Immediate Effects of Ankle–Foot Orthosis Using Wire on Static Balance of Patients with Stroke with Foot Drop: A Cross-Over Study



Abstract
1. Introduction
2. Material and Methods
2.1. Patients
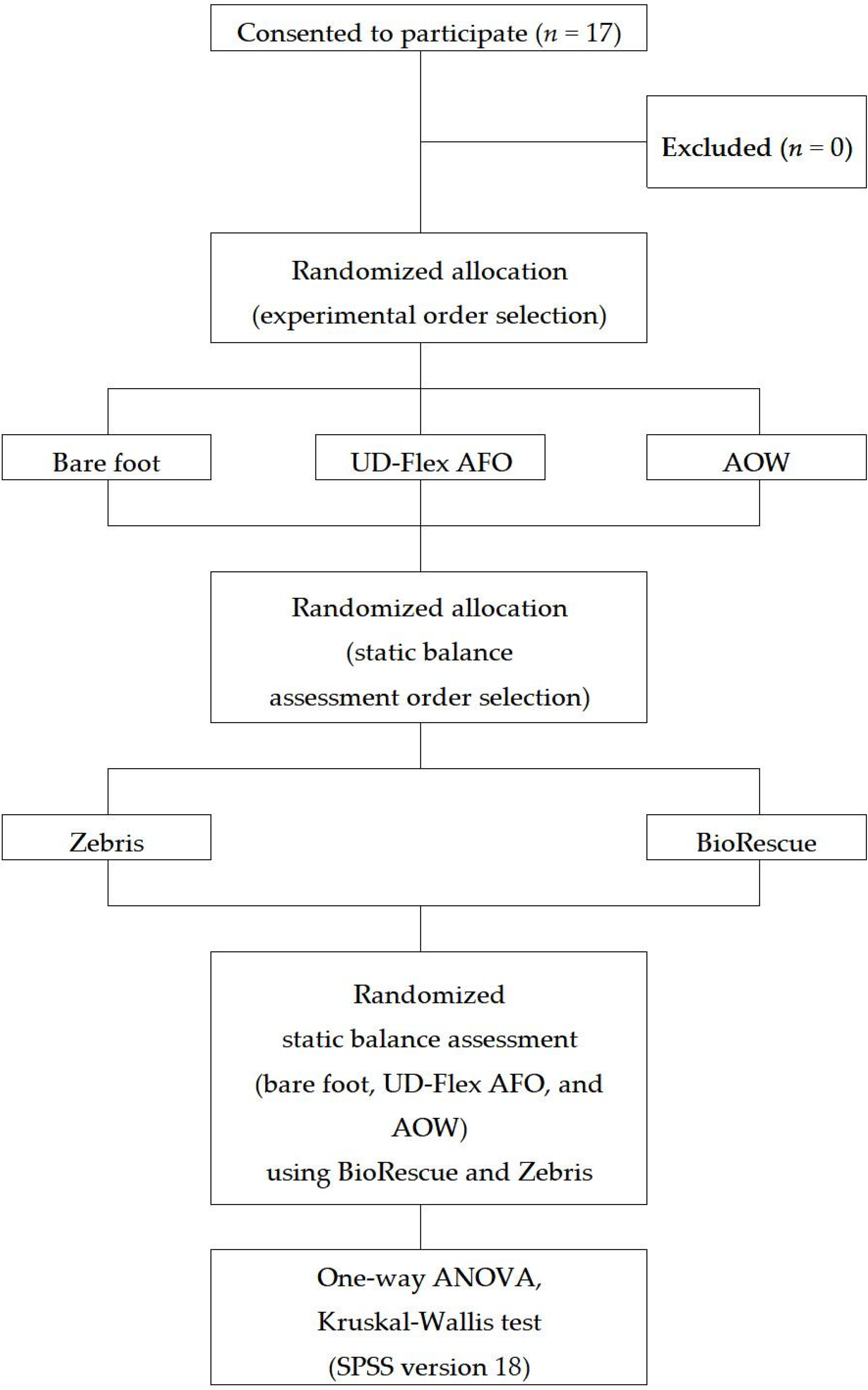
2.2. Study Design
2.3. Measurement
2.4. Orthosis
2.5. Statistical Analysis
3. Results
3.1. Participants’ General Characteristics
3.2. Static Balance Using Zebris
3.3. Static Balance Using BioRescue
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Geurts, A.C.; de Haart, M.; van Nes, I.J.; Duysens, J. A review of standing balance recovery from stroke. Gait Posture 2005, 22, 267–281. [Google Scholar] [CrossRef]
- Smania, N.; Montagnana, B.; Faccioli, S.; Fiaschi, A.; Aglioti, S.M. Rehabilitation of somatic sensation and related deficit of motor control in patients with pure sensory stroke. Arch. Phys. Med. Rehabil. 2003, 84, 1692–1702. [Google Scholar] [CrossRef]
- Langhorne, P.; Coupar, F.; Pollock, A. Motor recovery after stroke: a systematic review. Lancet Neurol. 2009, 8, 741–754. [Google Scholar] [CrossRef]
- Tyson, S.F.; Hanley, M.; Chillala, J.; Selley, A.; Tallis, R.C. Balance disability after stroke. Phys. Ther. 2006, 86, 30–38. [Google Scholar] [CrossRef]
- Vearrier, L.A.; Langan, J.; Shumway-Cook, A.; Woollacott, M. An intensive massed practice approach to retraining balance post-stroke. Gait Posture 2005, 22, 154–163. [Google Scholar] [CrossRef]
- Byun, S.D.; Jung, T.D.; Kim, C.H.; Lee, Y.S. Effects of the sliding rehabilitation machine on balance and gait in chronic stroke patients—a controlled clinical trial. Clin. Rehabil. 2011, 25, 408–415. [Google Scholar] [CrossRef]
- Cheng, P.T.; Chen, C.L.; Wang, C.M.; Hong, W.H. Leg muscle activation patterns of sit-to-stand movement in stroke patients. Am. J. Phys. Med. Rehbil. 2004, 83, 10–16. [Google Scholar] [CrossRef]
- Wade, D.T.; Wood, V.A.; Heller, A.; Maggs, J.; Langton Hewer, R. Walking after stroke: Measurement and recovery over the first 3 months. Scand. J. Rehabil. Med. 1987, 19, 25–30. [Google Scholar]
- Hyndman, D.; Ashburn, A.; Stack, E. Fall events among people with stroke living in the community: Circumstances of falls and characteristics of fallers. Arch. Phys. Med. Rehabil. 2002, 83, 165–170. [Google Scholar] [CrossRef]
- Kararas, M.; Cetin, N.; Bayramoglu, M.; Dilek, A. Truck muscle strength in relation to balance and functional disability in unihemispheric stroke patients. Am. J. Phys. Med. Rehabil. 2004, 83, 81–87. [Google Scholar] [CrossRef]
- Laufer, Y.; Ring, H.; Sprecher, E.; Hausdorff, J.M. Gait in individuals with chronic hemiparesis: One-year follow-up of the effects of a neuroprosthesis that ameliorates foot drop. J. Neurol. Phys. Ther. 2009, 33, 104–110. [Google Scholar] [CrossRef]
- Cho, D.Y.; Park, S.W.; Lee, M.J.; Park, D.S.; Kim, E.J. Effects of robot-assisted gait training on the balance and gait of chronic stroke patients: Focus on dependent ambulators. J. Phys. Ther. Sci. 2015, 27, 3053–3057. [Google Scholar] [CrossRef]
- Eser, F.; Yavuzer, G.; Karakus, D.; Karaoglan, B. The effect of balance training on motor recovery and ambulation after stroke: a randomized controlled trial. Eur. J. Phys. Rehabil. Med. 2008, 44, 19–25. [Google Scholar]
- Jutai, J.; Coulson, S.; Teasell, R.; Bayley, M.; Garland, J.; Mayo, N.; Wood-Dauphinee, S. Mobility assistive device utilization in a prospective study of patients with first-ever stroke. Arch. Phys. Med. Rehabil. 2007, 88, 1268–1275. [Google Scholar] [CrossRef]
- O‘Sullivan, S.B.; Schmitz, T.J. Physical Rehabilitation: Assessment and Treatment, 5th ed.; F.A. Davis Company: Philadelphia, PA, USA, 2007. [Google Scholar]
- Fatone, S.; Gard, S.A.; Malas, B.S. Effect of ankle-foot orthosis alignment and foot-plate length on the gait of adults with poststroke hemiplegia. Arch. Phys. Med. Rehabil. 2009, 90, 810–818. [Google Scholar] [CrossRef]
- Wang, R.Y.; Yen, L.; Lee, C.C.; Lin, P.Y.; Wang, M.F.; Yang, Y.R. Effects of an ankle-foot orthosis on balance performance in patients with hemiparesis of different durations. Clin. Rehabil. 2005, 19, 37–44. [Google Scholar] [CrossRef]
- Cakar, E.; Durmus, O.; Tekin, L.; Dincer, U.; Kiralp, M.Z. The ankle-foot orthosis improves balance and reduces fall risk of chronic spastic hemiparetic patients. Eur. J. Phys. Rehabil. Med. 2010, 46, 363–368. [Google Scholar]
- Doğğan, A.; Mengüllüoğlu, M.; Özgirgin, N. Evaluation of the effect of ankle-foot orthosis use on balance and mobility in hemiparetic stroke patients. Disabil. Rehabil. 2011, 33, 1433–1439. [Google Scholar] [CrossRef]
- Youn, H.K. The Effects of Biodex Balance Training to Affected Side by PLS and UD-Flex Orthosis on Ambulation Speed and Balance Ability in Hemiplegic Patients. Master Thesis, Korea University, Seoul, Korea, 2013. [Google Scholar]
- Mulroy, S.J.; Eberly, V.J.; Gronely, J.K.; Weiss, W.; Newsam, C.J. Effect of AFO design on walking after stroke: Impact of ankle plantar flexion contracture. Prosthet. Orthot. Int. 2010, 34, 277–292. [Google Scholar] [CrossRef]
- Everaert, D.G.; Stein, R.B.; Abrams, G.M.; Dromerick, A.W.; Francisco, G.E.; Hafner, B.J.; Huskey, T.N.; Munin, M.C.; Nolan, K.J.; Kufta, C.V. Effect of a foot-drop stimulator and ankle-foot orthosis on walking performance after stroke: a multicenter randomized controlled trial. Neurorehabil. Neural Repair 2013, 27, 579–591. [Google Scholar] [CrossRef]
- Sherk, K.A.; Sherk, V.D.; Anderson, M.A.; Bemben, D.A.; Bemben, M.G. Lower limb neuromuscular function and blood flow characteristics in AFO using survivors of stroke. J. Geriatr. Phys. Ther. 2015, 38, 56–61. [Google Scholar] [CrossRef] [PubMed]
- Janssen, W.G.; Bussmann, H.B.; Stam, H.J. Determinants of the sit-to-stand movement: A review. Phys. Ther. 2002, 82, 866–879. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Routledge: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Kalron, A.; Fonkatz, I.; Frid, L.; Baransi, H.; Achiron, A. The effect of balance training on postural control in people with multiple sclerosis using the CAREN virtual reality system: A pilot randomized controlled trial. J. Neuroeng. Rehabil. 2016, 13, 13. [Google Scholar] [CrossRef]
- Roerdink, M.; De Haart, M.; Daffertshofer, A.; Donker, S.F.; Geurts, A.C.; Beek, P.J. Dynamical structure of center-of-pressure trajectories in patients recovering from stroke. Exp. Brain. Res. 2006, 174, 256–269. [Google Scholar] [CrossRef]
- Pau, M.; Arippa, F.; Leban, B.; Corona, F.; Ibba, G.; Todde, F.; Scorcu, M. Relationship between static and dynamic balance abilities in Italian professional and youth league soccer players. Phys. Ther. Sport. 2015, 16, 236–241. [Google Scholar] [CrossRef] [PubMed]
- Kim, N.H.; Cha, Y.J. Effect of gait training with constrained-induced movement therapy (CIMT) on the balance of stroke patients. J. Phys. Ther. Sci. 2015, 27, 611–613. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Weng, C.; Liu, M.; Wang, Q.; Liu, L.; He, Y. Effect of whole-body vibration exercise on mobility, balance ability and general health status in frail elderly patients: A pilot randomized controlled trial. Clin. Rehabil. 2014, 28, 59–68. [Google Scholar] [CrossRef]
- Geronimi, M. Reproductibilité intra-et intersessions du test des limites de stabilité sur plateforme podobarométrique. Neurophysiol. Clin. Neurophysiol. 2014, 44, 139. [Google Scholar] [CrossRef]
- Delafontaine, A.; Gagey, O.; Colnaghi, S.; Do, M.C.; Honeine, J.L. Rigid ankle foot orthosis deteriorates mediolateral balance control and vertical braking during gait initiation. Front. Hum. Neurosci. 2017, 28, 214. [Google Scholar] [CrossRef]
- Kim, J.H.; Sim, W.S.; Won, B.H. Effectiveness of elastic band-type ankle-foot orthoses on postural control in poststroke elderly patients as determined using combined measurement of the stability index and body weight-bearing ratio. Clin. Interv. Aging. 2015, 13, 1839–1847. [Google Scholar] [CrossRef][Green Version]
- Lin, P.Y.; Yang, Y.R.; Cheng, S.J.; Wang, R.Y. The relation between ankle impairments and gait velocity and symmetry in people with stroke. Arch. Phys. Med. Rehabil. 2006, 87, 562–568. [Google Scholar] [CrossRef]
- Yildizgoren, M.T.; Velioglu, O.; Demetgul, O.; Turhanoglu, A.D. Assessment of the anterior talofibular ligament thickness in patients with chronic stroke: An ultrasonographic study. J. Med. Ultrasound 2017, 25, 145–149. [Google Scholar] [CrossRef]
- Saltzman, C.L.; Nawoczenski, D.A. Complexities of foot architecture as a base of support. J. Orthop. Sports Phys. Ther. 1995, 21, 354–360. [Google Scholar] [CrossRef]
- Chung, S.G.; Van Rey, E.; Bai, Z.; Roth, E.J.; Zhang, L.Q. Biomechanic changes in passive properties of hemiplegic ankles with spastic hypertonia. Arch. Phys. Med. Rehabil. 2004, 85, 1638–1646. [Google Scholar] [CrossRef]
- Sahrmann, S.A. Movement System Impairment Syndromes of the Extremities, Cervical and Thoracic Spines; Mosby: St. Louis, MO, USA, 2010. [Google Scholar]
- Willems, T.M.; Witvrouw, E.; Delbaere, K.; Mahieu, N.; De Bourdeaudhuij, I.; De Clercq, D. Intrinsic risk factors for inversion ankle sprains in male subjects: A prospective study. Am. J. Sports Med. 2005, 33, 415–423. [Google Scholar] [CrossRef]
- Daher, N.; Lee, S.J.; Yang, Y.J. Effects of elastic band orthosis (aider) on balance and gait in chronic stroke patients. Phys. Ther. Rehabil. Sci. 2013, 2, 81–86. [Google Scholar] [CrossRef]
- Lee, J.; Kim, J.O.; Lee, B.H. The effect of posterior talar glide with dorsiflexion on the ankle on mobility, muscle strength and balance in stroke patients: A randomized controlled trial. J. Phys. Ther. Sci. 2017, 29, 452–456. [Google Scholar] [CrossRef]
- Kang, M.H.; Kim, J.W.; Kim, M.H.; Park, T.J.; Park, J.H.; Oh, J.S. Influence of walking with talus taping on the ankle dorsiflexion passive range of motion. J. Phys. Ther. Sci. 2013, 25, 1011–1013. [Google Scholar] [CrossRef][Green Version]
- Park, D.; Lee, J.H.; Kang, T.W.; Cynn, H.S. Immediate effects of talus-stabilizing taping on balance and gait parameters in patients with chronic stroke: A cross-sectional study. Top Stroke Rehabil. 2018, 25, 417–423. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Mean ± SD or Mode (%) |
|---|---|
| Sex | |
| Male | 8 (47.1) |
| Female | 9 (52.9) |
| Age (years) | 53.94 ± 14.65 |
| Height (cm) | 166.18 ± 9.47 |
| Weight (kg) | 64.76 ± 10.61 |
| Diagnosis | |
| Infarction | 11 (64.7) |
| Hemorrhage | 4 (23.5) |
| Tumor | 2 (11.8) |
| Affected side | |
| Right | 10 (58.8) |
| Left | 7 (41.2) |
| Modified Ashworth Scale | 1.29 (0.47) |
| The duration of stroke (month) | 12.29 (7.03) |
| Foot size (mm) | 253.82 (12.81) |
| Orthosis | |
| UD-Flex AFO | 16 (94.1) |
| Elastic band | 1 (5.9) |
| Variables | Bare Foot | UD-Flex AFO | AOW | p-Value |
|---|---|---|---|---|
| COP path length (mm) | 484.47 ± 208.42 | 414.59 ± 144.43 | 318.29 ± 157.60 | 0.025 |
| Variables | Bare Foot | UD-Flex AFO | AOW | p-Value |
|---|---|---|---|---|
| Surface area ellipse (mm2) | 241.35 ± 153.76 | 277.41 ± 381.83 | 68.06 ± 48.98 | 0.001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.-H.; Choi, I.-R.; Choi, H.-S. Immediate Effects of Ankle–Foot Orthosis Using Wire on Static Balance of Patients with Stroke with Foot Drop: A Cross-Over Study. Healthcare 2020, 8, 116. https://doi.org/10.3390/healthcare8020116
Lee J-H, Choi I-R, Choi H-S. Immediate Effects of Ankle–Foot Orthosis Using Wire on Static Balance of Patients with Stroke with Foot Drop: A Cross-Over Study. Healthcare. 2020; 8(2):116. https://doi.org/10.3390/healthcare8020116
Chicago/Turabian StyleLee, Jung-Hoon, Im-Rak Choi, and Hyun-Su Choi. 2020. "Immediate Effects of Ankle–Foot Orthosis Using Wire on Static Balance of Patients with Stroke with Foot Drop: A Cross-Over Study" Healthcare 8, no. 2: 116. https://doi.org/10.3390/healthcare8020116
APA StyleLee, J.-H., Choi, I.-R., & Choi, H.-S. (2020). Immediate Effects of Ankle–Foot Orthosis Using Wire on Static Balance of Patients with Stroke with Foot Drop: A Cross-Over Study. Healthcare, 8(2), 116. https://doi.org/10.3390/healthcare8020116