Recruitment Strategies for a Randomised Controlled Trial Comparing Fast Versus Slow Weight Loss in Postmenopausal Women with Obesity—The TEMPO Diet Trial

 , , ,
, , , 
 and
and
Abstract
1. Introduction
2. Methods
2.1. Ethics
2.2. Recruitment of Potential Participants
2.3. E-mail Screening
- Do you live in the Sydney metropolitan area?
- Are you female?
- Are you 45–65 years of age?
- Are you at least 5 years postmenopausal?
- Are you free from diabetes?
- Do you have a body mass index (BMI) of 30–40 kg/m2?
2.4. Telephone Screening
2.5. Face-To-Face Medical Screening
2.6. Interventions
3. Results
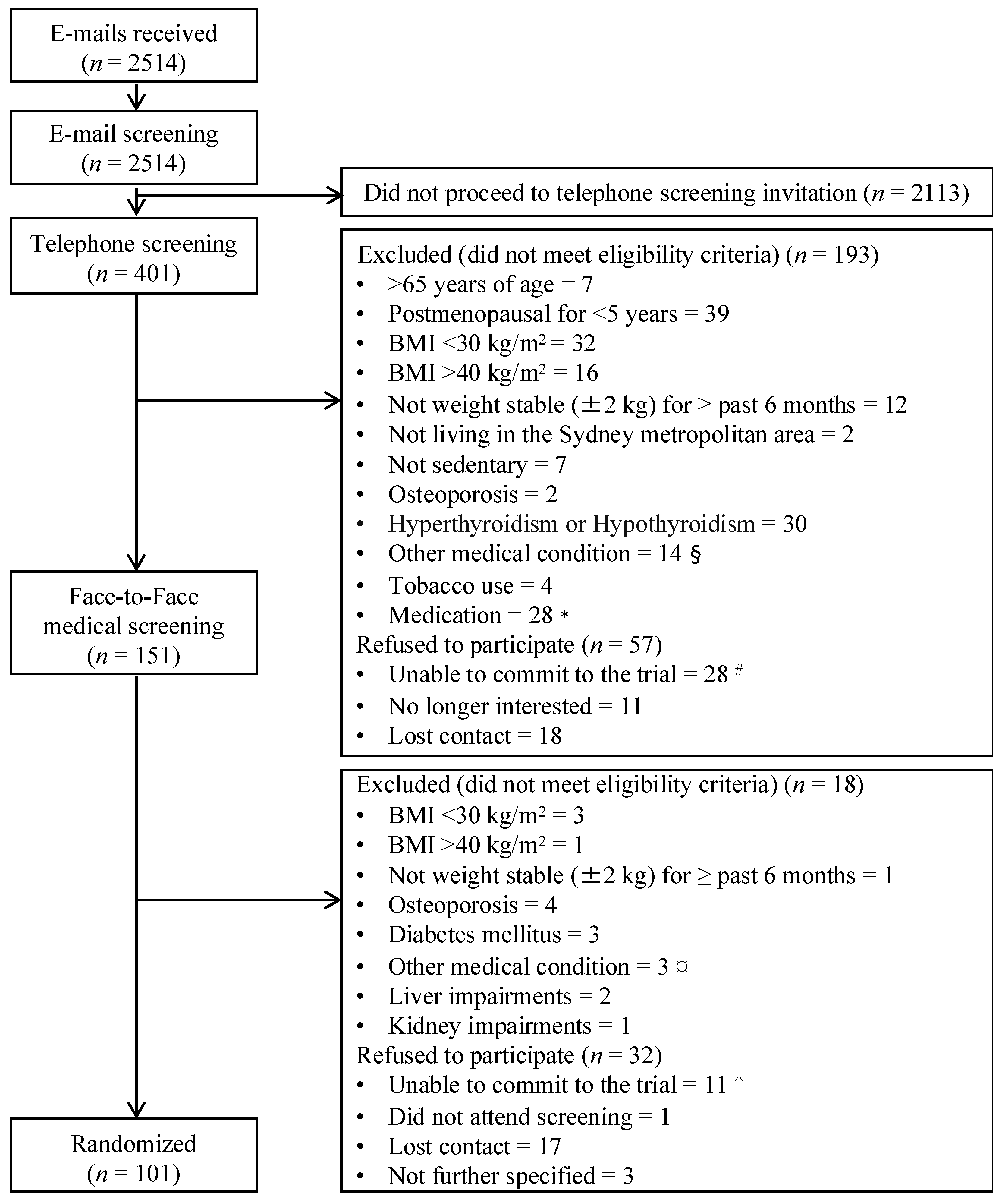
3.1. Participant Recruitment
3.2. Recruitment Strategies
3.3. Time or Monetary Cost per Randomised Participant, and Yield of Recruitment Strategies
3.4. Level of Detail Provided in Recruitment Strategies and Impact on Time Cost per Randomised Participant
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Davis, S.R.; Castelo-Branco, C.; Chedraui, P.; Lumsden, M.A.; Nappi, R.E.; Shah, D.; Villaseca, P. Understanding weight gain at menopause. Climacteric 2012, 15, 419–429. [Google Scholar] [CrossRef] [PubMed]
- Baker, A.; Sirois-Leclerc, H.; Tulloch, H. The impact of long-term physical activity interventions for overweight/obese postmenopausal women on adiposity indicators, physical capacity, and mental health outcomes: A systematic review. J. Obes. 2016, 2016, 6169890. [Google Scholar] [CrossRef] [PubMed]
- Afshin, A.; Forouzanfar, M.H.; Reitsma, M.B.; Sur, P.; Estep, K.; Lee, A.; Marczak, L.; Mokdad, A.H.; Moradi-Lakeh, M.; Naghavi, M.; et al. Health effects of overweight and obesity in 195 countries over 25 years. N. Engl. J. Med. 2017, 377, 13–27. [Google Scholar] [PubMed]
- Hassan, Y.; Head, V.; Jacob, D.; Bachmann, M.O.; Diu, S.; Ford, J. Lifestyle interventions for weight loss in adults with severe obesity: A systematic review. Clin. Obes. 2016, 6, 395–403. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, B.; Gheorghe, A.; Moore, D.; Wilson, S.; Damery, S. Improving the recruitment activity of clinicians in randomised controlled trials: A systematic review. BMJ Open 2012, 2, e000496. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.T.; Jayadeva, V.; Cizza, G.; Brown, R.J.; Nandagopal, R.; Rodriguez, L.M.; Rother, K.I. Challenging recruitment of youth with type 2 diabetes into clinical trials. J. Adolesc. Health 2014, 54, 247–254. [Google Scholar] [CrossRef] [PubMed]
- Robinson, L.; Adair, P.; Coffey, M.; Harris, R.; Burnside, G. Identifying the participant characteristics that predict recruitment and retention of participants to randomised controlled trials involving children: A systematic review. Trials 2016, 17, 294. [Google Scholar] [CrossRef] [PubMed]
- Lindenstruth, K.A.; Curtis, C.B.; Allen, J.K. Recruitment of African American and white postmenopausal women into clinical trials: The beneficial effects of soy trial experience. Ethn. Dis. 2006, 16, 938–942. [Google Scholar] [PubMed]
- Butt, D.A.; Lock, M.; Harvey, B.J. Effective and cost-effective clinical trial recruitment strategies for postmenopausal women in a community-based, primary care setting. Contemp. Clin. Trials 2010, 31, 447–456. [Google Scholar] [CrossRef] [PubMed]
- Warner, E.T.; Glasgow, R.E.; Emmons, K.M.; Bennett, G.G.; Askew, S.; Rosner, B.; Colditz, G.A. Recruitment and retention of participants in a pragmatic randomized intervention trial at three community health clinics: Results and lessons learned. BMC Public Health 2013, 13, 192. [Google Scholar] [CrossRef] [PubMed]
- City of Sydney. Metropolitan Sydney. Available online: www.cityofsydney.nsw.gov.au/learn/research-and-statistics/the-city-at-a-glance/metropolitan-sydney (accessed on 12 February 2017).
- Australian Bureau of Statistics. Frequently Asked Questions: How Does the Abs Define Metropolitan and Non-Metropolitan? Available online: www.abs.gov.au/websitedbs/d3310114.nsf/home/frequently+asked+questions#Anchor8 (accessed on 12 February 2017).
- American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care 2014, 37 (Suppl. 1), S81–S90. [Google Scholar]
- Gibson, A.A.; Seimon, R.V.; Franklin, J.; Markovic, T.P.; Byrne, N.M.; Manson, E.; Caterson, I.D.; Sainsbury, A. Fast versus slow weight loss: Development process and rationale behind the dietary interventions for the tempo diet trial. Obes. Sci. Pract. 2016, 2, 162–173. [Google Scholar] [CrossRef] [PubMed]
- Bryson, J.M.; King, S.E.; Burns, C.M.; Baur, L.A.; Swaraj, S.; Caterson, I.D. Changes in glucose and lipid metabolism following weight loss produced by a very low calorie diet in obese subjects. Int. J. Obes. Relat. Metab. Disord. 1996, 20, 338–345. [Google Scholar] [PubMed]
- Byrne, N.M.; Meerkin, J.D.; Laukkanen, R.; Ross, R.; Fogelholm, M.; Hills, A.P. Weight loss strategies for obese adults: Personalized weight management program vs. Standard care. Obesity 2006, 14, 1777–1788. [Google Scholar] [CrossRef] [PubMed]
- McMillan-Price, J.; Petocz, P.; Atkinson, F.; O’Neill, K.; Samman, S.; Steinbeck, K.; Caterson, I.; Brand-Miller, J. Comparison of 4 diets of varying glycemic load on weight loss and cardiovascular risk reduction in overweight and obese young adults: A randomized controlled trial. Arch. Intern. Med. 2006, 166, 1466–1475. [Google Scholar] [CrossRef] [PubMed]
- Krusche, A.; Rudolf von Rohr, I.; Muse, K.; Duggan, D.; Crane, C.; Williams, J.M. An evaluation of the effectiveness of recruitment methods: The staying well after depression randomized controlled trial. Clin. Trials 2014, 11, 141–149. [Google Scholar] [CrossRef] [PubMed]
- Chin Feman, S.P.; Nguyen, L.T.; Quilty, M.T.; Kerr, C.E.; Nam, B.H.; Conboy, L.A.; Singer, J.P.; Park, M.; Lembo, A.J.; Kaptchuk, T.J.; et al. Effectiveness of recruitment in clinical trials: An analysis of methods used in a trial for irritable bowel syndrome patients. Contemp. Clin. Trials 2008, 29, 241–251. [Google Scholar] [CrossRef] [PubMed]
- Tate, D.F.; LaRose, J.G.; Griffin, L.P.; Erickson, K.E.; Robichaud, E.F.; Perdue, L.; Espeland, M.A.; Wing, R.R. Recruitment of young adults into a randomized controlled trial of weight gain prevention: Message development, methods, and cost. Trials 2014, 15, 326. [Google Scholar] [CrossRef] [PubMed]
- Lam, E.; Partridge, S.R.; Allman-Farinelli, M. Strategies for successful recruitment of young adults to healthy lifestyle programmes for the prevention of weight gain: A systematic review. Obes. Rev. 2016, 17, 178–200. [Google Scholar] [CrossRef] [PubMed]
- Frandsen, M.; Thow, M.; Ferguson, S.G. The effectiveness of social media (facebook) compared with more traditional advertising methods for recruiting eligible participants to health research studies: A randomized, controlled clinical trial. JMIR Res. Protoc. 2016, 5, e161. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Inclusion Criteria | E-mail Screening | Telephone Screening | Face-To-Face Medical Screening |
|---|---|---|---|
| Female | X | X | X |
| 45–65 years of age | X | X | X |
| Postmenopausal for ≥5 years (calculated from date of last menses) | X | X | X |
| Body Mass Index (BMI) 30–40 kg/m2 | X | X | X |
| Weight stable (±2 kg) for ≥past 6 months | X | X | |
| English-speaking | X | ||
| Living in the Sydney metropolitan area (defined by the City of Sydney Statistical Division [11,12]) and able to attend all in-person appointments at the University of Sydney Camperdown campus | X | X | |
| Sedentary (defined as <3 h of structured physical activity per week) | X | X | |
| Asked if they were capable of completing activities required for the trial (e.g., keeping a food, activity and sleep diary, wearing accelerometers for 7 days at a time, etc.) | X * | ||
| Exclusion Criteria | |||
| Not ambulatory, or having restrictions to physical movement that would impede completion of trial activities | X | X | |
| Osteoporosis | X | ||
| Extreme anaemia that could be exacerbated by the fast weight loss intervention (very low energy diet) to be used in the trial | X | ||
| Hyperthyroidism or hypothyroidism | X | ||
| Diabetes mellitus (defined by self-report during e-mail screening and by fasting blood glucose level ≥7.0 mmol/L and glycated haemoglobin (HbA1c) ≥ 6.5% at the face-to-face medical screening) [13] | X | X | |
| Cardiovascular disease | X | ||
| Gastrointestinal disease | X | ||
| Previous gastric or other surgery that may affect appetite | X | ||
| Any loose metal in the body (e.g., pacemaker or bullet) that is contraindicated for magnetic resonance imaging for safety reasons, or which may result in artefacts in medical imaging | X | X | |
| Planning to undertake any major surgery in the next three years | X | ||
| Tobacco use | X | ||
| Alcohol or drug dependency | X | ||
| Taking medication that affects heart rate, body composition or bone mass (e.g., beta-blockers, glucocorticoids) | X | X | |
| Having taken anti-resorptive therapy within the last 3 years | X | X | |
| Having taken medication that affects appetite, metabolism, or weight within the past 6 months | X | X | |
| Any of the following contraindications for following a total meal replacement diet: lactose intolerance; following a strict vegan diet; or unwillingness to be randomised to one of the two diets | X | X | |
| Donated whole blood within 3 months prior to trial commencement | X | ||
| Liver or kidney impairments (which may render fast weight loss unsuitable) | X |
| Strategies | Description | Number of Instances Used | Total Response n (% of Total Response from all Strategies) | Screened n (% of Total Responses from Strategy) | Eligible n (% of Total Responses from Strategy) | Randomised n (% of Total Responses from Strategy) | Total Time Invested (Active Recruitment/Correspondence Time) (hours) | Time cost per Randomised Participant * (hours) |
|---|---|---|---|---|---|---|---|---|
| All strategies | - | 2514 (100.0) | 401 (16.0) | 151 (6.0) | 101 (4.0) | 1828 (828/1000) | 18 | |
Other
| Informally used throughout the trial through individuals directly involved with the trial (researchers, students, volunteers, ineligible participants and enrolled participants) and indirect associates (health practitioners, family, friends, acquaintances who may have learnt about the trial through the other recruitment strategies). | Continuous | 29 (1.2) | 17 (58.6) | 11 (37.9) | 5 (17.2) | 10 (NA/10) | 2 |
| Individuals did not specify or could not recall their source of information in their initial enquiry. | - | 1009 (40.1) | 156 (15.5) | 44 (4.4) | 26 (2.6) | 401 (NA/401) | 15 |
| Free publicity on radio and TV (total) | TV and radio programs that invited trial researchers to provide commentary on health topics featured a free advertorial about the trial in exchange for accepting the interview. The suggested content of advertorials included brief description of the trial and trial e-mail address, which was announced verbally on air or as a web link on the channel website. | 9 | 58 (2.3) | 21 (36.2) | 16 (27.6) | 15 (25.9) | 65 (42/23) | 4 |
| Trial recruitment information was mentioned on radio stations 2GB and ABC, during/at the end of segments involving guest researcher and was included on the radio station website. | 6 | 17 (0.7) | 8 (47.1) | 8 (47.1) | 8 (47.1) | 25 (18/7) | 3 |
| Brief advertisement was included for stories about weight loss and health featuring trial researchers. | 3 | 41 (1.6) | 13 (31.7) | 8 (19.5) | 7 (17.1) | 40 (24/16) | 6 |
| Print media (total) | Printed advertorials in magazines and a local newspaper, and flyers. | - | 78 (3.1) | 61 (78.2) | 40 (51.3) | 22 (28.2) | 588 (556/32) | 27 |
| Commercial advertisements included as part of magazine and newspaper articles featuring expert commentary from trial researchers. Advertisements were free of charge in exchange for providing expert commentary. Advertisement mentioned brief description of trial, key eligibility criteria and trial e-mail address, but was ultimately determined by the journalist or media liaison. | 6 | 9 (0.4) | 7 (77.8) | 6 (66.7) | 6 (66.7) | 22 (18/4) | 4 |
| University of Sydney alumni magazine and newsletter. | 2 | 4 (0.2) | 4 (100.0) | 3 (75.0) | 3 (75.0) | 8 (6/2) | 3 |
| Local and national newspaper and magazines, including one paid advertisement (AU$500) for a free local newspaper, entitled Mx, that was available to train commuters in Sydney metropolitan area. | 4 | 5 (0.2) | 3 (60.0) | 3 (60.0) | 3 (60.0) | 14 (12/2) | 5 |
| A4 and brochure-sized flyers were printed using university facilities free of charge and distributed to locations in the Sydney metropolitan area by researchers, volunteers and students. The flyer included a brief description of the trial, key eligibility criteria and trial e-mail address. Over 17,000 flyers delivered in total, at AU$0.05 per flyer (total of AU$850). | - | 69 (2.7) | 27 (39.1) | 17 (24.6) | 16 (23.2) | 566 (538/28) | 35 |
| Annual Sydney Craft & Quilt Fair held over 4 consecutive days (300 flyers delivered per day). | 1 | 14 (0.6) | 5 (35.7) | 3 (21.4) | 3 (21.4) | 20 (14/6) | 7 |
| Hospitals in the Sydney metropolitan area, in waiting rooms, staff rooms and common areas. | Continuous | 6 (0.2) | 3 (50.0) | 2 (33.3) | 2 (33.3) | 22 (20/2) | 11 |
| Libraries, common rooms and study spaces within the University of Sydney campus. | Continuous | 5 (0.2) | 3 (60.0) | 2 (40.0) | 2 (40.0) | 22 (20/2) | 11 |
| 50–70 pharmacy and/or chemist sites (10 flyers delivered per site) and 100 medical practices (10 flyers delivered per site). | Continuous | 8 (0.3) | 4 (50.0) | 4 (50.0) | 4 (50.0) | 243 (240/3) | 61 |
| Houses and unit complexes (15,000 flyers delivered in total) | Continuous | 10 (0.4) | 4 (40.0) | 2 (20.0) | 2 (20.0) | 244(240/4) | 122 |
| Individual did not specify or could not recall where they found flyer. | - | 19 (0.8) | 7 (36.8) | 4 (21.1) | 3 (15.8) | 8 (NA/8) | 3 |
| 6 libraries, 10–20 grocery stores/shopping centres, gyms and women’s centre (10 flyers delivered per site). | Continuous | 7 (0.3) | 1 (14.3) | 0 (0.0) | 0 (0.0) | 7 (4/3) | NE |
| Internet-based (total) | Free advertisements were featured in online health articles and social networking sites. Researchers requested a brief advertisement of the trial to be included in the footer of articles or as social media posts, including at least a brief description of the trial and e-mail address. | - | 1082 (43.0) | 128 (11.8) | 40 (3.7) | 24 (2.2) | 541 (110/431) | 23 |
| Free advertisements were featured at the bottom of online health and nutrition-related articles of news and magazine sites which requested expert commentary from trial researchers. | 37 | 1,033 (41.1) | 127 (12.3) | 40 (3.9) | 24 (2.3) | 521 (110/411) | 22 |
| Image of the trial flyer was posted on Facebook health pages related to women’s health and fitness. | 1 | 32 (1.3) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 13 (NA/13) | NE |
| Individual read about trial through other online source which referred to an article or media release that advertised the trial. | Continuous | 17 (0.7) | 1 (5.9) | 0 (0.0) | 0 (0.0) | 7 (NA/7) | NE |
| Clinical trial databases and intranets | Advertisements and trial flyer were featured on staff intranets and portals of the University of Sydney, local tertiary hospitals (St Vincent’s Hospital and Royal Prince Alfred Hospital) and a local health network (Human Services Network). An ongoing advertisement was also listed on the University of Sydney clinical trials webpage which includes a database for research volunteers. Registrants in the database who met the trial criteria were invited by e-mail to arrange a telephone screening. | Continuous | 248 (9.9) | 40 (16.1) | 17 (6.9) | 9 (3.6) | 199 (100/99) | 22 |
| Referrals from healthcare professionals | Personal letter invitations and trial information packs (10 flyers and a participant information sheet per pack) sent to healthcare professionals in medical clinics across Sydney metropolitan suburbs requesting referrals of suitable patients. Follow-up packs were sent to healthcare professionals or clinics that responded to initial invitations or referred individual(s). Participants enrolled into the trial provided details of referring healthcare professionals. ~50 professionals or clinics were sent packs, at AU$1.10 per pack (total of AU$55). | Continuous | 10 (0.4) | 5 (50.0) | 0 (0.0) | 0 (0.0) | 24 (20/4) | NE |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsu, M.S.H.; Harper, C.; Gibson, A.A.; Sweeting, A.N.; McBride, J.; Markovic, T.P.; Caterson, I.D.; Byrne, N.M.; Sainsbury, A.; Seimon, R.V. Recruitment Strategies for a Randomised Controlled Trial Comparing Fast Versus Slow Weight Loss in Postmenopausal Women with Obesity—The TEMPO Diet Trial. Healthcare 2018, 6, 76. https://doi.org/10.3390/healthcare6030076
Hsu MSH, Harper C, Gibson AA, Sweeting AN, McBride J, Markovic TP, Caterson ID, Byrne NM, Sainsbury A, Seimon RV. Recruitment Strategies for a Randomised Controlled Trial Comparing Fast Versus Slow Weight Loss in Postmenopausal Women with Obesity—The TEMPO Diet Trial. Healthcare. 2018; 6(3):76. https://doi.org/10.3390/healthcare6030076
Chicago/Turabian StyleHsu, Michelle S.H., Claudia Harper, Alice A. Gibson, Arianne N. Sweeting, John McBride, Tania P. Markovic, Ian D. Caterson, Nuala M. Byrne, Amanda Sainsbury, and Radhika V. Seimon. 2018. "Recruitment Strategies for a Randomised Controlled Trial Comparing Fast Versus Slow Weight Loss in Postmenopausal Women with Obesity—The TEMPO Diet Trial" Healthcare 6, no. 3: 76. https://doi.org/10.3390/healthcare6030076
APA StyleHsu, M. S. H., Harper, C., Gibson, A. A., Sweeting, A. N., McBride, J., Markovic, T. P., Caterson, I. D., Byrne, N. M., Sainsbury, A., & Seimon, R. V. (2018). Recruitment Strategies for a Randomised Controlled Trial Comparing Fast Versus Slow Weight Loss in Postmenopausal Women with Obesity—The TEMPO Diet Trial. Healthcare, 6(3), 76. https://doi.org/10.3390/healthcare6030076