




Pilot Randomized Controlled Study on the Effectiveness of a Virtual Reality-Based Dementia Prevention Program Using Self-Regulated Learning Strategies Among Older Adults with Mild Cognitive Impairment

 , , , , , and
, , , , , and
Abstract
1. Introduction
2. Materials and Methods
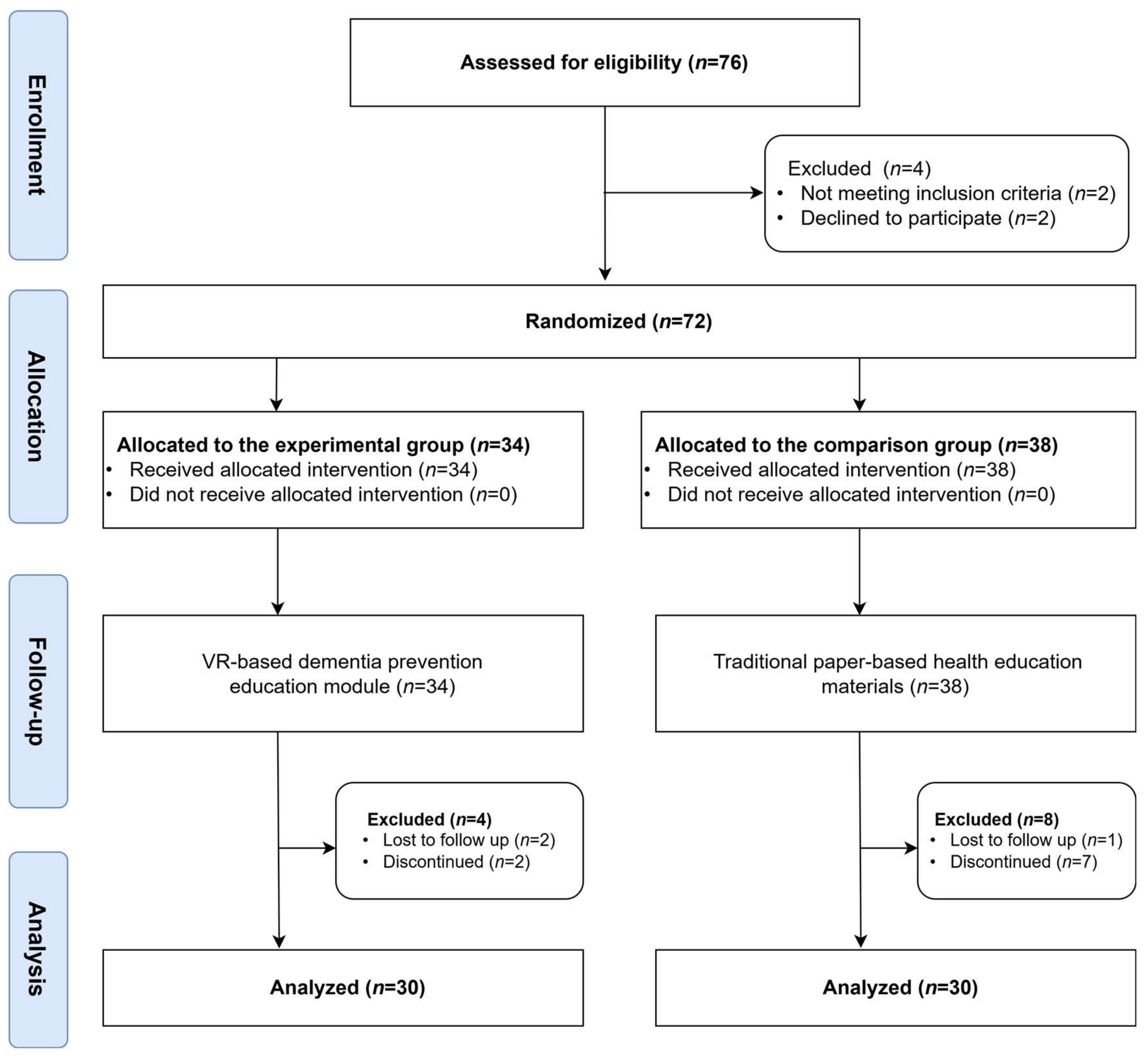
2.1. Study Design
2.2. Participants
2.3. Study Procedure
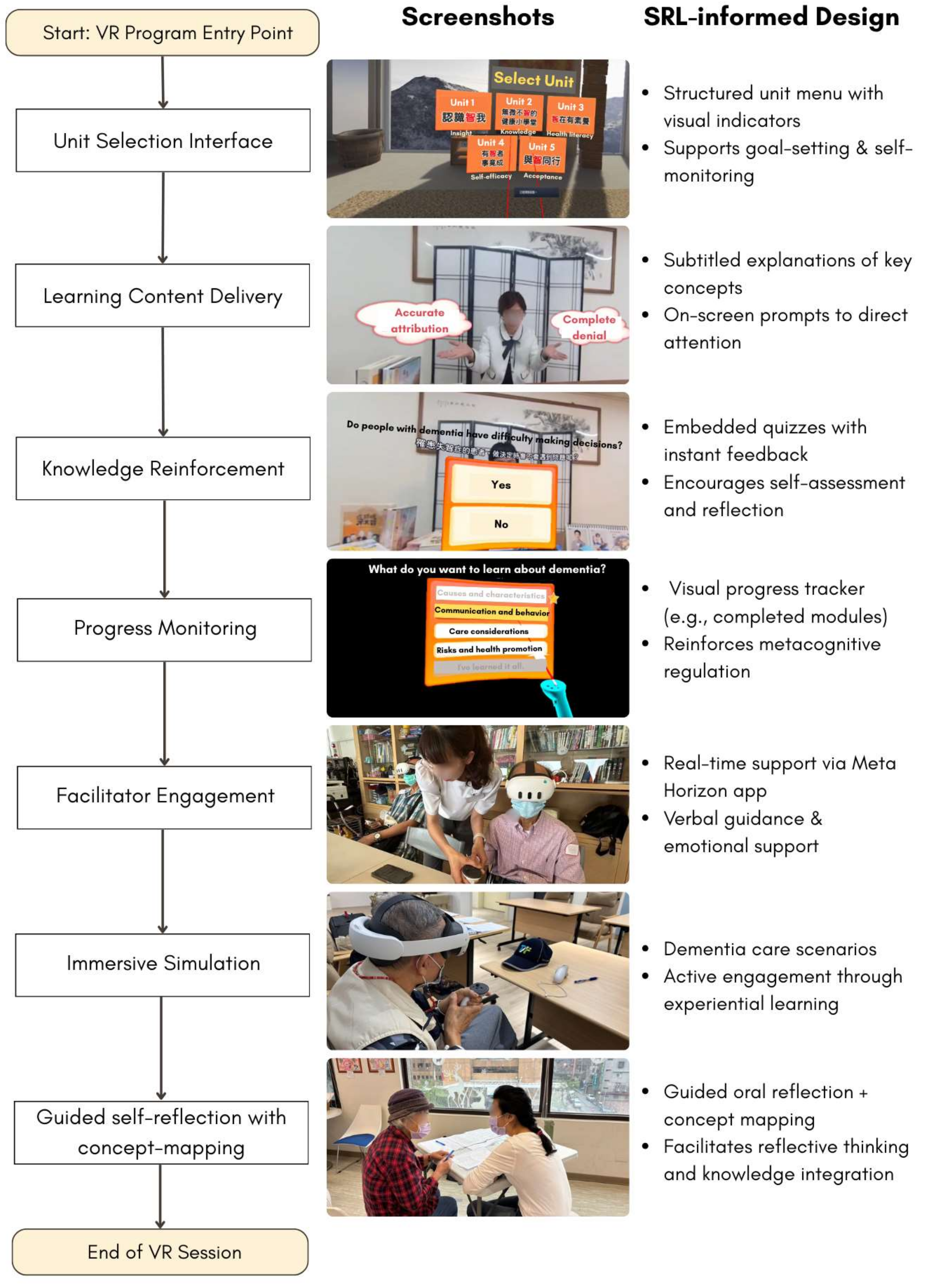
2.4. Intervention Development
2.5. Measurements
2.5.1. Dementia-Related Knowledge
2.5.2. Dementia-Related Health Literacy
2.5.3. Self-Efficacy
2.6. Data Collection and Analysis
2.7. Ethical Considerations
3. Results
3.1. Demographic Characteristics
3.2. Intervention Effects on Dementia Knowledge, Health Literacy, and Self-Efficacy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
AI Disclosure Statement
Abbreviations
| MCI | Mild cognitive impairment |
| SRL | Self-regulated learning |
References
- World Health Organizations. Dementia. Available online: https://www.who.int/news-room/fact-sheets/detail/dementia (accessed on 28 December 2024).
- Alzheimer’s Association. 2023 Alzheimer’s disease facts and figures. Alzheimers Dement. 2023, 19, 1598–1695. [Google Scholar] [CrossRef] [PubMed]
- Rabins, P.V.; Mace, N.L.; Lucas, M.J. The impact of dementia on the family. JAMA 1982, 248, 333–335. [Google Scholar] [CrossRef]
- Bradfield, N.I. Mild cognitive impairment: Diagnosis and subtypes. Clin. EEG Neurosci. 2023, 54, 4–11. [Google Scholar] [CrossRef]
- Ganguli, M.; Jia, Y.; Hughes, T.F.; Snitz, B.E.; Chang, C.C.H.; Berman, S.B.; Sullivan, K.J.; Kamboh, M.I. Mild cognitive impairment that does not progress to dementia: A population-based study. J. Am. Geriatr. Soc. 2019, 67, 232–238. [Google Scholar] [CrossRef]
- Xiao, L.; Zhou, C.; Zhang, S.; Wang, Y. A bibliometric analysis on the health behaviors related to mild cognitive impairment. Front. Aging Neurosci. 2024, 16, 1402347. [Google Scholar] [CrossRef]
- Perry, M.; Drašković, I.; Lucassen, P.; Vernooij-Dassen, M.; van Achterberg, T.; Rikkert, M.O. Effects of educational interventions on primary dementia care: A systematic review. Int. J. Geriatr. Psychiatry 2011, 26, 1–11. [Google Scholar] [CrossRef]
- D’Cruz, K.; Meikle, L.; White, M.; Herrmann, A.; McCallum, C.; Romero, L. Tailoring education of adults with cognitive impairment in the inpatient hospital setting: A scoping review. Aust. Occup. Ther. J. 2021, 68, 90–102. [Google Scholar] [CrossRef]
- Pintrich, P.R. A conceptual framework for assessing motivation and self-regulated learning in college students. Educ. Psychol. Rev. 2004, 16, 385–407. [Google Scholar] [CrossRef]
- Zimmerman, B.J. Self-regulated learning and academic achievement: An overview. Educ. Psychol. 1990, 25, 3–17. [Google Scholar] [CrossRef]
- Robinson, J.D.; Persky, A.M. Developing self-directed learners. Am. J. Pharm. Educ. 2020, 84, 847512. [Google Scholar] [CrossRef]
- Schlomann, A.; Even, C.; Hammann, T. How older adults learn ICT—Guided and self-regulated learning in individuals with and without disabilities. Front. Comput. Sci. 2022, 3, 803740. [Google Scholar] [CrossRef]
- Lin, Y.; Wang, S.; Lan, Y. The research on the self-regulation strategies support for virtual interaction. Multimed. Tools Appl. 2024, 83, 49723–49747. [Google Scholar] [CrossRef]
- An, J.; Oh, J.; Park, K. Self-Regulated Learning Strategies for Nursing Students: A Pilot Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2022, 19, 9058. [Google Scholar] [CrossRef]
- D’Cunha, N.M.; Nguyen, D.; Naumovski, N.; McKune, A.J.; Kellett, J.; Georgousopoulou, E.N.; Frost, J.; Isbel, S. A Mini-Review of Virtual Reality-Based Interventions to Promote Well-Being for People Living with Dementia and Mild Cognitive Impairment. Gerontology 2019, 65, 430–440. [Google Scholar] [CrossRef] [PubMed]
- Bauer, A.C.M.; Andringa, G. The Potential of Immersive Virtual Reality for Cognitive Training in Elderly. Gerontology 2020, 66, 614–623. [Google Scholar] [CrossRef]
- Mandal, K.; Morrison, A.M.; Bag, S. Developing virtual reality tourism for people with dementia based on meeting psychological and behavioural needs. Tour. Manag. 2025, 108, 105100. [Google Scholar] [CrossRef]
- Porras-Garcia, B.; Rojas-Rincón, J.; Adams, A.; Garolera, M.; Chang, R. Immersive Virtual Reality Cognitive Training for Improving Cognition and Depressive Symptoms Among Older Adults. Current Evidence and Future Recommendations. A Systematic Review. Cyberpsychology Behav. Soc. Netw. 2024, 27, 692–703. [Google Scholar] [CrossRef]
- Liu, J.Y.W.; Yin, Y.-H.; Kor, P.P.K.; Cheung, D.S.K.; Zhao, I.Y.; Wang, S.; Su, J.J.; Christensen, M.; Tyrovolas, S.; Leung, A.Y. The effects of immersive virtual reality applications on enhancing the learning outcomes of undergraduate health care students: Systematic review with meta-synthesis. J. Med. Internet Res. 2023, 25, e39989. [Google Scholar] [CrossRef]
- Oliveira, J.; Gamito, P.; Souto, T.; Conde, R.; Ferreira, M.; Corotnean, T.; Fernandes, A.; Silva, H.; Neto, T. Virtual reality-based cognitive stimulation on people with mild to moderate dementia due to Alzheimer’s disease: A pilot randomized controlled trial. Int. J. Environ. Res. Public Health 2021, 18, 5290. [Google Scholar] [CrossRef]
- Appel, L.; Appel, E.; Kisonas, E.; Lewis-Fung, S.; Pardini, S.; Rosenberg, J.; Appel, J.; Smith, C. Evaluating the impact of virtual reality on the behavioral and psychological symptoms of dementia and quality of life of inpatients with dementia in acute care: Randomized controlled trial (VRCT). J. Med. Internet Res. 2024, 26, e51758. [Google Scholar] [CrossRef]
- Kim, O.; Pang, Y.; Kim, J.-H. The effectiveness of virtual reality for people with mild cognitive impairment or dementia: A meta-analysis. BMC Psychiatry 2019, 19, 219. [Google Scholar] [CrossRef]
- Manera, V.; Chapoulie, E.; Bourgeois, J.; Guerchouche, R.; David, R.; Ondrej, J.; Drettakis, G.; Robert, P. A feasibility study with image-based rendered virtual reality in patients with mild cognitive impairment and dementia. PLoS ONE 2016, 11, e0151487. [Google Scholar] [CrossRef]
- Thompson, M.; Yu, Z.; Odum, S. Randomization Strategies. In Introduction to Surgical Trials; Lyman, S., Ayeni, O.R., Koh, J.L., Nakamura, N., Karlsson, J., Eds.; Springer Nature Switzerland: Cham, Switzerland, 2024; pp. 13–19. [Google Scholar]
- Coban, M.; Bolat, Y.I.; Goksu, I. The potential of immersive virtual reality to enhance learning: A meta-analysis. Educ. Res. Rev. 2022, 36, 100452. [Google Scholar] [CrossRef]
- Hendry, K.; Green, C.; McShane, R.; Noel-Storr, A.H.; Stott, D.J.; Anwer, S.; Sutton, A.J.; Burton, J.K.; Quinn, T.J. AD-8 for detection of dementia across a variety of healthcare settings. Cochrane Database Syst. Rev. 2019. [Google Scholar] [CrossRef]
- Cines, S.; Farrell, M.; Steffener, J.; Sullo, L.; Huey, E.; Karlawish, J.; Cosentino, S. Examining the pathways between self-awareness and well-being in mild to moderate Alzheimer disease. Am. J. Geriatr. Psychiatry 2015, 23, 1297–1306. [Google Scholar] [CrossRef]
- Annear, M.J.; Toye, C.; Elliott, K.-E.J.; McInerney, F.; Eccleston, C.; Robinson, A. Dementia knowledge assessment scale (DKAS): Confirmatory factor analysis and comparative subscale scores among an international cohort. BMC Geriatr. 2017, 17, 168. [Google Scholar] [CrossRef]
- Kimzey, M.; Howe, C.J.; Martin, C.; McLarty, J.; Baucham, R. Development of health literacy in persons and caregivers living with dementia: A qualitative directed content analysis. Dementia 2022, 21, 540–555. [Google Scholar] [CrossRef]
- Ishimaru, M.; Nagata, A.; Sato, T.; Sakai, A.; Suzuki, S.; Kubota, K. Developing an Instructional Design-Based Dementia Education Program. Gerontol. Geriatr. Med. 2022, 8, 23337214221134874. [Google Scholar] [CrossRef]
- Tordet, C.; Fernandez, J.; Jamet, E. The effects of embedded quizzes on self-regulated processes and learning performance during a multimedia lesson. J. Comput. Assist. Learn. 2025, 41, e13083. [Google Scholar] [CrossRef]
- Wang, Y.; Zhang, H.; Wang, J.; Ma, X. The Impact of Prompts and Feedback on the Performance during Multi-Session Self-Regulated Learning in the Hypermedia Environment. J. Intell. 2023, 11, 131. [Google Scholar] [CrossRef]
- Chang, C.-C.; Hwang, G.-J. A structured reflection-based graphic organizer approach for professional training: A technology-supported AQSR approach. Comput. Educ. 2022, 183, 104502. [Google Scholar] [CrossRef]
- Kuo, L.-H.; Chang, C.-H.; Huang, S.-F.; Chien, H.-C.; Huang, C.-M.; Guo, J.-L. User Experience Evaluation of a Spherical Video-based Virtual Reality Dementia Educational Program among Older Adults with Mild Cognitive Impairment. In Proceedings of the 2024 International Conference on Consumer Electronics-Taiwan (ICCE-Taiwan), Taichung, Taiwan, 9–11 July 2024; pp. 27–28. [Google Scholar]
- DeVellis, R.F.; Thorpe, C.T. Scale Development: Theory and Applications; Sage Publications: London, UK, 2021. [Google Scholar]
- Oliveira, D.; Bosco, A.; di Lorito, C. Is poor health literacy a risk factor for dementia in older adults? Systematic literature review of prospective cohort studies. Maturitas 2019, 124, 8–14. [Google Scholar] [CrossRef]
- Nutbeam, D. Health literacy as a public health goal: A challenge for contemporary health education and communication strategies into the 21st century. Health Promot. Int. 2000, 15, 259–267. [Google Scholar] [CrossRef]
- Lin, L.-C.; Huang, C.-M.; Hsu, H.-P.; Liao, J.-Y.; Lin, C.-Y.; Guo, J.-L. Integrating health literacy into a theory-based drug-use prevention program: A quasi-experimental study among junior high students in Taiwan. BMC Public Health 2021, 21, 1768. [Google Scholar] [CrossRef]
- Chiang, C.-H.; Huang, C.-M.; Sheu, J.-J.; Liao, J.-Y.; Hsu, H.-P.; Wang, S.-W.; Guo, J.-L. Examining the effectiveness of 3D virtual reality training on problem-solving, self-efficacy, and teamwork among inexperienced volunteers helping with drug use prevention: Randomized controlled trial. J. Med. Internet Res. 2021, 23, e29862. [Google Scholar] [CrossRef]
- Ren, Y.; Wang, Q.; Liu, H.; Wang, G.; Lu, A. Effects of immersive and non-immersive virtual reality-based rehabilitation training on cognition, motor function, and daily functioning in patients with mild cognitive impairment or dementia: A systematic review and meta-analysis. Clin. Rehabil. 2024, 38, 305–321. [Google Scholar] [CrossRef]
- Van der Kruk, S.R.; Zielinski, R.; MacDougall, H.; Hughes-Barton, D.; Gunn, K.M. Virtual reality as a patient education tool in healthcare: A scoping review. Patient Educ. Couns. 2022, 105, 1928–1942. [Google Scholar] [CrossRef]
- Fang, J.-W.; Li-Yuan, H.; Gwo-Jen, H.; Xiu-Wei, Z.; Chu-Nu, B.; Fu, Q.-K. A concept mapping-based self-regulated learning approach to promoting students’ learning achievement and self-regulation in STEM activities. Interact. Learn. Environ. 2023, 31, 7159–7181. [Google Scholar] [CrossRef]
- Dinh, T.T.H.; Bonner, A. Exploring the relationships between health literacy, social support, self-efficacy and self-management in adults with multiple chronic diseases. BMC Health Serv. Res. 2023, 23, 923. [Google Scholar] [CrossRef]
- Lee, J.; Cho, E.; Kim, H.; Lee, K.H.; Kim, E.; Ye, B.S. The development and evaluation of a self-efficacy enhancement program for older adults with mild cognitive impairment. Appl. Nurs. Res. 2023, 73, 151726. [Google Scholar] [CrossRef]
- Chen, J. The effectiveness of self-regulated learning (SRL) interventions on L2 learning achievement, strategy employment and self-efficacy: A meta-analytic study. Front. Psychol. 2022, 13, 1021101. [Google Scholar] [CrossRef]
- Follmer, D.J. Implementing a Simple, Scalable Self-Regulated Learning Intervention to Promote Graduate Learners’ Statistics Self-Efficacy and Concept Knowledge. J. Stat. Data Sci. Educ. 2023, 31, 80–90. [Google Scholar] [CrossRef]
- Niu, Z.; Willoughby, J.; Zhou, R. Associations of Health Literacy, Social Media Use, and Self-Efficacy With Health Information–Seeking Intentions Among Social Media Users in China: Cross-sectional Survey. J. Med. Internet Res. 2021, 23, e19134. [Google Scholar] [CrossRef]
- Park, S.; Shin, H.J.; Kwak, H.; Lee, H.J. Effects of immersive technology–based education for undergraduate nursing students: Systematic review and meta-analysis using the grading of recommendations, assessment, development, and evaluation (GRADE) approach. J. Med. Internet Res. 2024, 26, e57566. [Google Scholar] [CrossRef]
- Skidmore, N.; Ryan, C.; Mankelow, J.; Bradford, C.; Graham, A.; Martin, D. Exploring the potential of virtual reality for the self-management of chronic pain–a scoping review of its use to address health literacy. Musculoskelet. Sci. Pract. 2024, 72, 102962. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Unit | Learning Objective | Outcome Variable |
|---|---|---|
| 1 |
| Insight |
| 2 | Acquire knowledge about dementia, encompassing its causes, characteristics, communication and behavioral aspects, care considerations, risks, and preventive methods. | Dementia-related knowledge |
| 3 |
| Health literacy |
| 4 | Foster confidence and a sense of capability in accomplishing specific tasks or goals. | Self-efficacy |
| 5 |
| Acceptance of dementia |
| Variables | Experimental Group (n = 30, 50%) | Comparison Group (n = 30, 50%) | χ2/t | p-Value |
|---|---|---|---|---|
| Age (years), mean (SD) | 76.83 (6.70) | 76.67 (7.01) | −0.094 | 0.925 |
| Gender, n (%) | 0.000 | 1.000 | ||
| Male | 6 (20.00) | 6 (20.00) | ||
| Female | 24 (80.00) | 24 (80.00) | ||
| Marital status, n (%) | 2.072 | 0.558 | ||
| Unmarried | 0 (0.00) | 2 (6.67) | ||
| Married | 13 (43.33) | 12 (40.00) | ||
| Divorced or separated | 1 (3.33) | 1 (3.33) | ||
| Widowed | 16 (53.33) | 15 (50.00) | ||
| Educational level, n (%) | 0.328 | 0.988 | ||
| Elementary school | 8 (27.59) | 9 (32.14) | ||
| Middle school | 4 (13.79) | 4 (14.29) | ||
| High school | 9 (31.03) | 9 (32.14) | ||
| University and above | 8 (27.59) | 6 (21.43) | ||
| Past experience with dementia-related health education, n (%) | 1.014 | 0.314 | ||
| Yes | 12 (40.0) | 8 (27.59) | ||
| No | 18 (60.0) | 21 (72.41) | ||
| Relatives diagnosed with dementia, n (%) | 4.109 | 0.128 | ||
| Yes | 2 (6.67) | 7 (24.14) | ||
| No | 23 (76.67) | 16 (55.17) | ||
| Not sure | 5 (16.67) | 6 (20.69) | ||
| Variables | Coefficient (β) | SE | Wald χ2 | p-Value |
|---|---|---|---|---|
| Dementia-related Knowledge (0–25 points) | ||||
| Group (Experimental group) b | −0.400 | 1.229 | 0.106 | 0.745 |
| Time (Post-test) c | 0.700 | 0.640 | 1.197 | 0.274 |
| Group (Experimental) Time (Post-test) d | 5.333 | 1.359 | 15.391 | <0.001 *** |
| Causes and Characteristics (0–7 points) | ||||
| Group (Experimental group) b | −0.333 | 0.428 | 0.606 | 0.436 |
| Time (Post-test) c | 0.567 | 0.244 | 5.415 | 0.020 * |
| Group (Experimental) Time (Post-test) d | 1.767 | 0.503 | 12.318 | <0.001 *** |
| Communication and Behavior (0–6 points) | ||||
| Group (Experimental group) b | −0.367 | 0.384 | 0.910 | 0.340 |
| Time (Post-test) c | −0.033 | 0.186 | 0.032 | 0.857 |
| Group (Experimental) Time (Post-test) d | 1.167 | 0.443 | 6.943 | 0.008 ** |
| Care Consideration (0–6 points) | ||||
| Group (Experimental group) b | −0.033 | 0.415 | 0.006 | 0.936 |
| Time (Post-test) c | −0.067 | 0.320 | 0.044 | 0.835 |
| Group (Experimental) Time (Post-test) d | 1.400 | 0.450 | 9.664 | 0.002 ** |
| Risks and Health Promotion (0–6 points) | ||||
| Group (Experimental group) b | 0.333 | 0.390 | 0.730 | 0.393 |
| Time (Post-test) c | 0.233 | 0.187 | 1.562 | 0.211 |
| Group (Experimental) Time (Post-test) d | 1.000 | 0.360 | 7.710 | 0.005 ** |
| Health Literacy (20–100 points) | ||||
| Group (Experimental group) b | 0.333 | 4.944 | 0.005 | 0.946 |
| Time (Post-test) c | −0.867 | 2.398 | 0.131 | 0.718 |
| Group (Experimental) Time (Post-test) d | 6.700 | 4.518 | 2.199 | 0.138 |
| Functional Health Literacy (8–40 points) | ||||
| Group (Experimental group) b | 0.367 | 1.971 | 0.035 | 0.852 |
| Time (Post-test) c | −0.533 | 0.947 | 0.317 | 0.573 |
| Group (Experimental) Time (Post-test) d | 0.933 | 1.695 | 0.303 | 0.582 |
| Critical Health Literacy (7–35 points) | ||||
| Group (Experimental group) b | 0.067 | 1.902 | 0.001 | 0.972 |
| Time (Post-test) c | −0.600 | 0.953 | 0.396 | 0.529 |
| Group (Experimental) Time (Post-test) d | 3.700 | 1.728 | 4.584 | 0.032 * |
| Interactive Health Literacy (5–25 points) | ||||
| Group (Experimental group) b | −0.100 | 1.458 | 0.005 | 0.945 |
| Time (Post-test) c | 0.267 | 1.052 | 0.064 | 0.800 |
| Group (Experimental) Time (Post-test) d | 2.067 | 1.734 | 1.421 | 0.233 |
| Self-efficacy (6–30 points) | ||||
| Group (Experimental group) b | −1.267 | 1.633 | 0.602 | 0.438 |
| Time (Post-test) c | −0.033 | 0.947 | 0.001 | 0.972 |
| Group (Experimental) Time (Post-test) d | 4.200 | 1.588 | 6.997 | 0.008 ** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, C.-H.; Huang, K.-Y.; Kuo, L.-H.; Cheng, Y.-W.; Huang, S.-F.; Chuang, T.-H.; Huang, C.-M.; Guo, J.-L. Pilot Randomized Controlled Study on the Effectiveness of a Virtual Reality-Based Dementia Prevention Program Using Self-Regulated Learning Strategies Among Older Adults with Mild Cognitive Impairment. Healthcare 2025, 13, 1082. https://doi.org/10.3390/healthcare13091082
Chang C-H, Huang K-Y, Kuo L-H, Cheng Y-W, Huang S-F, Chuang T-H, Huang C-M, Guo J-L. Pilot Randomized Controlled Study on the Effectiveness of a Virtual Reality-Based Dementia Prevention Program Using Self-Regulated Learning Strategies Among Older Adults with Mild Cognitive Impairment. Healthcare. 2025; 13(9):1082. https://doi.org/10.3390/healthcare13091082
Chicago/Turabian StyleChang, Ching-Hao, Kuei-Yu Huang, Lou-Hui Kuo, Ya-Wen Cheng, Su-Fei Huang, Tien-Hsi Chuang, Chiu-Mieh Huang, and Jong-Long Guo. 2025. "Pilot Randomized Controlled Study on the Effectiveness of a Virtual Reality-Based Dementia Prevention Program Using Self-Regulated Learning Strategies Among Older Adults with Mild Cognitive Impairment" Healthcare 13, no. 9: 1082. https://doi.org/10.3390/healthcare13091082
APA StyleChang, C.-H., Huang, K.-Y., Kuo, L.-H., Cheng, Y.-W., Huang, S.-F., Chuang, T.-H., Huang, C.-M., & Guo, J.-L. (2025). Pilot Randomized Controlled Study on the Effectiveness of a Virtual Reality-Based Dementia Prevention Program Using Self-Regulated Learning Strategies Among Older Adults with Mild Cognitive Impairment. Healthcare, 13(9), 1082. https://doi.org/10.3390/healthcare13091082