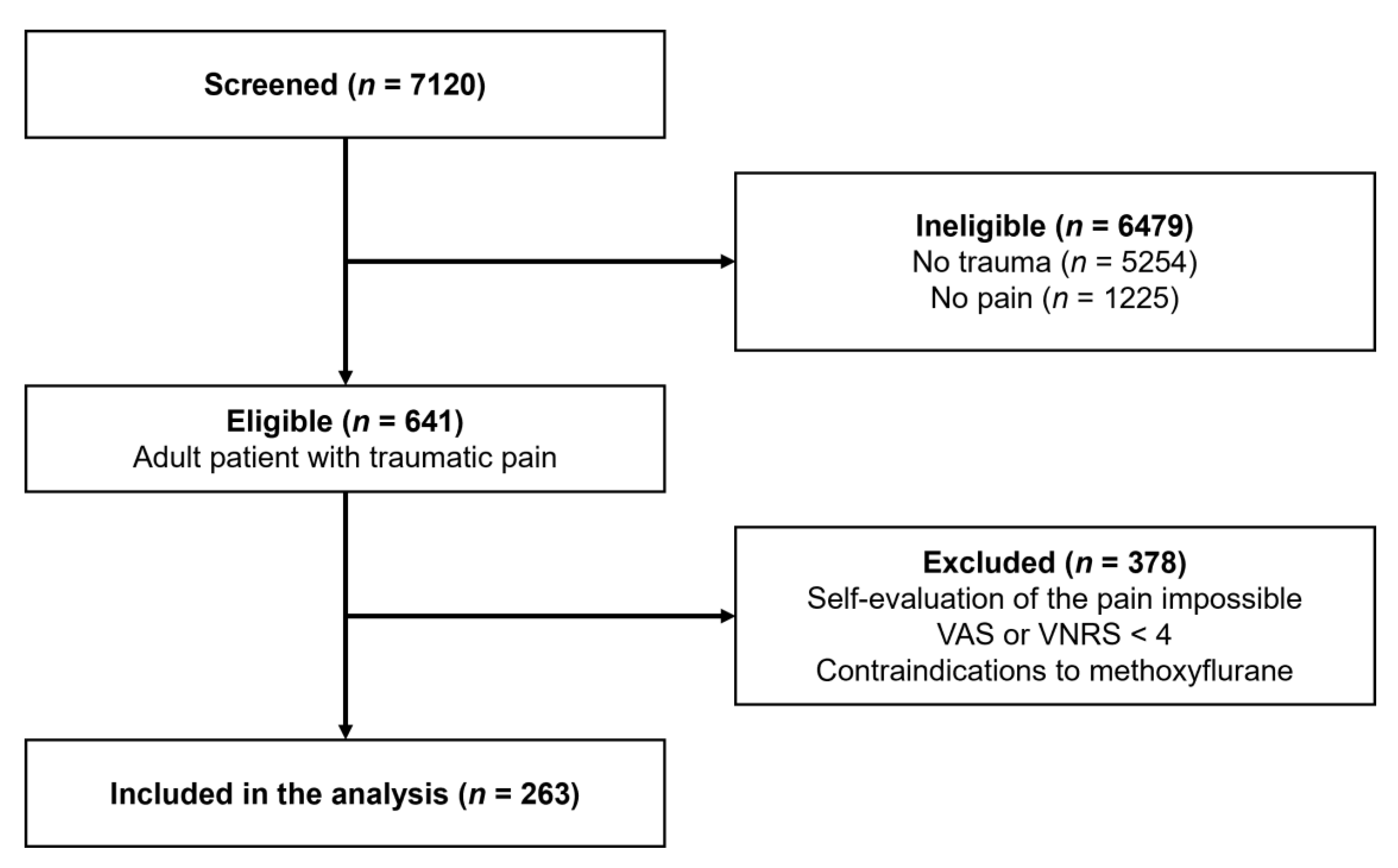
2.2. Inclusion and Exclusion Criteria
2.3. Data Collection
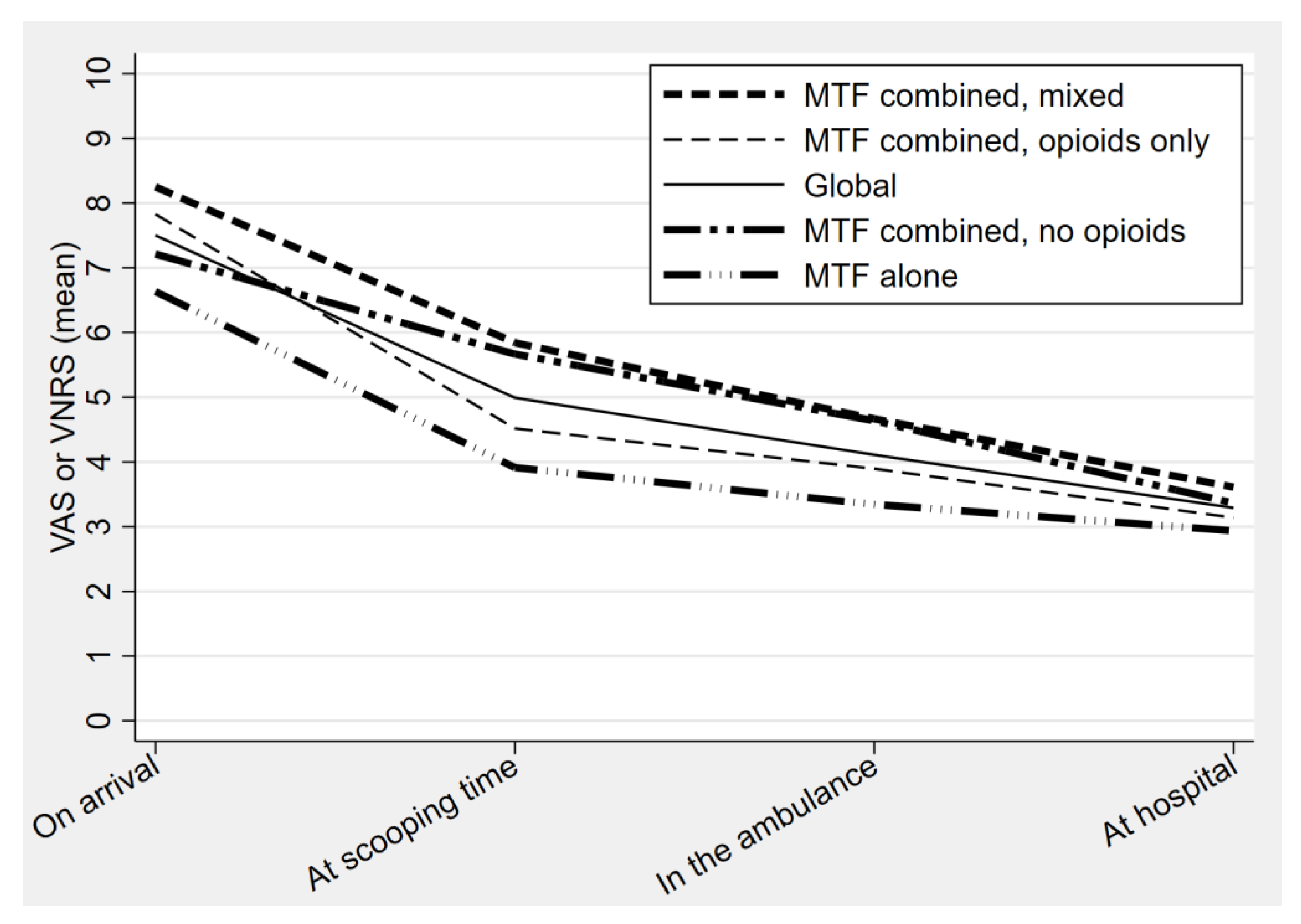
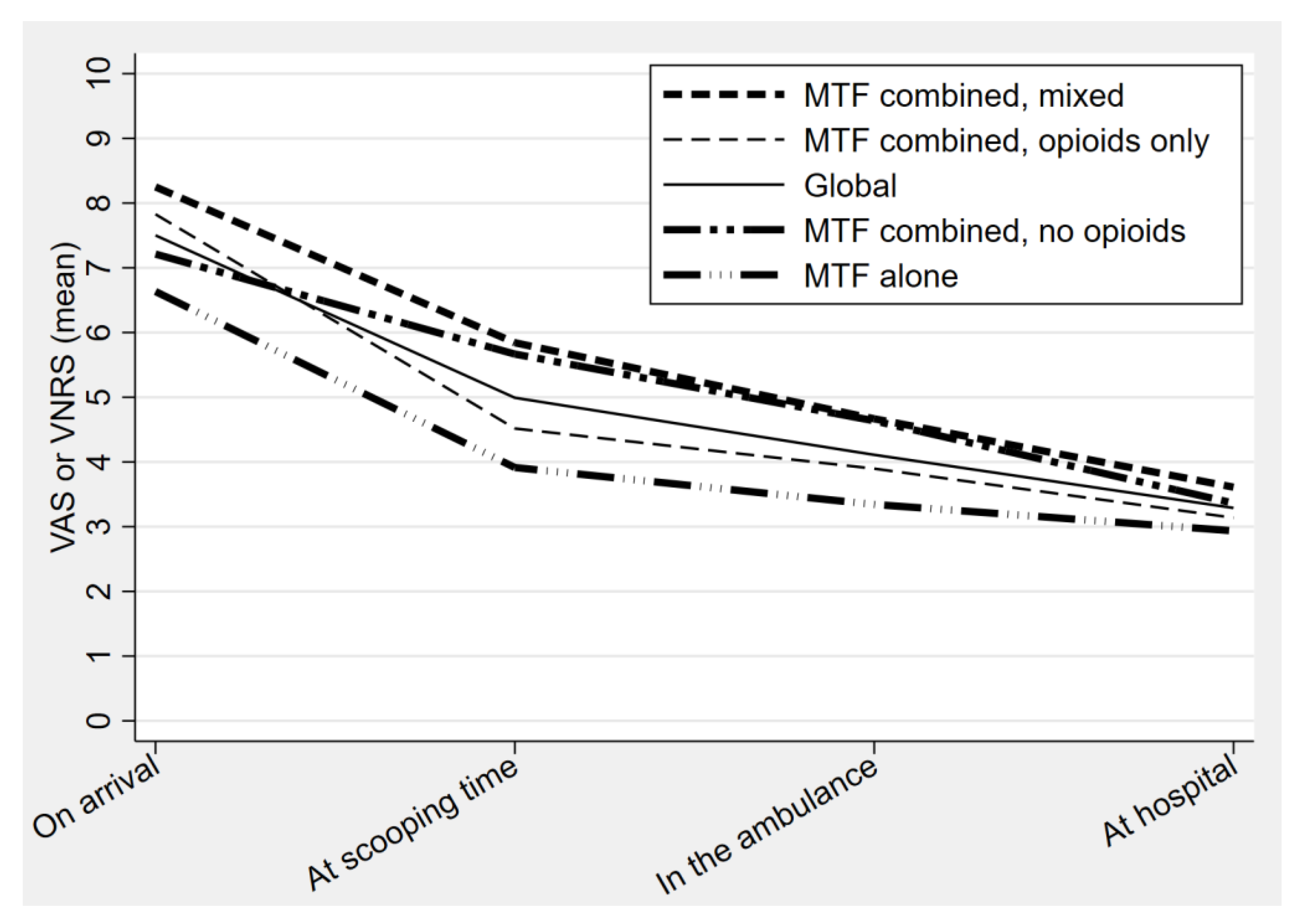
2.4. Outcomes
2.5. Statistical Analysis
2.6. Research Ethics Review
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Galinski, M.; Ruscev, M.; Gonzalez, G.; Kavas, J.; Ameur, L.; Biens, D.; Lapostolle, F.; Adnet, F. Prevalence and management of acute pain in prehospital emergency medicine. Prehospital Emerg. Care 2010, 14, 334–339. [Google Scholar] [CrossRef] [PubMed]
- Berben, S.A.; Schoonhoven, L.; Meijs, T.H.; van Vugt, A.B.; van Grunsven, P.M. Prevalence and relief of pain in trauma patients in emergency medical services. Clin. J. Pain 2011, 27, 587–592. [Google Scholar] [CrossRef] [PubMed]
- Luiz, T.; Scherer, G.; Wickenkamp, A.; Blaschke, F.; Hoffmann, W.; Schiffer, M.; Zimmer, J.; Schaefer, S.; Voigt, C. Prehospital analgesia by paramedics in Rhineland-Palatinate: Feasability, analgesic effectiveness and safety of intravenous paracetamol. Anaesthesist 2015, 64, 927–936. [Google Scholar] [CrossRef] [PubMed]
- Ducasse, J.L.; Siksik, G.; Durand-Bechu, M.; Couarraze, S.; Valle, B.; Lecoules, N.; Marco, P.; Lacombe, T.; Bounes, V. Nitrous oxide for early analgesia in the emergency setting: A randomized, double-blind multicenter prehospital trial. Acad. Emerg. Med. 2013, 20, 178–184. [Google Scholar] [CrossRef]
- Buckland, D.M.; Crowe, R.P.; Cash, R.E.; Gondek, S.; Maluso, P.; Sirajuddin, S.; Smith, E.R.; Dangerfield, P.; Shapiro, G.; Wanka, C.; et al. Ketamine in the Prehospital Environment: A National Survey of Paramedics in the United States. Prehospital Disaster Med. 2018, 33, 23–28. [Google Scholar] [CrossRef] [Green Version]
- Kanowitz, A.; Dunn, T.M.; Kanowitz, E.M.; Dunn, W.W.; Vanbuskirk, K. Safety and effectiveness of fentanyl administration for prehospital pain management. Prehospital Emerg. Care 2006, 10, 1–7. [Google Scholar] [CrossRef]
- Garrick, J.F.; Kidane, S.; Pointer, J.E.; Sugiyama, W.; Van Luen, C.; Clark, R. Analysis of the paramedic administration of fentanyl. J. Opioid Manag. 2011, 7, 229–234. [Google Scholar] [CrossRef]
- Fleischman, R.J.; Frazer, D.G.; Daya, M.; Jui, J.; Newgard, C.D. Effectiveness and safety of fentanyl compared with morphine for out-of-hospital analgesia. Prehospital Emerg. Care 2010, 14, 167–175. [Google Scholar] [CrossRef] [Green Version]
- Bounes, V.; Barthelemy, R.; Diez, O.; Charpentier, S.; Montastruc, J.L.; Ducasse, J.L. Sufentanil is not superior to morphine for the treatment of acute traumatic pain in an emergency setting: A randomized, double-blind, out-of-hospital trial. Ann. Emerg. Med. 2010, 56, 509–516. [Google Scholar] [CrossRef]
- Oyegunle, A.O. Clinical evaluation of methoxyflurane administered through a disposable vaporizer (‘Analgizer’). Niger. Med. J. 1978, 8, 141–144. [Google Scholar]
- Marx, G.F.; Chen, L.K.; Tabora, J.A. Experiences with a disposable inhaler for methoxyflurane analgesia during labour: Clinical and biochemical results. Can. Anaesth. Soc. J. 1969, 16, 66–71. [Google Scholar] [CrossRef]
- Lojo Rial, C.; Ozainne, F.; Fehlmann, C.; Von During, S.; Cottet, P. Acute pain management: The role of inhaled methoxyflurane in clinical practice. Rev. Med. Suisse 2020, 16, 553–556. [Google Scholar]
- Coffey, F.; Wright, J.; Hartshorn, S.; Hunt, P.; Locker, T.; Mirza, K.; Dissmann, P. STOP!: A randomised, double-blind, placebo-controlled study of the efficacy and safety of methoxyflurane for the treatment of acute pain. Emerg. Med. J. 2014, 31, 613–618. [Google Scholar] [CrossRef]
- Mercadante, S.; Voza, A.; Serra, S.; Ruggiano, G.; Carpinteri, G.; Gangitano, G.; Intelligente, F.; Bonafede, E.; Sblendido, A.; Farina, A.; et al. Analgesic Efficacy, Practicality and Safety of Inhaled Methoxyflurane Versus Standard Analgesic Treatment for Acute Trauma Pain in the Emergency Setting: A Randomised, Open-Label, Active-Controlled, Multicentre Trial in Italy (MEDITA). Adv. Ther. 2019, 36, 3030–3046. [Google Scholar] [CrossRef] [Green Version]
- Austin, M.A. Prehospital Analgesia in Adults Using Inhaled Methoxyflurane: A Feasibility Study. 2020. Available online: https://clinicaltrials.gov/ct2/show/NCT04287803 (accessed on 8 August 2021).
- Marinangeli, F.; Reggiardo, G.; Sblendido, A.; Soldi, A.; Farina, A.; Group, M. Prospective, Multicentre Trial of Methoxyflurane for Acute Trauma-Related Pain in Helicopter Emergency Medical Systems and Hostile Environments: Meteora Protocol. Adv. Ther. 2018, 35, 2081–2092. [Google Scholar] [CrossRef] [Green Version]
- Chan, M.; Fehlmann, C.A.; Pasquier, M.; Suppan, L.; Savoldelli, G.L. Endotracheal Intubation Success Rate in an Urban, Supervised, Resident-Staffed Emergency Mobile System: An 11-Year Retrospective Cohort Study. J. Clin. Med. 2020, 9, 238. [Google Scholar] [CrossRef] [Green Version]
- Ismail, A.K.; Abdul Ghafar, M.A.; Shamsuddin, N.S.; Roslan, N.A.; Kaharuddin, H.; Nik Muhamad, N.A. The Assessment of Acute Pain in Pre-Hospital Care Using Verbal Numerical Rating and Visual Analogue Scales. J. Emerg. Med. 2015, 49, 287–293. [Google Scholar] [CrossRef]
- Buntine, P.; Thom, O.; Babl, F.; Bailey, M.; Bernard, S. Prehospital analgesia in adults using inhaled methoxyflurane. Emerg. Med. Australas 2007, 19, 509–514. [Google Scholar] [CrossRef] [PubMed]
- Johnston, S.; Wilkes, G.J.; Thompson, J.A.; Ziman, M.; Brightwell, R. Inhaled methoxyflurane and intranasal fentanyl for prehospital management of visceral pain in an Australian ambulance service. Emerg. Med. J. 2011, 28, 57–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Middleton, P.M.; Simpson, P.M.; Sinclair, G.; Dobbins, T.A.; Math, B.; Bendall, J.C. Effectiveness of morphine, fentanyl, and methoxyflurane in the prehospital setting. Prehospital Emerg. Care 2010, 14, 439–447. [Google Scholar] [CrossRef] [PubMed]
- McManus, J.G., Jr.; Sallee, D.R., Jr. Pain management in the prehospital environment. Emerg. Med. Clin. N. Am. 2005, 23, 415–431. [Google Scholar] [CrossRef] [PubMed]
- Albrecht, E.; Taffe, P.; Yersin, B.; Schoettker, P.; Decosterd, I.; Hugli, O. Undertreatment of acute pain (oligoanalgesia) and medical practice variation in prehospital analgesia of adult trauma patients: A 10 yr retrospective study. Br. J. Anaesth. 2013, 110, 96–106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oberholzer, N.; Kaserer, A.; Albrecht, R.; Seifert, B.; Tissi, M.; Spahn, D.R.; Maurer, K.; Stein, P. Factors Influencing Quality of Pain Management in a Physician Staffed Helicopter Emergency Medical Service. Anesth. Analg. 2017, 125, 200–209. [Google Scholar] [CrossRef]
- Kiavialaitis, G.E.; Muller, S.; Braun, J.; Rossler, J.; Spahn, D.R.; Stein, P.; Kaserer, A. Clinical practice of pre-hospital analgesia: An observational study of 20,978 missions in Switzerland. Am. J. Emerg. Med. 2020, 38, 2318–2323. [Google Scholar] [CrossRef] [PubMed]
- Brichko, L.; Gaddam, R.; Roman, C.; O’Reilly, G.; Luckhoff, C.; Jennings, P.; Smit, D.V.; Cameron, P.; Mitra, B. Rapid Administration of Methoxyflurane to Patients in the Emergency Department (RAMPED) Study: A Randomized Controlled Trial of Methoxyflurane Versus Standard Care. Acad. Emerg. Med. 2021, 28, 164–171. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Variables | All Patients (n = 263) |
|---|---|
| Sex (female)—n (%) | 123 (46.8) |
| Age (years)—mean ± SD | 53.6 ± 22.5 |
| Weekend intervention—n (%) | 55 (20.9) |
| Night intervention—n (%) | 70 (26.6) |
| Place of intervention—n (%) | |
| Public place | 121 (46.0) |
| Home | 85 (32.3) |
| Work/school/sport/leisure | 46 (17.5) |
| Others | 11 (4.2) |
| Pain localisation—n (%) | |
| Lower limb | 119 (45.3) |
| Upper limb | 76 (28.9) |
| Back | 37 (14.1) |
| Thorax | 20 (7.6) |
| Pelvis | 6 (2.3) |
| Skull | 5 (1.9) |
| Systolic blood pressure (mmHg)—mean ± SD | 137 ± 24 |
| Diastolic blood pressure (mmHg)—mean ± SD | 82 ± 15 |
| Heart rate (/min)—mean ± SD | 81 ± 14 |
| Oxygen saturation (%)—mean ± SD | 97 ± 2 |
| Initial VAS or VNRS score—median (IQR) | 7 (6–10) |
| Treatment—n (%) | |
| Methoxyflurane alone | 93 (35.4) |
| Methoxyflurane combined (no opioids) | 29 (11.3) |
| Methoxyflurane combined (opioids only) | 33 (12.5) |
| Methoxyflurane combined (mixed) | 108 (41.1) |
| Outcome | All Patients (n = 263) | MTF 1 Alone (n = 93) | MTF 1 Combined, No Opioids (n = 29) | MTF 1 Combined, Opioids Only (n = 33) | MTF 1 Combined, Mixed (n = 108) |
|---|---|---|---|---|---|
| Pain improvement—mean (95% CI) | 4.2 (3.9–4.5) | 3.7 (3.2–4.2) | 4.7 (3.8–5.6) | 3.8 (2.6–5.1) | 4.6 (4.2–5.1) |
| Successful analgesia—n (%) | 152 (57.8) | 55 (59.1) | 20 (69.0) | 20 (60.6) | 57 (52.8) |
| Modified successful analgesia 2—n (%) | 196 (74.5) | 77 (82.8) | 23 (79.3) | 25 (75.8) | 71 (65.7) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ozainne, F.; Cottet, P.; Lojo Rial, C.; von Düring, S.; Fehlmann, C.A. Methoxyflurane in Non-Life-Threatening Traumatic Pain—A Retrospective Observational Study. Healthcare 2021, 9, 1360. https://doi.org/10.3390/healthcare9101360
Ozainne F, Cottet P, Lojo Rial C, von Düring S, Fehlmann CA. Methoxyflurane in Non-Life-Threatening Traumatic Pain—A Retrospective Observational Study. Healthcare. 2021; 9(10):1360. https://doi.org/10.3390/healthcare9101360
Chicago/Turabian StyleOzainne, Florian, Philippe Cottet, Carlos Lojo Rial, Stephan von Düring, and Christophe A. Fehlmann. 2021. "Methoxyflurane in Non-Life-Threatening Traumatic Pain—A Retrospective Observational Study" Healthcare 9, no. 10: 1360. https://doi.org/10.3390/healthcare9101360
APA StyleOzainne, F., Cottet, P., Lojo Rial, C., von Düring, S., & Fehlmann, C. A. (2021). Methoxyflurane in Non-Life-Threatening Traumatic Pain—A Retrospective Observational Study. Healthcare, 9(10), 1360. https://doi.org/10.3390/healthcare9101360